










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 no.5 Pretoria may. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i5.16791
RESEARCH
Prevalence of secondary health conditions and mental status in persons with long-term spinal cord injury in South Africa: Comparison between public and private healthcare sectors
C JosephI; C ThurstonII; E NizeyimanaI; E ScribaIII; DM ConradssonI, IV, VI; A RhodaV
IMSc; PhD; Department of Health and Rehabilitation Sciences, Division of Physiotherapy, Stellenbosch University, Cape Town, South Africa
IIMSc; Department of Neurobiology, Care Sciences and Society, Division of Physiotherapy, Karolinska Institutet, Sweden
IIIMBChB; Spescare Medical Facility, Stellenbosch, Cape Town
IVMSc; PhD; Women's Health and Allied Health Professionals Theme, Medical Unit Occupational Therapy and Physiotherapy, Karolinska University Hospital, Stockholm, Sweden
VMSc; PhD; Deanery, Faculty of Community and Health Sciences, University of the Western Cape, Cape Town, South Africa
VIMSc; PhD; Department of Neurobiology, Care Sciences and Society, Division of Physiotherapy, Karolinska Institutet, Sweden
ABSTRACT
BACKGROUND: Spinal cord injuries typically result in a range of negative health outcomes and health states, which impacts overall functioning, health and well-being. It remains important to establish the prevalence (burden) of health outcomes to help with the development of optimal treatment strategies
OBJECTIVES: To determine the prevalence and treatment rates of secondary health conditions (SHCs) and mental health states in persons with long-term spinal cord injury (SCI) receiving public compared with private healthcare services in South Africa
METHODS: A cross-sectional survey included 200 community-dwelling persons with long-term SCI, 60% with paraplegia, 53% with complete injuries and 156 from the public and 44 from private healthcare sectors. The following modules of the International Spinal Cord Injury (InSCI) community survey were used: (i) demographic and injury characteristics; (ii) SHCs and treatment rates; and (iii) vitality and emotional well-being. All statistical analyses were stratified according to healthcare sector
RESULTS: Pain (47% v. 57), sexual dysfunction (59% v. 41%) and muscle spasms (54% v. 43%) were the most common SHCs in both cohorts, and the period prevalence was significantly higher for sleeping problems (41% v. 25%), sexual dysfunction (59% v. 41%) and contractures (42% v. 20%) in the public compared with the private cohort. Persons with SCI in the private cohort received treatment more often for sleeping problems (100% v. 45%), autonomic dysreflexia (75% v. 27%) and pain (56% v. 33%) than their counterparts with public insurance. Negative mental health states were prevalent in both groups
CONCLUSION: SHCs and negative mental health were common in persons with SCI in South Africa, while those with public insurance reporter a higher occurrence of sleep problems and contractures, as well as lower treatment rates. Overall, a need exists to better support persons with SCI in the long-term context to facilitate improved functioning and wellbeing
Spinal cord injury (SCI) is a serious medical event that almost always requires hospitalisation for medical intervention as well as rehabilitation.[1] The primary effects of SCI are sensory-motor deficits and autonomic system dysfunction, which if left unmonitored could set in motion a cascade of secondary health conditions (SHCs).[2,3] To mitigate these, specialised and comprehensive healthcare and rehabilitation services are needed to limit the impact of the primary and secondary effects of the injury on functioning and health.[4]
The literature reports a varying prevalence of SHCs at various stages of living with SCI, with the most common ones pressure injuries, pneumonia, urinary tract infection, neuropathic pain, spasticity and autonomic dysreflexia.[5-7] Since SHCs are often responsible for detrimental declines in functioning and health, and in some cases death, prevalence indices and timeous management of complications are seen as indicators of health systems response and quality. Previous reports on SHCs in the acute care phase and long-term follow-up in the community highlight unacceptable levels of preventable complications among persons with SCI accessing public-funded facilities in South Africa (SA).[2,3] Limited reports exist on the nature and prevalence of SHCs of those with private medical insurance locally. Such knowledge could assist with better co-ordination and sharing of knowledge between parallel healthcare systems.
