










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 no.3b Pretoria mar. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i3b.16851
RESEARCH
'Listen to my heart': Qualitative researchers and people living with rheumatic heart disease collaborate to direct future RHD research
C ReadI; A MitchellII; TD JohnsonIII; ME EngelIV; O MatshabaneV; I SsinabulyaVI; A ScheelVII; T ErioVIII; J LawrensonIX, X; S PerkinsXI; J de VriesXII, XIII; L ZühlkeXIV, XV, XVI
IPhD; Telethon Kids Institute, University of Western Australia, Perth, Australia
IIPhD; Charles Darwin University, Darwin, Australia
IIIBIntlDev MCHMED; Telethon Kids Institute, University of Western Australia, Perth, Australia
IVMPH PhD; Department of Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
VPhD; Department of Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
VIMD; Uganda Heart Institute, Kampala, Uganda
VIIMD; Children's National Health System, Washington DC, USA
VIIIMPH; Mwanza Intervention Trials Unit, National Institute for Medical Research, Mwanza, Tanzania
IXMB ChB MMed; Department of Paediatrics, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, Cape Town, South Africa
XMB ChB MMed; Division of Paediatric Cardiology, Department of Paediatrics, Red Cross War Memorial Children's Hospital, Faculty of Health Sciences, University of Cape Town, South Africa
XIMX; Department of Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
XIIDPhil Oxon; Department of Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
XIIIDPhil Oxon; NeuroScience Institute, University of Cape Town, South Africa
XIVMB ChB PhD; Department of Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
XVMB ChB PhD; Division of Paediatric Cardiology, Department of Paediatrics, Red Cross War Memorial Children's Hospital, Faculty of Health Sciences, University of Cape Town, South Africa
XVIMB ChB PhD; South African Medical Research Council, Tygerberg, Cape Town, South Africa
ABSTRACT
BACKGROUND: Rheumatic heart disease (RHD) is a preventable chronic cardiac condition that causes over 350 000 deaths annually, largely in low and middle-income countries, as a direct result of structural inequalities and inadequate access to comprehensive healthcare. People living with and affected by this disease are a key stakeholder group and need to be directing research priorities
OBJECTIVE: To improve care and provide direction for future research, a group of qualitative researchers and pe living with RHD from six countries convened in Cape Town in 2016
METHODS: People with RHD shared their lived experiences while RHD researchers, clinicians and advocates presented a spectrum of qualitative research methods to explore these experiences. The Continuum of Care© (CoC, developed by the Medtronic Foundation) was used as a framework to guide participant discussions. Thematic summaries of the discussions were undertaken in an iterative process throughout the workshop
RESULTS: Three themes emerged in the summaries: there is no 'typical' patient journey; a biomedical focus on RHD does not reflect people's lived experiences; and a diversity of research methods is required to investigate experiences of people living with RHD
PRACTICE IMPLICATIONS: Qualitative research methods are invaluable for allowing patient 'voices' to be heard. To this end, qualitative approaches should be incorporated in all RHD research to ensure maximum benefit for patients
CONCLUSION: Greater understanding of the patient journey was gained for strengthening and expanding the global RHD research agenda. Future research should reflect on and incorporate the realities of patients' lived experiences, and these experiences should be integrated into healthcare models for chronic conditions
In recent years, there has been considerable focus in RHD research on epidemiology and burden of disease, laboratory-based studies into human genetic susceptibility, and immunology.[1-7] Although the importance of the 'patient voice' has been progressively acknowledged,[7,8] relatively few studies include a focus on people with the disease and their lived experiences.[9] Qualitative research - such as ethnographic studies, participatory action research and lived experience studies - examines social issues and seeks explanations into the 'how and why' of people's behaviour and their understanding of their medical conditions.[10] The inclusion of qualitative methods better informs all research on RHD and has potential to inform improved care practices and care models.[11]
The critical need to integrate a broader perspective in RHD research prompted this first workshop of researchers proficient in qualitative methods and people living with RHD in Cape Town, South Africa on 12 September 2016.[12] With a strong focus on hearing patients' narratives, the workshop provided a networking opportunity and a forum to share experiences of living with RHD, and of RHD research. The workshop facilitated the formation of a group of mixed-methods researchers who are committed to ongoing qualitative research to strengthen global knowledge and insight around living with RHD and thereby improve care.
