










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 no.5 Pretoria may. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i5.666
CME
Approach to the diagnosis and management of snakebite envenomation in South Africa in humans: Layperson aspects and the role of emergency medical services
T C HardcastleI, II, III; M KajeeIV; K LachenichtV; N van der WaltVI
IMMed, PhD; Trauma and Burns Service, Inkosi Albert Luthuli Central Hospital and KwaZulu-Natal Department of Health, South Africa
IIMMed, PhD; Department of Surgical Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IIIMMed, PhD; National Snakebite Advisory Group, Durban, South Africa
IVDip Trauma Nursing; South African Snakebite Symposium Organising Committee, Gauteng, South Africa
VMSc, HSc (EMC); Rocket Helicopter Emergency Services, Germiston, South Africa
VIBTech (EMC); Access Professional Development, Vereeniging, South Africa
ABSTRACT
Snakebites occur in the community, not in the Emergency Unit. As such it is important to understand the first-aid concepts and pre-hospital emergency care aspects of this neglected disease. This article will highlight the concepts for emergency care within the context of the current pre-hospital arena and in light of the recent South African Snakebite Symposium consensus meeting held in July 2022, where wilderness rescue, emergency medical services and other medical participants agreed through evidence review and consensus debate on the current best approaches to care of the snakebite victim outside the hospital environment.
South Africa (SA) has over 170 species of snakes, but of these, around 20 comprise the 'dangerous and deadly' category. Regarding management of snake envenomation, the World Health Organization (WHO) Africa document is now more than 10 years old, covers aspects of management that are not specific to SA and mentions treatment options that may no longer be accepted or available.[1]
This paper focuses on the human treatment guidelines to be used by the layperson when confronted with a snakebite and the role of the emergency medical services in emergency care and transport of the snakebite victim. What we mean by the layperson is the nonprofessional 'first-aider' level.
Snakebites occur in one of two distinct scenarios, which are categorised as legitimate and illegitimate: so-called legitimate bites occur where a person unintentionally and unknowingly provokes a venomous snake (e.g. stepping on a snake while out walking), while illegitimate bites occur when someone sees a snake and then tries to catch, kill or otherwise interact with it and is bitten. The latter bites are typically seen in snake owners, breeders or snake-removers who are intentionally interacting with often the more venomous species.[2]
Most of what is recommended in the care of snakebite is largely expert opinion based on retrospective data, with little or no randomised or prospective studies available on the treatment of snake envenomation in this country. The article aims to provide the current best evidence and best practice information for the benefit of every SA citizen. The attached flip-chart addressing the level of care aims to provide a pocket-friendly resource for the layperson and the emergency medical services (EMS) practitioner.
Layperson role
The layperson who assists a snakebite victim is encouraged to move the victim to safety away from the snake. The victim should be moved as minimally as possible, washing away excess venom and marking the bite-site, but not engaging in the use of cutting, sucking, electrocuting or amputating the wounded area. Tourniquets are actively discouraged, with the designated exceptions of cape cobra or black mamba bites in cases where more than a 90-minute delay to emergency care is expected (wilderness environment). These specific bites should rather have tight pressure bandages applied over a broad area proximal to the bite site (e.g. wrist to elbow for a hand bite), or commercial-type tourniquets applied, rather than improvised tourniquets, although these are not strongly advocated.
A list of whom to contact for advice and evacuation is supplied (emergency numbers) on the flip-chart (Fig. 1).[3] Flow-charts provide emergency life-saving support advice (breathing support and cardiopulmonary resuscitation) and basic first aid using the syndromic approach, rather than reliance on snake identification. If it is possible to photograph the snake, this is advised, rather than risking an illegitimate bite while trying to catch the snake. From a wound management perspective, pressure bandaging and immobilisation for suspected neurotoxic bites and limb mobilisation for suspected cytotoxic bites are detailed, in line with newer evidence showing less cytotoxicity if mobility is maintained.