Apart from physical complications, persons with SCI may experience changes in mental health and psychological well-being.[8] The prevalence of mental health conditions, such as depression, anxiety, and post-traumatic stress disorder, is elevated in persons with SCI.[9] This increase in mental health conditions could be because of pre-morbid health conditions, the traumatic nature of the SCI or the evolution of mental health symptomatology as the individual with SCI lives with the injury. Sources of influence, considered as personal, injury related and environmental, on mental health in persons with SCI are multifactorial, with literature supporting the moderating effect of poor structural relationships (e.g. partner status, social contact frequency) and functional aspects (e.g. satisfaction with overall social support, family relationships) on general mental health decline and depressive symptomatology.[10] The elevated prevalence of physical and mental health conditions in persons with SCI is partly attributed to limited health literacy among healthcare practitioners (service providers) and persons with SCI (service users) with respect to secondary prevention.[11] Health literacy refers to the awareness of the nature and management strategies concerning SHCs, but also beliefs, attitudes and behaviours associated with prevention, which should be understood and addressed in service providers and service users. Furthermore, there is limited implementation of rehabilitation models that are geared towards empowering clients to manage their health conditions.[12] The perceived limited implementation of behavioral interventions in both public and private healthcare sectors are due to insufficient workforce, limited risk screening for SHCs on admission and during the care episode, few education sessions on SHCs prevention and development, and challenges to accessing primary healthcare for annual checks and treatment modifications.[13]
The incidence of (traumatic) SCI in SA is among the highest globally, at 76 per million.[14] In the absence of scientific evidence on the incidence/prevalence of non-traumatic SCI in the local context, it is also thought to be elevated in comparison with other contexts because of the HIV/Aids and tuberculosis (TB) endemic.[15] The local SA context is one of great diversity, with ~84% of inhabitants relying on public healthcare services, while the private sector serves the remaining portion of the population, largely those from more affluent backgrounds.[16] Despite the National Department of Health's mandate on the provision of comprehensive and client-centred healthcare, the lack of adequate healthcare facilities as well as insufficient human and financial resources are some of the challenges plaguing the public-funded healthcare system,[17] and owing to this, systematic disparities in service delivery and patient-oriented outcomes, such as work and social participation, exist. While previous studies conducted in SA have reported differences in incidence, aetiology and sociodemographic factors between public and private cohorts,[18] it remains unknown how they differ in terms of functioning, specifically health status, impairments and functional abilities, since significantly more resources are available to those with private healthcare insurance. To unravel health systems-specific differences, this study primarily set out to determine the prevalence of SHCs and mental health states (i.e. vitality and emotional well-being) in persons with long-term SCIs receiving public or private healthcare in SA, as well as the extent to which SHCs were treated in the two parallel healthcare sectors.
Methods
Design, setting and participants
In this descriptive cross-sectional survey, non-probabilistic sampling was used to recruit participants aged >18 years with a confirmed primary diagnosis of SCI, including both traumatic and nontraumatic. This study was founded on a larger international project under the World Health Organization's Learning Health Systems initiative for SCI.[19] The aim of this initiative was to examine the lived experiences of persons with SCI worldwide, as well as assessing societal response to addressing their needs, utilising the International Spinal Cord Injury (InSCI) community survey.
Two out of a potential of nine provinces were conveniently selected to form the target population. The selection of these provinces was based on the availability of existing databases/registries for persons with SCI. Gauteng Province is SA's administrative capital. In terms of size, it is the smallest of all provinces with the highest population density (~16 million; 26% of population). This province also has the highest gross domestic product (GDP) per capita. The Western Cape Province is the fourth largest in size, home to ~12 million persons, and has the second highest GDP per capita in the country. In terms of healthcare expenditure, the Western Cape and Gauteng provincial governments spend annually ZAR3 867 (~USD271) and ZAR3 523 (~USD246) per person, respectively.[20]
Participants were consecutively recruited from public and private registries in the respective regions of the City of Cape Town (Western Cape Province) and Pretoria/Johannesburg (Gauteng Province) of SA. Eligible participants were recruited from (i) a pre-existing database of acute public healthcare hospitals and (ii) a public rehabilitation facility database, while those from the private sector (Gauteng Province) were recruited from a private rehabilitation hospital database. All participants were initially telephonically contacted to be invited to voluntarily partake in this study. Of 426 individuals invited to partake, 200 consented and completed the survey. Of these, 156 and 44 were recruited from the public and private healthcare registries, respectively. Individuals who were hospitalised at the time of the survey, or who had severe cognitive impairments, were excluded from the study.
Data collection tools and procedure
The InSCI community survey data model was informed and underpinned by the International Classification of Functioning, Disability and Health and the Health Core Sets for SCI. The development process of the InSCI survey has previously been described.[21,22] In short, the InSCI survey aims to capture the lived experiences of persons with SCI through the inclusion of 6 components operationalised with 125 questions, including functioning (n=28 body functions and structures; n=42 activities and participation), contextual factors (n=26 environmental; n=19 personal factors), lesion characteristics (n=2) and appraisal of health and well-being (n=8). The (i) demographic and lesion characteristics, (ii) body functions and structures ('health problems') and (iii) appraisal of health and well-being ('energy and feelings') components of the InSCI survey were used in this paper. Demographic variables included gender, age, marital status, education level and household income, while injury characteristics related to age at, and time since, injury, aetiology, as well as impairment level and severity. Health problems, also referred to as SHCs arising from SCI, were collected using items from the Spinal Cord Injury Secondary Health Conditions Scale (SCI-SHC), which is both valid and reliable with a test re-test reliability ranging from 0.569 to 0.805.'231 In addition, the Self-Administered Comorbidity Questionnaire, which is an efficient method with good reliability and validity for the assessment of comorbid conditions in the absence of medical records, was completed by participants.'241 Lastly, 'energy and feelings' questions were evaluated using the SF-36 Version 2. These relate to vitality and fatigue levels of individuals, plus their emotional status. This subscale showed adequate reliability and validity as a measure of mood in persons with SCI.'251 Concerning SHCs alone, participants were also asked to indicate whether treatment was received for respective complications, using yes/no response options. Interviews were conducted either face-to-face or via telephone between 1 June 2017 and 31 December 2018. Due to the length of the questionnaire, i.e. 125 items, some participants (n=6), especially those completing the survey via telephone, requested data collection in two phases due to fatigue or time constraints. All who requested a second session completed the survey.
