










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 no.5 Pretoria Mai. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i5.16736
RESEARCH
SARS-CoV-2 transmission risk in the school environment: A pilot case-ascertained prospective study to inform future school-based surveillance
N L SiegfriedI; A de VouxII; K JonasIII; J A YunIV; T ChettyV; M MabonaVI; F ElsVII; H MdoseVIII; L KuonzaIX; M HsiaoX; C MathewsXII
IMB ChB, DPhil; Health Systems Research Unit, South African Medical Council, and Faculty of Health Sciences, University of Cape Town, South Africa
IIBSc (Hons), PhD; South African Field Epidemiology Training Programme, Division of Public Health, Surveillance and Response, National Institute for Communicable Diseases of the National Health Laboratory Service, and Division of Epidemiology and Biostatistics, School of Public Health, University of the Witwatersrand, Johannesburg, South Africa
IIIBSc Com Health Sciences, PhD; Health Systems Research Unit, South African Medical Council, and Faculty of Health Sciences, University of Cape Town, South Africa
IVBPH, MSc; Health Systems Research Unit, South African Medical Council, and Faculty of Health Sciences, University of Cape Town, South Africa
VBVMCh; South African Field Epidemiology Training Programme, Division of Public Health, Surveillance and Response, National Institute for Communicable Diseases of the National Health Laboratory Service, and Division of Epidemiology and Biostatistics, School of Public Health, University of the Witwatersrand, Johannesburg, South Africa
VIBCMP; South African Field Epidemiology Training Programme, Division of Public Health, Surveillance and Response, National Institute for Communicable Diseases of the National Health Laboratory Service, and Division of Epidemiology and Biostatistics, School of Public Health, University of the Witwatersrand, Johannesburg, South Africa
VIIBSc, MSc; South African Field Epidemiology Training Programme, Division of Public Health, Surveillance and Response, National Institute for Communicable Diseases of the National Health Laboratory Service, and Division of Epidemiology and Biostatistics, School of Public Health, University of the Witwatersrand, Johannesburg, South Africa
VIIIBSc (Hons), MPH; South African Field Epidemiology Training Programme, Division of Public Health, Surveillance and Response, National Institute for Communicable Diseases of the National Health Laboratory Service, and Division of Epidemiology and Biostatistics, School of Public Health, University of the Witwatersrand, Johannesburg, South Africa
IXMB ChB, MPH; South African Field Epidemiology Training Programme, Division of Public Health, Surveillance and Response, National Institute for Communicable Diseases of the National Health Laboratory Service, and Division of Epidemiology and Biostatistics, School of Public Health, University of the Witwatersrand, Johannesburg, South Africa
XMB BCh, MPH; South African Field Epidemiology Training Programme, Division of Public Health, Surveillance and Response, National Institute for Communicable Diseases of the National Health Laboratory Service, and Division of Epidemiology and Biostatistics, School of Public Health, University of the Witwatersrand, Johannesburg, South Africa
XIDivision of Medical Virology, University of Cape Town and National Health Laboratory Service, Faculty of Health Science, Cape Town, South Africa
XIIBA, PhD; Health Systems Research Unit, South African Medical Council, and Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND: There is no current active or passive disease surveillance programme focused on schools in South Africa (SA). As such, the country is missing an opportunity to rapidly and effectively flag and address pathogen outbreaks, for example SARS-CoV-2, in a key closed setting. Furthermore, the role of school transmission in the spread of the SARS-CoV-2 virus within communities is uncertain
OBJECTIVE: This pilot study, conducted during March 2022 in Cape Town, aimed to indicate the feasibility of conducting intense active contact-tracing in a school environment prior to a large national study to compare school v. community SARS-CoV-2 transmission risk
METHODS: We conducted a pilot school-level case-ascertained prospective study with a component of enhanced surveillance. Following study initiation, the first learner at a participating school who tested SARS-CoV-2 positive (via polymerase chain reaction (PCR) or a rapid antigen test (RAT)) was invited to join the study as the index case and all their school-based close contacts were followed up telephonically, monitored for symptoms for 14 days, and tested using PCR if any symptoms were reported
RESULTS: On 8 March 2022, a student with RAT laboratory-confirmed COVID-19 was identified and they and their guardian consented to participate as the index case. Of the 11 eligible close contacts, six provided consent/assent and completed symptom-monitoring calls until the end of the 14-day study period. The secondary attack rate (SAR) was 2/11 (18.18%) of all close contacts who were at risk of infection, 2/4 (50.0%) of all those close contacts who developed symptoms, and 2/4 (50.0%) of all those close contacts who developed symptoms and were tested for SARS-CoV-2. During the same period, the school reported that 9 of the 926 learner body tested COVID-19 positive (0.97%). Total hours spent conducting monitoring for 6 learners was 27 hours, with each learner requiring approximately 4.5 hours of contact time during the study period
