










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 no.3b Pretoria mar. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i3b.16830
RESEARCH
The impact of HIV co-infection on presentation and outcome in adults with tuberculous pericarditis: Findings from the IMPI trial
F GumedzeI; S PandieII; J B NachegaIII, IV, V; Z KerbelkerVI; V FrancisVII, *; L ThabaneVIII; M SmiejaIX; J BoschX; S YusufXI; M NtsekheXII; G MeintjesXIII; B M MayosiXIV, *
IPhD; Department of Statistical Sciences, University of Cape Town, Cape Town, South Africa
IIMB ChB, FCP(SA); The Cardiac Clinic, Department of Medicine, Groote Schuur Hospital and University of Cape Town, Cape Town, South Africa
IIIMD, PhD; Department of Medicine and Centre for Infectious Diseases, Stellenbosch University, Cape Town, South Africa
IVMD, PhD; Department of Epidemiology, University of Pittsburgh Graduate School of Public Health, Pittsburgh, PA, USA
VMD, PhD; Departments of Epidemiology and International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA
VIMB ChB; The Cardiac Clinic, Department of Medicine, Groote Schuur Hospital and University of Cape Town, Cape Town, South Africa
VIIRN; The Cardiac Clinic, Department of Medicine, Groote Schuur Hospital and University of Cape Town, Cape Town, South Africa
VIIIPhD; McMaster University and the Population Health Research Institute, Hamilton Health Sciences, Hamilton, ON, Canada
IXMD; McMaster University and the Population Health Research Institute, Hamilton Health Sciences, Hamilton, ON, Canada
XPhD; McMaster University and the Population Health Research Institute, Hamilton Health Sciences, Hamilton, ON, Canada
XIDPhil; McMaster University and the Population Health Research Institute, Hamilton Health Sciences, Hamilton, ON, Canada
XIIMB ChB, PhD; The Cardiac Clinic, Department of Medicine, Groote Schuur Hospital and University of Cape Town, Cape Town, South Africa
XIIIMB ChB, PhD; Wellcome Centre for Infectious Diseases Research in Africa, Institute of Infectious Disease and Molecular Medicine and Department of Medicine, University of Cape Town, Cape Town, South Africa
XIVMB ChB, DPhil (Oxon); for the IMPI trial investigators; The Cardiac Clinic, Department of Medicine, Groote Schuur Hospital and University of Cape Town, Cape Town, South Africa
ABSTRACT
BACKGROUND: Little is known about the impact of HIV infection on clinical presentation, complications, and morbid pericarditis-related outcomes of tuberculous pericarditis and its predictors
OBJECTIVE: To assess the impact of HIV infection on presentation and outcomes in the multicountry Investigation of the Management of Pericarditis (IMPI) randomised controlled trial of immunotherapy in tuberculous pericarditis conducted in sub-Saharan Africa
METHODS: We compared clinical features and outcomes of 1 370 adult patients treated for tuberculous pericarditis (939 and 431 HIV-infected and uninfected, respectively) enrolled in the IMPI trial. Cox proportional hazards models were used to determine independent predictors of outcomes of HIV-associated tuberculous pericarditis
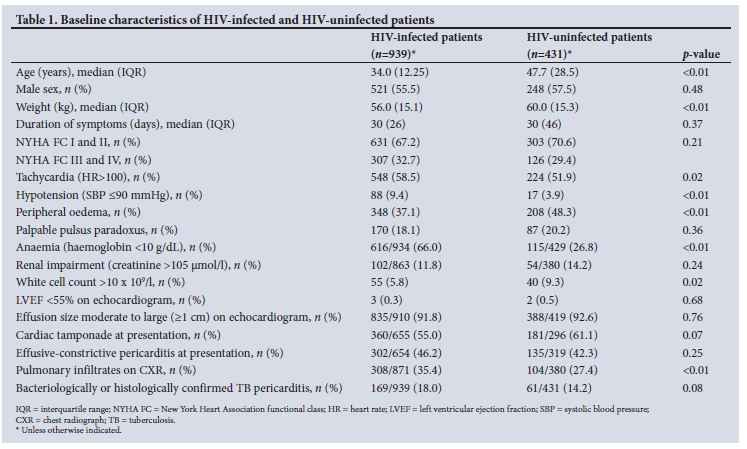
RESULTS: At presentation, HIV-infected (v. uninfected) patients were younger (median age 34.0 years v. 47.7 years), had lower body mass (mean weight 56 kg v. 60 kg), higher prevalence of tachycardia (58.5% v. 51.9%), hypotension (9.4% v. 3.9%), anaemia (65.9% v. 26.8%), and radiographic pulmonary infiltrates compatible with tuberculosis (35.4% v. 27.4%), but had lower rates of peripheral oedema (37.1% v. 48.3%). HIV-infected (v. uninfected) patients were less likely to develop constrictive pericarditis (4.1% v. 10.0% at 1 year, p<0.0001 (hazard ratio (HR) 0.41, 95% confidence interval (CI) 0.27 - 0.63, p<0.0001)). However, there was no difference in case fatality rate at 1 year (14.9% v. 12.2%, respectively, p=0.09; (HR 1.20, 95%CI 0.90 - 1.59, p=0.22)). Among HIV-infected patients, heart failure New York Heart Association (NYHA) class III - IV, low body mass, hypotension, and peripheral oedema were independently associated with death
