










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 no.11 Pretoria nov. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i11.1558
SPECIAL SERIES ON THE DISTRICT HEALTH SYSTEM
Improving health outcomes and quality at the subdistrict level: Evaluation of the '3 feet model' in Waterberg District, Limpopo Province, South Africa
H SchneiderI; F MukindaI; J CupidoII; J WesselsIII; P KupaIV; P LebohoIV; N NkoanaIV; N BoschV; Y PillayVI
IPhD; School of Public Health and SAMRC Health Services to Systems Research Unit, University of the Western Cape, Cape Town, South Africa
IIMB ChB; Clinton Health Access Initiative, Pretoria, South Africa
IIIMPH; Clinton Health Access Initiative, Pretoria, South Africa
IVMB ChB; Waterberg Health District, Limpopo Department of Health, Polokwane, South Africa
VDipl Nursing Administration; Waterberg Health District, Limpopo Department of Health, Polokwane, South Africa
VIPhD; Clinton Health Access Initiative, Pretoria, South Africa, and Department of Public Health and Health Systems, Stellenbosch University, Cape Town, South Africa
ABSTRACT
BACKGROUND: There is a gap in understanding of potential roles and actions at the subdistrict level to improve quality of care and health outcomes in South Africa (SA
OBJECTIVES: To report on the evaluation of a subdistrict health system-strengthening initiative that aimed to reduce maternal, newborn and child mortality, referred to as the '3 feet model' in Waterberg District, Limpopo Province, SA. The model is centred on systems of real-time morbidity/mortality surveillance and co-ordinated responses. It was implemented in three of five Waterberg subdistricts over an 18-month period in 2021 and 2022
METHODS: A prospective, process-tracing evaluation was conducted jointly between researchers, intervention partners and subdistrict decision-makers. Data sources combined ~100 hours of researcher participant observation, interviews with 14 health system actors, structured reflections by three subdistrict managers and information from the routine District Health Information System. Sources were triangulated and analysed based on a priori hypotheses on mechanisms of action
RESULTS: Following uptake of the model, the perinatal mortality rate (PMR) improved by 28.8%, 11.5% and 28% in the three subdistricts, respectively, while the PMR worsened in two of four neighbouring subdistricts. Plausible factors in implementation successes were the presence of stable and committed hybrid (clinical-managerial) subdistrict leaders and their ability to overcome entrenched silos between a variety of system actors; new collaborative relationships between primary healthcare facilities, hospitals and emergency medical services; the generation and packaging of information in ways that directed responses ('actionable intelligence'); and support from senior district managers
CONCLUSION: While not advocating for a cut-and-paste approach to improving quality and outcomes, positive experiences in Waterberg District suggest that the principles and mechanisms of action of the 3 feet model have wider relevance for policy and practice, especially as emphasis shifts towards the subdistrict as a core unit of population health and wellbeing in SA
The District Health System (DHS) was formally established in the National Health Act No. 61 of 2003 as the building block of South Africa (SA)'s national health system.[1] This policy followed the World Health Organization (WHO)'s recommendation of the DHS as the most decentralised structure of governance for the achievement of an equitable health system based on primary healthcare (PHC).[2] Geographically and population-wise, the subdistrict in SA most closely resembles the WHO's ideal of a health district, that is, of sufficient scale and scope to impact on health while retaining the ability to respond to local needs and co-ordinate actors.[2] With the advent of National Health Insurance (NHI) reforms, and post-COVID-19 pandemic recovery plans, the subdistrict is (re-)emerging as an important unit of governance and service delivery co-ordination in SA. In the NHI Bill (2019),[3] the 'contracting unit for primary healthcare' is 'comprised of a district hospital, clinics or community health centres and ward-based outreach teams and private providers organised in horizontal networks within a specified geographical subdistrict area'.[3]
Strengthening the subdistrict is therefore key to improving the quality of healthcare and health outcomes, which still fall far short of expectations for most health and disease priorities.[4] Poor maternal and newborn care, in particular, is one of the drivers of the large burden of medicolegal claims in provincial health departments.[5] Despite longstanding efforts to address quality shortfalls through training, clinical outreach and various audit systems, these efforts have tended to be fragmented locally and across levels of the health system.[4] There is a gap in understanding of the governance and leadership roles required at the subdistrict level to sustain quality and improve outcomes.[4,6]
Using a process-tracing evaluation methodology, this article reports experiences with a bottom-up approach to strengthening quality and outcomes, colloquially referred to as the '3 feet model', in three subdistricts of the Waterberg District, Limpopo Province, SA. The 3 feet model was supported by a partner organisation with the goal of improving maternal and newborn health (MNH) outcomes. We describe the elements of the model and their implementation, report routine data on outcomes, consider plausible pathways of effectiveness and conclude by discussing strategies for achieving sustainability and scale of such a model. The article is jointly written by subdistrict and district managers (PK, PL, NN, NB), partners (JC, JW, YP) and researchers (HS, FM) and compiled from formal data gathering and structured reflections.