CONCLUSION: This is the first SA school-based COVID-19 transmission study, the results of which can inform national discussions regarding the role of schools and school-based active and passive surveillance in pathogen prevention and control
A systematic review of global studies of SARS-CoV-2 school-based studies identified that transmission is low in schools, but that most studies are not sufficiently controlled or well designed to provide comparative data to ascertain the true risk in schools compared with the community.[1] In addition, results may be biased, as the initial response to the COVID-19 pandemic resulted in school closures across the world, with few early studies conducted with schools in full attendance. The role of school transmission in the spread of the SARS-CoV-2 virus within communities therefore remains uncertain.[2,3]
Rapid identification of clusters in closed settings (such as schools) followed by active contact tracing has been the mainstay of epidemiological surveillance and disease outbreak control. Under the South African (SA) National Health Act No. 61 of 2003,[4] all notifiable medical conditions (NMC) including SARS-CoV-2 must be reported to the National Institute of Communicable Diseases (NICD) either through (i) laboratory reports from private and public laboratories, or (ii) clinical reports from diagnosing healthcare providers.[5] These data are reported to the NMC surveillance system and upon receipt, clinical and laboratory reports are merged. The laboratory report contains key demographics of a case, including residential address and occupation, but currently does not capture the name of the school attended in the case of a child. As a result, identification of clusters of cases in schools is reliant on alert school staff, and effective management thereof is dependent on timeous notification of the relevant health authorities and their operational capacity to respond.
Schools were tasked with incorporating the Department of Basic Education Standard Operating Procedures (SOPs) on COVID-19 management into their daily school practices during 2020.[6] Despite disease management being a health competency, the onus to identify and report clusters at schools remains on the school principal in the revised SOPs of February 2022.[7] The directive for the Integrated School Health Programme (ISHP) to assist schools in managing COVID-19 is questionable given that several evaluations have shown the ISHP to be fragmented and unco-ordinated.[8-10] There is no current active or passive disease surveillance programme focused on schools in SA, and as such the country is missing an opportunity to rapidly and effectively flag and address pathogen outbreaks in a key closed setting.
This pilot study aimed to indicate the feasibility of conducting intensive active contact-tracing in a school environment prior to a large national study to compare school v. community SARS-CoV-2 transmission risk. The primary objective was to determine the secondary infection risk among close contacts of a single index case in a secondary school, with the following secondary objectives: (i) describe and document the flow of contact tracing from identification of the index case to secondary contacts to inform future NMC reporting and surveillance; (ii) document any SARS-CoV-2 infection within the school during the same time period via passive symptom monitoring; and (iii) describe the environmental controls and use of non-pharmaceutical interventions within the classroom and broader school environment, and within the main modes of learner transport.
Methods
We conducted a pilot school-level case-ascertained prospective study with a component of enhanced surveillance. Following study initiation, the first learner at a participating school in the Western Cape Province who tested SARS-CoV-2 positive (via polymerase chain reaction (PCR) or rapid antigen test (RAT)) was invited to join the study as the index case, and all their school-based close contacts were followed up telephonically, monitored for symptoms for 14 days, and tested using PCR if any symptoms were reported.
Study partners
The study was led by the SA Medical Research Council Health Systems Research Unit in collaboration with the NICD SA Field Epidemiology Training Programme (SAFETP) in partnership with the Western Cape Education Department, the Western Cape Department of Health and Stellenbosch University and the University Cape Town. The SAFETP provided the dedicated contact tracing teams, and conducted sampling with nasopharyngeal swabs for PCR testing. PCR testing and viral genomic sequencing was done by the UCT Division of Medical Virology/National Health Laboratory Service.
