










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 n.5 Pretoria May. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i5.16556
RESEARCH
Knowledge, attitudes and practices of undergraduate health sciences students on hepatitis B vaccination at a South African university highlight the need for improvement of policies, implementation and co-ordination
N MakanI, II; E SongIII; A KramvisIV
IBSc, MB BCh; Hepatitis Virus Diversity Research Unit, Department of Internal Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIBSc, MB BCh; African Leadership in Vaccinology Expertise (ALIVE), School of Pathology, Faculty of Health Sciences, University of the Witwatersrand., Johannesburg, South Africa
IIIMB BCh, FRCP (Lond); Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVBSc (Hons), PhD; Hepatitis Virus Diversity Research Unit, Department of Internal Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Hepatitis B virus (HBV) infection causes nearly 300 million chronic infections globally. Healthcare workers face up to four times the risk of HBV infection through occupational exposure to contaminated blood and bodily fluids. Health sciences students (HSSs) are regarded as at an even greater risk as they embark on their clinical training journey. While chronic hepatitis B is incurable, it can be prevented by the safe and effective hepatitis B vaccine (HepB). The South African National Department of Health recommends at least three doses of vaccine (HepB3) for HSSs before patient contact. However, data on policy implementation at training institutions, vaccine coverage and HBV immunity in HSSs are lacking or limited
OBJECTIVES: To investigate knowledge, attitudes and practices of HSSs at the University of the Witwatersrand (Wits) in relation to international guidelines and institutional HepB programmes included in the Wits vaccination policy. Sociodemographic factors predicting HepB uptake were also investigated
METHODS: A cross-sectional study was conducted between February and June 2021. An electronic, self-administered survey was emailed to all current HSSs (N=3 785). The survey included questions on sociodemographic characteristics, knowledge of and attitudes towards HepB-related international guidelines and Wits policies, and HepB uptake and vaccine practices at Wits. Descriptive statistical analyses, followed by multivariable regression modelling, were used to identify factors associated with HepB uptake
RESULTS: A response rate of only 7.1% yielded 269 returned surveys, of which 221 were adequate for analysis. Most respondents were female (69.2%), with a mean (standard deviation) age of 22.5 (3.5) years, and were studying a Bachelor of Medicine and Surgery (MB BCh) degree (76.9%). Only 78% of those students who reported a history of vaccination (89.1% of study sample) reported a completed vaccine series. The only significant predictor, when adjusted for interactions, was being enrolled in MB BCh compared with other courses (odds ratio 4.69; p=0.026). Students displayed higher levels of knowledge around institutional (Wits) vaccine recommendations (94.1%) compared with international recommendations (75.6%). Most students were in favour of mandatory vaccination (91.4%), but not of serological testing following vaccination (42.5%). Half of our students received vaccinations in private facilities, but no follow-up or record was made of this by the designated Wits Campus Health and Wellness Centre
CONCLUSION: Institutional HepB policies are suboptimal, with no centralised co-ordination or implementation strategy. Urgent efforts are required to create awareness around policy and management, ensure vaccination coverage in this high-risk group, and foster positive practices with adequate monitoring
Hepatitis B is a potentially life-threatening liver disease that is caused by the hepatitis B virus (HBV). It remains a major public health challenge, with approximately 296 million people chronically infected globally, and ~1 million persons dying annually from consequent complications, such as liver cirrhosis and hepatocellular carcinoma.[l,2] HBV is estimated to be up to 100 times more infectious than HIV,[3] and can survive outside of the body for up to 7 days, during which the virus is still capable of causing infection.[4,5] Transmission of HBV occurs through exposure to infected blood and other bodily fluids. The timing of exposure and transmission routes typically accounts for the geographic variation in severity and prevalence of HBV infection. Chronic HBV infection disproportionately affects low- and middle-income countries, including many in sub-Saharan Africa, where exposure typically occurs at an earlier age (infancy and early childhood), leading to hyperendemic levels.[6] With no curative' therapies currently available, the prevention and control of HBV infection depends on the effective implementation of policies ensuring the provision of the safe and highly effective hepatitis B vaccine (HepB) to at-risk populations.[7]
In 1991, the World Health Organization (WHO) recommended the inclusion of a three-dose HepB schedule (HepB3) into routine infant immunisation programmes to reduce horizontal transmission in infants and young children.[8] In total, 190 WHO member states have introduced HepB3, with a current global coverage estimated at 83%.[9] Following this success, the WHO endorsed the addition of a first dose within 24 hours of birth (HepB-BD) to prevent mother-to-child transmission. Although coverage remains short of the WHO target of >90% for HepB3 and HepB-BD, together these strategies have resulted in a global reduction in the proportion of children under 5 years becoming chronically infected, from 4.7% to 1.3%,[1] and a prevention of more than 14 million potential cases.[11]
Another key strategy to achieving the goal of eliminating HBV as a global public health threat by 2030 is the need to endorse and strengthen similar prevention strategies among high-risk adult groups. One such group includes healthcare workers (HCWs), whose risk of infection is estimated to 2 - 4 times the level in the general population.[12-14] Occupational exposure to infectious blood and bodily fluids (BBF) through percutaneous or mucocutaneous routes is a major cause of HBV infection among HCWs.[15] Annually, an estimated 2.1 million HCWs are exposed to a 'sharp' injury, leading to -66 000 work-related HBV infections globally.[13] In the unvaccinated individual, the risk of acquiring HBV infection after a single exposure approaches 30%.[15] Rates of accidental exposure to BBF are greater among health sciences students (HSSs) when compared with their qualified counterparts,[16] particularly when clinical exposure occurs early in their respective curricula. Other factors contributing to the increased risk include inadequate knowledge around the risks of exposure and correct infection prevention methods, inexperience and a lack of confidence when performing procedural skills, and a reluctance to admit to accidental exposure in the workplace for fear of embarrassment.[17-19] The WHO therefore recommends that all HCWs and HSSs should be vaccinated with HepB3 if previously unvaccinated, followed by post-vaccination immunity testing 1 - 3 months after the last vaccine dose.[20] Globally, national policies regarding the vaccination of HCWs, and HSSs in particular, vary considerably, thus leading to marked differences in HepB coverage. Moreover, where national policies are not clearly stipulated, regional or institutional policies are used to govern vaccination practices, resulting in intranational variations.[21]