To ensure that laypersons can quickly access and follow a safe care pathway, an 8-page share-ware flipchart was designed for widespread public distribution, partially illustrated in Fig. 1.[3]
Emergency medical service role
While the main role of the EMS is patient access, stabilisation, extrication and urgent evacuation to an appropriate definitive care facility, there are aspects of the EMS clinical practice guidelines (CPGs) that are affected by the envenomation syndromes, and as such, it is important to highlight to EMS the essential adjustments to be considered when treatment of snake envenomation is undertaken.[4]
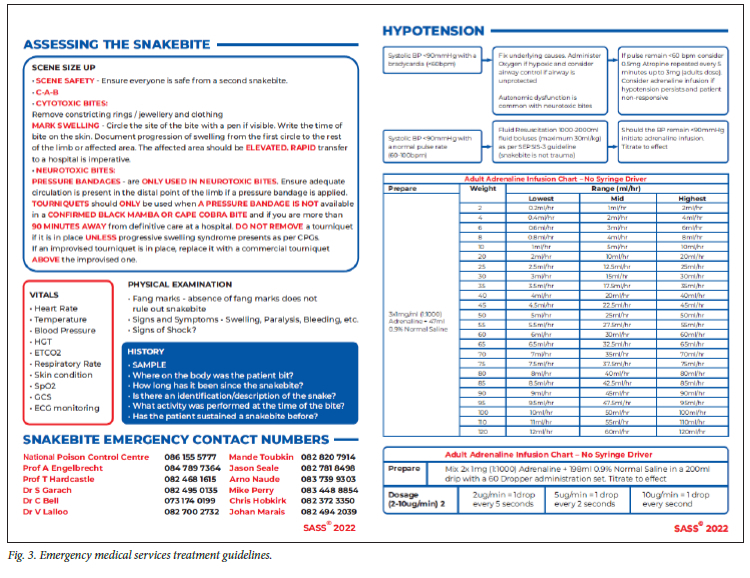
Aspects of scene safety, relevant historic information and the essential minimum vital signs are emphasised. Important physical examination aspects for documentation of bites and related physiology or pathology are listed. Removal of rings and other tight circumferential items is encouraged. The care provider is instructed to circle the site of the bite with a marking pen if visible, and record the time of bite on the skin. Progression of swelling from the first circle to the rest of the limb or affected area should be recorded at least every hour. The affected area should be elevated, if possible, at least to the level of the heart, and then rapid transfer to a hospital with access to monitoring and antivenom is imperative.
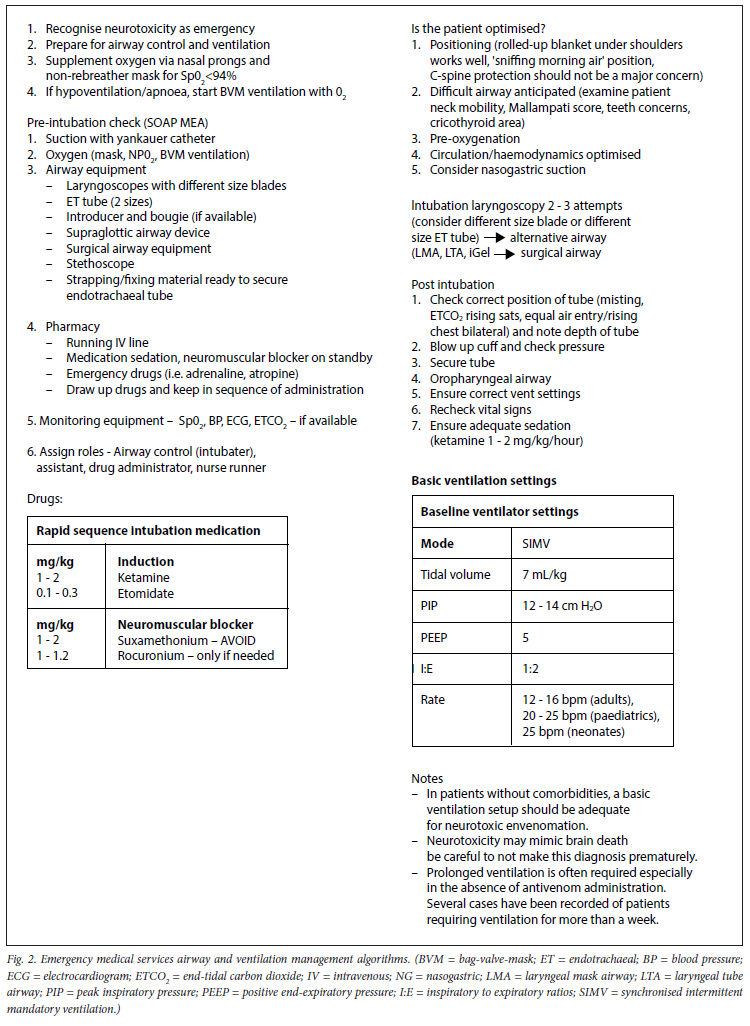
For care on the way to a receiving facility, management algorithms for airway control, breathing and hypotension are provided. For airway and breathing considerations, the risk of respiratory depression due to respiratory muscle paralysis is great in neurotoxic bites. Bag-valve-mask ventilations are advised for respiratory depression until intubation can be safely performed. Respiratory depression can be potentiated by opioids, by potentiating certain venom components, so ketamine is advised both for intubation and analgosedation in transit. Etomidate is a suitable alternative for induction. See Fig. 2 for a practical airway and ventilation management algorithm.