Objective
To improve care by learning from patients about their experiences of living with RHD; to inform an agenda for future research through discussion on the contribution and significance of qualitative research in building global knowledge around RHD; and to consider methods to enhance qualitative research on RHD. This paper reports on the main outcomes of the collaborative workshop between researchers and patients.
Methods
Participants
The researcher and patient workshop had global participation, with attendees from South Africa, Uganda, Tanzania and Australia, as well as representatives from the World Heart Federation, Switzerland and Children's HeartLink, USA. A range of disciplinary backgrounds was incorporated in the workshop. Attendants included five academics/ clinicians; one epidemiologist/microbiologist; three social scientists; four PhD students in the social sciences; one nurse/healthcare worker; and seven representatives of RHD advocacy organisations. One advocate had grown up with congenital heart disease and meaningfully contributed in terms of the shared experience of being a patient with heart disease. Most importantly, the workshop included five people living with RHD from rural and urban areas of South Africa and Uganda, one of whom is also a nurse. These participants had travelled to Cape Town for an annual event for people living with RHD named 'Listen to my Heart'; co-organised by RHD Action and the University of Cape Town to strengthen patient empowerment and advocacy by including, recognising and celebrating the RHD patient community.[13] After the patient event, the attendees participated in the researcher and patient workshop. A total of 26 people took part in the workshop.
Framework for workshop discussions
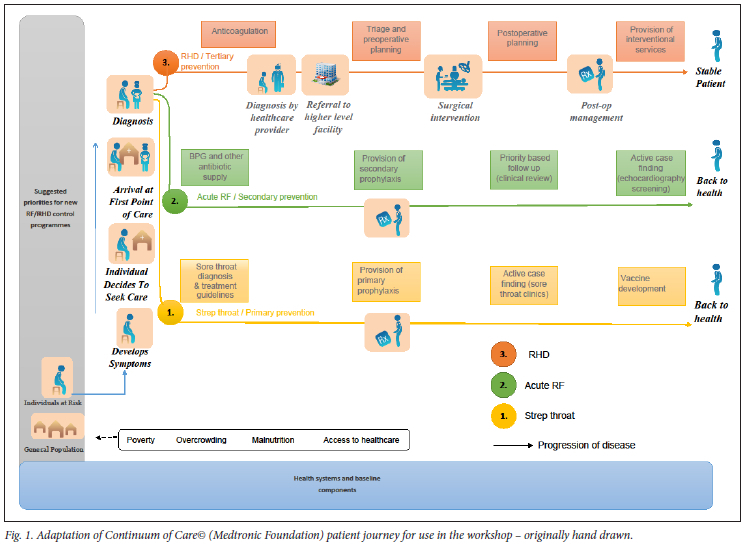
The CoC is a patient-centred framework developed by the Medtronic Foundation. It has been utilised for a range of medical conditions, including RHD, to track 'the movement of a hypothetical patient at risk of or affected by RHD through the health system.'[14] The workshop commenced with dialogues on the 'typical' patient pathway for RHD using a hand-drawn linear version of the CoC adapted especially for use in the workshop (Fig. 1).[14,15] The CoC stimulated discussions on the various points at which a person may enter the healthcare system, barriers that might prevent people from accessing care, and opportunities that exist to address gaps in the healthcare system for people to regain stable health.
Data collection
Five people living with RHD shared their experiences and personal health narratives in response to the CoC pathway in an interactive process within the group. Clinicians reported their experiences of caring for people living with RHD, particularly in relation to the CoC pathway, while one clinician also shared personal experiences of needing cardiac care. Researchers presented their experiences of conducting qualitative research on RHD topics. A broad range of methodologies was shared: from traditional qualitative methods using focus groups and in-depth interviews, through ethnographic research, case studies, use of media and participatory action research. As the meeting evolved, emerging insights were frequently summarised, presented and discussed to gain consensus with the entire group in an iterative process.