Recruitment of school and identification of positive learner
We planned to identify a paediatric (aged 12 - 18 years) COVID-19 case by (i) monitoring reports to the NMC surveillance system of individuals aged <18 years who are positive, or (ii) a convenience sample through direct reporting to the study investigators from a selected government school, or from a general practitioner treating learners from the selected school, or (iii) via the Western Cape Education Department. To be eligible as the index case, the learner who tested SARS-CoV-2 positive must have attended school during their period of infectivity, defined as 48 hours prior to symptom onset until 10 days after symptom onset.
In partnership with the Western Cape Department of Education and through an informal network of general practitioners providing COVID-19 advice to schools, we identified several Cape Town secondary schools that met study eligibility criteria: (i) learners aged 12 - 18 years old, (ii) a diverse socioeconomic learner population, and (iii) learner households in reasonable travel distance within Cape Town.
We contacted school principals directly to explain the study, provide study information material, and requested permission from the school governing body. We planned to continue recruiting schools on a rolling basis depending on whether a case was identified timeously. Once permission was provided by several eligible schools, the principals circulated an invitation letter regarding the study produced in English, Afrikaans and isiXhosa to the school community, including teachers and guardians. Guardians were asked to return a signed sheet if they did not wish their child to participate in the study (opt-out); a statement was included that if no communication was received, it was assumed that the guardian was willing for their child to participate in the study.
Once a case was identified from any of the three sources, the index case and parent/guardian (if the child was <18 years old) would be contacted by a member of the study team and asked (i) whether they attended school during the period of infectivity, (ii) to confirm the name and contact information of their current school if identified via the laboratory list, and (iii) to provide the names, surnames, and contact information of all persons they came into close contact with during their period of infectivity.
Identification of the close contacts and symptom monitoring
Once the index case learner was identified, all school-based close contacts of the index case learner (both learners and staff) were identified in consultation with the school COVID-19 liaison officer, and invited to participate in the study. For this study, a close contact was defined as a staff member or learner who had been in contact with the index case learner with confirmed SARS-CoV-2:
(i) for >15 minutes within 1.5 metres, regardless of wearing a mask or face shield or face visor; or
(ii) in a shared closed classroom or workspace for >2 hours regardless of wearing a mask or face shield or face visor.
We defined close contact more broadly than the NICD guidelines current at the time including 'regardless of mask-wearing' given the diversity of mask materials and uncertainty regarding source control properties in non-standardised masks.
Once consent and assent were provided in the language of the participant's choice, the learners who were identified as close contacts completed a brief demographic survey as well as detailing exposure to the index case and whether or not they were wearing a mask, face visor and/or shield, and the type of mask worn at the time (e.g. cloth or surgical). The NICD SAFETP team then conducted daily telephonic symptom monitoring of each learner for 14 days. A learner who reported any of the following symptoms in the prior 24 hours during the 14-day monitoring period was advised to stay at home: fever, sore throat, congestion, cough, shortness of breath, myalgia, headache, diarrhoea, nausea and vomiting, dysgeusia, anosmia. The NICD SAFETP team performed a nasopharyngeal swab on the learner at their home within 24 hours of reporting symptoms. A PCR test was conducted on the specimen and results relayed to the learner. If results were negative and symptoms persisted, a second swab and PCR test was conducted within the following 24 hours.
As quarantine was no longer a legal requirement for close contacts at the time of the study, learners continued to attend school throughout the study period. Daily symptom monitoring was thus conducted in the late afternoon to accommodate learners attending school, and continued each day regardless of development of symptoms or test results. All learners who tested positive were advised to isolate for 7 days as per the clinical guidelines current at the time of the study, and offered information and contact details of their local clinic where they could seek further medical attention if necessary. If any learners exhibited anxiety or COVID-19-related stress when reporting to the NICD SAFETP team, they were offered social worker assessment and counselling provided specifically for the study participants.
Data collection, integrity and analysis
Data were collected and managed using the Research Electronic Data Capture (REDCap, USA) electronic data collection system, and uploaded directly to a secure REDCap database hosted by the University of the Witwatersrand, which provides data collection support.[11,12] Unique identifiers for participants were used and no personal identifiers were displayed in reports or communication. The database is password protected and a daily data quality and verification process was conducted by the data manager to ensure accuracy and completeness of data. The data were then transferred to Excel (Microsoft, USA) for analysis.