Data analysis
Descriptive statistics were generated in Statistical Package for Social Sciences (SPSS, USA) version 26 for sociodemographic variables and injury characteristics of the cohorts. Individual items of the health problems module were originally scored on a Likert scale, with 1 = no problem, 2 = mild problem, 3 = moderate problem, 4 = severe problem and 5 = extreme problem. Furthermore, the five aforesaid categories were subsequently re-categorised and thus considered as 'absent and mild' if rated 0 and 1, and 'significant and existing problem' if rated between 3 and 5. Similarly, for the energy and feelings module, the prevalence of 'significant problem' was determined by clustering the following response options: 'all of the time', 'most of the time' and 'some of the time', while options related to 'a little of the time' and 'none of the time' constituted absent or insignificant problem. Ages have been categorised according to the International Spinal Cord Society guidelines.[26] Categories for aetiology, marital status, household income and level of education variables were collapsed to ensure comparability with other studies.[27,28] All presented results were stratified according to the health sector (public v. private). Lastly, inferential statistics (e.g. independent samples f-tests for continuous data and χ2 for categorical data) were conducted to identify statistically significant differences between cohorts. For all inferential statistics, the p-value (alpha level) was set at 0.05 (95% confidence intervals).
Ethics
Ethical approval was granted by the Research Ethics Committee of University of the Western Cape (ref. no. BM16/3/24). We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the research. These principles related to the obtainment of informed consent, voluntary participation of participants, right to withdraw, right to remain anonymous, and storage of data in a secured space for a 5-year period.
Results
Participant characteristics: demographics and injury-related variables
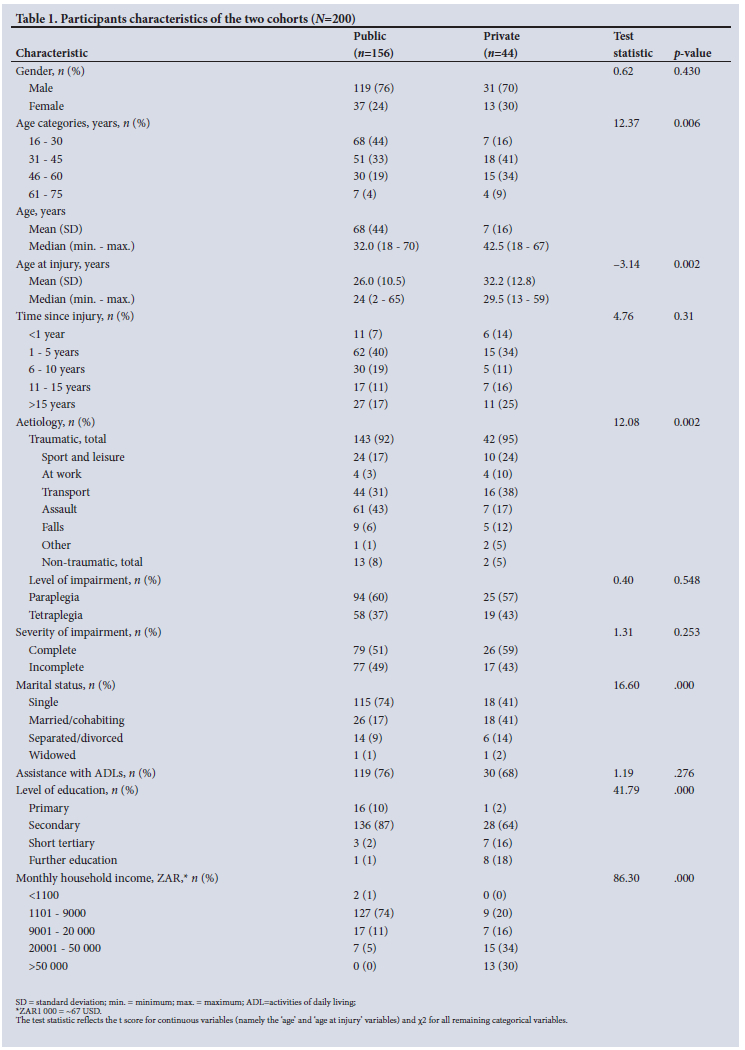
Table 1 presents sociodemographic and injury-related details of participants in the public and private cohorts. Distribution of gender and level of injury were similar across the cohorts, with around three-quarters being male and about 60% living with paraplegia. Slightly more than half had complete injuries in both cohorts. The mean age of the public cohort was 35.5 years, almost 8 years less than that of the private group. While >90% of injuries were traumatic in nature in both cohorts, a significant difference in the distribution of cases to cause of injury was found, with more assault-related injuries in the public sector, compared with road accidents as the most common cause in the private cohort.
The most profound differences between the cohorts appear in relation to socioeconomic position. With respect to education, a small fraction of the public cohort (3%) had any education following secondary school, compared with 34% of the private cohort who had gone on to further education. Furthermore, significant monthly household income differences were observed, with 74% of the public cohort receiving <ZAR9000 (~USD600) in contrast to 64% of those in the private cohort reporting at least ZAR20 000 (~USD1 350 SD) per month.