Detailed notes were taken throughout the meeting. Together, the summaries and notes were used to develop the contents of this meeting report.
Ethical considerations
This is a meeting report and as such no ethics approval was secured. Where the perspectives of patients are presented in the paper, we have ensured that they are not identifiable in any way. Where names are used, these are pseudonyms. All attendees gave permission for the paper.
Results
Thematic summary of the workshop
Three themes emerged in the discussions at the meeting: there is no 'typical' patient journey; a biomedical focus does not reflect people's real-life experiences of their condition; and diverse research methods are required to investigate the experiences of people living with RHD.
There is no 'typical' patient journey
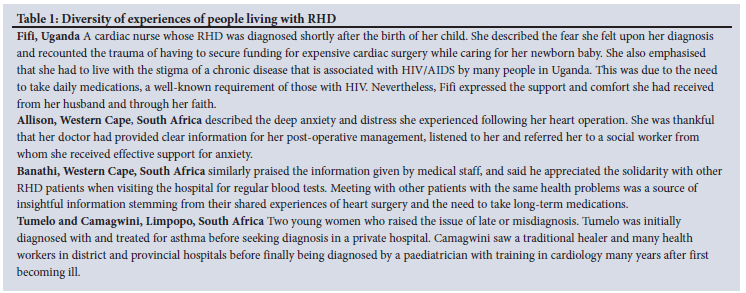
The biological disease pathway for RHD is universally recognised. After group A streptococcal infection, a susceptible person may develop rheumatic fever, which may go on to cause permanent damage to the heart, termed rheumatic heart disease. Cardiac valve repair or replacement surgery may then be required for survival. However, each participant living with RHD at the workshop experienced a different path to diagnosis, treatment and ongoing management. Table 1 outlines the experiences of people from Uganda and South Africa living with RHD.
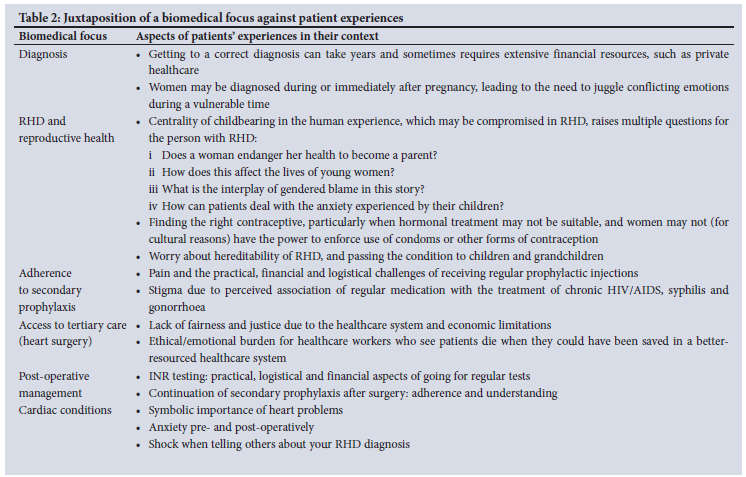
A biomedical focus does not reflect people's real-life experiences
A key outcome was agreement among participants on the need to expand the CoC model to better reflect the reality of patients' lives. This should include consideration of social, psychological and emotional factors, such as stigma and similar experiences that are not currently captured in the CoC model. People living with RHD emphasised the importance of various aspects of their lives. The group outlined the following aspects that should be considered: the impact of RHD on the chances of finding a partner; on the ability of female patients to have children; on patients' ability to find and maintain employment; the burdens imposed by regular clinic visits; and fear associated with heart surgery in the case of South African patients. These aspects were identified as central in patients' journeys. While each patient's interaction with the healthcare system is an individual experience, it was collectively agreed that an integrated approach to RHD management and care is needed. This involves ensuring a strong social support network; providing psychological and counselling support; creating patient support groups and other coping strategies; and recognising religious beliefs as a source of comfort and strength. A non-biomedical perspective recognises the impact of these factors on RHD health outcomes. Inequality, poverty, disempowerment, crowded housing and poor hygiene are influential in all components of the CoC model. These socioeconomic factors impact on the entire CoC model and affect health outcomes and should be integrated into the design of RHD prevention strategies within healthcare systems.