In South Africa (SA), universal HepB3 was integrated into the childhood Expanded Programme on Immunisation (EPI) schedule in 1995.[22] Two years later, vaccine coverage for HepB3 was estimated at just 74%, and it remains below the 90% target more than two decades later.[23] Consequently, a significant proportion of individuals born after 1995 remain inadequately vaccinated (incomplete HepB3 series or unvaccinated). In addition, universal HepB-BD was not routinely carried out in SA during that period. With regard to high-risk adult population groups, such as HCWs and HSSs, the SA National Department of Health (DoH) recommends pre-exposure vaccination - i.e. vaccination before engaging in any clinical activities.[24] However, guidelines for post-vaccination immunity testing are ambiguous, only stipulating 'high-risk HCWs' with no reference to HSSs.[24] In addition, HSSs are not provided with free vaccination,[25] leaving academic institutions to create and implement their own guidelines and policies for the protection of their students.[21] Two studies at other SA higher-education institutions show coverage levels exceeding 90% among HSSs, with one institution enforcing mandatory HBV vaccination, and the other providing free vaccination and serological testing services.[26,27]
Current guidelines at the University of the Witwatersrand (Wits) recommend HBV vaccination to all students registered within the Faculty of Health Sciences (FHS) during their first year of study. HSSs born after the introduction of HepB3 in the SA EPI receive a single 'booster' dose of HepB, with HepB3 reserved for only those students born before the introduction of HepB3 and non-SA residents who fail to provide proof of prior HepB3 receipt. There are no recommendations stipulated for HBV serological testing, to confirm immunity following vaccination, under the current Wits policy. The university's Campus Health and Wellness Centre (CHWC) provides healthcare services to Wits staff and students, including the administration of vaccines to HSSs for a nominal fee that is billed to the student's account. The CHWC services are currently the only source of records for determining HBV vaccine coverage among HSSs at Wits. However, this record is incomplete as many students may choose to be vaccinated at other health facilities (HF), or remain unvaccinated without the knowledge of the university. At present HBV vaccine coverage among FHS students at Wits remains unclear. Data on current vaccination practices among HSSs at Wits are necessary to inform policy and protect this high-risk cohort. Surveys designed to assess the knowledge, attitude and practices (KAP) have been validated for the identification of knowledge gaps and behavioural patterns related to vaccination among at-risk population groups. Further, they provide baseline data that may be used to evaluate any proposed interventions. We aimed to investigate the HepB uptake and KAP of undergraduate HSSs in relation to international and institutional (Wits) HepB policies, and further, investigate factors associated with HepB uptake.
Methods
A cross-sectional analytical study was conducted at the Wits FHS Campus. An electronic, self-administered questionnaire was sent to all students registered with the FHS from February to June 2021. A total of 3 785 students were invited to participate via email through the undergraduate office. The questionnaire was created and managed using an electronic data capture system (REDCap Software, USA). Validation of the questionnaire was completed through a pilot study on 15 undergraduate students (not included in the final analysis) in February 2021. The amended questionnaire consisted of sections related to student sociodemographic characteristics and prior hepatitis B vaccination, both HepB and HepB3. In addition, three domains were included that assessed the KAP of students towards HBV vaccination policies at Wits. The practice domain was limited to those students who had previously received HepB, and included questions on the timing and setting of vaccination in the Wits context.
The responses within the questionnaires were analysed to determine the HBV vaccine coverage among our study population. Questionnaire items did not contain forced-choice formats due to the sensitive nature of some of the questions. Several variables also contained options for 'prefer not to say' or 'unsure'. Through the REDCap survey instrument we were able to create a branching logic to questions, depending on the options selected. This allowed a logical flow of targeted and congruous questions between students with different vaccination histories/statuses.
The invitation email included an information sheet that described the purpose of the study, and guaranteed anonymity and strict confidentiality. Consent was obtained electronically from each participant prior to commencement of the questionnaire. Ethics approval was obtained from the Wits Human Research Ethics Committee (Medical) (ref. no. M201157) in February 2021.
All data were captured and stored on the encrypted REDCap online database. Completed questionnaires were anonymised, and personal identifiers were removed before importing the raw data into a password-protected Excel (Microsoft, USA) document. The data were then cleaned and checked for the significance of missing values (no significance was detected). A final version of the data was then imported into SPSS Statistics version 20.0 (IBM Corp., USA) for analysis.
Statistical analysis
Descriptive analysis of the dataset is presented as frequencies (n) and proportions (%) of the total study sample (N). Continuous variables are reported as means with standard deviation (SD) for normally distributed data and median and interquartile ranges (IQR) for non-normally distributed data.
Loglinear analysis, as a non-directional test, was used to determine if any significant associations existed between any categorical variables. The output of this analysis (K-way and higher-order effects) showed that only main effects between variables were significant, and no significant interactions were found between predictor variables. Following this, Pearson's χ2 test (or Fisher's Exact test where appropriate) was conducted on all variables that showed statistical significance in the loglinear analysis. Predictor variables that showed a significance of p<0.20 on χ2 testing were included in the final analysis. This multivariable binary logistic regression model was conducted to calculate the effect size (in the form of an adjusted odds ratio (OR) and 95% confidence interval (CI)) of predictor variables on the outcome (whether the respondent had been previously vaccinated coded as 1; or not vaccinated coded as 0). Responses recorded as 'unsure' were excluded from the binary logistic regression model.