CONCLUSION: HIV infection alters the cardiovascular presentation and reduces the incidence of constrictive pericarditis, but does not increase case fatality. Mortality in HIV-infected patients is independently predicted by markers of pericardial and tuberculosis disease severity
The intersecting epidemics of HIV and tuberculosis (TB) are a major public health challenge in Africa.[1] In 2017, the World Health Organization (WHO) and the Joint United Nations Programme on HIV/AIDS (UNAIDS) estimated that in sub-Saharan Africa there were an estimated 26 million people living with HIV infection, with approximately 663 000 and 252 000 HIV-associated annual incident TB cases and related deaths, respectively.[2,3] HIV-infected patients are at substantially higher risk for extrapulmonary dissemination of TB, including TB pericarditis. TB is the commonest cause of large pericardial effusion in developing countries in which TB is endemic, and in Africa accounts for approximately 7% of hospital admissions for acute heart failure.[4,5]
Evidence about the impact of HIV infection on survival in TB pericarditis is conflicting. A prospective study of 74 patients with HIV-associated TB pericarditis in Malawi found that the outcome compared favourably with quoted survival rates from the pre-HIV
era.[6] By contrast, a South African (SA) study of 233 patients with TB pericarditis showed that the 30-day mortality was higher for HIV-positive patients than for HIV-negative patients (9.9% v. 6.2%, p=0.04).[7] Furthermore, the Investigation of the Management of Pericarditis (IMPI) in Africa registry, that preceded the clinical trial, of 185 patients, not only showed a higher mortality in patients with HIV and/or signs of immunosuppression (compared with those without) at 6 months of follow-up (40% v. 17%), but also greater evidence of myopericarditis, dyspnoea, haemodynamic instability and systemic dissemination of TB.[4,8,9] However, these studies enrolled relatively small numbers of patients and were conducted before or during the early phase of the introduction of large-scale antiretroviral therapy (ART) programmes.
The multicountry IMPI randomised trial enrolled adults in sub-Saharan Africa with definite and probable TB pericarditis. Patients were randomised to: (i) adjunctive prednisolone or placebo; and (ii) Mycobacterium indicus pranii (MIP) or placebo in a 2-by-2 factorial design, together with standard TB treatment.[10] In primary analyses, neither intervention had an effect on the composite endpoint of death, recurrent cardiac tamponade requiring pericardiocentesis or constrictive pericarditis.
The IMPI trial provided an opportunity to examine the impact of HIV infection on clinical presentation and outcome in a cohort of patients who were followed up over 4 years with a progressive uptake of ART during the course of the study. In the pre-specified secondary analyses reported here, we also aimed to identify predictors of death, recurrent pericardial effusion with tamponade requiring pericardiocentesis, and constriction among the HIV-infected patients.
Methods
Study design
The IMPI trial, which was conducted in 19 centres across 8 African countries, was co-ordinated by teams at the University of Cape Town, SA, and the Population Health Research Institute (PHRI) at McMaster University, Canada. The design has been reported elsewhere.[10] Briefly, adult patients with a moderate to large pericardial effusion and a confirmed or clinically suspected diagnosis of TB pericarditis were randomly assigned to receive: (i) tapering doses of prednisolone (120 mg/day to 5 mg/day over 6 weeks) or placebo; and (ii) intradermal injections of heat-killed MIP (five doses over 3 months) or placebo. Patients were followed up twice-weekly for the first 6 weeks, then 3-monthly to 6 months, then twice-yearly for up to 4 years (minimum follow-up of 6 months, median follow-up period 636.5 days). HIV-infected patients were referred to ART clinics for ART initiation. The study was approved by relevant regulatory authorities and ethics committees, and patients provided written informed consent. For the purposes of this report, we conducted a pre-specified secondary analysis of data from the IMPI trial.