Methods
Setting
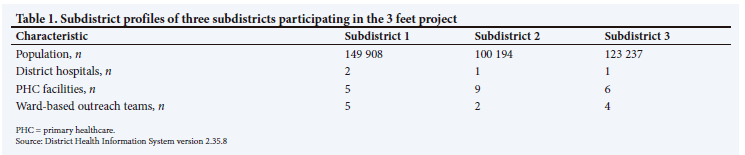
Waterberg District is one of five districts in Limpopo, bordering on Gauteng and North West provinces and Botswana. The district is largely rural, with a population of ~760 000. More than 90% of Limpopo Province's population is reliant on the public health system, provided in Waterberg District through a mix of 59 PHC facilities, 7 district hospitals and 1 regional hospital, organised into five subdistricts. Table 1 gives the profiles of the three subdistricts participating in the 3 feet project.
Description of the model and implementation
The 3 feet model was first developed and introduced in 2014 in response to high maternal, neonatal and child mortality in selected districts of the country, and was inspired by the Malaysian strategy of local, bottom-up (3 feet) rather than central (30 000 feet) planning.[7,8] The model is an outcome-orientated approach to stewardship of quality at subdistrict level, centred on real-time mortality surveillance and response, and establishment of a local governance process, the Monitoring and Response Unit (MRU). The MRU seeks to create functional co-ordination between community, PHC and district hospital services, and between line managers ('drivers'), clinicians across professions ('experts'), and health programme and information managers ('navigators'), referred to as the 'management triangle'. The model promotes whole-systems thinking, real-time and 'actionable' data/intelligence, local decision-making and evidence-informed responses, underpinned by the principles of comprehensive, person-centred PHC and integration into DHS systems. In these various ways, the model seeks to address 'systematic fragmentation of critical components of the health system', which is a barrier to improved outcomes.[8] An implementation package includes a step-wise introduction to the model and reporting and decision-making heuristics and tools.[9] The latter include the 'open tap analogy', a framework showing the links between prevention and care, a real-time mortality review and response framework/algorithm, consolidated death reports and data and decision-making dashboards (Appendix 1: https://www.samedical.org/file/2133).
The model was successfully trialled in the Waterberg and Gert Sibande districts of Limpopo and Mpumalanga provinces, respectively, between 2014 and 2018. It was designed and supported by two facilitators (JC, JW) with extensive prior managerial and training experience, respectively, who visited the districts monthly initially, and then less frequently over time. A principle of the approach was that no new resources would be provided and that interventions would be integrated into existing managerial and accountability processes (referred to as the 'add in, not add on' principle). An evaluation of the model in 2017 documented declines in mortality (most notably from severe acute malnutrition) in the districts, and described its key mechanisms of impact.[10,11] Elements of the model were subsequently incorporated into revised district planning guidelines and later institutionalised in Limpopo Province in the form of subdistrict and district 'performance, monitoring and response forums'.[6]
In March 2021, the original facilitators (JC, JW) were re-engaged to support a new phase of work in Waterberg District, focused on maternal, newborn and child (<5 years) health. They initially worked in three subdistricts, one of which was still implementing the model from the prior phase of work. The other two subdistricts had had a change of leadership and were newly inducted into the model. Over 18 months (until September 2022), the facilitators made a total of seven visits to the district (typically over 4 days), and held virtual meetings in between visits. The visits and meetings provided training, support to the monthly MRU meetings in each subdistrict, technical support around specific interventions and district-level debriefings. In October 2021, a senior manager in the district mandated expansion of the model to the remaining two Waterberg subdistricts.
