










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 n.8 Pretoria Aug. 2023
http://dx.doi.org/10.7196/samj.2023.v113i8.428
IN PRACTICE
Potential drug-drug interactions with phentermine among long-term phentermine consumers: A retrospective analysis
A FourieI; M JulyanII; C S MostertIII; J M du PlessisIV
IBPharm; Medicine Usage in South Africa (MUSA), Faculty of Health Sciences, North-West University, Potchefstroom, South Africa
IIBPharm, PhD; Medicine Usage in South Africa (MUSA), Faculty of Health Sciences, North-West University, Potchefstroom, South Africa
IIIBPharm, MHPE; Medicine Usage in South Africa (MUSA), Faculty of Health Sciences, North-West University, Potchefstroom, South Africa
IVMB ChB, MPharm; Medicine Usage in South Africa (MUSA), Faculty of Health Sciences, North-West University, Potchefstroom, South Africa
ABSTRACT
BACKGROUND: Phentermine is an internationally recognised amphetamine derivative with significant appetite-suppressing properties. The drug is indicated for the short-term management of obesity, as the long-term (LT) use of phentermine may potentially be associated with severe cardiovascular side-effects, abuse and dependence. The LT use hereinafter describes periods exceeding 12 consecutive weeks. This use may also be associated with potential drug-drug interactions (PDDIs), which may result in adverse drug reactions (ADRs). The literature reports that phentermine is often prescribed LT and for several other off-label indications, increasing the risk for individuals to experience adverse drug events (ADEs) and drug-drug interactions (DDIs). There are, to our knowledge, no South African (SA) studies investigating the prevalence of co-prescribing LT phentermine with drugs that may potentially cause DDIs
OBJECTIVE: To determine the prevalence of mild, moderate and severe DDIs with phentermine use when the duration of therapy in private healthcare exceeded 12 consecutive weeks
METHODS: A cross-sectional drug utilisation review (DUR) was done by using data obtained from a SA pharmacy benefit management (PBM) company's database. Retrospective data of medicine claims for phentermine, from 1 January 2015 to 31 December 2019, were extracted for analysis. The number of days phentermine was supplied was used to identify the study population, in other words, those patients who received the drug LT. A drug interaction checker (Drugs.com) was used to identify potential mild, moderate and severe DDIs when using phentermine and co-prescribed drugs concurrently
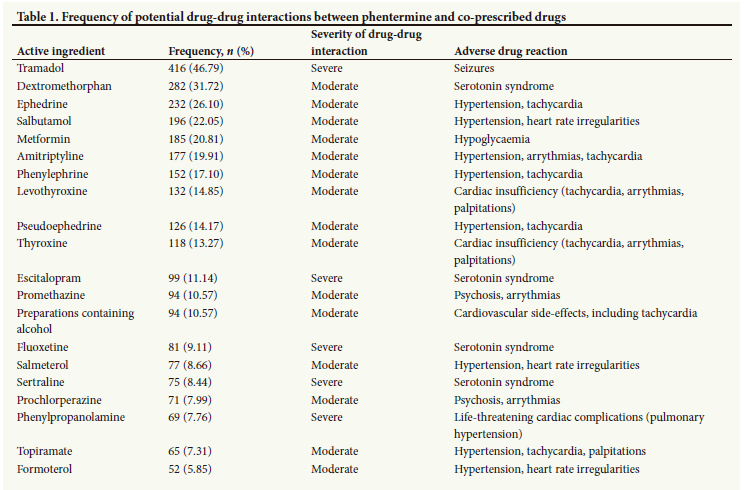
RESULTS: A total of 889 patients received phentermine LT. The top 20 drugs identified as being frequently co-prescribed in this study population demonstrated no mild PDDI, 15 (75%) moderate PDDIs and 5 (25%) severe PDDIs. The most common co-prescribed drug in the moderate group was dextromethorphan (n=282, 31.72%) and the least co-prescribed was formoterol (n=52, 5.85%). Among the drug group 'severe PDDIs', tramadol (n=416, 46.79%) was most frequently prescribed, whereas phenylpropanolamine (n=69, 7.76%) was the least prescribed to patients in this group
CONCLUSION: There are patients who receive LT phentermine therapy despite the potential severe consequences that may result. These patients may receive concomitant therapy with phentermine and other pharmaceutical constituents, which may potentially cause DDIs, more specifically, moderate and severe DDIs. As such, these patients are not only confronted with the consequences of DDIs but are also at risk to experience ADRs as the residual effect of PDDIs
Phentermine, an extraordinary amphetamine derivate, is South Africa (SA)'s most popular prescription-only anti-obesity medication used for its appetite-suppressing properties.[1-3] The drug stimulates the central nervous system (CNS), inhibiting the reuptake and stimulating the release of endogenous neurotransmitters, including dopamine (DA), serotonin (5-HT) and norepinephrine (NE).[4-6] Consequently, there is an increase in the concentration of these neurotransmitters in the CNS and stimulatory effects.[4,5] In the brain, the increased DA concentration will provide a constant DA-induced feeling/sensation of reward (associated with eating), which will result in appetite suppression.[5,7] Persistent 5-HT neurotransmission in the brain may also result in appetite suppression; however, these effects are only achieved at doses higher than the recommended maximum daily dosage, that is >30 mg phentermine.[8,9] Once NE is released, the hormone cascade of the hypothalamus-pituitary axis (HPA) is activated via the amygdala of the brain.[10-12] Signals are transmitted from the amygdala to the hypothalamus, then to the pituitary gland, and finally to the adrenal cortex, positioned on top of the kidneys.[12,13] As a result, DA, NE and epinephrine are released into the bloodstream, where they will bind to adrenergic receptors (a and p receptors) of fat tissue and smooth muscles.[13,14]