Study definitions and outcomes
Definitions of all measured outcomes are published elsewhere.[10] All outcomes and causes of death were independently adjudicated. Patients were defined as being HIV-infected at baseline if they had a positive HIV ELISA test prior to, at, or within the first 4 weeks of enrolment. Patients who refused or did not have an HIV test were classified as having unknown HIV status and were excluded from these analyses. Additional HIV-related variables recorded included ART status (at baseline and during follow-up) and CD4 counts. Demographic, baseline clinical, echocardiographic, and radiological features were recorded.
Statistical analysis
Data were analysed with the use of STATA software, version 13.1 (Stata Corp., USA). Categorical variables were described using count and percentage, and continuous variables by mean and standard deviation (if normally distributed), or median and interquartile range (IQR) (if data not normally distributed). The distributions of categorical variables were compared using the χ2 test or Fisher's exact test. The distributions of continuous variables were compared using the Student's t-test or analysis of variance (ANOVA) or Kruskal-Wallis test, where appropriate.
Baseline characteristics were compared for HIV-infected v. uninfected patients. Comparisons within the HIV-infected group were stratified by CD4 counts and ART status at enrolment. CD4 counts strata used for analyses were: <50 cells/µl; 50 -200 cells/µl; 200 - 350 cells/µl; and >350 cells/µl. Patients who were receiving ART at enrolment were categorised as on ART and compared with those not on ART at enrolment. Patients who were previously on ART but had defaulted at the time of enrolment were classified as not on ART.
Kaplan-Meier (KM) survival curves were used to compare time-to-death, recurrent tamponade or constriction by HIV status, CD4 counts, baseline ART status and haemoglobin level. The log rank test was used to compare survival curves by selected baseline characteristics.
In analyses restricted to HIV-infected patients, Cox proportional hazards models were used to determine the association of baseline characteristics with time-to-death, recurrent tamponade and constriction including adjustment for receipt of prednisolone. Receipt of MIP was excluded from multivariate models because not all patients were randomised to MIP or its placebo and because of its lack of effect on the primary outcome and its components.[10] Covariates that were at least marginally associated with the outcomes of interest in univariate analyses (p<0.10) and a priori clinical factors of interest were included in these multivariate models. Different a priori factors were included in the models for death, recurrent tamponade and constriction. The findings are reported as adjusted hazard ratios (aHRs) with 95% confidence intervals (CIs). We also used the competing risk methodology to identify independent predictors for constriction which accounted for the competing event of death, based on the proportional subdistribution hazard model.[11] A Cox proportional hazards model for constriction differs from a model in which time-to-death is also competing. The standard Cox model of time-to-constriction censored any preceding deaths, precluding constriction. The incidence rate of constriction will thus be biased upward. In a competing risk analysis, time-to-death is no longer censored but rather modelled by a separate Cox model with time-to-death as the endpoint. Our findings are reported as subhazard ratios (SHRs) with 95% CIs.
Sensitivity analyses were restricted to patients with microbiologically confirmed TB (i.e. smear-positive for acid-fast bacilli and/or culture-positive for Mycobacterium tuberculosis on any clinical sample). Analyses of ART use as a time-dependent variable (i.e. influence of being on ART at baseline or starting after enrolment) were also performed for death, recurrent tamponade and constriction. The criterion for statistical significance was set at alpha = 0.05. There was no adjustment for multiple testing since these secondary analyses were primarily exploratory.
Results
The IMPI trial enrolled 1 400 patients at 19 clinical sites in 8 African countries; most (72%) were recruited at SA sites. Baseline HIV status was known in 1 370 patients (97.9%), of whom 939 were HIV-infected (68.5%). Mean follow-up time for HIV-infected patients was 661 days (IQR 835) v. 667 days (IQR 710) for HIV-uninfected patients.
Clinical presentation
Compared with HIV-uninfected patients, HIV-infected patients were younger with lower body mass, and had a higher prevalence of anaemia, and lower prevalence of leukocytosis; additionally, more HIV-infected patients had radiographic pulmonary infiltrates compatible with TB (Table 1). Furthermore, HIV-infected patients had a higher prevalence of both tachycardia (resting heart rate >100 beats/minute) and hypotension (resting systolic blood pressure <90 mmHg) but less pedal oedema than HIV-uninfected patients.