The principles and core approach of the model were the same as in the previous phase, with adaptations and new components. These included:
• audit tools for antenatal care in PHC, addressing the major causes of maternal and perinatal mortality ('3Hs': hypertension, HIV and haemorrhage) and associated quality improvement plans
• introduction of clinical governance processes in district hospitals, going beyond maternal, newborn and child health (MNCH), and including:
• training in the International Classification of Diseases (ICD10) coding
• reviews of registers/processes of recording in emergency centres, inpatient wards and outpatient departments
• reviews of both morbidity and mortality data
• assessment of continuing professional development (CPD) needs and mobilising partnerships with public health and family medicine expertise to support CPD
• linkage of mortality and morbidity review processes with formal quarterly performance reviews
• peer networking and support platforms between the subdistricts.
In September 2022, a 1-day reflection, handover and dissemination workshop was held with representatives of the implementing subdistricts, other subdistricts, districts and provincial managers.
Evaluation methodology
Process tracing is a theory-driven methodology suited to studying causal mechanisms in single case studies of multifaceted and multi-actor interventions such as the 3 feet model.[12] Process tracing goes beyond tracking 'implementation fidelity' (adoption of interventions as intended) to elucidating the mechanisms of change. It does this by documenting: (i) actors or 'entities' engaged in activities or 'events'; (ii) how these come together as 'parts' of a change process that plausibly result in outcomes; and (iii) outcomes (improved quality/ reduced mortality).[13]
A flexible, multi-method and prospective evaluation strategy was adopted, intended to generate triangulated insights on real-world implementation. As in the previous phase, evaluative processes were 'wrapped around' an improvement initiative, primarily designed to produce change rather than generate new scientific knowledge.[14] Taking an embedded approach,[15] a joint partner-researcher team was established at the start of the (re)engagement phase, in which the researchers (FM and HS) were both observers (collecting data) and participants (supporting specific activities). The findings in this article combine researcher observations and analysis of routine data with reflections by the facilitators/partners and subdistrict 'drivers'.
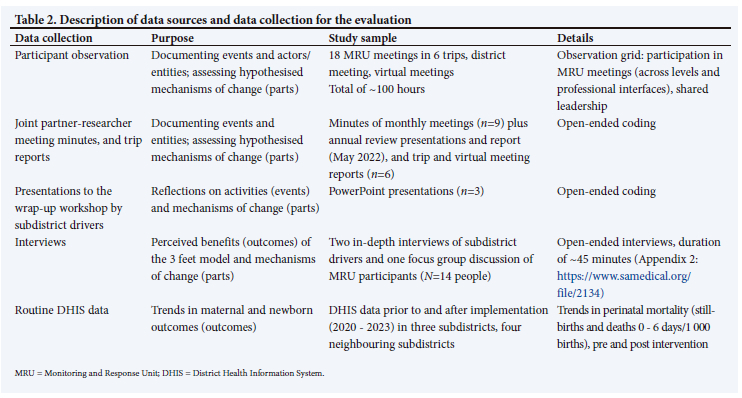
Data collection was informed by hypotheses based on the previous evaluation, namely, that the 3 feet model would enable co-ordinated action through a driver-led system of governance (structuring local collaboration and accountability), supported by actionable intelligence (directing action), empowered mindsets (finding solutions) and an enabling district context (supporting rather than discouraging local innovation).[7,16] The sources of data for the evaluation combine researcher participant observations (documented in notes, trip reports and partner meetings), structured reflections by the subdistrict drivers (documented in presentations to the dissemination workshop in September 2022), interviews by the researchers and the District Health Information System (DHIS).