The stimulatory effects of DA and NE will enhance the breakdown of fat tissue, consequently resulting in weight loss.[14-16] Epinephrine will result in increased blood glucose concentrations: the individual will feel satiated, and the appetite is suppressed.[10,15,16] Unfortunately, the effects of these catecholamines are not limited to the abovementioned desired effects, as these hormones bind to multiple adrenergic receptors located throughout the body.[17] As such, an individual may experience some undesired effects, also known as side-effects.[17,18] The most common side-effects of phentermine are dry mouth and insomnia,[19,20] as phentermine is generally used short-term (ST),[2,21] in other words not longer than 12 consecutive weeks.[22] It is recommended that phentermine not be used for longer than 12 consecutive weeks (hereinafter referred to as long-term (LT)), as LT use (off-label indication for the drug) may be associated with severe cardiovascular side-effects, abuse and dependence.[23,24] The increase in the blood concentration of DA and NE will also increase the stimulatory effects of the heart,[15,16,25,26] kidneys[15,16] and blood vessels,[25,26] which may result in heart rate irregularities (tachycardia, arrythmias and palpitations) and hypertension.[23,27-31] The increase in the stimulatory effects of the CNS may also result in drug abuse, dependence[23,28] and seizures,[23] or trigger DA-induced hallucinations or episodes of psychosis.[16-23] The LT use of phentermine may, theoretically, cause significant harm to patients; the US Food and Drug Administration (FDA) therefore restricted the duration of this medicine's use to ST use.[3,23]
The LT use of phentermine is permitted, provided the drug is administered as the FDA-approved, fixed-dose combination phentermine/topiramate.[32] This is also the only instance in which phentermine may be combined with other pharmaceutical preparations for the treatment of obesity.[32,33] The success of this drug combination can be attributed to a moderate drug-drug interaction (DDI) between phentermine and topiramate.[28] Moderate DDIs are classified as such, since they may cause distinctively stressful or intolerable adverse drug reactions (ADRs) in individuals.[34 Topiramate is an anti-epileptic that can, in its own capacity, induce weight loss, and if administered together with phentermine, increase the plasma concentration thereof and thus also the efficacy.[28,33,35] However, as it increases the plasma concentration of phentermine, it may also increase the adverse effects thereof, such as tachycardia, increased blood pressure levels and palpitations.[35] Evidently, no matter how successful this combination may be, there are risks associated with it that may potentially be harmful to individuals. This drug combination is not available in SA.
Not all DDIs are as beneficial as the use of phentermine/ topiramate, and some may, depending on the severity, cause significant harm to individuals.[36] Consequently, not only is the LT use of phentermine not recommended, but also the simultaneous use of phentermine with drugs that may potentially cause mild, moderate or severe DDIs.[23,35] The patient information leaflet (PIL) of the drug warns against the simultaneous use of phentermine with other pharmaceutical preparations, including sympathomimetics, selective serotonin reuptake inhibitors (SSRIs), oral hypoglycaemic preparations and antihypertensive and epileptogenic agents, as the simultaneous use thereof may result in DDIs and thus ADRs.[23,35] Unfortunately, it is not uncommon for phentermine to be administered concurrently with preparations intended to lower blood glucose and blood pressure levels, as the drug is indicated for the treatment of obesity, which is commonly associated with diabetes and/or cardiovascular diseases such as hypertension.[23,37] Additionally, it is likely for phentermine to be used LT and in combination with pharmaceutical preparations that may cause DDIs.[24] There is, to our knowledge, no SA study investigating the prevalence of potential drug-drug interactions (PDDIs) among patients receiving LT therapy with phentermine. The objective of this study was therefore to determine the prevalence of potentially mild, moderate and severe DDIs with phentermine when the duration of therapy (DOT) in the private healthcare sector of SA exceeded 12 consecutive weeks.
Methods
Study design
A descriptive, retrospective, quantitative drug utilisation review (DUR) study design was used, making use of longitudinal patient medicine claims data from a SA pharmacy benefit management (PBM) company's database.