We had planned to calculate percentages to describe demographic, laboratory and epidemiological characteristics of the close contacts of the school-based case. As the sample was small, we report the absolute numbers instead, and a narrative description of the demographic, laboratory and epidemiological characteristics of the study participants.
Secondary attack rates are calculated as a percentage derived from the number of close contacts who test positive after exposure to the case using the following denominators: (i) all close contacts, (ii) all those close contacts who developed symptoms, and (iii) all those close contacts who developed symptoms and were tested for SARS-CoV-2. We also requested data from the school on the number of learners testing positive for the same period.
Standard operating procedures
The NICD SAFETP study team followed study-specific SOPs to ensure maximal protection from viral transmission to and from learners, and to maintain the safety of study participants and the study team. This was necessary when travelling together and when collecting nasopharyngeal swabs from learners. These included wearing KN95 masks when travelling together in a vehicle, ensuring opposite front and back windows were open in the vehicle, ensuring that two members of the team always travelled together, one of whom identified as male for security concerns, and performing swabbing outdoors at the learner household in the presence of at least one household member. The team member performing the swabbing donned a KN95 mask, a plastic apron and goggles. All waste was disposed of in a designated plastic bag in the appropriate receptacle at the Groote Schuur Hospital NHLS laboratory when the specimen was delivered. In addition, SAFETP team members were tested for COVID-19 weekly (midway through the study and within 72 hours of the end of study).
Safety advisory board
A safety advisory board (SAB) was established to advise investigators on the safety procedures required in the study, to review and advise on study design to secure the safety of study staff and participants and to make recommendations to modify safety and other procedures during the study as these arose. Composition comprised a virologist, an occupational and health medical practitioner with infection prevention and control expertise, a senior staff member of the Western Cape Education Department and a learner representative from the student representative council of a non-participating school. The SAB met virtually via Teams (Microsoft, USA) at the initiation of the study and again at day 7, and was available for assistance on an ad hoc basis.
School environmental assessment
The study team conducted an environmental health assessment of the school on day 2 of the study to record the extent to which the school implemented the following COVID-19 mitigation measures: (i) adequate ventilation (inadequate ventilation was defined as the room feeling stuffy or air smelling stale or being able to smell the body odour of other people in the room OR if the room was airconditioned, with closed windows or doors), (ii) physical distancing of school desks and learners in classrooms (a floor space of 1.5 m2 provided for each learner), (iii) availability of hand sanitisers, soap and running water, and (iv) wearing of masks.
Ethics
The study protocol was approved by the SAMRC Ethics Committee (ref. no. EC019-5/2021) in September 2021, with amendments approved in February 2022 to reflect changes in the laws regarding isolation and quarantine for COVID-19. Consent and assent procedures were conducted by trained SAMRC researchers using verbal consent/assent responses recorded on Teams. Responses were anonymised, saved with linkages between parental consent and child assent, password protected and archived. At study termination all participants were reimbursed a voucher of ZAR150 for their time and inconvenience.
Dissemination
Following the study completion period, we met with the school principal and COVID-19 liaison officer and presented them with the school environmental assessment findings and preliminary results of the study. The school suggested we prepare a brief summary of the findings for sharing in the school newsletter once the results are made public.
Results
Identification of the index case
The study recruitment period was opened on 7 March 2022. On the afternoon of Tuesday 8 March 2022, a principal of a girls' secondary school alerted us to a RAT laboratory-confirmed SARS-CoV-2 positive matric learner. On the morning of Wednesday 9 March 2022, the school confirmed that the guardian was willing to be contacted regarding study participation. The co-principal investigator (PI) then confirmed with the guardian that the learner met the index case eligibility criteria, having reported fatigue, body aches, sore throat and a cough on Sunday 6 March 2022 and a confirmatory test conducted on Monday 7 March 2022. The learner had attended school on Friday 4 March within the infectivity period 48 hours preceding symptom onset. Both guardian and learner agreed to participate and provided telephonic consent and assent, respectively, on Wednesday 9 March (Day 0 of the study).
School-based and related activities and identification of the close contacts
On Day 0, the co-PI contacted the index case learner who identified attending two school-based and one school-related activity during the 48-hour infectivity period. During school attendance on Friday 4 March 2022, individual lessons were of <45 minutes duration and held in different classrooms, so no contacts were identified from classroom attendance. Six friends who shared break time together with the index case met eligibility criteria for close contacts. On the evening of Friday 4 March 2022, the index case attended an outdoor fundraiser at the school where a teacher and three of the six friends already identified as close contacts met close contact criteria. On Saturday evening, the index case attended a sleepover at a private home where five additional close contacts were identified, all of whom attended the school.