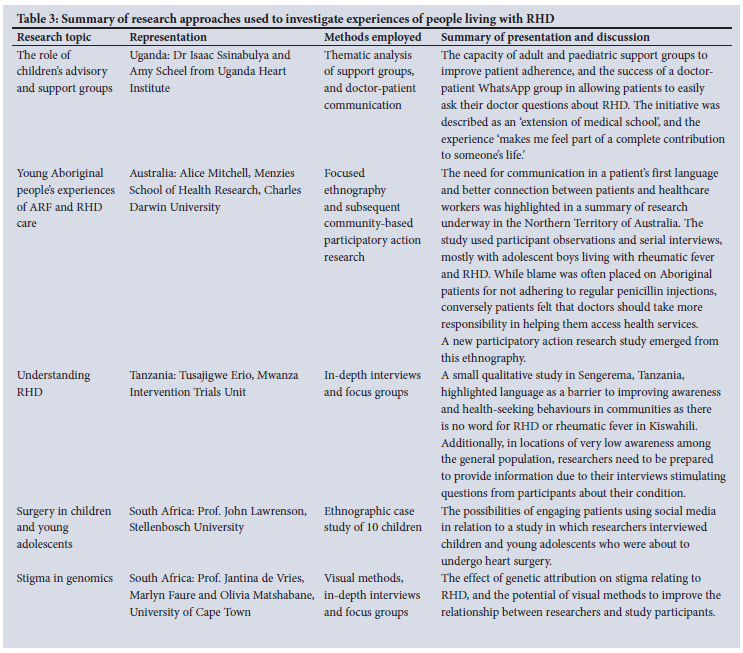
A range of research methods is required to investigate the experiences of people living with RHD
The workshop group recognised the need to draw on and integrate the broad diversity of methods that can assist in the investigation of experiences of people living with RHD. During the workshop, examples across a broad range of RHD qualitative research methods were presented. These are summarised in Table 3.
Discussion
Research in recent decades has had an increased focus on care models for chronic disease management due to the escalation in chronic conditions globally and the resultant increasing demand on healthcare systems.[16-19] Additionally, there has been a desire to improve practices by using alternative care models including integrating and leveraging off care models for other chronic conditions, such as tuberculosis, HIV and RHD.[20] There has been a corresponding emphasis on and acceptance of the need for patient-centredness in healthcare.[21] While care models are useful for providing an overall framework for practice and for planning and resourcing healthcare systems, they can be greatly enhanced if they are informed by patients' multifaceted experiences as 'expert witnesses' on health conditions.[22,23] The results reported here highlight that conducting collaborative qualitative research with people living with the chronic condition of interest, is critical for gaining insight into and enhancing chronic care models, and therefore patient care. This sentiment is expressed in the statement encapsulating the Listen to My Heart events in South Africa, 'Nothing about me without me.'[13]
The CoC framework aptly presents a stylised patient journey on the topic of RHD to inform healthcare system design for a global audience.[15] However, patients' narratives, presented in our workshop data, build an informed understanding of patient journeys and have potential to improve care by ensuring that the experiences of people with the conditions are known; for instance, while a patient is depicted in the model as having symptoms that lead to care-seeking and then to diagnosis, patient experience is that it may take years and much effort to receive a correct diagnosis, or a diagnosis may be missed and only revealed traumatically during pregnancy or childbirth. We argue that qualitative research methods should be prioritised for building global knowledge around patients' lived experiences of RHD.
A range of qualitative research methods can be used to explore multiple components on the patient journey of people living with RHD as depicted in the CoC model. However, more importantly, these methods have the capacity, and provide an opportunity, to modify the predilection to a purely biomedical approach in healthcare systems on the part of clinicians and researchers. Through revealing the deeper human experiences of both clinicians and researchers on the one hand, and people living with the condition in question on the other, development of an integrated approach to RHD care is made possible.