Study setting and data source
The study was conducted in the private healthcare sector of SA, using approved and paid medicine claims data for phentermine from 1 January 2015 to 31 December 2019. The data comprised dispensing information from all SA pharmacies across all provinces in SA, as the PBM is linked to all pharmacies in SA and 98% of dispensing practitioners. The data fields from all patient records used included the date the prescription was issued, the number of days the drug was provided for, the information on the dispensed product (including the active ingredient), the National Pharmaceutical Product Index (NAPPI) code, and the gender and age of the patient. Each patient medication record was assigned a random number to mask the identity of the patient.
Study population
The study population comprised all patients on the PBM company's database who received phentermine LT from 1 January 2015 to 31 December 2019. A grace period of 5 days was given for early/late collection of prescriptions. Data comprising the NAPPI codes 721786006 (15 mg phentermine) and 721794-009 (30 mg phentermine) were analysed. Information on gender and age was used to interpret the demographic results of patients receiving LT therapy with phentermine. Based on their gender, patients were considered either female or male.
Data analysis
The data were analysed by the director of Medicine Usage in South Africa (MUSA), Faculty of Health Sciences at the NorthWest University (NWU), Potchefstroom, SA. Descriptive statistics were used to explain and interpret the data spread, and included frequencies and percentages. The frequency and percentage were used to numerise the demographic information of those patients receiving phentermine LT. A list of drugs co-prescribed to patients receiving phentermine LT was also extracted for analysis. A drug interaction checker from Drugs.com was used to identify the drugs that may potentially cause a mild, moderate or severe DDI when co-prescribed with phentermine.[36] Mild DDIs are those interactions that may cause some discomfort in individuals, but do not require change in therapy and are of little clinical significance.[34,381 Moderate DDIs, however, may cause distress, are of moderate clinical significance and usually require change in therapy.[34,38] Severe DDIs may have life-threatening repercussions and are therefore of major clinical significance and require change in therapy.[34,38] The top 20 drugs that may cause PDDIs and are most frequently prescribed to patients receiving phentermine LT were listed accordingly. The potential ADRs that may occur between such DDIs were also listed.
Ethics
Through a contractual agreement, the PBM company's board of directors has consented to the research entity MUSA accessing and using their database if the data are intended for research purposes. As such, the researchers were permitted, through the PBM company's consent, to use the company's data for this study. A confidentiality agreement was signed by the researchers involved and the director of MUSA prior to gaining access to the database. The PBM company's name was therefore not disclosed throughout the study in order to ensure that confidentiality and anonymity are maintained. All patient records were de-identified, that is, any personal information of the patients, medical schemes or prescribers was depersonalised prior to the researchers accessing the database. Each patient record was therefore assigned a random 'dummy' member number; this ensured that confidentiality and anonymity were maintained throughout the study. The Health Research Ethics Committee of the Faculty of Health Sciences of the NWU, Potchefstroom campus, granted ethical approval to conduct the study (ref. no. NWU-00179-14-A1-11).
Results
The study population consisted of 889 patients on the medicine claims database who received LT therapy with phentermine during the study period. Of these patients, most were female (775, 87.18%) and aged 35 - 59 years (n=602, 67.72%). The top 20 drugs that were most commonly co-prescribed with phentermine, which may potentially have caused a DDI among these LT phentermine consumers, are summarised in Table 1. The drugs are listed in descending order according to the number of people who received the respective co-prescribed drugs. The table also gives the ADRs that may have resulted from a PDDI between phentermine and the relevant co-prescribed drugs.
As seen from the results in Table 1, there were 15 (75%) drugs that may potentially have caused a moderate DDI with phentermine. The remainder of the drugs (n=5, 25%) may potentially have caused a severe DDI.
Prevalence of potential DDIs with phentermine among patients receiving the drug LT
The data were analysed to determine the prevalence of co-prescribing of phentermine with drugs that may potentially cause mild, moderate and severe DDIs among patients receiving phentermine LT.
Prevalence of potentially mild DDI
According to the data, there were no PDDIs that were mild to severe among the patients receiving phentermine LT.
Prevalence of potentially moderate DDIs
Results indicated that dextromethorphan (n=282, 31.72%) was the drug most frequently prescribed to patients receiving phentermine LT that may potentially have caused moderate DDIs. Thereafter, ephedrine (n=232, 26.10%) was most frequently prescribed, followed by salbutamol (n=196, 22.05%) and metformin (n=185, 20.81%). The drug that was least prescribed to patients in this group was formoterol (n=52, 5.85%). Other drugs co-prescribed with phentermine that may potentially have caused moderate DDIs are given in Table 1.
Prevalence of potentially severe DDIs
The most common drug prescribed together with phentermine was tramadol, which means that 46.79% (n=416) of patients receiving phentermine LT potentially experienced severe DDIs with tramadol. The second drug was escitalopram (n=99, 11.14%), followed by fluoxetine (n=81, 9.11%) and sertraline (n=75, 8.44%). Phenylpropanolamine was the drug least prescribed to patients (n=69, 7.76%) in this category.