Routine DHIS data analysed included perinatal mortality rates (PMRs) in three intervention (SD 1 - 3) and four neighbouring (SD 4 - 7) subdistricts (one in the district and three in other districts) starting 1 year prior to project inception (2020/1) and extending 6 months beyond the last engagement (2022/3). Two neighbouring subdistricts were excluded, as they reported data from regional and tertiary facilities and had much higher mortality rates than other subdistricts. Perinatal mortality is amenable to health service interventions,[17] as compared with infant or under-5 mortality, which are influenced by wider socioeconomic contexts. The PMR is also more easily assessed than in-facility maternal mortality, which was a rare event in the three subdistricts over the period.
Details on the different sources of data are outlined in Table 2.
Each source of data was analysed, and synthesised as a description of events, entities, parts and outcomes. Qualitative data were coded and triangulated in these four categories and a final set of themes was generated. The outcome data from the DHIS were analysed in an Excel (Microsoft Corp., USA) spreadsheet.
The research was approved by the University of the Western Cape Biomedical Research Committee (ref. no. BM19/10/16) and the Limpopo Provincial Research Committee (ref. no. LP_2020-12-014). We have anonymised the subdistricts (named D1 - D7), and qualitative observations and interviews are reported by stakeholder group (driver, researcher, partner). Although these data emanate from the co-authors, we report them in the third person.
Results
The detailed thematic analysis of the qualitative data is available as Appendix 3 (https://www.samedical.org/file/2135). Here we summarise the key findings of model implementation (bringing together events and entities), followed by an analysis of trends in perinatal mortality, and finally evidence for the hypothesised mechanisms of change (parts).
Implementation of the 3 feet model (events and entities)
Appendix 1 gives a timeline of events over the 18 months of the programme. The model was (re)-introduced with training on the core tools and processes. They included the open tap analogy framework, the real-time mortality surveillance and response processes, the data/ decision-making dashboards and the MRU structure and meetings. The other elements of the revised model were introduced over the subsequent months.
By the end of the 18 months, the real-time death reporting, review and responses for MNCH had become institutionalised in the routines of the three subdistricts. These were supported by locally developed standard operating procedures (SOPs) with accountability to a senior manager (chief executive officer (CEO) or medical manager) (Table 3). The response to death was 'systematic, holistic and standardised' (driver, SD2), and was integrated into practices at all levels. The methodology and tools were viewed as meaningful, providing 'a system, a structure to work with, you know exactly what you are looking for' (driver, SD1) and directing action on 'when, where, who to act on identified problems at different levels' (driver, SD2). Examples of actions noted during MRU meetings and on dashboards (Appendix 1) included intensification of emergency drills in maternities, new screening processes in clinics, and identification of hot spots and household outreach to identify children with malnutrition.
The real-time review processes drove improved data quality (Appendix 1) and reporting from the three subdistricts. While 'the quality of the data is at the core of the whole process' (driver, SD2), the emphasis on accurate data, rather being an end in itself, was motivated by a search for meaningful actions that could improve outcomes.
There was evidence of the methodology being applied beyond MNCH to include non-communicable diseases (Appendix 1: example of diabetes), and 'even with COVID we applied it, we reviewed all the deaths ... the case [fatality] rate of COVID-19 we are at 15% one of the lowest in the province' (driver, SD1). A widened application of the tools led to the standardisation of morbidity/mortality review across services in the subdistricts, while also shaping priority setting for clinical governance (audits and CPD) and prompting greater engagement with and valuing of community-based care, where, for example 'CHWs [community health workers] [became] involved in identifying and responding appropriately to complications related to NCD [non-communicable diseases] in the community' (driver, SD1).
Implementation was led by the most senior clinician-manager (as CEO or medical manager of the district hospital) in each subdistrict. These 'drivers' were a stable presence throughout the 18 months and believed in the model's theory of change: 'This model works ... this model is one of the best models thus far that I have been exposed to, I will forever ensure that it is there wherever I go' (driver, SD1). These three drivers established successful MRUs to co-ordinate actions in a multidisciplinary team of providers (nurses, doctors, social workers, dietitians) and operational and senior managers from PHC, the district hospital and emergency medical services (EMS). Within a few months, the MRUs were observed to have 'a healthy status' (partner trip report, April 2021), with the 'quality' participation of actors in a model of shared leadership (researcher observation April 2021). As one driver indicated, 'They know that, yes I am the driver, but one can say they are co-drivers. If I'm not here they jump in' (driver, SD2).