Secondary health conditions and corresponding treatment levels
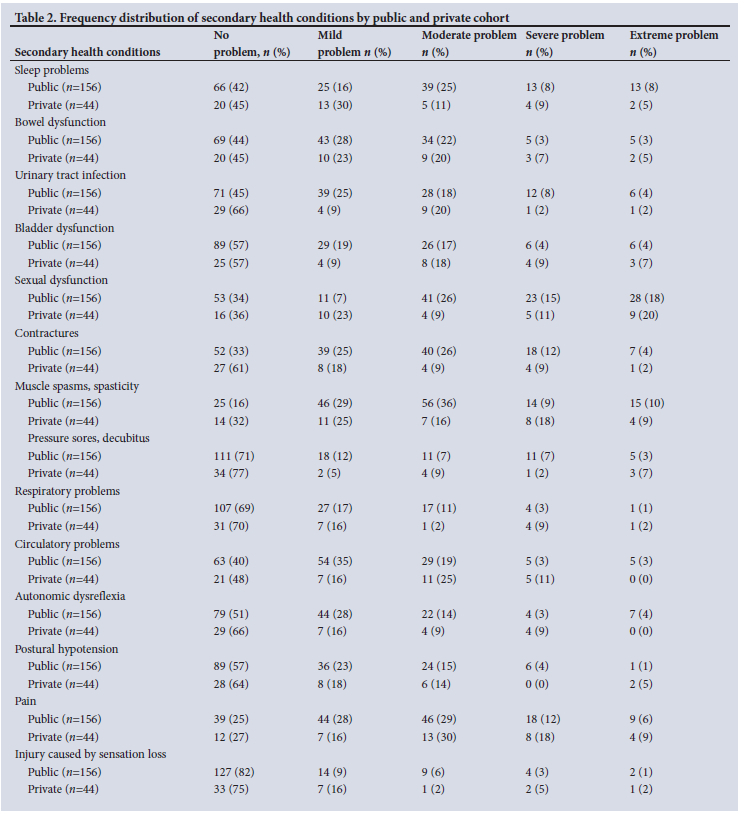
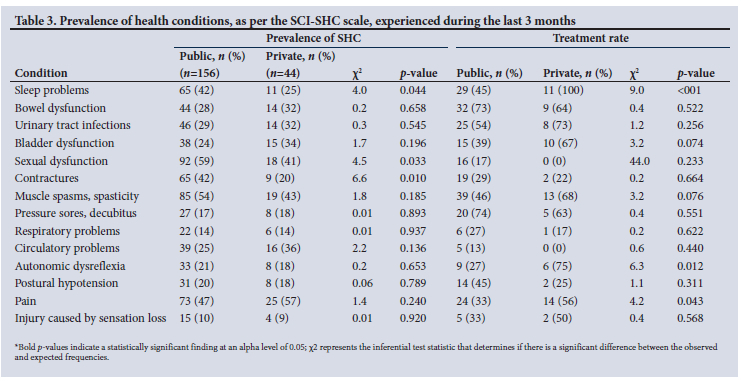
Table 2 illustrates the frequency distribution of SHCs for both public and private healthcare cohorts, while Table 3 presents the prevalence of SHCs and treatment rates during the last three months prior to data collection. Taken together (Table 3), pain, sexual dysfunction and muscle spasms were the three most prevalent SHCs, irrespective of the cohort, with each of these factors affecting at least 40% of participants.
Compared with the private cohort, a larger proportion in the public cohort experienced sleep problems (41% v. 25%; p=0.044), sexual dysfunction (59% v. 41%; p=0.033), and contractures (42% v. 20%; p=0.010). Respiratory problems, pressure sores and injuries related to loss of sensation were the least problematic health problems, with <20% reported as a notable complication in either cohort.
In terms of treatment rates for SHCs (Table 3), those in the public sector indicated that treatment was received more readily for pressure injuries/sores (74%), bowel dysfunction (73%) and urinary tract infection (54%), while sleep problems (100%), autonomic dysreflexia (75%) and urinary tract infections (73%) were most treated in the private cohort. Compared with the public cohort, a significantly larger proportion in the private cohort had received treatment for sleep problems (45% v. 100%; p<0.001), although the prevalence was higher in the public sector cohort. Significantly better treatment rates were further found for autonomic dysreflexia (27% v. 75%; p=0.012) and pain (33% v. 56%; p=0.043) in the private cohort compared with the public cohort.
Vitality and emotional well-being
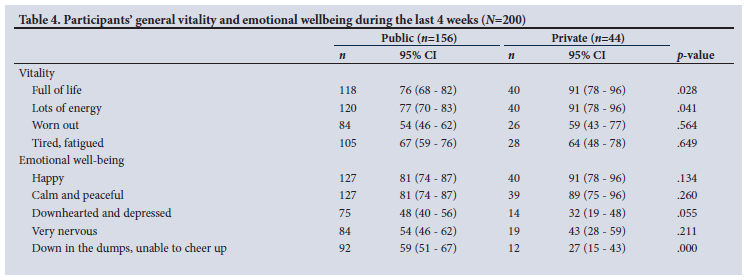
Table 4 presents vitality and emotional well-being outcomes of the two cohorts during the last 4 weeks prior to data collection. The most common positive vitality and emotional well-being states in both cohorts were 'happy' and 'calm and peaceful', stated by at least 80% of participants. On the contrary, the most common negative vitality and emotional wellbeing states in both cohorts were 'tiredness/fatigue', 'worn out and downhearted and depressed'. For the vitality domain, a larger proportion in the private cohort perceived states 'full of life' (91% v. 76%; p=0.028) and 'lots of energy' (91% v. 77%, p=0.041) compared with the public cohort. For emotional well-being, a larger proportion in the public cohort experienced 'feeling down in the dumps, unable to cheer up' compared with the private cohort (59% v. 27%; p<0.001).