Baseline CD4 count was available for n=633/939 (67.4%) of HIV-infected patients with a median CD4 count of 144 cells/µl (IQR 200); 103 patients (16.3%) had <50 cells/µl, 295 (46.6%) 50 - 199 cells/µl, 144 (22.7%) 200 - 350 cells/µl, and 91 (14.4%) >350 cells/ µl. Patients with the lowest CD4 counts (<50 cells/µl) were more likely to present with severe dyspnoea (assessed using New York Heart Association (NYHA) functional class), anaemia, and renal impairment (Supplementary Table 1: https://www.samedical.org/file/1984). Neither HIV status nor CD4 counts were associated with cardiac tamponade or effusive-constrictive pericarditis at presentation.
ART status was known for n=912/939 (97.1%) patients with HIV infection. At enrolment, n=199/912 (21.8%) were on ART. Patients on ART were older and more had anaemia and tachycardia at presentation than those not on ART (Supplementary Table 2: https://www.samedical.org/file/1984). The number of patients on ART increased to n=550/746 (73.7%) of patients at 6 months' follow-up.
Mortality
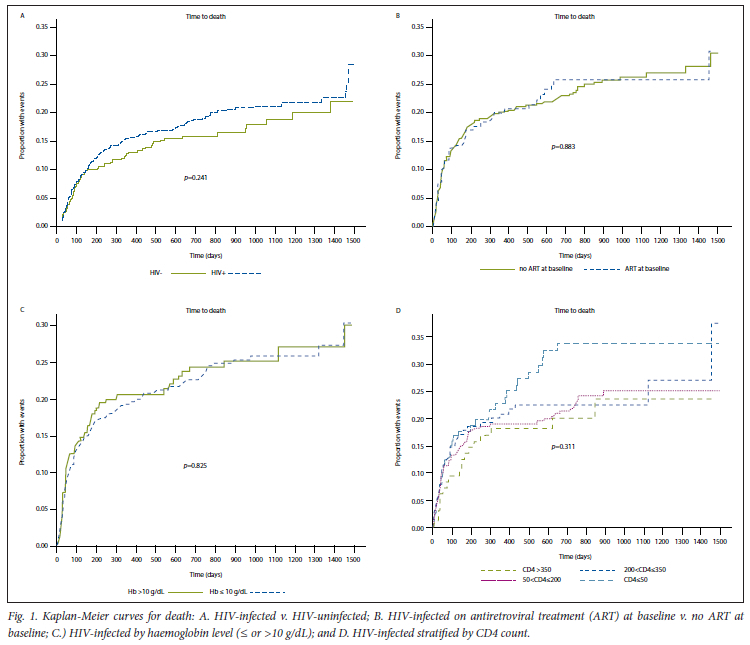
Cumulative mortality in HIV-infected and HIV-uninfected patients was 11.3% and 9.3% at 6 months, and 14.9% and 12.2% at 1 year, respectively (p=0.22 at 1 year). KM analysis revealed that survival did not differ between HIV-infected and HIV-uninfected patients (Fig. 1A). For HIV-infected patients, neither low haemoglobin nor ART at baseline were associated with death (Fig. 1B and C), whereas patients with a CD4 count of <50 cell/μl had a significantly increased risk of death compared with patients with higher CD4 counts (Fig. 1D).
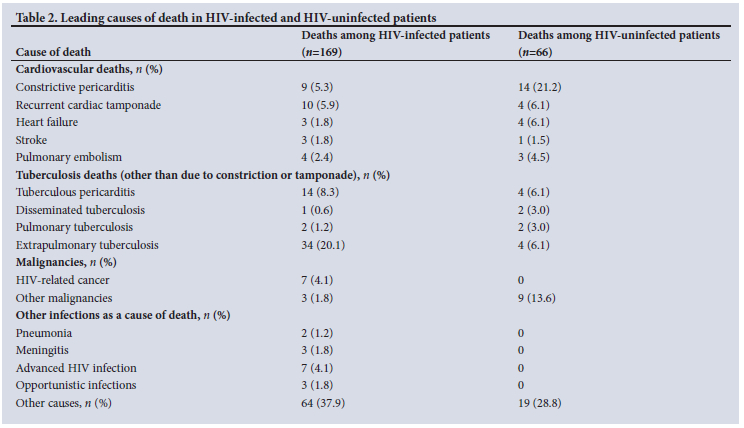
In the HIV-infected patients, 63.4% of deaths occurred within the first 6 months and 30.2% of deaths were attributed to TB (Table 2; Fig. 1A). The TB deaths included deaths related to the original diagnosis of TB pericarditis, but not those related to constrictive pericarditis or recurrent tamponade. Extrapulmonary TB accounted for 20.1% (n=34/169) of deaths among HIV-infected patients, compared with 6.1% (n=4/66) in the HIV-uninfected patients. Pericardial constriction caused a greater proportion of deaths in the HIV-uninfected patients: n=14/66 (21.2%) compared with n=9/169 (5.3%) in HIV-infected patients.