All tests were two-tailed and a p-value <0.05 was considered statistically significant. Data will be maintained and stored in the REDCap database for a period of 6 years, as per regulatory and institutional requirements.
Results
A total of 3 785 questionnaires were distributed electronically, of which 269 responses (7.1% response rate) were received, and 221 (82.2%) were regarded as satisfactorily completed for analysis - i.e. data on the primary outcome variable of vaccination history was entered.
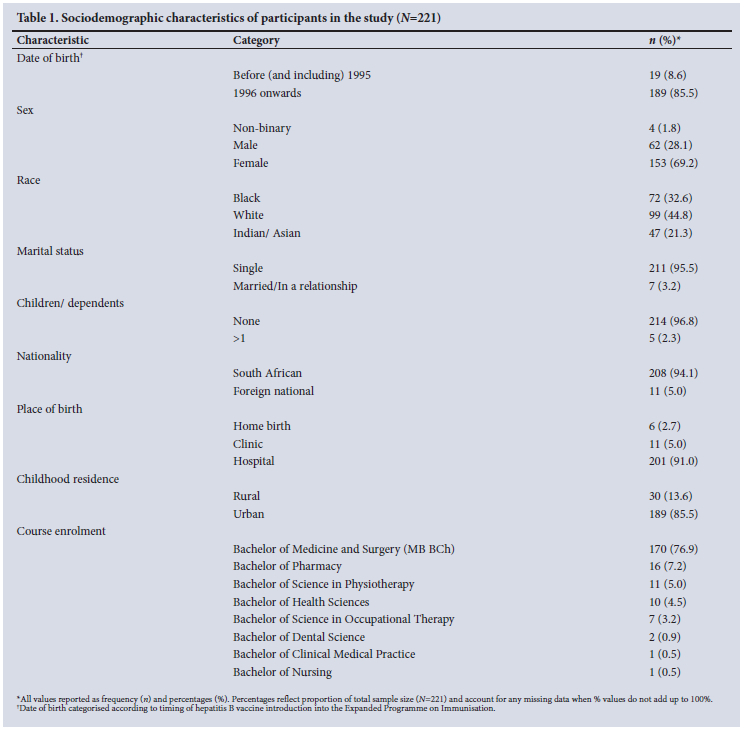
Table 1 describes the participant characteristics. More than two-thirds of the 221 respondents were female (69.2%; 153/221), with a mean (SD) age of 22.5 (3.5) years. The majority (85.5%; 189/221) were born after 1995 when the HBV vaccine was introduced into the EPI in SA. Most of the respondents were of SA nationality (94.1%: 208/221), had grown up in urban settings (85.5%; 189/221) and were studying a Bachelor of Medicine and Surgery (MB BCh) degree (76.9%; 170/221).
HepB history
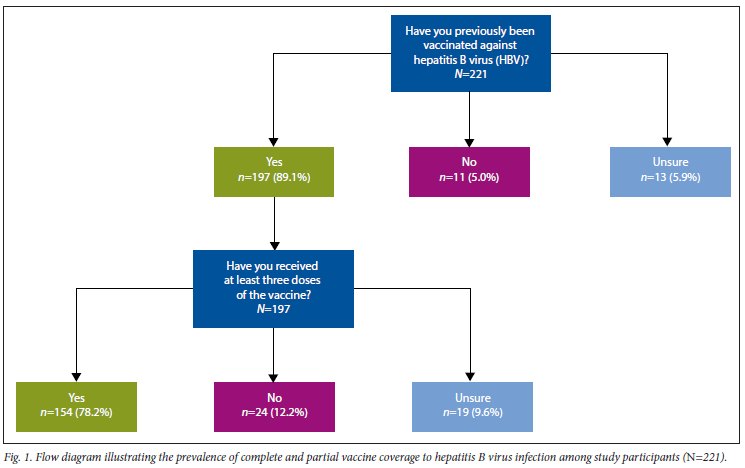
Of the 221 students, 89.1% (197/221) reported having been vaccinated against HBV, with 78.2% (154/197) of these having received a complete vaccine schedule of at least three doses (HepB3). Those who were unsure of any previous vaccination account for 5.9% (13/221) of our study sample, with a further 8.6% (19/221) unsure of the number of doses received (Fig. 1).
Only 5% (n=11) of students had never been vaccinated. The most common reasons cited by participants, for either no vaccination or an incomplete series, were vaccine stock-outs (n=7), a lack of information around institutional vaccination policies (n=5), financial cost implications (n=4) and a fear of needles (n=2).
In order to identify any associations between predictor variables and a positive vaccination history, only students who reported previous vaccination (n=197) and those who reported no vaccination (n=ll) were analysed. Students who were 'unsure' of their vaccine status (n=13) were excluded from this analysis as their impact did not change the outcome interpretation (separate independent analyses conducted) and could not be used as a stand-alone group by themselves due to the low sample size.