Following receipt of the above information, the PIs met with the school COVID-19 liaison officer to confirm the school-based activities and obtain contact details of those learners and staff identified as close contacts. Of the 12 close contacts, two were excluded: one learner had reported being COVID-19 positive to the school in the preceding 3 weeks, and one learner's guardian had signed the opt-out form in advance of the study. Due to concerns regarding the Protection of Personal Information Act (POPIA), the Compliance Officer requested that the school first contact the guardians of the remaining nine learner close contacts to assess their willingness to participate in the study. No refusals were received by the school 24 hours later by day 1 of the study, and approval was given to commence the study consent process.
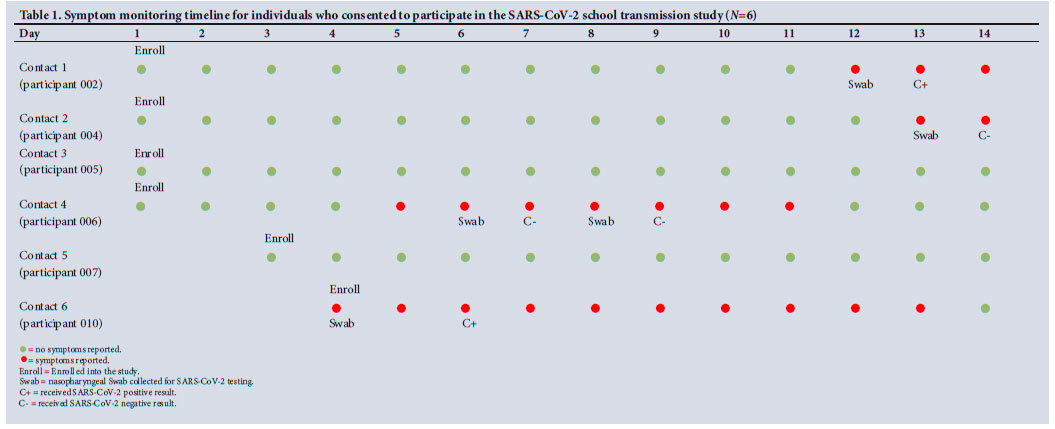
Two guardians declined participation on behalf of their children when contacted by the consent team, and a learner and a teacher did not respond to emails or telephone calls from the consent team at any time during the study period (more than three attempts were made). The remaining six close contacts provided consent/assent at staggered intervals. These close contacts completed symptom monitoring calls from the NICD SAFETP team every day from day of consent until the end of the 14-day study period (Table 1).
Descriptive details of index case and close contacts
The index case and six close contacts were assigned as female at birth and lived at home with their families. The index case was aged 17 years and presented with no underlying medical conditions. Among the six close contacts, four were aged 17 years and two were 18 years old, with one reporting an underlying condition of asthma and one of obesity. The index case and all the close contacts reported using their own family transport to travel to school. All had received the Pfizer vaccine, with the index case and four close contacts reporting receipt of a single dose, and two contacts reporting receipt of two doses.
SARS-CoV-2 positivity and secondary attack rate
The index case reported having a headache, sore throat, nausea and vomiting, myalgia, diarrhoea and fatigue. Of the six close contacts who were monitored for symptoms, four reported symptoms, and specimens were collected on the same or subsequent day they presented with symptoms. Symptoms were reported between day 4 and day 14 (13 - 23 March 2022), with symptom duration ranging from 2 to 10 days. The most common symptoms reported among the close contacts include headache (4/4), sore throat (4/4), cough (4/4) and fatigue (3/4). Of the four individuals who were swabbed, two were positive for SARS-CoV-2, while the other two tested negative for SARS-CoV-2. One learner was swabbed twice as the first SARS-CoV-2 result was negative, but symptoms persisted. The second test was also negative for SARS-CoV-2.
The SAR was 2/11 (18.18%) of all close contacts who were at risk of infection, 2/4 (50.0%) of all those close contacts who developed symptoms, and 2/4 (50.0%) of all those close contacts who developed symptoms and were tested for SARS-CoV-2. During the same period, the school reported that 9 of the 926 learner body tested COVID-19 positive (0.97%).