Discussion
The aim of this study was to determine the prevalence of SHCs and mental health states affecting individuals living with an SCI in SA, and report on the proportion of individuals who received treatment for SHCs in the public and private health sectors. In this novel context, characterised by large wealth disparities and a lack of universal healthcare, we further attempted to highlight differences in SHCs and mental health states between the cohorts.
Secondary health conditions and treatment rates
In line with our findings, sexual dysfunction,[29,30] pain[29,31] and muscle spasms[32] have previously been indicated as substantial SHCs following SCI. With this in mind, treatment rates for these SHCs were not the highest when compared with other less prevalent SHCs found in this study. The finding of disproportionate lower treatment rates among more prevalent SHCs could be due to stigma attached to sexual dysfunction, which influences healthcare-seeking behavior. Also, lower treatment rates for pain and muscle spasms could be due to lower health literacy as well as awareness of treatment options. Findings revealed a significant difference in the prevalence of contractures and sleep problems, with those in the public sector demonstrating a greater period prevalence. Interestingly, those in the private sector received treatment for sleep problems to a greater extent than their public cohort counterparts. One possible reason for this could be better access to medications for sleep disorders in the private cohort.[33] Similarly, better access to medication, as well as improved access to comprehensive service delivery, including primary care and rehabilitation, could also be attributed to better treatment rates for pain in the private compared with the public cohort.[34,35]
Concerning the less prevalent SHCs, bladder and bowel dysfunction were not perceived to be particularly problematic for those with an SCI living in this context, which is, however, not the case in some reported literature originating from middle- and high-income settings.[30,36] A possible reason for lower reported prevalence of bladder and bowel dysfunction could be the use of efficacious evidence-based treatments. This is evident in the availability of evidence-based recommendations available for persons with SCIs in SA.[37] Pressure ulcers are commonly understood to be a major SHC in the spinal cord-injured population, and affected about one in five persons, in either cohort in this study, with >60% receiving treatment for them. On the one hand, as Mashola and Mothabeng[38] have postulated, good health behaviours, such as skin checking, could be partly responsible for the low prevalence of pressure ulcers. On the other hand, we postulate that the observed lower prevalence of pressure ulcers could be due to the high mortality rate among persons with SCI in SA,[3] as pressure ulcers have been significantly associated with premature death in this population.[39] Those with pressure ulcers have a greater likelihood of succumbing to death in the absence of time-sensitive treatments than those without.
Mental health states - vitality and emotional well-being
With respect to the vitality domain of mental health states, a significantly larger proportion of participants with private healthcare than those with public health insurance reported 'feeling full of life' and 'full of energy'. The better state of such vitality items could be due to an improved socioeconomic position and less financial strain among those with private healthcare compared with their counterparts with public healthcare.[10] Irrespective of cohort, fatigue was found to affect approximately two-thirds of participants in our study, and its relation to the emotional sequelae in SCI is supported by existing literature.[40] Tiredness and fatigue are not entirely unexpected owing to the increased effort and concentration required for many tasks following injury. Further, fatigue may also be related to health behaviours, such as low levels of exercise and poor diet.[41] In gaining a better understanding of the severity and character of fatigue, a more robust fatigue scale, such as the Fatigue Severity Scale or Modified Fatigue Impact Scale - SCI, should be used to account for the multidimensionality of fatigue in SCI, potentially leading to better understanding and subsequent management strategies for fatigue.
Low mood, particularly the item 'down in the dumps, unable to cheer up', was an important finding of this study, particularly as the prevalence of this emotional well-being dimension was more than double (27% v. 59%) in the public health, compared to the private health, cohort. Although the item selected on emotional well-being is not for diagnostic purposes of depression and anxiety, it does provide an indication of risk. A recent meta-analysis reported higher prevalence and greater risk for developing depression in individuals with SCI compared with the general population.[42] The literature suggests that the mental health of an individual with an SCI can be influenced by several factors, including SHCs,[43] social support,[44] self-efficacy[45] and socioeconomic status,[10] and may provide some explanation for a higher prevalence of depression among the public cohort. Given that those in the private cohort reported less frequent SHCs for many of the SHCs examined, coupled with better treatment rates generally, and less frequent mental health problems, the importance of socioeconomic status as a determinant of health is highlighted. Therefore, increased focus must be placed on improving public health services in this setting.
Further research and implications
This study focused on the prevalence of SHCs and mental health states and not the impact of these on functioning as defined by the WHO's International Classification of Functioning, Disability and Health. Previous research in the area has highlighted relationships between fatigue and depression, pain and depression[46] and the impact of SHCs on mental health, activity and participation, social participation[30] and quality of life.[33] There is therefore a justifiable need to further understand whether any clear associations exist between various factors, considering the context with special reference to different healthcare insurance packages and differences in sociodemographic and injury characteristics.
From a clinical perspective, health professionals can play an important role in minimising negative outcomes for individuals with SCI by promoting education on the prevention of SHCs, promoting healthy behaviours and addressing energy conservation. Likewise, peer support telephone interventions have proven to be effective in the prevention of health complications,[47] and may prove beneficial in this setting, especially due to existing environmental barriers, such as access to healthcare, financial hardships and transportation.