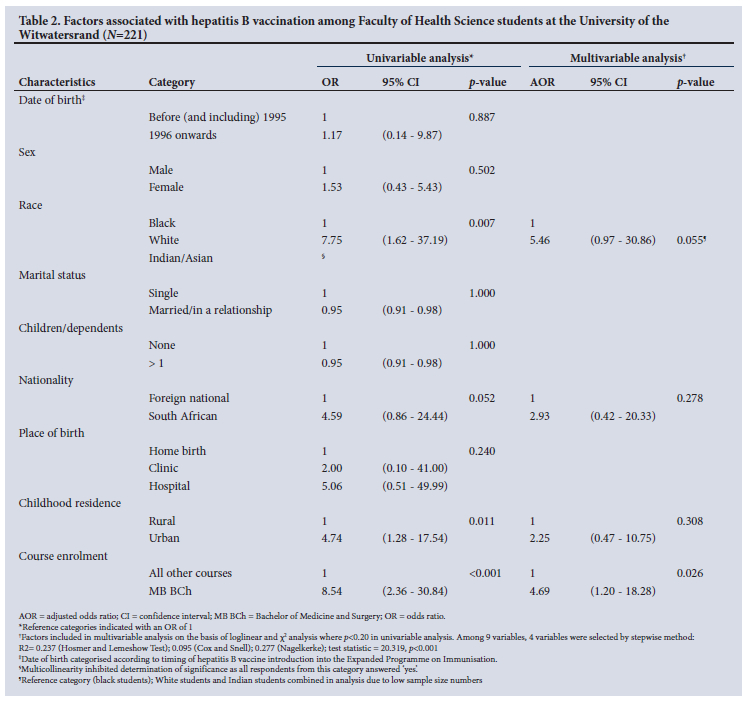
The following variables were significantly associated with a positive vaccine history (Table 2): white students compared with black students (OR 7.75; p=0.007); growing up in an urban setting (OR 4.74; p=0.011) and academic course enrolment - MB BCh compared with all others (OR 8.54; p<0.001). Following multivariable binary logistic regression, course enrolment remained the only significant predictor of a positive vaccine history (adjusted OR 4.69; p=0.026). Sex (p=0.502), marital status (p=1.000) and number of children (p=1.000) showed no significant association. All students born after 1995 were 1.17 times more likely to be vaccinated compared with those born during and before 1995, although this was not significant (p=0.887).
Knowledge around HBV vaccination policy and implementation
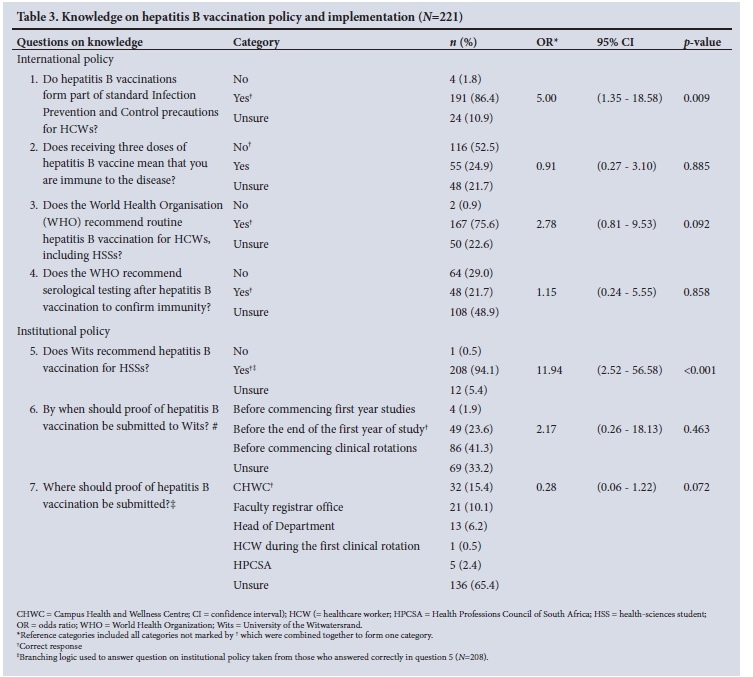
A number of questions were posed to the students to determine their knowledge on HBV vaccination policy and implementation (Table 3). Respondents who stated that vaccinations form part of standard infection prevention and control precautions for HCWs were five times more likely to be vaccinated (p=0.009) than those who disagreed or were unsure. Approximately half (52.5%) of the students knew that HepB3 vaccination does not necessarily equate to immunity, while 24.9% (55/221) incorrectly viewed three vaccine doses as immunity and a further 21.7% (48/221) were unsure. Further, 29% did not know that antibody testing was required after vaccination to measure immunity, while nearly half (48.9%) were unsure.
Respondents displayed higher levels of knowledge around institutional (Wits) vaccine recommendations (94.1%) than international (WHO) recommendations (75.6%). Notably, HSSs who were aware of Wits vaccination policies were 12 times more likely to have been vaccinated than those who did not know the policy (p<0.001). However, less than one-quarter of students were aware of when (23.6%) or to whom (15.4%) they should submit proof of vaccination.
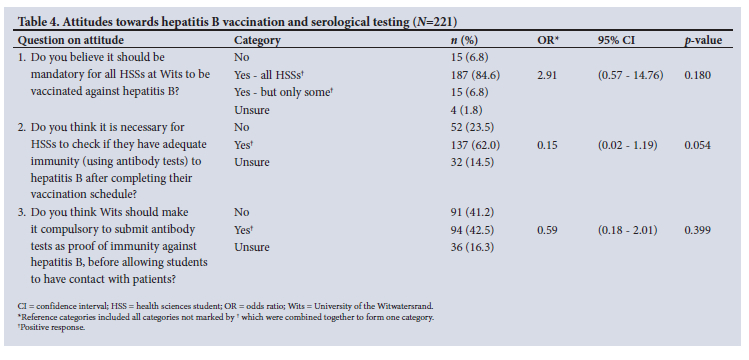
Attitudes towards Hepatitis B vaccination
From Table 4 it is apparent that the majority of respondents (84.6%) believed that HBV vaccination should be mandatory for all HSSs at Wits. Only 6.8% stated that it should not be mandatory, while 1.8% were uncertain. Qualitative inputs from some students (n=15; 6.8%) stated that mandatory policies should be limited to specific groups, including those students who 'have high clinical risk exposure', 'are patient-facing' or 'participate in laboratory dissections or other high-risk activities'. Fewer than two-thirds of the respondents (62%) thought post-vaccination antibody testing was necessary to confirm immunity, while less than half (42.5%) agreed that this practice should be made mandatory. No significant associations were noted between attitudes towards HBV vaccination and a history of having been vaccinated.