In a multivariable Cox proportional hazards model, severe dyspnoea (NYHA class III - IV), weight, peripheral oedema, and hypotension were independent predictors of mortality in HIV-infected patients (Table 3). CD4 count was not independently associated with mortality.
Recurrent cardiac tamponade requiring pericardiocentesis
The cumulative incidence of recurrent tamponade requiring pericardiocentesis among HIV-infected and uninfected patients was 3.5% and 0.4% at 6 months, and 3.5% and 4.0% at 1 year, respectively. There were no differences in times to event in KM analyses when comparing HIV-infected with uninfected patients, nor by CD4 counts, exposure to ART or haemoglobin levels in the HIV-infected patients (Supplementary Fig. 1A - D: https://www.samedical.org/file/1984). No variables were independently associated with recurrent tamponade in the multivariable Cox proportional hazards model (Table 3).
Constrictive pericarditis
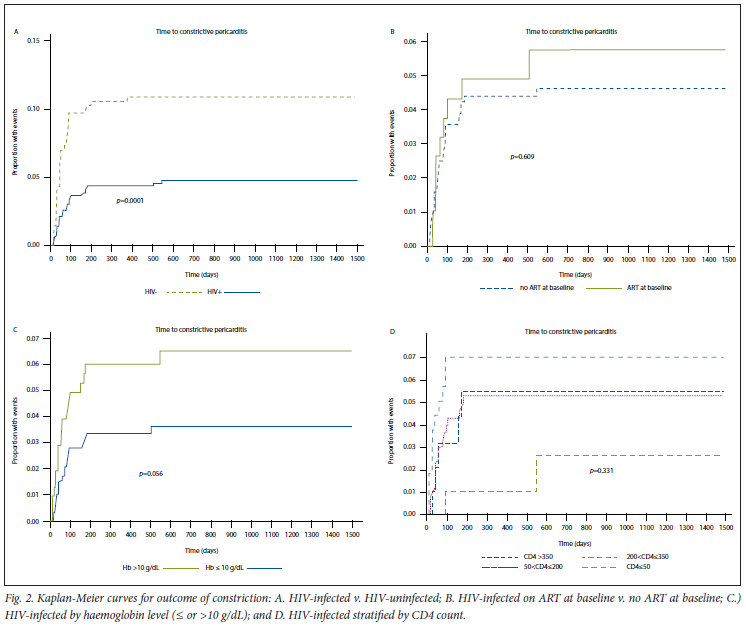
HIV-infected patients were at a significantly lower risk of developing constrictive pericarditis than HIV-uninfected patients (Fig. 2A). The cumulative incidence was 4.2% for HIV-infected and 10.2% for HIV-uninfected patients at 6 months, and 4.1% and 10.0% at 1 year respectively (p<0.01 at 1 year). Within the HIV-infected group, ART status, haemoglobin level and CD4 counts were not associated with risk of constriction (Fig. 2B-D).
In the multivariate Cox proportional hazards model, female sex was associated with a reduced risk of constriction, while tachycardia and peripheral oedema at enrolment were associated with increased risk in HIV-infected patients.
Sensitivity analyses, competing risk model, and analysis of ART as a time-dependent variable
When the analyses were restricted to patients with confirmed TB, the findings in respect of differences in clinical presentation and predictors of outcomes were unchanged (data not shown). In the competing risk analysis (with death as the competing event) sex, peripheral oedema, and tachycardia remained significantly associated with constrictive pericarditis in HIV-infected patients (data not shown).