The three senior managers also established a peer network, attending each other's meetings, and communicating informally in between meetings. They began reaching out to others within their subdistricts: '... we are calling our neighbouring hospital to try and get them on board ... us calling our neighbour is so that he can see and learn, it's sort of benchmarking how we are running the business of the day. We have decided to support them in their own meeting' (driver, SD1).
During the period of the programme, there were deliberate efforts to engage with and obtain the endorsement and support of senior district managers (who convened two district-wide meetings on the model in 2022), and in the final dissemination workshop, of provincial-level decision-makers, considered key to sustainable implementation and spread.
Constraints to implementation observed were:
• the challenges of working across district and provincial boundaries, as natural health services catchment areas and referral systems did not correspond with formal subdistrict geographical areas
• weak recording and information systems, particularly in the emergency and inpatient departments of district hospitals, limiting possibilities of morbidity surveillance
• the lack of structured approaches to CPD (including clinical, managerial and public health competencies), and significant network and connectivity challenges. In a context of high turnover of staff in these subdistricts, these posed a threat to the continuous induction and renewal required to sustain the model
• the numerous crises and competing demands on managers, where the structured reflections and proactive responses to problems could easily be displaced by other priorities: 'You can have three deadlines at the same time, out of which you need to pick up what matters the most, the one that you know that is important, then you give your whole to it' (driver, SD2).
Outcomes
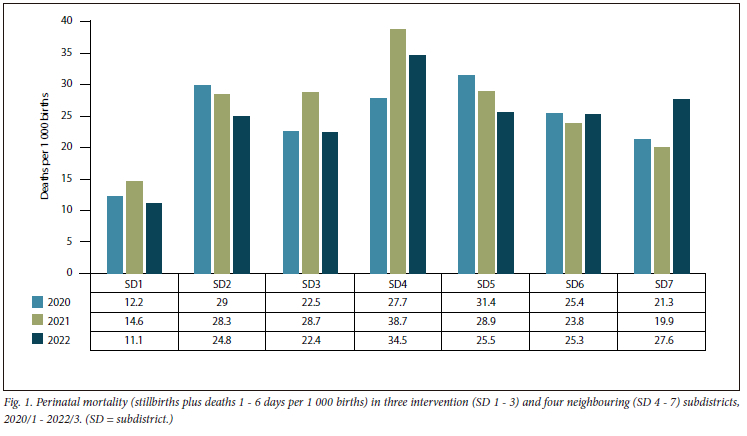
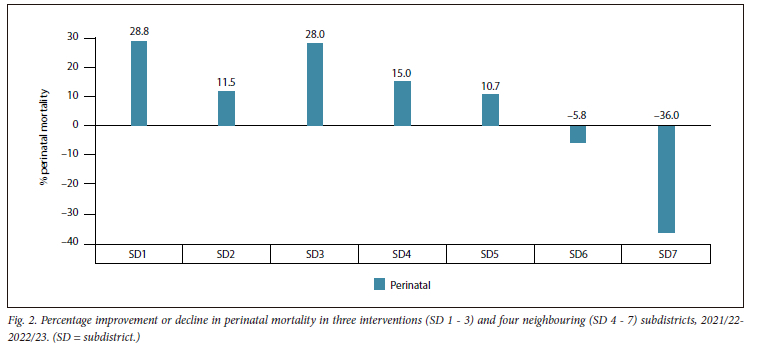
Fig. 1 reports trends in PMRs in the three intervention (SD 1 - 3) and four 'control' (SD 4-7) subdistricts for the 3-year period 2020/1 - 2022/3. The findings present a mixed picture of baseline performance and trends. However, it is possible to make a few tentative observations. Firstly, at the end of the period, the three subdistricts recorded the lowest PMRs of the seven subdistricts, most evident in SD1 and SD3. Secondly, all three subdistricts recorded improvements in PMR over the intervention period (2021/2 -2022/3), again notably in SD1 and SD3, while two of the four control subdistricts recorded declines in performance (Fig. 2).