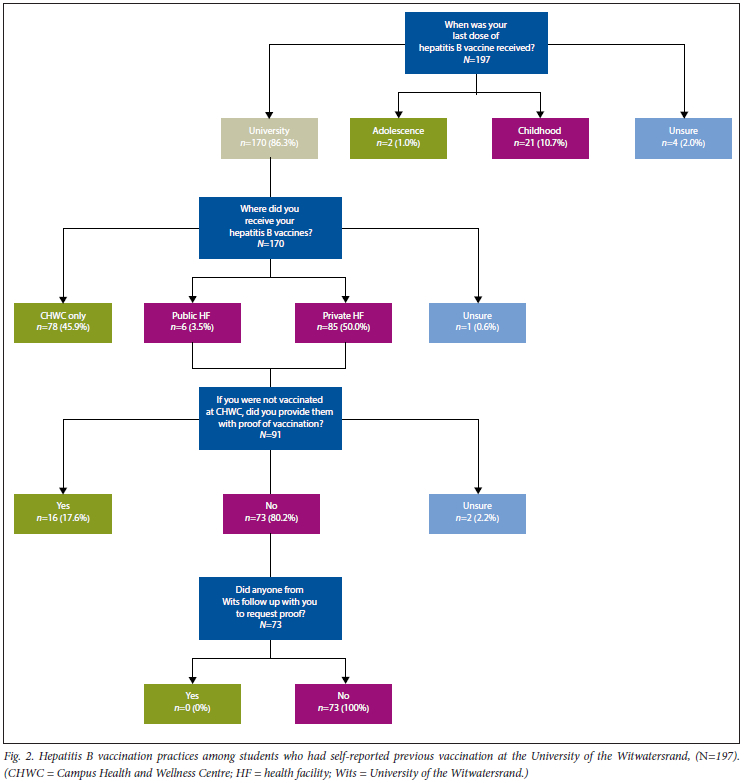
Vaccination practices at Wits
Of the students who had been previously vaccinated against HBV infection (n=197), a significant majority of 170 (86.3%) students had received their most recent vaccine dose while attending university (Fig. 2). CHWC was responsible for vaccinating less than half of these students (78/170), with most using private health facilities (85/170). Up to 80% (73/91) of respondents who had not been vaccinated at CHWC did not provide evidence of their vaccination status to CHWC, and all 73 students reported that no follow-up was made by Wits authorities on confirming proof of vaccination.
Discussion
This study sought to provide a cross-sectional description and understanding of the KAP of HBV vaccination in undergraduate FHS students at Wits. In addition, we sought to identify associations between sociodemographic characteristics and vaccination practices influencing HepB uptake among HSSs.
Due to COVID-19 regulations and the limited access to the university campus, questionnaire surveys were distributed electronically to students via university-linked emails. Despite several invitations to participate in the study, <10% of the HSSs responded to the questionnaire. This is not uncommon for digital surveys, which can be at least 10 percentage points lower than paper-based surveys, with response rates of approximately one-quarter of the population.[28] However, our response rate was shown to be markedly lower than other studies conducted in higher-education institutions,[29] particularly among undergraduate students.[30] Several reasons for student non-participation in surveys have been suggested, including a general decrease in volunteerism among students, higher demands for participation (exponential increase in online survey methodology for research purposes) that results in over-surveying, and preferential use of mobile devices (questionnaire functionality is not always optimised for mobile devices).[31] Additionally, concerns around safety and confidentiality may contribute to a reluctance to use web-based methods. Non-connectivity could not account for the lack of response, since all registered students received monthly data allowances, and the majority of teaching and learning occurred online during the 2021 academic year.
Although 89% of the respondents had received at least one dose of HepB, only 78% of those completed the vaccination series (HepB3). The 89% coverage in our study is similar to other SA studies that showed >90% coverage among HSSs.[26,27] These findings are in stark contrast to other African institutions, where coverage has been reported as low as 5%.[32] The major reasons for lack of vaccination within our cohort (5% of respondents) included vaccine stock-outs, inadequate education and information around the benefits and potential side-effects of vaccination at Wits as well as the costs associated with vaccination. The financial burden of vaccination has also been the principal factor contributing to non-vaccination in other African and European institutions.[26,32,33] Therefore, the provision of free and accessible vaccines for high-risk students, through either government or private donor funds, is a necessary means of protecting HSSs against HBV infection, and in turn the patients they care for. This recommendation is supported by other studies showing that the provision of free vaccination to students led to a significant increase of coverage, from 9.4% to 48.8% (p<0.001).[33]
Although the poor response rate limited the statistical power of our study, several significant associations were found. Certain sociodemographic traits were positively associated with a participant s likelihood of previous vaccination. These factors include white race and growing up in urbanised areas. These associations are similar to studies from other low- and middle-income countries and reflect the institutionalised effects of marginalisation on certain population groups, as well as a failure to provide redress to social determinants of health. The higher rates of vaccination in some race groups or those living in certain geographic locations may reflect differences in access to centralised healthcare services as well as socioeconomic, educational and health literacy differences. A positive association with HBV knowledge and urban residence, for instance, has been documented in some studies,[34] but not in others.[35] However, these aspects were not evaluated directly in this study, and future studies will be required to expound on this finding.