Further studies should explore health literacy - in service users and service providers - and healthcare-seeking behaviour in persons with SCI to inform the development of interventions to improve treatment rates, and subsequently limit the impact of SHCs and mental health states on functioning and quality of life, as well as inform the development of novel new treatments.
Limitations
This study is not without limitations. The InSCI survey provides a helpful overview of the lived experiences of individuals with a SCI. However, some outcomes are not explored in depth in terms of intensity and frequency. For example, the limited data collected were not able to inform us whether participants sought treatment for SHCs but did not manage to receive needed care, whether they did not know where to find information on possible treatments, or whether environmental factors (e.g. financial constraints, transportation, climate, attitudes, etc.) impacted treatment rates.
Another limitation relates to the cross-sectional nature of the study, which provides no information on how responses to outcomes may change over time and whether any cause and effect exists between exposures and outcomes. To this effect, the results on measures of association should be taken with caution due to the potential of type I errors because of multiple testing of significance. The results should be considered through the lens of exploratory testing of associations between outcomes and healthcare sectors to stimulate more robust investigations using probabilistic sampling in future. Lastly, the convenient sample hampers the ability to extrapolate findings to other settings and provinces in SA. Although the private cohort sample size was small in comparison with the public cohort, we believe results are still comparable owing to similar distribution in gender, age, lesion characteristics and time since injury.
Conclusion
A high similarity in the most common SHCs was observed between cohorts, and significant differences in period prevalence for sleep problems, contractures and certain mental health states ('full of life, lots of energy' and 'down in the dumps, unable to cheer up') were found, with better experiences in the private cohort. Higher treatment rates in the management of certain SHCs ('sleep problems', 'autonomic dysreflexia' and 'pain') were also observed in the private cohort. Overall, a need exists to improve self-management of SHCs in the long term, as well as the availability of more comprehensive rehabilitation packages, including physical and mental health support, for individuals with SCI living in SA.
Data availability statement. Derived data supporting the findings of this study are available from the corresponding author on request.
Declaration. None.
Acknowledgements. A special thanks to all participants who agreed to take part in this study. Also, this study is based on data from the InSCI Community Survey, providing the evidence for the Learning Health System for Spinal Cord Injury.
Author contributions. CJ: conceived the study, collected and processed the data, interpreted the results, and assisted with writing the manuscript. CT: processed the data, assisted with data interpretation, and co-wrote the first draft of the manuscript. EN: assisted with data interpretation and reviewed the different versions of the manuscript. ES: assisted with data interpretation and reviewed the different versions of the manuscript. DMC: assisted with study conception, assisted with data interpretation and co-wrote sections of the manuscript. AR: assisted with study conception, assisted with data interpretation and reviewed all versions of the manuscript.
Funding. The work reported herein was made possible through funding by the SA Medical Research Council (MRC) through its Division of Research Capacity Development. The content hereof is the sole responsibility of the authors and does not necessarily represent the official views of the SAMRC.
Conflicts of interest. None.
References
1. Nas K, Yazmalar L, Sah V, Aydin A, Önes K. Rehabilitation of spinal cord injuries. World J Orthop 2015;6(1):8-16. doi: 10.5312/wjo.v6.i1.8. [ Links ]
2. Joseph C, Nilsson Wikmar L. Prevalence of secondary medical complications and risk factors for pressure ulcers after traumatic spinal cord injury during acute care in South Africa. Spinal Cord 2016;54(7):535-539. https://doi.org/10.1038/sc.2015.189. [ Links ]
3. Madasa V, Boggenpoel B, Phillips J, Joseph C. Mortality and secondary complications four years after traumatic spinal cord injury in Cape Town, South Africa. Spinal Cord Ser Cases 2020;6(1):84. https://doi.org/10.1038/s41394-020-00334-w. [ Links ]
4. Cheng CL, Plashkes T, Shen T, et al. Does specialised inpatient rehabilitation affect whether or not people with traumatic spinal cord injury return home? J Neurotrauma 2017;34(20):2867-2876. https://doi.org/10.1089/neu.2016.4930. [ Links ]