Discussion
This is the first SA study to investigate the prevalence of PDDIs with phentermine when the recommended DOT exceeded 12 consecutive weeks. The study revealed that a total of 889 patients from the private healthcare sector in SA received phentermine LT. In other words, from 1 January 2015 to 31 December 2019, there were 889 patients on the database who received phentermine LT despite this use not being recommended.[23] The LT use of phentermine is not advised, since there are no data supporting its use and it may potentially be associated with severe cardiovascular side-effects (including tachycardia and hypertension), abuse and dependence.[19-24] DDIs may also occur among patients who receive the drug LT, thereby increasing the risk for ADRs to occur.[24]
Analysis of the top 20 drugs that were co-prescribed with phentermine and may potentially have caused a DDI indicates that these drugs may potentially have caused moderate and severe DDIs. There were no drugs co-prescribed with phentermine that may potentially have caused mild DDIs (e.g. evening primrose oil). It may therefore be deduced that patients receiving LT therapy with phentermine may potentially have experienced moderate and severe DDIs.
The drugs co-prescribed with phentermine that may possibly have caused moderate DDIs are listed in Table 1. There were 282 (31.72%) patients who received phentermine together with the opium
alkaloid[3] dextromethorphan, which is used as a cough suppressant and is a weak 5-HT reuptake inhibitor.[3,35] As previously discussed, phentermine may also increase 5-HT concentration in the CNS.[8,9] Therefore, if administered together, phentermine may potentiate the effects of dextromethorphan, thereby potentially causing a moderate DDI.[35] Consequently, excessive nerve cell activity and life-threatening symptoms (e.g. high blood pressure and temperature) may surface, a condition also known as serotonin syndrome (5-HT syndrome).[6,8,19,39,40] As such, patients receiving LT therapy with phentermine may potentially have experienced 5-HT syndrome as the residual effect of a moderate DDI between phentermine and dextromethorphan.
Phentermine may potentially cause a moderate DDI with ephedrine, pseudoephedrine and phenylephrine as well. Pseudoephedrine and phenylephrine are used as systemic decongestants, whereas ephedrine is used as a pressor agent for low blood pressure (hypotension).[3] These agents, as with phentermine, stimulate adrenergic receptors in the body and, if administered together, phentermine can potentiate the adrenergic response to these agents.[3,35] As such, these drugs will add to the stimulatory effects of the heart, kidneys and blood vessels, which will further increase the blood pressure levels and heart rate.[35] Patients may therefore experience hypertension and tachycardia (increased heart rate) as the result of PDDIs between phentermine and these agents.'351 Phentermine may also potentiate the adrenergic response to salbutamol, salmeterol and formoterol. These agents also stimulate adrenergic receptors, and are indicated for the treatment of asthma and chronic obstructive pulmonary disease.[3] Therefore, patients who received phentermine together with salbutamol (n=196, 22.05%), salmeterol (n=77, 8.66%), or formoterol (n=52, 5.85%) may potentially have experienced hypertension and/or heart rate irregularities.[15]
Approximately 21% of patients who received phentermine LT also received metformin, a biguanide designed to lower the blood glucose levels.[3] Metformin is indicated for the treatment of obesity among diabetic individuals, as it provokes mild anorexia and therefore assists in controlling weight gain.[3] As previously discussed, phentermine increases the concentration of NE in the bloodstream and consequently also the blood glucose levels.[14,26] As such, these constituents oppose each other's mechanism of action, thereby potentially causing a moderate DDI. However, this is not the mechanism through which the ADR hypoglycaemia occurs.[35] Phentermine initially causes an increase in blood glucose levels, resulting in appetite suppression and consequently also weight loss.[14,15,26] Weight loss may have an impact on glycaemic control, as it lowers blood glucose levels.[35] Therefore, since metformin and phentermine lower the blood glucose levels and the last-mentioned medicine causes weight loss, administering these drugs together may have additive effects that may potentially result in hypoglycaemia.[14] In this instance, hypoglycaemia may commonly present with adrenergic neurogenic signs and symptoms such as anxiety, tremors and palpitations.[41]
Moreover, the use of phentermine together with amitriptyline, a tricyclic antidepressant, may cause moderate DDIs that may potentially result in hypertension, arrythmias and/or tachycardia.[3,35] Amitriptyline is indicated for the management of depressive disorders and the drug acts by inhibiting the reuptake of NE.[3,35] Consequently, administering phentermine together with this pharmaceutical constituent may further increase the concentration and stimulatory effects of NE, because phentermine (as previously discussed) also increases NE concentration.[9,35,42] Therefore, patients who received these two agents simultaneously (n=177, 19.91%) may potentially have experienced the abovementioned ADRs as the residual effect of potentially moderate DDIs.