The strongest predictor of a students vaccination status was the course in which they were enrolled. Students enrolled in the medical course (MB BCh) were 8.5 times more likely to have been vaccinated than other HSSs (OR 8.54; p<0.001). These findings concur with those in other studies,[36] which attribute the higher levels of vaccine coverage among medical students to more clinical experience, as well as greater knowledge around HBV infection and prevention measures. A study by Ochu et al.[37] found that HCWs (i.e. persons with greater health literacy) exhibited higher perceptions of both susceptibility to contracting HBV and disease severity of HBV, if contracted. These health beliefs in turn drove positive health-related behaviours, such as vaccination, in this subgroup.[37] Thus, improving health literacy on HBV can directly improve one's health behaviour.[35]
The majority of students displayed good knowledge of both institutional (94.1%) and international (75.6%) recommendations for HepB. However, only institutional knowledge was significantly associated with HepB uptake (OR 11.94, p<0.001). Despite this, most students were still not aware of where or by when proof of vaccination needed to be submitted to the health authorities at Wits. It is clear that the Wits policy on HepB is not implemented effectively. Increasing awareness of Wits HepB policy, coupled with earlier education on the risk of HBV exposure and infection and benefits of timely and appropriate vaccination, will improve vaccine uptake and HSS engagement in positive vaccination behaviours.
Uncertainty around concepts of vaccination and immunity following vaccination ('immunisation) was noted among our student cohort. Approximately half of the students (52.5%) knew that a complete primary series (HepB3) did not necessarily equate to immunity. Levels of knowledge on post-vaccination immunity showed no significant association with a student's prior vaccine status. This is not a surprising finding, as a study of SA HIEs found a poor understanding of what constituted adequate immunity following vaccination among academic principals and heads of departments at these universities and nursing colleges.[21] Authority figures such as these have been shown to influence a students decision to vaccinate with improved uptake among those who are better informed by professional sources or medical teachers.[38] The introduction of formal training by academic authorities for newly admitted HSSs could address the shortfalls in knowledge surrounding HepB and immunity.
More than 90% of the students in our study stated that 'mandatory policies for HepB should be implemented by the university. This shows that students understand and value the importance of vaccines in preventing HBV infection and transmission. Similarly, strong recommendations and mandates have been shown to improve vaccine coverage, while other studies show that one of the principal reasons behind non-vaccination (cited by HSSs) was the 'non-compulsory nature of HepB policies.[39]
In addition, the majority of students (62%) felt that HSSs should confirm their immune status following vaccination, despite the omission thereof from current Wits HepB policy. Less than half agreed that this practice should be made mandatory by the institution. The lower response in favour of mandatory policy could be the result of suspected financial implications for the students, who are expected to pay for their own vaccines, and may have assumed similar costs would be incurred by them if additional mandates come into effect. A study by Le Roux and Dramowski[26] at another SA university saw their HSSs calling for vaccination and immunity testing to be subsidised by the university funders or the National DoH, a sentiment not examined in our study. When vaccination and immunity testing are provided free of charge, >90% of students complete their vaccination schedules and at least 80% receive immunity testing.[27] The subsidisation of vaccination and serological testing to confirm immunity to HBV should be considered by both institutional and national health authorities.
Limitations
This study was conducted in a single academic institution within SA, which limits the generalisability of the results found. In addition, the questionnaire relied upon self-reported HBV vaccination practices, without documented proof of prior vaccine receipt, which is subject to recall bias particularly for vaccines received in childhood. Despite guaranteeing and safeguarding the anonymity of our participants, several students were not comfortable with answering questions around vaccine practices, as seen by those choosing to select the option 'prefer not to say' or omitting the options altogether. The contribution of the COVID-19 pandemic to the remote online teaching and learning interface may have also contributed to 'survey fatigue', leading to a low response rate for the online survey used. Questions referring to knowledge may be subject to social desirability bias as students may have searched for the correct answers online during the survey - no time limits or website browser restrictions were implemented. The use of an electronically distributed questionnaire in our study may have introduced a volunteer bias whereby the characteristics of respondents may differ systematically from non-respondents and thus the greater target population. This volunteer bias is likely inflated by the poor response rate in our study (7.1%) as well as the skewed sampling distribution towards medical students (76.9%). Furthermore, the lack of record-keeping and corroborating data from the Wits CHWC prevents a true understanding of the potential over- or under-estimation of HepB uptake within our sample compared with the total HSS population at Wits. It is therefore not possible to generalise these findings to our target population or similar populations at other tertiary institutions.
Conclusion
As students play an important role in the dissemination of knowledge and raising awareness among their communities, more opportunities to improve education and drive awareness around hepatitis B should be provided to the students themselves. Furthermore, HBV-related educational and empowerment initiatives should occur, to improve health-seeking behaviour and create a culture of health advocacy among the HSS communities at Wits. It is apparent from our study that policies regarding HepB at Wits require strengthening and reform. The current CHWC facility serves as the principal provider for preventive care services for students actively seeking assistance. However, both the FHS and CHWC facilities are currently not equipped to monitor and evaluate the vaccination practices of HSSs, and as a result may overlook those students who are unvaccinated and thus remain at high risk for infection when entering clinical practice. The responsibility to ensure completed vaccine series should not be left to students, but rather current policy should be enforced and centralised, and the CHWC should be provided with sufficient powers and resources for monitoring, follow-up and facilitation of a completed three-dose vaccination. In addition, Wits HepB policies should include serological testing to confirm immunity following vaccination, as well as to identify potential vaccine non-responders or those who may be infected, with these services and costs subsidised by the institution. We further recommend collaboration with the National DoH to assist with the following: identify prior vaccination status through national immunisation records; create a central electronic repository for HepB and immunity testing for all HSSs; provide extensive training, knowledge and up-to-date research for the prevention and management of exposure to HSSs through institutional authorities; and offer subsidies and incentives for complete vaccination and immunity testing, given the potential for non-immune healthcare personnel to transmit infection to vulnerable patients and pose a risk to their own well-being. Future research that samples a greater proportion of the target population of HSSs are needed to validate and expand on the findings of this study as well as facilitate the gene ral i sab ility of our conclusions.