5. Wahman K, Wikmar LN, Chlaidze G, Joseph C. Secondary medical complications after traumatic spinal cord injury in Stockholm, Sweden: Towards developing prevention strategies. J Rehabil Med 2019;51(7):513-517. https://doi.org/10.2340/16501977-2568. [ Links ]
6. Sezer N, Akku§ S, Ugurlu FG. Chronic complications of spinal cord injury. World J Orthop 2015;6(1):24-33. doi.org/10.5312%2Fwjo.v6.i1.24 [ Links ]
7. Adriaansen JJE, Post MWM, de Groot S, et al. Secondary health conditions in persons with spinal cord injury: A longitudinal study from one to five years post-discharge. J Rehabil Med 2013;45(10):1016-1022. https://doi.org/10.2340/16501977-1207 [ Links ]
8. Van Leeuwen C, Edelaar-Peeters Y, Peter C, Stiggelbout AM, Post MWM. Psychological factors and mental health in persons with spinal cord injury: An exploration of change or stability. J Rehabil Med 2015;47(6):531-537. https://doi.org/10.2340/16501977-1953 [ Links ]
9. Post MWM, van Leeuwen CMC. Psychosocial issues in spinal cord injury: A review. Spinal Cord 2012;50(5):382-389. https://doi.org/10.1038/sc.2011.182 [ Links ]
10. Zürcher C, Tough H, Fekete C, Group SS. Mental health in individuals with spinal cord injury: The role of socioeconomic conditions and social relationships. PloS One 2019;14(2). https://doi.org/10.1371/journal.pone.0206069 [ Links ]
11. Visser AM, Visagie S. Pressure ulcer knowledge, beliefs and practices in a group of South Africans with spinal cord injury. Spinal Cord Ser Cases 2019;5:83. https://doi.org/10.1038/s41394-019-0226-4 [ Links ]
12. Wakefield D, Bayly J, Selman LE, Firth AM, Higginson IJ, Murtagh FEM. Patient empowerment, what does it mean for adults in the advanced stages of a life-limiting illness: A systematic review using critical interpretive synthesis. Palliat Med 2018;32(8):1288-1304. https://doi.org/10.1177/0269216318783919 [ Links ]
13. Ahmat A, Okoroafor SC, Kazanga I, et al. The health workforce status in the WHO African Region: Findings of a cross-sectional study. BMJ Glob Health 2022;7:e008317. http://doi.org/10.1136/bmjgh-2021-008317 [ Links ]
14. Joseph C, Delcarme A, Vlok I, Wahman K, Phillips J, Wikmar LN. Incidence and aetiology of traumatic spinal cord injury in Cape Town, South Africa: A prospective, population-based study. Spinal Cord 2015;53(9):692-696. https://doi.org/10.1038/sc.2015.51 [ Links ]
15. Mann TN, Schaaf HS, Dunn RN, et al. Child and adult spinal tuberculosis at tertiary hospitals in the Western Cape, South Africa: 4-year burden and trend. Epidemiol Infect 2018;146(16):2107-2115. https://doi.org/10.1017%2FS0950268818002649 [ Links ]
16. Maart S, Jelsma J. Disability and access to health care - a community based descriptive study. Disabil Rehabil 2014;36(18):1489-1493. https://doi.org/10.3109/09638288.2013.807883 [ Links ]
17. Mayosi BM, Benatar SR. Health and health care in south africa - 20 years after Mandela. N Engl J Med 2014;371(14):1344-1353. https://doi.org/10.1056/NEJMsr1405012 [ Links ]
18. Phillips J, Braaf J, Joseph C. Another piece to the epidemiological puzzle of traumatic spinal cord injury in Cape Town, South Africa: A population-based study. S Afr Med J 2018;108(12):1051-1054. https://doi.org/10.7196/SAMJ.2018.v108i12.13134 [ Links ]
19. Stucki G, Bickenbach J. The implementation challenge and the learning health system for SCI initiative. Am J Phys Med Rehabil 2017;96(2):S55-S60. https://doi.org/10.1097/PHM.0000000000000672. [ Links ]
20. Ngobeni V, Breitenbach MC, Aye GC. Technical efficiency of provincial public healthcare in South Africa. Cost Eff Resour Alloc 2020;18(1):3. https://doi.org/10.1186/s12962-020-0199-y. [ Links ]
21. Gross-Hemmi MH, Post MWM, Ehrmann C, et al. Study protocol of the International Spinal Cord Injury (InSCI) community survey. Am J Phys Med Rehabil 2017;96(2):S23-S34.https://doi.org/10.1097/PHM.0000000000000647. [ Links ]
22. Fekete C, Post MWM, Bickenbach J, et al. A structured approach to capture the lived experience of spinal cord injury: Data model and questionnaire of the International Spinal Cord Injury community survey. Am J Phys Med Rehabil 2017;96(2):S5-S16.https://doi.org/10.1097/PHM.0000000000000622. [ Links ]
23. Kalpakjian CZ, Scelza WM, Forchheimer MB, Toussaint LL. Preliminary reliability and validity of a spinal cord injury secondary conditions scale. J Spinal Cord Med 2007;30(2):131-139. doi:10.1080/10790268.2007.11753924. [ Links ]
24. Sangha O, Stucki G, Liang MH, Fossel AH, Katz JN. The Self-Administered Comorbidity Questionnaire: A new method to assess comorbidity for clinical and health services research. Arthritis Care Res Off J Am Coll Rheumatol 2003;49(2):156-163. https://doi.org/10.1002/art.10993. [ Links ]
25. Van Leeuwen C, Van Der Woude L, Post M. Validity of the mental health subscale of the SF-36 in persons with spinal cord injury. Spinal Cord 2012;50(9):707-710. https://doi.org/10.1038/sc.2012.33. [ Links ]
26. DeVivo MJ, Biering-S0rensen F, New P, Chen Y. Standardisation of data analysis and reporting of results from the International Spinal Cord Injury Core Data Set. Spinal Cord 2011;49(5):596-599. https://doi.org/10.1038/sc.2010.172. [ Links ]