The thyroid hormones, levothyroxine and thyroxine, are indicated for hypothyroidism, a medical disease in which the thyroid hormone produces insufficient amounts of the hormone thyroxine.[3,43] The thyroid gland co-operates with the adrenal glands to release NE into the bloodstream in order to ensure that the body's metabolism works sufficiently.[44,45] Administration of these thyroid hormones will stimulate the adrenal gland to release NE into the bloodstream, and administering phentermine together with these hormones will have additive effects.[46] The net result will be excessive concentrations of NE in the bloodstream, which may potentially result in cardiovascular side-effects such as tachycardia, arrythmias and palpitations.[46] Phentermine may also cause a moderate DDI with preparations containing alcohol, as alcohol potentiates the CNS and cardiovascular effects of phentermine.[35]
There were 94 (10.57%) and 71 (7.99%) patients receiving phenter-mine together with promethazine and prochlorperazine, respectively. These pharmaceutical agents are indicated, among other indications, for the treatment of nausea and vomiting.[3,35] Promethazine and prochlorperazine supposedly oppose the dopaminergic activity of phentermine, which may reduce the weight-reducing properties of the drug.[35] Phentermine is expected to reduce the neuroleptic efficacy and potentiate the arrhythmogenicity of these agents, which may cause psychosis and arrythmias, respectively.[35] Additionally, phentermine may also exacerbate pre-existing symptoms of psychosis.'351 As such, the mechanism of the PDDI is based on the fact that these agents may oppose the pharmacological effects of phentermine, and vice versa.
Lastly, 65 (7.31%) patients received phentermine together with the anti-epileptic topiramate, and may therefore have experienced moderate DDIs. The combination phentermine/topiramate was approved by the FDA in 2012 for the LT management of obesity, as these constituents have proven to cause significantly more weight loss when combined than when each agent is used individually as monotherapy.[32,47,48] The precise mechanism of interaction between phentermine and topiramate has not been determined yet; however, it is known that topiramate increases the plasma concentration of phentermine and therefore also its efficacy.[14] It is also known that weight loss is a common side-effect of topiramate, thereby adding to phentermine's weight-reducing effects if the two are administered simultaneously.[32] Individuals may also experience more intense adverse effects caused by the increased plasma concentration of phentermine, for example tachycardia, increased blood pressure levels and palpitations.[35] Nevertheless, the FDA has approved this drug combination as it has been proven to be safe and effective.[48] Regrettably, this combination is not available in SA yet.[33]
Furthermore, patients receiving LT therapy with phentermine also received drugs that may potentially have caused severe DDIs with phentermine (Table 1). Approximately 50% (n=416, 46.79%) of patients in the study population potentially experienced severe DDIs with phentermine and tramadol. Tramadol is indicated for the management of moderate and severe pain, and acts by inhibiting the reuptake of 5-HT.[3] The use of phentermine and tramadol is not recommended, since phentermine can lower the threshold for convulsions and tramadol may sometimes cause seizures.[33,35] The combination of these epileptogenic agents may have additive effects, potentially causing a medical emergency and causing significant harm to an individual.[28,51]
The PIL of phentermine warns explicitly against the simultaneous use of the drug with SSRIs, as these drugs inhibit serotonin metabolism and may be associated with cardiac valvular disease.[23] The drugs are mainly indicated for depressive disorders,[3] and there were 99 (11.14%), 81 (9.11%) and 75 (8.44%) patients receiving phentermine together with escitalopram, fluoxetine and sertraline, respectively. The combination of phentermine with SSRIs may result in 5-HT syndrome and should be avoided, given its severity.[35,40]
As seen from Table 1, the simultaneous use of phentermine with phenylpropanolamine may also result in life-threatening complications.[28,35] In a case-control epidemiological study, the use of anorexigenic agents such as phenylpropanolamine and phentermine may be correlated with a greater risk for pulmonary hypertension.[35] Therefore, if these agents were to be used simultaneously, their combined effects on the cardiovascular system may cause life-threatening cardiac complications.[35,52] Evidently, given the severity of the potential ADRs that may result from these PDDIs, such interactions require instant medical attention and a change in therapeutical regimens.[38]
Study limitations
The present study is not without limitations. Firstly, it only included approved and paid claims for phentermine and excluded cash paid claims; therefore, the actual number of patients in the study population could not be accurate. Secondly, the total number of patients receiving phentermine LT could potentially be miscalculated, since the analysis of the duration of use was limited to the study period and the number of patients in the database. The abovementioned is also applicable to the prevalence of PDDIs with phentermine. Only one drug interaction checker was used to identify drugs that may potentially cause DDIs with phentermine; therefore, other PDDIs could possibly exist. The study investigated the prevalence of PDDIs and it could therefore not be known for sure if the patients actually experienced a DDI. Furthermore, the data reflected the dispensing information of phentermine; the actual consumption patterns of the drug could not be known for sure, as there was no evidence that these patients in fact consumed the phentermine. Lastly, the analyses were done with the understanding that the data obtained from the PBM company's database were precise and reliable.