Declaration. This research article formed part of the requirements for fulfilment of a Masters of Science in Vaccinology for author NM. All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the Helsinki Declaration. This research paper formed part of the requirements for fulfilment of a Masters of Science in Vaccinology for author NM.
Acknowledgements. We acknowledge the work by Dr C Le Roux and Prof. A Dramowski whose research on HBV vaccination practices at Stellenbosch University was used to help create the questionnaire in the current study. We would also like to thank the Wits Faculty Registrar's Office for the dissemination of the questionnaire to all registered students and the Wits Office for Statistical Support for their guidance in statistical analyses. Thank you to the participants of the study.
Author contributions. Conceived the study: AK, NM; Designed the questionnaire: NM, AK; Analysed the data: NM, ES, AK; Wrote the article: NM, AK. Read, contributed to and critically revised the article: NM, ES, AK. All authors read and approved the final manuscript.
Funding. Prof. Ernest Song, Administered Fund, University of the Witwatersrand.
Conflicts of interest. None.
References
1. World Health Organization. Global hepatitis report, 2017. Geneva. WHO, 2017. https://www.who.int/pubhcations-detail-redirect/global-hepatitis-report-2017 (accessed 5 November 2021). [ Links ]
2. World Health Organization. Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. Geneva. WHO, 2021. https://www.who.int/publications-detail-redirect/9789240027077 (accessed 23 November 2021). [ Links ]
3. Alter MJ. Epidemiology of viral hepatitis and HIV co-infection. J Hepatol 2006;44(1 Suppl):S6-S9. https://doi.org/10.1016/j.jhep.2005.11.004 [ Links ]
4. Centers for Disease Control and Prevention. Hepatitis B FAQs. Atlanta. CDC, 2020. https://www.cdc.gov/hepatitis/hbv/bfaq.htm (accessed 2 February 2022). [ Links ]
5. Bond WW, Favero MS, Petersen NJ, Gravelie CR, Ebert JW, Maynard JE. Survival of hepatitis B virus after drying and storage for one week. Lancet 1981;1(8219):550-551. https://doi.org/10.1016/s0140-6736(81)92877-4 [ Links ]
6. Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. Estimations of worldwide prevalence of chronic hepatitis B virus infection. A systematic review of data published between 1965 and 2013. Lancet 2015;386(10003):1546-1555. https://doi.org/10.1016/S0140-6736(15)61412-X [ Links ]
7. Suk-Fong Lok A. Hepatitis B treatment. What we know now and what remains to be researched. Hepatol Commun 2018;3(1):8-19. https://doi.org/10.1002/hep4.1281 [ Links ]
8. Expanded programme on immunisation. Global Advisory Group - part I. Weekly Epidemiol Ree 1992;67:11-15. https://apps.who.int/iris/handle/10665/228245 (accessed 25 January 2022). [ Links ]
9. World Health Organization. Hepatitis B Fact Sheet. Geneva. WHO, 2021. https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed 5 November 2021). [ Links ]
10. De Villiers MJ, Nayagam S, Haliett TB. The impact of the timely birth dose vaccine on the global elimination of hepatitis B. Nat Commun 2021;12(1):6223. https://doi.org/10.1038/s41467-021-26475-6 [ Links ]
11. Edmunds J, Jones E, Apolloni A, et al. Estimating the impact of HBV vaccination policies, 2016. https://www.who.int/immunization/sage/meetings/2016/october/Session9-Estimating-the-impact-of-HBV-vaccination-policies.pdf (accessed 2 November 2021). [ Links ]
12. West DJ. The risk of hepatitis B infection among health professionals in the United States. A review. Am J Med Sei 1984;287(2):26-33. https://doi.org/10.1097/00000441-198403000-00006 [ Links ]
13. Prüss-Ustün A, Rapiti E, Hutin Y. Estimation of the global burden of disease attributable to contaminated sharps injuries among health-care workers. Am J Ind Med 2005;48(6):482-490. https://doi.org/10.1002/ajim.20230 [ Links ]
14. Byrne EB. Viral hepatitis. An occupational hazard of medical personnel, experience of the Yale-New Haven Hospital, 1952 to 1965. JAMA 1966;195(5):362-364. https://doi.org/10.1001/jama.1966.03100050070021 [ Links ]
15. Shepard CW, Simard EP, Finelli L, Fiore AE, Bell BP. Hepatitis B virus infection. Epidemiology and vaccination. Epidemiol Rev 2006;28(1):112-125. https://doi.org/10.1093/epirev/mxj009 [ Links ]
16. Schmid K, Schwager C, Drexier H. Neediestick injuries and other occupational exposures to body fluids among employees and medical students of a German university. Incidence and follow-up. J Hosp Infect 2007;65(2):124-130. https://doi.org/10.1016/j.jhin.2006.10.002 [ Links ]
17. Musekene E, Modjadji P, Madiba S. The occurrence and contributing factors of needle stick and sharp injuries among dental students in a South African university. Open Public Health J 2020;13(1). https://doi.org/10.2174/1874944502013010126 [ Links ]
18. Sharma GK, Gilson MM, Nathan H, Makary MA. Neediestick injuries among medical students. Incidence and implications. Acad Med 2009;84(12):1815-1821. https://doi.org/10.1097/ACM.0b013e3181bf9e5f [ Links ]
19. Yang Y-Η, Wu M-T, Ho C-K, et al. Needlestick/sharps injuries among vocational school nursing students in southern Taiwan. Am J Infect Control 2004;32(8):431435. https://doi.org/10.1016/j.ajic.2004.02.007 [ Links ]