Interestingly, the rise in perinatal (and under-5) mortality rates in 2021/2 was noted in the MRU meetings of SD3, provoking reflection and analysis of the consequences of COVID-19 lockdown measures for maternal and child health, including in 'unbooked' deliveries, reduced child health clinic attendance, and increasing child malnutrition (partner trip report, November 2021). In general, however, narratives reflected positive experiences of improved outcomes with respect to maternal, child and perinatal outcomes.
Mechanisms of change (parts)
Do the hypothesised mechanisms of the 3 feet model explain positive changes in service delivery and possibly outcomes (whether subjective or objective)?
The first and obvious key success factor in the three subdistricts was the enlistment of the three senior managers as drivers of implementation, their stable presence and capabilities in 'leadership, decision-making and resource allocation' (driver, SD2). As affirmed by one, 'I feel that it needs the driver to be there. Now, once you have the driver for any reason being committed to other activities, for me it become a hindrance to the progress' (driver, SD1). Key to their success, in turn, was their ability to establish shared accountability in the MRU team as a 'co-ordinated, inclusive and functional structure in pursuit of positive clinical outcomes' across professional cadres and levels. This involved strategic calculations on who best to involve in collective processes: 'you found yourself mostly having community service medical officers, these are people that are leaving, or their contracts are 'at the] end of 12 months ... so you cannot reliably say this one will chair ... but your OPMs 'nurse operational managers] ... I know they can reliably report to me' (driver, SD1). Also important was being willing to challenge problematic professional hierarchies '. I can call and say doc, please respect this sister's call for this meeting because it is important' (driver, SD1).
Secondly, co-ordination and improved working relationships between PHC facilities and the district hospital - linking prevention, care and cure - were considered the 'breakthrough' to achieving outcomes: 'Before, the PHC, the hospital and the clinics we were working in parallel from each other, there was no communication, we were isolated from each other. So, when we are at the clinic we are at the clinic, we don't care about the patient; when we are at the hospital you manage what is coming in . Clearly that was not yielding any result . Until we started the 3 feet model, that's when we started to sit in the same boardroom with our PHCs. So, the bringing of the 2 teams together was a breakthrough for me' (driver, SD1).
Thirdly, as indicated earlier, the tools configured around the open tap analogy framework provided the 'actionable intelligence' to guide the actions of local actors, the 'real-time data to inform resource allocation at the local executive level . to set short-term wins for challenges from community to hospital levels' (driver, SD2). The tools were described as 'very, very effective especially for someone in my office, because they give you an overall view of the hospital within 30 minutes without even having to page 50 pages of a document' (driver, SD1).
Together, the elements of the model promoted a culture of learning and improvement where lessons were transferred to other conditions and 'every meeting is an opportunity to learn' (driver, SD2). Peer networking between subdistricts further enabled sharing of experiences and learning.
Finally, the implementation of the model and the associated innovations would not have been possible without the endorsement of district managers. During implementation there were strong nodes of support at this level, with senior district players convening meetings and mandating scale up to other subdistricts. As pointed out by a subdistrict driver, 'in terms of sustainability, it . needs someone at the top to be a pressure and oversight view . a district boost where it becomes as a compulsory meeting that is monitored by someone else' (driver, SD1).
Discussion
The 3 feet model is a subdistrict approach to improving quality and outcomes. Experiences in Waterberg District suggest that the core elements of the model have wide applicability, beyond the starting points in MNH, and can drive innovation. The model provides a meaningful theory of change, centred on local leadership, outcome-orientated decision-making and collective action, supported by tools that direct action. It takes a systems approach, emphasising connectedness and relationship building, and has similarities with an emerging evidence base on systems thinking,[18] networks of care[19] and learning health systems.[20] As such, the specific features and 3 feet model 'brand' are less important than its underlying mechanisms of change.