Conclusion
Phentermine is the most frequently used anorexigenic appetite suppressant in SA, and the drug's popularity can be owed to its judicious use.[19,21,22] The DOT with the drug was restricted in 1977 to ST use only, as there were concerns that the LT use of phentermine may be associated with severe cardiovascular side-effects.[49,53] To this day, the DOT with phentermine remains restricted to periods not surpassing 12 consecutive weeks, as no evidence has been provided to support the safety and effectiveness of LT therapy.[49,53] Nonetheless, the results from this study indicate that prescribers in the private healthcare sector of SA prescribe phentermine off-label LT despite the potentially severe consequences. The results also indicate that these prescribers combine LT therapy with phentermine with other drugs such as SSRIs, despite the PIL advising against this.[23] The PIL of phentermine specifically warns against such a drug combination, as these drugs may have harmful interactions that may cause PDDIs and ADRs.[23,50] It is evident from the study results that the patients who received LT therapy with phentermine were also at risk to experience other potentially moderate and severe DDIs, and as one can see from Table 1, the potential ADRs that may have occurred from these PDDIs seem rather severe. This raises the following concern: why would prescribers put their patients at risk of potentially experiencing such ADEs? It also raises the question of whether a proper benefit-to-risk analysis was done prior to initiating pharmacotherapy with phentermine. These aspects deserve further investigation.
To conclude, patients receiving LT therapy with phentermine in the private healthcare sector of SA are at risk of experiencing moderate to severe DDIs. The ADRs that may occur from these PDDIs are rather serious, and may be harmful to the patients involved. Prescribers should be more vigilant in the co-prescribing of phentermine with other drugs that may potentially cause DDIs. These prescribers should also be made aware of the label indications of phentermine, as they are provided to assist in the rational and safe prescribing of the drug so that DDIs and ADRs can be prevented.
Declaration. This publication forms part of the partial completion of the requirements for AF's Master of Pharmacy degree.
Acknowledgements. We thank Prof. Martie Lubbe for the data analysis.
Author contributions. AF: first author (drafting and editing of the manuscript), conducting the research and data interpretation; MJ: assessment and review of the manuscript; CM: assessment and review of the manuscript; JMDP: corresponding author, reviewing the manuscript and expert opinion.
Funding. None.
Conflict of interest. None.
References
1. Truter I. Prescription appetite suppressants: A drug utilisation study using a claims database. J Pharm Sci 2014;4(8):32-35. https://doi.org/10.7324/japs.2014.40806 [ Links ]
2. Truter I. Dispensing patterns of prescription-only antiobesity preparations in South Africa. S Afr J Clin Nutr 2016;29(4):139-144. https://doi.org/10.1080/16070658.2016.1217643 [ Links ]
3. Rossiter DP. South African Medicines Formulary. 12th edition. Pretoria: SAMF, 2016:70-71. [ Links ]
4. Marais A. The pharmacological management of obesity. S Afr Fam Pract 2018;58(4):16-21. https://doi.org/10.4102/safp.v58i4.4510 [ Links ]
5. Kalyanasundar B, Perez CI, Luna A, et al. The appetite suppressant D-norpseudoephedrine (cathine) acts via D1/D2-like dopamine receptors in the nucleus accumbens shell. Front Neurosci 2020;14(572328):1-16. https://doi.org/10.3389/fnins.2020.572328 [ Links ]
6. Sanchez-Ramos J. Neurologic complications of psychomotor stimulant abuse. Int Rev Neorobiol 2015;120(2015):131-160. https://doi.org/10.1016/bs.irn.2015.02.003 [ Links ]
7. Rege S. The dopamine hypothesis of schizophrenia - advances in neurobiology and clinical application. Psych Scene Hub, 2018. https://psychscenehub.com/psychinsights/the-dopamine-hypothesis-of-schizophrenia/ (accessed 14 May 2022). [ Links ]