Sequencing of positive specimens
Both specimens underwent genotype sequencing at the UCT Virology Laboratory and were confirmed as the BA.2 sublineage of the Omicron variant. However, the sequence homology does not support the two as part of the transmission cluster.
Adverse events
A learner who underwent nasopharyngeal swab collection at home collapsed and lost consciousness immediately after the procedure. The learner recovered consciousness within a minute after her parents placed her on her back and elevated her feet. The family reported that similar episodes had taken place in the past, most recently during her COVID-19 vaccination. The incident was reported to the Co-PI, and a written report was submitted to the SAB within the stipulated 48 hours, with the event classified as a probable vasovagal syncopal episode in the presence of a trigger event. The SAB agreed that it was the likely diagnosis and that no changes were required to current study safety procedures. The learner accepted the opportunity to receive a social worker assessment and counselling after disclosure of ongoing anxiety following the event. This was arranged, but the learner later reported that their anxiety had resolved and no longer required social worker intervention.
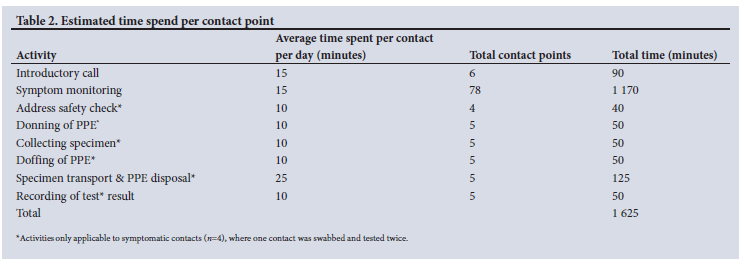
Contact tracing time
Table 2 records the estimated time required per individual contact informed by the SAFETP time-logs. Total hours spent conducting monitoring for six learners was 27 hours, with each learner requiring approximately 4.5 hours of contact time during the study period.
School environmental assessment
A SAFETP team member and the study co-PI observed nine classrooms on the school grounds and noted that they were adequately ventilated with a floor space of 1 m2 for each learner. There were several outdoor play areas, and outdoor wooden benches were available for seating, as well as tables and chairs provided for lunch seating.
There were separate classrooms available for each grade. The newer classrooms (n=8) could accommodate approximately 15 learners with distancing of 1 m2 between desks. The desks in newer classrooms were wider to accommodate two learners per desk, but were limited to one learner per desk under the 1 m2 social distancing guidelines. The older classrooms were able to accommodate 30 learners with 1 m2 distancing between single-user desks.
The school did not have a designated sick bay for isolation of sick learners. Learners presenting with symptoms were isolated in the front office waiting/reception area. While the space was large, it was indoors and could only accommodate a limited number of learners while employing social distancing, and there was no designated space for ill learners to lie down or rest in a supine position.
There were toilet blocks for learners situated throughout the school, with each toilet block containing 10 - 12 separate toilet stalls and hand-washing facilities with hot and cold water located inside the block. In order to minimise crowding or queueing to access the toilets, learners were encouraged to use any of the available toilets around the school grounds, as opposed to using the toilet most closely located to their classroom. All ablution facilities had 70% alcohol hand sanitisers, soap and running potable water. Toilet facilities were well ventilated with no detectable odours present. There were separate toilets designated for staff members and visitors to use.
During the environmental assessment, every school person observed in the corridors or classrooms was noted to be wearing a mask.
Discussion
Our pilot study demonstrated the potential feasibility of conducting active surveillance and contact tracing in the school environment if resources permit. However, such intensive engagement required dedicated field epidemiology teams and close partnerships with school authorities and communities. It proved time-consuming, with an average of 4.5 hours per contact followed up over a 2-week period, and is unlikely to be sustainable at scale. The secondary attack rate in those contacts who had symptoms and underwent swabbing was high at 50%, but may be at risk of selection bias due to the very low response rate.
We postulate multiple reasons for the small sample in our study. Firstly, the index case was infectious at school on a Friday, when no lessons were longer than 45 minutes. According to our inclusion criteria, we would consider all learners as close contacts in a classroom where attendance was for <2 hours. Secondly, the elimination of quarantine immediately prior to the conduct of our study resulted in little incentive for learners to participate in the study. Thirdly, reduction of disease severity due to vaccination and acquired immunity may have led to significant changes in the school community's perception of the need to test and isolate for COVID-19 (so-called COVID-19 fatigue). The secondary attack rates observed in our small sample can therefore not be considered generalisable or indicative of COVID-19 transmission in schools.