Central to achievements was the presence of stable and committed hybrid (clinical-managerial) leaders[21] in the three subdistricts, with sufficient authority to direct the actions of others, and an ability to overcome entrenched silos across levels, professions, managers and clinicians.[22] A key focus of the programme was in bolstering the confidence, skills and networks of these individual leaders. Equally important, however, was the way the three drivers forged shared/distributed leadership and teamwork. Such skilled subdistrict leadership is the exception rather than the norm in SA.[23] In the absence of ongoing processes of induction and renewal, a turnover in local leadership could very well threaten the survival of the 3 feet model. Effective leadership and management development programmes and plans are key to sustainable implementation of subdistrict innovations.
The 3 feet programme's engagement with district decision-makers, and the introduction of clinical information systems and CPD frameworks, sought to secure the support and systems for sustainability. To be anchored, such systems require appropriate provincial policies and procedures, attuned to quality and outcomes.
Study limitations
As indicated in the methodology, the 3 feet model was not established as a research intervention, and the evaluation, while systematic, deliberately remained relatively light, as a background element rather than central feature of implementation. The ability to draw causal inferences on the impact of the model, while a firm part of district narratives, is limited.
Conclusions
Although not advocating for a cut-and-paste approach to improving quality and outcomes, positive experiences in Waterberg District suggest that the principles and mechanisms of action of the 3 feet model have wider relevance for policy and practice. This is especially relevant as emphasis shifts towards the subdistrict as a core unit of population health and wellbeing in SA. Sustainable implementation and scale-up of such approaches requires not only induction and support in the methodologies of these innovations, but also appropriate accountabilities, support networks and systems development at district and provincial levels, embedded in enabling national policy.
Declaration. None.
Acknowledgements. The authors would like to acknowledge the participation of managers and staff of Waterberg District in the implementation and evaluation of the 3 feet model.
Author contributions. All authors contributed to the conduct of the evaluation. FM and HS designed the formal data collection component. HS drafted the manuscript and all authors commented on and approved the final manuscript.
Funding. HS and FM were funded by the SA Research Chairs Initiative of the Department of Science and Technology and National Research Foundation of SA (grant no. 98918), and the SA Medical Research Council. The 3 feet model support (JC, JW, YP) was funded by Elma Philanthropies through the Clinton Health Access Initiative. Any opinion, finding and conclusion or recommendation expressed in this material is that of the authors and not the funders.
Conflicts of interest. None.
References
1. South Africa. National Health Act No. 61 of 2003. [ Links ]
2. Tarimo E. Towards a health district: Organizing and managing district health systems based on primary health care. Geneva: World Health Organization, Division of Strengthening of Health Services, 1991. https://iris.who.int/handle/10665/40785 (accessed 22 September 2023). [ Links ]
3. South Africa. National Health Insurance Bill B-11, 2019. [ Links ]
4. South African Lancet National Commission. Confronting the right to ethical and accountable quality health care in South Africa: A consensus report. Pretoria: National Department of Health, 2019. https://bhekisisa.org/wp-content/uploads/2019/07/620a9eb9-final-sa-lnc-report.pdf (accessed 22 September 2023). [ Links ]
5. Prinsen L. Medicine and the law. S Afr Med J 2023;113(4):e134. https://doi.org/10.7196/SAMJ.2023.v113i4.134 [ Links ]
6. Schneider H, Mianda S. District and subdistrict stewardship of quality and health outcomes: Roles, systems and strategies (briefing document). Cape Town: University of the Western Cape, 2022. https://repository.uwc.ac.za/xmlui/handle/10566/7498 (accessed 22 September 2023). [ Links ]