8. Perez CI, Kalyanasundar B, Moreno MG, et al. The triple combination phentermine plus 5-htp/ carbidopa leads to greater weight loss, with fewer psychomotor side-effects than each drug alone. Front Pharmacol 2019;10:1327. [ Links ]
9. Rothman RB, Baumann MH. Neurochemical mechanisms of phentermine and fenfluramine: Therapeutic and adverse effects. Drug Devel Res 2000;51(2):52-65. https://doi.org/10.1002/1098-2299%28200010%2951%3A2%3C52%3A%3AAID-DDR2%3E3.0.CO%3B2-H [ Links ]
10. Volkow ND, Wang G, Baler RD. Reward, dopamine and the control of food intake: Implications for obesity. Trens Cogn Sci 2011;15(1):37-46. https://doi.org/10.1016/j.tics.2010.11.001 [ Links ]
11. McCorry LK. Physiology of the autonomic nervous system. Am J Pharm Educ 2007;71(4):1-11. https://doi.org/10.5688/aj710478 [ Links ]
12. Sheng JA, Bales NJ, Myers SA, et al. The hypothalamic-pituitary-adrenal axis: Development, programming actions of hormones, and maternal-fetal interactions. Front Behav Neurosci 2021;14(601939):1-21. https://doi.org/10.3389/fnbeh.2020.601939 [ Links ]
13. Dutt M, Wehrle CJ, Jialal I. Physiology, adrenal gland. StatPearls, 2021. https://www.ncbi.nlm.nih.gov/books/NBK537260/ (accessed 22 July 2022). [ Links ]
14. Paravati S, Rosani A, Warrington SJ. Physiology, catecholamines. StatPearls, 2020. https://www.ncbi.nlm.nih.gov/books/NBK507716/ (accessed 23 April 2022). [ Links ]
15. Alhayek S, Preuss CV. Beta 1 receptors. StatPearls, 2022. https://www.ncbi.nlm.nih.gov/books/NBK532904/ (accessed 23 April 2022). [ Links ]
16. Bathia A, Lenchner JR, Saadabadi A. Biochemistry, dopamine receptors. StatPearls, 2020. https://www.ncbi.nlm.nih.gov/books/NBK538242/ (accessed 8 July 2022). [ Links ]
17. Farzam K, Kidron A, Lakhkar AD. Adrenergic drugs. StatPearls, 2021. https://www.ncbi.nlm.nih.gov/books/NBK534230/ (accessed 16 August 2022). [ Links ]
18. Law J, Martin E. Concise Medical Dictionary. 10th edition. Oxford: Oxford University Press, 2020. https://www-oxfordreference-com.nwulib.nwu.ac.za/view/10.1093/acref/9780198836612.001.0001/acref-9780198836612-e-9254?rskey=RuBbkp&result=10652 (accessed 13 January 2022). [ Links ]
19. WebMD. Phentermine HCL - uses, side-effects, and more. New York: WebMD, 2021. https://www.webmd.com/drugs/2/drug-4151/phentermine-oral/details (accessed 12 May 2022). [ Links ]
20. Trantrachoti P, Klomjit S, Rassameehiran S, et al. Supraventricular tachycardia associated with phentermine use. S West Respir Crit Care Chron 2016;4(15):70-74. https://doi.org/10.12746swrccc2016.0415.206 [ Links ]
21. Kim KK, Cho H, Kang H, et al. Effects on weight reduction and safety of short-term phentermine administration in Korean obese people. Yonsei Med J 2006;47(5):614-625. https://doi.org/10.3349/ymj.2006.47.5.614 [ Links ]
22. Hampp C, Kang EM, Borders-Hemphill V. Use of prescription anti-obesity drugs in the United States. Pharmacotherapy 2013;33(12):1299-1307. https://doi.org/10.1002/phar.1342 [ Links ]
23. iNova Pharmaceuticals Pty Ltd. Duromine. Package insert. Bedfordview: iNova Pharmaceuticals, 2000. [ Links ]
24. Kokkinos J, Levin SR. Possible association of ischemic stroke with phentermine. Stroke 1993;24(2):310-313. https://doi.org/10.1161/01STR.24.2.310 [ Links ]
25. Hussain LS, Reddy V, Maani CV. Physiology, noradrenergic synapse. StatPearls, 2021. https://www.ncbi.nlm.nih.gov/books/NBK540977/ (accessed 26 June 2022). [ Links ]
26. Alshak MN, Das JM. Neuroanatomy, sympathetic nervous system. StatPearls, 2020. https://www.ncbi.nlm.nih.gov/books/NBK542195/ (accessed 23 April 2022). [ Links ]
27. AMBOSS. Sympathomimetic drugs. AMBOSS, 2020. https://www.amboss.com/us/knowledge/Sympathomimeticdrugs (accessed 1 September 2020). [ Links ]
28. Drugs.com. Phentermine disease interactions. Drugs.com, 2020. https://www.drugs.com/disease-interactions/phentermine.html#seizure_disorders (accessed 3 May 2022). [ Links ]
29. Goyal A, Robinson KJ, Sanchack KE. Palpitations. StatPearls, 2020. https://www.ncbi.nlm.nih.gov/books/NBK436016/ (accessed 14 August 2022). [ Links ]
30. Hermiz C, Sedhai YR. Angina. StatPearls, 2020. https://www.ncbi.nlm.nih.gov/books/NBK557672/ (accessed 16 September 2022). [ Links ]