Timeous identification of close contacts of an index case is key to successful outbreak control. Our study attempted to mirror an operational outbreak response when additional dedicated teams are deployed to assist local health authorities responding to a disease cluster in a closed setting. We achieved this by working closely with the relevant health facilities and the Department of Education to identify operational constraints in advance of the study. Notification of the index case was received from the school approximately 16 hours after laboratory results were first available. Identification and engagement of close contacts was delayed by the interpretation of POPIA in the school environment, which would arguably not apply under a real-world outbreak investigation conducted according to the NMC Act. Nevertheless, tracking and documenting delays between laboratory reporting and outbreak response highlights the urgent need to better integrate laboratory reporting into a surveillance system that includes schools as a key focal point for monitoring disease. Inclusion of the name of a child's school on the laboratory form would allow immediate identification of school-based cases and possible clusters as they arise in real time, triggering an outbreak response when necessary.
Our study was informed by a 2020 school-based active contact tracing study conducted in New South Wales (NSW), Australia, in which all laboratory-confirmed cases in schools were identified via the NSW Notifiable Conditions Information Management System.[13] Their close contacts were monitored at home under quarantine conditions, and an enhanced surveillance component of the study tested both symptomatic and asymptomatic contacts. Unlike our study, this study was large and included 15 schools and monitored 1 448 close contacts over a 3-month period. It was commissioned by the NSW Department of Health under operational conditions to inform their school closure policy. Given the deleterious effects of lengthy school closures on children, we argue that in SA, attention should be given to investment in systems to signal and monitor epidemic trends in schools in order to keep schools maximally and safely open, alongside ongoing advocacy for provision of the most basic tools for prevention and control of disease in the school environment, including adequate water and sanitation.
Our study methods proved robust and confirmed the feasibility of conducting a larger research study in the school environment. However, greater utility for similar operational efforts would have been achieved if we had costed each component of the contact trace and testing process. Our study methodology shares similar limitations to other school-based studies identified in the global systematic review, in which few have comparator arms and many are limited by selection bias.[1] Ideally, we would have tested all asymptomatic close contact learners, and conducted comparative analysis to add to the evidence base regarding sub-clinical infection. This remains a research gap in the school and paediatric literature. Researchers active in the school space may wish to consider developing an ethically-approved protocol template in advance of future novel pathogen epidemics to address these gaps, such as has been advocated for Ebola vaccines.[14] Close collaboration with government educational and health authorities remains key to future success.
Conclusion
This is the first SA school-based COVID-19 transmission study. We believe it opens a discussion about future school surveillance and how this can be optimally facilitated by supportive legislation and enhanced laboratory systems. The potential protective role that schools play in preventing disease when appropriate and adequate non-pharmaceutical interventions are in place remains unanswered. A large, adequately powered comparative study of COVID-19 transmission in schools v. communities may yet be required dependent on the unfolding nature of successive COVID-19 waves in SA. Future national discussions regarding pathogen prevention and control must consider the role of schools and school-based active and passive surveillance. As such, our findings have implications beyond COVID-19.
Declaration. None.
Acknowledgements. We are grateful to the following: All learners and their families who participated in the study. All schools who agreed to initial recruitment and the staff and community of the participating school. The Western Cape Education Department who agreed to partner with us. Prof. Carolyn Williamson and Prof. Wolfgang Preiser who contributed to the protocol and facilitating access to virological sequencing. Members of the SAB: Mr Oscar Apollis (chair), Ms Carina Dickson, Dr Feizal Majiet, and Dr Tim Tucker. Dr Hassan Mahomed, Dr Katie Murie and Ms Fathima Jacobs of Western Cape Department of Health who facilitated logistics in the facility. Drs Lindy Dickson and Nasreen Allie who assisted with linkages to schools and provided helpful guidance. We thank Ms Liezl Moodie and Ms Nomvuyiso Sirayi for translation and managing the consent and assent processes with such dedication. Addition to the acknowledgement: Dr Ziyaad Valley-Omar and Mr Arash Iranzedeh for assistance on interpretation of molecular epidemiology. We are grateful to Prof. Kristine Macartney of the Australian National Centre for Immunisation Research and Surveillance in Sydney who shared her school study protocol with us and to Dr Jakob Armann of University Children's Hospital in Dresden who shared his protocol, both of which informed our thinking.