7. Schneider H, George A, Mukinda F, Tabana H. District governance and improved maternal, neonatal and child health in South Africa: Pathways of change. Health Syst Reform 2020;6(1):1-12. https://doi.org/10.1080/23288604.2019.1669943 [ Links ]
8. Cupido J. Development of the 3 Feet Model: A Bottom-Up and System Wide Approach to Reducing Mortality and Morbidity. Cape Town: University of the Western Cape, 2021. [ Links ]
9. Wessels J, Cupido J. Health Systems Strengthening at the Sub-district Level: The Three Feet Model. An Implementation Guide. Johannesburg: Clinton Health Access Initiative, 2021. [ Links ]
10. Schneider H, McKenzie A, Tabana H, Mukinda F, George A. Evaluation of health system strengthening initiatives for improving the quality and outcomes of maternal, neonatal and child health care in four South African districts (report). Cape Town: School of Public Health, SAMRC Health Services to Systems Research Unit, University of the Western Cape, 2017. [ Links ]
11. Schneider H, van der Merwe M, Marutla B, Cupido J, Kauchali S. The whole is more than the sum of the parts: Establishing an enabling health system environment for reducing acute child malnutrition in a rural South African district. Health Policy Plan 2019;34(6):430-439. https://doi.org/10.1093/heapol/czz060 [ Links ]
12. Rothgang M, Lageman B. The unused potential of process tracing as evaluation approach: The case of cluster policy evaluation. Evaluation 2021;27(4):527-543. https://doi.org/10.1177/135638902110416 [ Links ]
13. Beach D, Pedersen R. Process-Tracing Methods: Foundations and Guidelines. Ann Arbor: University of Michigan Press, 2013. https://doi.org/10.3998/mpub.10072208 [ Links ]
14. Portela MC, Pronovost PJ, Woodcock T, Carter P, Dixon-Woods M. How to study improvement interventions: A brief overview of possible study types. BMJ Qual Saf 2015;24(5):325-336. https://doi.org/10.1136/bmjqs-2014-003620 [ Links ]
15. Barry D, Kimble LE, Nambiar B, et al. A framework for learning about improvement: Embedded implementation and evaluation design to optimise learning. Int J Qual Health Care 2018;30(suppl 1):S10-S14. https://doi.org/10.1093/intqhc/mzy008 [ Links ]
16. Mukinda FK, van Belle S, Schneider H. Local dynamics of collaboration for maternal, newborn and child health: A social network analysis of healthcare providers and their managers in Gert Sibande District, South Africa. Int J Health Policy Manag 2021:1-11. https://doi.org/10.34172/ijhpm.2021.106 [ Links ]
17. Kinney MV, George AS, Rhoda NR, Pattinson RC, Bergh AM. From pre-implementation to institutionalisation: Lessons from sustaining a perinatal audit program in South Africa. Glob Health Sci Pract 2023;11(2):e2200213. https://doi.org/10.9745/GHSP-D-22-00213 [ Links ]
18. Thelen J, Sant Fruchtman C, Bilal M, et al. Development of the Systems Thinking for Health Actions framework: A literature review and a case study. BMJ Glob Health 2023;8(3):e010191. https://doi.org/10.1136/bmjgh-2022-010191 [ Links ]
19. Carmone AE, Kalaris K, Leydon N, et al. Developing a common understanding of networks of care through a scoping study. Health Syst Reform 2020;6(2):e1810921. https://doi.org/10.1080/23288604.2020.1810921 [ Links ]
20. Sheikh K, Abimbola S. Learning health systems: Pathways to progress. Flagship report of the Alliance for Health Policy and Systems Research. Geneva: World Health Organization, 2021. https://ahpsr.who.int/publications/i/item/learning-health-systems-pathways-to-progress (accessed 22 September 2023). [ Links ]
21. McGivern G, Currie G, Ferlie E, Fitzgerald L, Waring J. Hybrid manager-professionals' identity work: The maintenance and hybridisation of medical professionalism in managerial contexts. Pub Admin 2015;93(2):412-432. https://doi.org/10.1111/padm.12119 [ Links ]
22. Nzinga J, McGivern G, English M. Examining clinical leadership in Kenyan public hospitals through the distributed leadership lens. Health Policy Plan 2018;33(suppl 2):ii27-ii34. https://doi.org/10.1093/heapol/czx167 [ Links ]
23. Engelbrecht B, Gilson L. Governance, leadership and management. In: Matsoso MP, Chikte U, Makubalo L, Pillay Y, Fryatt R, (eds). The South African Health Reforms 2015 - 2020. Johannesburg: Trackstar Trading, 2022:291-312. Accepted 9 October 2023. [ Links ]
 Correspondence:
Correspondence:
H Schneider
hschneider@uwc.ac.za
Accepted 9 October 2023


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}