Since the majority of cases that require airway support and ventilation are neurotoxic bites that cause respiratory paralysis, it is advised to use no, or reduced-dose, paralytic agents and to avoid suxamethonium in this circumstance, with rocuronium as the paralytic of choice if any is used. Suxamethonium should be avoided since it has many overlapping effects accentuating those of the pre-synaptic venoms (fasciculins and dendrotoxins) of the black mamba and may lead to bradycardia or a prolonged paralysis.
With hypotensive patients the consensus group emphasises that the fluid therapy is not restrictive, but rather more in line with the 'surviving sepsis' values of up to 30 mL/kg using a balanced salt solution.[5] Should the patient still elicit signs of hypoperfusion, then adrenaline infusions are advised. Tranexamic acid (TXA) should not be given[6] (confirmed by Prof. David Warrel, WHO Expert antivenom group - personal communication).
For neurotoxic bites compression bandages only are advised in transit - this is to avoid the unnecessary use of the tourniquet, unless already in place, in which case this is left in place for safe removal at the receiving hospital, where a potential venom rush can be managed.[7] Since commercial tourniquets are included in the CPGs, inappropriate use should be discouraged. Adequate distal perfusion, however, takes priority over a tight bandage. All this information is summarised in an 8-page flipchart that is partially illustrated in Fig. 3.[8]
The flipcharts also illustrate the common venomous snakes and give a general idea of their distribution; however, this may vary, and snakes can be found outside the listed areas due to migration or captivity.
Conclusion
Laypersons and EMS providers are often the first contact that the snakebite victim has with any form of care-provider, and as such, it is better to know the basics and undertake these steps safely to ensure the patient arrives at the emergency department in a timely fashion with the best possible degree of resuscitation based on current best evidence.
Declaration. None.
Acknowledgements. We acknowledge the support of the professional societies and certain non-governmental organisations in the organisation of the SASS meeting.
Author contributions. Equal contributions.
Funding. None.
Conflicts of interest. None.
References
1. World Health Organization Africa Office, Sambo LG. Foreword. In: Guidelines for the prevention and clinical management of snakebite in Africa. Brazzaville: WHO, 2010. [ Links ]
2. Curry SC, Horning D, Brady P, Requa R, Kunkel DB, Vance MV The legitimacy of rattlesnake bites in central Arizona. Ann Emerg Med 1989;18(6):658-663. https://doi.org/10.1016/s0196-0644(89)80523-2 [ Links ]
3. South Africa Snakebite Symposium. Layperson Flipper. Nelspruit: SASS, 2022. [ Links ]
4. Health Professions Council of South South Africa Professional Board for Emergency Care. Clinical Practice Guidelines. Pretoria: HPCSA, 2018. https://www.hpcsa.co.za/Uploads/EMB/CLINICAL%20PRACTICE%20GUIDELINES%20%20-%20PROTOCOLS-%20JULY%202018.pdf (accessed 1 November 2022). [ Links ]
5. Evans L, Rhodes A, Alhazzani W, et al. Executive summary: Surviving Sepsis Campaign: International Guidelines for the Management of Sepsis and Septic Shock 2021. Crit Care Med 2021;49(11):1974-1982. https://doi.org/10.1097/CCM.0000000000005357 [ Links ]
6. Müller GJ, Modler H, Wium CA, Veale DJH, Marks CJ. Snake bite in southern Africa: Diagnosis and management. CME 2012;30(10):362-382. [ Links ]
7. Pelle RP, Engelbrecht A, Lalloo V. Case report: Safe tourniquet removal in black mamba (Dendroaspis polylepis) bites. Am J Trop Med Hyg 2021;106(1):338-341. https://doi.org/10.4269/ajtmh.21-0374 [ Links ]
8. South Africa Snakebite Symposium. Emergency care provider flipchart. Nelspruit: SASS, 2022. [ Links ]
 Correspondence:
Correspondence:
T C Hardcastle
hardcastle@ukzn.ac.za
Accepted 28 March 2023


{kind=link}
{kind=link}
{kind=link}