Author contributions. NS, AdV and CM developed the protocol with input from LK, MH, CW, and WP. NS and AdV conducted case and close contact identification and AdV and TM conducted the school environmental assessment. JY developed the technical study tools and provided database support. KJ, HM and CM provided guidance and support to the study and JY, TM, MM and FE conducted the monitoring and sampling. HM and CW conducted tests and sequencing. AdV conducted analysis and NS wrote the draft manuscript with all authors contributing to the final manuscript and approving it for publication.
Funding. This study was funded by the SAMRC and in-kind support was provided by the NICD SA Field Epidemiology Training Programme. Testing was provided by the University of Cape Town in terms of the shared agreement between the university and the Western Cape Department of Health. The viral genomic sequencing and analysis is supported by Wellcome Trust.
Conflicts of interest. None.
References
1. Xu W, Li X, Dong Y, et al. SARS-CoV-2 transmission in schools: An updated living systematic review (version 2; November 2020). J Glob Health 2021;11:10004. https://doi.org/10.7189/jogh.11.10004 [ Links ]
2. Krishnaratne S, Littlecott H, Sell K, et al. Measures implemented in the school setting to contain the COVID-19 pandemic. Cochrane Database Syst Rev 2022;1(1):CD015029. https://doi.org/10.1002/14651858.CD015029 [ Links ]
3. Walsh S, Chowdhury A, Braithwaite V, et al. Do school closures and school reopenings affect community transmission of COVID-19? A systematic review of observational studies. BMJ Open 2021;11(8):e053371. https://doi.org/10.1136/bmjopen-2021-053371 [ Links ]
4. South Africa. National Health Act No. 61 of 2003. [ Links ]
5. Morifi M, Malevu N, Odayan S, McCarthy K, Kufa T. Congenital syphilis case surveillance in South Africa 2017 - 19: Experience, challenges and opportunities. J Trop Pediatr 2021;67(4):fmab079. https://doi.org/10.1093/tropej/fmab079 [ Links ]
6. Department of Basic Education, South Africa. Standard Operating Procedure for the containment and management of COVID-19 for schools and communities (September 2020). https://www.education.gov.za/Resources/Publications.aspx (accessed 20 May 2022). [ Links ]
7. Department of Basic Education, South Africa. Standard Operating Procedure for the containment and management of COVID-19 for schools and communities (February 2022). https://www.education.gov.za/Resources/Publications.aspx (accessed 20 May 2022). [ Links ]
8. Lenkokile R, Hlongwane P, Clapper V. Implementation of the integrated school health policy in public primary schools in region C, Gauteng Province. Afr J Public Affairs 2019;11(1):196-211. [ Links ]
9. Rasesemola RM, Matshoge GP, Ramukumba TS. Compliance to the Integrated School Health Policy: Intersectoral and multisectoral collaboration. Curationis 2019;42(1):e1-e8. https://doi.org/10.4102/curationis.v42i1.1912 [ Links ]
10. Janse van Rensburg AP, Rau A. Assessing the implementation of the Integrated School Health Programme (ISHP) in anonymised local municipality, Free State Province. Bloemfontein: Centre for Health Systems Research & Development, 2017. [ Links ]
11. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform 2019;95:103208. https://doi.org/10.1016/j.jbi.2019.103208 [ Links ]
12. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42(2):377-381. https://doi.org/10.1016/j.jbi.2008.08.010 [ Links ]
13. Macartney K, Quinn HE, Pillsbury AJ, et al. Transmission of SARS-CoV-2 in Australian educational settings: A prospective cohort study. Lancet Child Adolesc Health 2020;4(11):807-816. https://doi.org/10.1016/s2352-4642(20)30251-0 [ Links ]
14. Heymann DL, Rodier GR, Ryan MJ. Ebola vaccines: Keep the clinical trial protocols on the shelf and ready to roll out. Lancet 2015;385(9980):1913-1915. https://doi:10.1016/S0140-6736(15)60645-6 [ Links ]
 Correspondence:
Correspondence:
N Siegfried
nandi.siegfried@mrc.ac.za
Accepted 9 February 2023


{kind=link}
{kind=link}