20. World Health Organization. Hepatitis B vaccines. WHO position paper, July 2017 - recommendations. Vaccine 2019;37(2):223-225. https://doi.org/10.1016/j.vaccine.2017.07.046 [ Links ]
21. Fernandes L, Burnett RJ, Francois G, Mphahlele MJ, Van Sprundel M, De Schryver A. Need for a comprehensive, consistently applied national hepatitis B vaccination policy for healthcare workers in higher educational institutions. A case study from South Africa. J Hosp Infect 2013;83(3):226-231. https://doi.org/10.1016/j.jhin.2012.11.026 [ Links ]
22. Aspinall S, Kocks DJ. Immuno geni city of a low-cost hepatitis B vaccine in the South African Expanded Programme on Immunisation. S Afr Med J 1998;88(1):36-39. [ Links ]
23. World Health Organization. WHO-UNICEF coverage estimates HepB3. Immunisation, Vaccines and Biologicals. Vaccine-preventable diseases, monitoring system 2020 global summary. Geneva. WHO, 2020. https://apps.who.mt/immunization_momtoring/globaisummary/timeseries/tswucoveragehepb3.html (accessed 17 February 2022). [ Links ]
24. National Department of Health, South Africa. National guidelines for the management of viral hepatitis. Pretoria. NdoH, 2020. https://sahivsoc.org/Files/SA%20NDOH_Viral%20Hepatitis%20guidelines%20final_.pdf (accessed 5 November 2021). [ Links ]
25. Primary Healthcare (PHC) Standard Treatment Guidelines and Essential Medicines List for South Africa, 2020. https://wwwknowledgehub.org.za/elibrary/primary-healthcare-phc-standard-treatment-guidelines-and-essential-medicines-list-south (accessed 5 November 2021). [ Links ]
26. Roux CL, Dramowski A. South African undergraduate health science students' knowledge, attitudes, practices and preferences regarding vaccination. Wits J Clin Med 2019;1(2):81-88. [ Links ]
27. Madiba T, Nkambule N, Kungoane T, Bhayat A. Knowledge and practices related to hepatitis b infection among dental and oral hygiene students at a university in Pretoria. J Int Soc Prev Community Dent 2018;8:200. https://doi.org/10.4103/jispcd.JISPCD_31_18 [ Links ]
28. Ebert JF, Huibers L, Christensen B, Christensen MB. Paper- or web-based questionnaire invitations as a method for data collection. Cross-sectional comparative study of differences in response rate, completeness of data, and financial cost J Med Internet Res 2018;20(1):e24. https://doi.org/10.2196/jmir.8353 [ Links ]
29. Greenlaw C, Brown-Welty S. A comparison of web-based and paper-based survey methods. Testing assumptions of survey mode and response cost. Eval Rev 2009;33(5):464-480. https://doi.org/10.1177/0193841X09340214 [ Links ]
30. McCabe SE. Comparison of web and mail surveys in collecting illicit drug use data. A randomised experiment. J Drug Educ 2004;34(1):61-72. https://doi.org/10.2190/4HEY-VWXL-DVR3-HAKV [ Links ]
31. Galea S, Tracy M. Participation rates in epidemiologic studies. Ann Epidemiol 2007;17(9):643- 653. https://doi.org/10.1016/j.annepidem.2007.03.013 [ Links ]
32. Harle K, Timerga A, Mose A, Mekonnen Z. Hepatitis B vaccination status and associated factors among students of medicine and health sciences in Wolkite University, Southwest Ethiopia. A cross-sectional study. PLOS One 2021;16(9):e0257621. https://doi.org/10.1371/journal.pone.0257621 [ Links ]
33. Launay O, Le Strat Y, Tosini W, et al. Impact of free on-site vaccine and/or healthcare workers training on hepatitis B vaccination acceptability in high-risk subjects. A pre-post cluster randomised study. Clin Microbiol Infect 2014;20(10):1033-1039. https://doi.org/10.1111/1469-0691.12689 [ Links ]
34. Vo TQ, Nguyen LHT, Pham MN. Exploring knowledge and attitudes toward the hepatitis B virus. An internet-based study among Vietnamese healthcare students. J Pharm Pharmacogn Res 2018;6(6):458-470. https://jppres.com/jppres/knowledge-attitudes-of-healthcare-students-toward-hbv/ (accessed 9 January 2022). [ Links ]
35. Machmud PB, Glasauer S, Gottschick C, Mikolajczyk R. Knowledge, vaccination status, and reasons for avoiding vaccinations against hepatitis b in developing countries. A systematic review. Vaccines 2021;9(6):625. https://doi.org/10.3390/vaccines9060625 [ Links ]
36. Pathoumthong K, Khampanisong P, Quet F, Latthaphasavang V, Souvong V, Buisson Y. Vaccination status, knowledge and awareness towards hepatitis B among students of health professions in Vientiane, Lao PDR. Vaccine 2014;32(39):4993-4999. https://doi.org/10.1016/j.vaccine.2014.07.022 [ Links ]
37. Ochu CL, Beynon CM. Hepatitis B vaccination coverage, knowledge and sociodemographic determinants of uptake in high risk public safety workers in Kaduna State, Nigeria. A cross sectional survey. BMJ Open 2017;7(5):e015845. https://doi.org/10.1136/bmjopen-2017-015845 [ Links ]
38. Diekema DJ, Ferguson KJ, Doebbeling BN. Motivation for hepatitis B vaccine acceptance among medical and physician assistant students. J Gen Intern Med 1995;10(1):1-6. https://doi.org/10.1007/BF02599567 [ Links ]
39. Adjei Gyimah A, Peprah P, Agyemang-Duah W, Frimpong E, Kwegyir Tsiboe A, Aboagye Darkwa M. Hepatitis B vaccination status and associated factors among university students in Ghana. A cross-sectional survey. Cogent Med 2021;8(1):2005226. https://doi.org/10.1080/2331205X.2021.2005226 [ Links ]
 Correspondence:
Correspondence:
N Makan
nisha.makanmurphy@gmail.com
Accepted 10 February 2023


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}