Setting a research agenda for RHD involves a commitment to ensuring people living with RHD are fully involved in project design and implementation, and have an opportunity to share their experiences. We recommend:
• People living with RHD be included on committees setting RHD research agendas;[22]
• All RHD research proposals, including biomedical and screening studies, have a component devoted to engaging people living with RHD, and social research investigating their experiences. We proffer that even laboratory-based projects, due to their nature, are not necessarily excluded from the possibility of incorporating qualitative components;
• Monitoring and evaluation mechanisms be included in all RHD studies;
• Research results are disseminated (first) to patients, patient advocacy groups and the broader research community; but also to policymakers and those setting healthcare system priorities and redesign;
• A repository of global research that utilises qualitative methods or qualitative components, including unpublished writings on RHD patient experiences, be collated.
Practice implications
Sociological studies describing the experiences of people living with RHD are scarce, leading to unrecognised limitations in widely adopted care models such as the CoC, as well as limitations in clinicians' knowledge and understanding of patients' experiences. As a priority, nuanced understandings of the non-biomedical patient journey are needed to complement biomedical understandings. This includes, where possible, incorporating qualitative research methods into biomedical studies, thus providing an opportunity to improve healthcare models through revealing deep human experiences so that deeper knowledge can be gained and people living with RHD receive maximum benefit.
Conclusion
The platform for in-depth discussion on RHD care provided in this workshop resulted in valuable information to inform and strengthen supportive healthcare models. Publication of the themes generated in this workshop details our collective commitment to ensuring that the patient voice is at the core of how we tackle RHD globally and for this understanding to complement and inform all research with an RHD focus more broadly.
Declaration.
Acknowledgements. We acknowledge the valuable insight provided by all participants in the Listen to My Heart patient event and workshop, especially those who are living with RHD, or caring for those with RHD.
Author contributions. LZ, CR, JdV and AM conceptualised the paper. CR wrote the first draft. AM completed writing and TJ and AM concluded the final draft. All authors critically revised and approved the final version.
Funding. LZ, SP and TDJ are supported by the Medtronic Foundation grant to RhEACH as part of the RHD Action global partnership. LZ is also supported by the Medical Research Council of South Africa and the National Research Foundation of South Africa. OMB and JdV are supported by the Stigma in African Genomics project, which was supported by Award Number 1 U01 HG008226-01 administered by the National Human Genome Research Institute as part of the NIH Common Fund H3Africa Initiative. JdV was also supported by the RHDGen H3Africa project supported by the Wellcome Trust (WT099313MA).
Conflicts of interest. None.
References
1. Cannon J, Roberts K, Milne C, Carapetis JR. Rheumatic heart disease severity, progression and outcomes: A multi-state model. J Am Heart Assoc 2017;6(3):e003498. [ Links ]
2. Gray LA, D'Antoine HA, Tong SYC, et al. Genome-wide analysis of genetic risk factors for rheumatic heart disease in Aboriginal Australians provides support for pathogenic molecular mimicry. J Infect Dis 2017;216(11):1460-1470. [ Links ]
3. Parks T, Kado J, Miller AE, et al. Rheumatic heart disease-attributable mortality at ages 5-69 years in Fiji: A five-year, national, population-based record-linkage cohort study. PLoS Negl Trop Dis 2015;9(9):e0004033. [ Links ]