31. Ojha N, Dhamoon AS. Myocardial infarction. StatPearls, 2022. https://www.ncbi.nlm.nih.gov/books/NBK537076/ (accessed 18 May 2022). [ Links ]
32. Aronne LJ, Wadden TA, Peterson C, et al Evaluation of phentermine and topiramate versus phentermine/ topiramate extended-release in obese adults. Obesity 2013;21(11):2163-2171. https://doi.org/10.1002/oby.20584 [ Links ]
33. Wilding JPH. Combination therapy for obesity. J Psychopharmacol 2017;31(11):1503-1508. https://doi.org/10.1177/0269881117737401 [ Links ]
34. Marsh DES. Severity of adverse drug reactions. Merck Manual, 2018. https://www.merckmanuals.com/home/drugs/adverse-drug-reactions/severity-of-adverse-drug-reactions (accessed 4 May 2022). [ Links ]
35. Drugs.com. 2021a. Drug Interactions Checker (Version 2.12.1) Mobile application. [ Links ]
36. Hendricks J. Pharmacotherapy. In: Steelman GM, Westman EC, eds. Obesity Evaluation and Treatment Essentials. London: CRC Press, 2016:137-167. [ Links ]
37. Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism 2019;92:6-10. https://doi.org/10.1016/j.metabol2018.09.005 [ Links ]
38. Shahabudin S, Bharti C, Faizal P. Surveillance of potential drug-drug interactions in the medicine department of a tertiary care hospital. JCDR 2012;6(7):1258-1261. https://www.jcdr.net/articles/PDF/2424/35%20-%204118_U.pdf (accessed 3 May 2022). [ Links ]
39. Maffei ME. 5-Hydroxytryptophan (5-HTP): Natural occurrence, analysis, biosynthesis, biotechnology, physiology and toxicology. Int J Mol Sci 2021;22(1):1-25. https://doi.org/10.3390/ijms22010181 [ Links ]
40. Simon LV, Keenaghan M. Serotonin syndrome. StatPearls, 2021. https://www.ncbi.nlm.nih.gov/books/NBK482377/ (accessed 3 May 2022). [ Links ]
41. Mathew P, Thoppil D. Hypoglycaemia. StatPearls, 2022. https://www.ncbi.nlm.nih.gov/books/NBK534841/ (accessed 10 May 2022). [ Links ]
42. Aggarwal S, Mortensen O. Overview of monoamine transporters. Curr Protoc Pharmacol 2017;79:12.16.1-12.16.17. https://doi.org/10.1002/cpph.32 [ Links ]
43. Patil N, Rehman A, Jialal I. Hypothyroidism. StatPearls, 2022. https://www.ncbi.nlm.nih.gov/books/NBK519536/ (accessed 10 May 2022). [ Links ]
44. Duttt M, Wehrle CJ, Jialal I. Physiology, adrenal gland. StatPearls, 2021. https://www.ncbi.nlm.nih.gov/books/NBK537260 (accessed 10 May 2022). [ Links ]
45. Teixeira P, dos Santos P, Pazos-Moura CC. The role of thyroid hormone in metabolism and metabolic syndrome. Ther Adv Endocrinol Metab 2020;11:1-33. https://doi.org/10.1177/2042018820917869 [ Links ]
46. Mayo Clinic. Hyperthyroidism (overactive thyroid). Mayo Clinic, 2020. https://www.mayoclinic.org/diseases-conditions/hyperthyroidism/symptoms-causes/syc-20373659 (accessed 10 May 2022). [ Links ]
47. Lewis KH, Fischer H, Ard J, et al. Safety and effectiveness of longer-term phentermine use: Clinical outcomes from an electronic health record cohort. Obesity 2019;27(4):591-602. https://doi.org/10.1002/oby.22430 [ Links ]
48. Lei X, Ruan G, Lai C, et al. Efficacy and safety of phentermine/topiramate in adults with overweight or obesity: A systematic review and meta-analysis. Obesity 2021;29(6):985-994. https://doi.org/10.1002/oby.23152 [ Links ]
49. Haslam D. Weight managements in obesity: Past and present. Int J Clin Pract 2016;70(3):206-217. https://doi.org/10.111/ijcp.12771 [ Links ]
50. Alomar MJ. Factors affecting the development of adverse drug reactions. Saudi Phar J 2013;22(2):83-94. https://doi.org/10.1016/j.jsps.2013.02.003 [ Links ]
51. Mayo Clinic. Seizures. Mayo Clinic, 2021. https://www.mayoclinic.org/diseases-conditions/seizure/symptoms-causes/syc-20365711 (accessed 3 May 2022). [ Links ]
52. Vilar S, Friedman C, Hripcsak G. Detection of drug-drug interactions through data mining studies using clinical sources, scientific literature and social media. Brief Bioinformat 2018;19(5):863-877. https://doi.org/10.1093/bib/bbx010 [ Links ]
53. Hendricks EJ. Off-label drugs for weight management. Diabetes Metab Syndr Obes 2017;10:223-234. https://doi.org/10.2147/dmso.s95299 [ Links ]
 Correspondence:
Correspondence:
J M du Plessis
jesslee.duplessis@nwu.ac.za
Accepted 25 April 2023


{kind=link}