27. Str0m V, Mánum G, Arora M, et al. Physical health conditions in persons with spinal cord injury across 21 countries worldwide. J Rehabil Med 2022;54. doi.org/10.2340/jrm.v54.2040 [ Links ]
28. Middleton JW, Arora M, Kifley A, et al. Australian arm of the International Spinal Cord Injury (Aus-InSCI) community survey: 1. Population-based design, methodology and cohort profile. Spinal Cord 2022 (epub ahead of print). doi.org/10.1038/s41393-022-00850-6 [ Links ]
29. New PW. Secondary conditions in a community sample of people with spinal cord damage. J Spinal Cord Med 2016;39(6):665-670. doi.org/10.1080%2F10790268.2016.1138600 [ Links ]
30. Park SE, Elliott S, Noonan VK, et al. Impact of bladder, bowel and sexual dysfunction on health status of people with thoracolumbar spinal cord injuries living in the community. J Spinal Cord Med 2017;40(5):548-559. https://doi.org/10.1080/10790268.2016.1213554. [ Links ]
31. Müller R, Landmann G, Béchir M, et al. Chronic pain, depression and quality of life in individuals with spinal cord injury: Mediating role of participation. J Rehabil Med 2017;49(6):489-496. https://doi.org/10.2340/16501977-2241. [ Links ]
32. Richardson A, Samaranayaka A, Sullivan M, Derrett S. Secondary health conditions and disability among people with spinal cord injury: A prospective cohort study. J Spinal Cord Med 2021;44(1):19-28. https://doi.org/10.1080/10790268.2019.1581392. [ Links ]
33. Gray A, Riddin J, Jugathpal J. Health Care and Pharmacy Practice in South Africa. Can J Hosp Pharm. 2016;69(1):36-41. https://doi.org/10.4212/cjhp.v69i1.1521 [ Links ]
34. Kula N, Fryatt RJ. Public-private interactions on health in South Africa: Opportunities for scaling up. Health Policy Plan 2014;29(5):560-569. https://doi.org/10.1093/heapol/czt042 [ Links ]
35. Maphumulo WT, Bhengu BR. Challenges of quality improvement in the healthcare of South Africa post-apartheid: A critical review. Curationis 2019;42(1):1-9. https://doi.org/10.4102%2Fcurationis.v42i1.1901 [ Links ]
36. Piatt JA, Nagata S, Zahl M, Li J, Rosenbluth JP. Problematic secondary health conditions among adults with spinal cord injury and its impact on social participation and daily life. J Spinal Cord Med 2016;39(6):693-698. https://doi.org/10.1080/10790268.2015.1123845 [ Links ]
37. Theron F, Wilson V, Scriba E, Campbell R, Van Zyl M. Best practice recommendations for bladder management in spinal cord-afflicted patients in South Africa. S Afr Med J 2019;2(2):195-202. https://doiorg/10.7196/SAMJ.2019.v109i3b.13690 [ Links ]
38. Mashola MK, Mothabeng DJ. Associations between health behaviour, secondary health conditions and quality of life in people with spinal cord injury. Afr J Disabil 2019;8: 463. doi.org/10.4102%2Fajod.v8i0.463 [ Links ]
39. Cao Y, DiPiro N, Krause JS. Health factors and spinal cord injury: A prospective study of risk of cause-specific mortality. Spinal Cord 2019;57(7):594-602. https://doi.org/10.1038/s41393-019-0264-6 [ Links ]
40. Craig A, Tran Y, Wijesuriya N, Middleton J. Fatigue and tiredness in people with spinal cord injury. J Psychosom Res 2012;73(3):205-210. https://doi.org/10.1016/j.jpsychores.2012.07.005 [ Links ]
41. Saunders LL, Krause JS. Behavioral factors related to fatigue among persons with spinal cord injury. Arch Phys Med Rehabil 2012;93(2):313-318. https://doi.org/10.1016%2Fj.apmr.2011.09.001 [ Links ]
42. Williams R, Murray A. Prevalence of depression after spinal cord injury: A meta-analysis. Arch Phys Med Rehabil 2015;96(1):133-140. https://doi.org/10.1016/j.apmr.2014.08.016 [ Links ]
43. Craig A, Perry KN, Guest R, Tran Y, Dezarnaulds A, Hales A, et al. Prospective study of the occurrence of psychological disorders and comorbidities after spinal cord injury. Arch Phys Med Rehabil 2015;96(8):1426-1434. https://doi.org/10.1016/j.apmr.2015.02.027 [ Links ]
44. Fekete C, Tough H, Arora M, et al Are social relationships an underestimated resource for mental health in persons experiencing physical disability? Observational evidence from 22 countries. Int J Public Health 2021;66:619823. doi.org/10.3389%2Fijph.2021.619823 [ Links ]
45. Van Diemen T, Crul T, van Nes I, Group SS, Geertzen JH, Post MW. Associations between self-efficacy and secondary health conditions in people living with spinal cord injury: A systematic review and metaanalysis. Arch Phys Med Rehabil 2017;98(12):2566-2577. https://doi.org/10.1016/j.apmr.2017.03.024 [ Links ]
46. Finnerup NB, Jensen MP, Norrbrink C, et al. A prospective study of pain and psychological functioning following traumatic spinal cord injury. Spinal Cord 2016;54(10):816-821. https://doi.org/10.1038/sc.2015.236 [ Links ]
47. Houlihan BV, Everhart-Skeels S, Gutnick D, et al. Empowering adults with chronic spinal cord injury to prevent secondary conditions. Arch Phys Med Rehabil 2016;97(10):1687-1695. https://doi.org/10.1016/j.apmr.2016.04.005 [ Links ]
 Correspondence:
Correspondence:
C Joseph
conran@sun.ac.za
Accepted 9 February 2023


{kind=link}
{kind=link}
{kind=link}
{kind=link}