4. Rothenbuhler M, O'Sullivan CJ, Stortecky S, et al. Active surveillance for rheumatic heart disease in endemic regions: A systematic review and meta-analysis of prevalence among children and adolescents. Lancet Glob Health 2014;2(12):e717-726. [ Links ]
5. Zuhlke L, Engel ME, Karthikeyan G, et al. Characteristics, complications, and gaps in evidence-based interventions in rheumatic heart disease: The Global Rheumatic Heart Disease Registry (the REMEDY study). Eur Heart J 2015;36(18):1115-1122a. [ Links ]
6. Zuhlke L, Karthikeyan G, Engel ME, et al. Clinical outcomes in 3 343 children and adults with rheumatic heart disease from 14 low- and middle-income countries: Two-year follow-up of the Global Rheumatic Heart Disease Registry (the REMEDY Study). Circulation 2016;134(19):1456-1466. [ Links ]
7. Zuhlke LJ, Engel ME, Remenyi B, Wyber R, Carapetis J, RHD Forum Meeting Report Writing Committee. The Second Rheumatic Heart Disease Forum Report. Glob Heart 2013;8(3):253-261. [ Links ]
8. Carapetis JR, Beaton A, Cunningham MW, et al. Acute rheumatic fever and rheumatic heart disease. Nat Rev Dis Primers 2016;2:15084. [ Links ]
9. Johnson T, Read C, Haynes E, Bessarab D. PT283 A systematic review of the lived experience of rheumatic heart disease of Aboriginal and Torres Strait Islanders in Australia. Glob Heart 2016;11(2):e173. [ Links ]
10. Pope C, Mays N. Reaching the parts other methods cannot reach: An introduction to qualitative methods in health and health services research. BMJ 1995;311(6996):42-45. [ Links ]
11. Huck DM, Nalubwama H, Longenecker CT, Frank SH, Okello E, Webel AR A qualitative examination of secondary prophylaxis in rheumatic heart disease: Factors influencing adherence to secondary prophylaxis in Uganda. Glob Heart 2015;10(1):63-69 e1. [ Links ]
12. RHD Action. RHD Action Participates in 'Listen to my Heart' Patient Event: RHD Action; 2016 [ Links ]
13. Zuhlke L, Perkins S, Cembi S. Rheumatic heart disease patient event: Cape Town hosts 4th annual Listen to My Heart Rheumatic Heart Disease for Patients at the South African Heart Association meeting in 2017. Eur Heart J 2018;39(19):1669-1671. [ Links ]
14. Zuhlke LJ, Watkins DA, Perkins S, et al. A comprehensive needs assessment tool for planning RHD control programs in limited resource settings. Glob Heart 2017;12(1):25-31. [ Links ]
15. Palafox B, Mocumbi AO, Kumar RK, et al. The WHF Roadmap for reducing CV morbidity and mortality through prevention and control of RHD. Glob Heart 2017;12(1):47-62. [ Links ]
16. Coleman K, Austin BT, Brach C, Wagner EH. Evidence on the Chronic Care Model in the new millennium. Health Aff (Millwood). 2009;28(1):75-85. [ Links ]
17. Farre A, Wood V, Rapley T, Parr JR, Reape D, McDonagh JE. Developmentally appropriate healthcare for young people: A scoping study. Arch Dis Child 2015;100(2):144-151. [ Links ]
18. Freed GL, Hudson EJ. Transitioning children with chronic diseases to adult care: Current knowledge, practices, and directions. J Pediatr 2006;148(6):824-827. [ Links ]
19. Hepburn CM, Cohen E, Bhawra J, Weiser N, Hayeems RZ, Guttmann A. Health system strategies supporting transition to adult care. Arch Dis Child 2015;100(6):559-564. [ Links ]
20. Katzenellenbogen JM, Ralph AP, Wyber R, Carapetis JR. Rheumatic heart disease: Infectious disease origin, chronic care approach. BMC Health Serv Res 2017;17(1):793. [ Links ]
21. Wagner EH, Bennett SM, Austin BT, Greene SM, Schaefer JK, Vonkorff M. Finding common ground: Patient-centeredness and evidence-based chronic illness care. J Altern Complement Med 2005;11 Suppl 1:S7-S15. [ Links ]
22. Wyber R, Johnson T, Perkins S, et al. Tools for Implementing Rheumatic Heart Disease Control Programmes (TIPs) Handbook, 2nd Edition. RHD Action. Geneva, Switzerland; 2018. [ Links ]
23. Keir M, Bailey B, Lee A, Kovacs AH, Lucy Roche S. Narrative analysis of adults with complex congenital heart disease: Childhood experiences and their lifelong reverberations. Congenit Heart Dis 2018;13(5):740-747. [ Links ]
 Correspondence:
Correspondence:
L Zühlke
liesl.zuhlke@mrc.ac.za


{kind=link}
{kind=link}
{kind=link}
{kind=link}