Univariate analyses of exposure to ART as a time-dependent variable were estimated for death (HR 0.88, 95% CI 0.59 - 1.33, p=0.57), recurrent tamponade (HR 1.31, 95% CI 0.59 - 2.94, p=0.51), and constrictive pericarditis (HR 0.89, 95% CI 0.46 - 1.74, p=0.73). When included as a variable in multivariate Cox proportional hazards models, adjusting for the same variables as shown in Table 3, ART exposure during follow-up was not associated with any of these outcomes (data not shown).
Discussion
This study has six main findings: (i) HIV-associated TB pericarditis was frequently an acute illness characterised by dyspnoea, tachycardia, and hypotension; (ii) HIV co-infection had no effect on recurrent cardiac tamponade requiring pericardiocentesis; (iii) HIV-infected patients with TB pericarditis had a lower incidence of constrictive pericarditis than HIV-uninfected patients; (iv) mortality rate in patients with HIV-associated TB pericarditis was similar to that in HIV-uninfected patients; (v) we confirmed earlier reports that HIV-infected (v. uninfected) adults with TB pericarditis were younger at presentation, had lower body mass, were more anaemic and had greater prevalence of radiographic pulmonary infiltrates compatible with TB;[4,12-14] and (vi) among HIV-infected patients, death was independently associated with severe dyspnoea, weight, peripheral oedema and hypotension, but not CD4 count.
While the more frequent tachycardia and hypotension in HIV-infected patients could reflect tamponade or effusive-constrictive pericarditis at presentation, neither of these severe compressive pericardial syndromes, which were assessed using objective clinical and echocardiographic measures, differed significantly between HIV-infected and uninfected patients.[10] It is therefore possible that the haemodynamic disturbances observed in HIV-infected patients are related to more severe and disseminated TB (beyond the pericardium) and a resultant sepsis syndrome. The more frequent anaemia, a common association with disseminated TB,[14] and more frequent radiographic pulmonary infiltrates in HIV-infected patients support this hypothesis.[15] Furthermore, around one-fifth of deaths in HIV-infected patients were attributed to extrapulmonary TB (excluding TB pericarditis), which caused fewer deaths among HIV-uninfected patients.
HIV infection was associated with a 50% lower rate in late pericardial constriction, the most significant long-term complication of TB pericarditis. The risk of constriction was further reduced in HIV-infected patients with the use of adjuvant prednisolone (of borderline statistical significance), but this finding needs to be viewed in the light of an increased cancer risk among HIV-infected patients who received prednisolone in the IMPI trial. Previous studies have reported that late constrictive pericarditis occurs in 15% - 25% of patients with TB pericarditis. By contrast, constriction was observed in about 6% of patients in the IMPI trial (4.1% and 10.0% in HIV-infected v. HIV-uninfected patients at 1 year, respectively).[10] Ntsekhe et al.[16] observed that HIV-infected patients, despite having more aggressive forms of TB pericarditis, develop less pericardial constriction. Our analysis confirmed this observation. The mechanism for HIV protecting against the development of pericardial fibrosis (which results in constriction) is not known; HIV co-infection has been shown not to affect the expression profile of inflammatory mediators in the pericardial fluid in TB pericarditis.[17]
The IMPI trial, evaluating treatment strategies in TB pericarditis, was the largest study ever conducted in patients with this condition; almost 70% of patients included were HIV-infected, representing the largest HIV-associated TB pericarditis cohort to date. Prior observational data with smaller sample sizes suggested that HIV co-infection was associated with increased mortality risk in TB pericarditis, with case fatality rates of up to 40% in patients with advanced AIDS.[8] Those studies largely predated the scale-up of ART programmes in sub-Saharan Africa.[18,19] Our contrary findings may be due to larger sample size, but more likely because of increased access to ART. In the IMPI trial, approximately 20% of HIV-infected patients were on ART at enrolment, and by 6 months, 74% had started ART. This is still suboptimal given that TB pericarditis is a WHO stage 4 defining illness, and therefore all patients were eligible for ART according to national guidelines at the time of the trial.
Cumulative mortality was 12% - 15% at 1 year and was similar in HIV-infected and uninfected patients. This mortality rate was similar to that described previously by our group for HIV-uninfected patients (based on registry data from the same study sites) but lower than what was described for HIV-infected patients.[8] It appears that with wider (yet still not optimal) use of ART, the mortality risk in HIV-infected patients is reduced to that of HIV-uninfected patients. In line with these observations, markers of severity of pericardial disease rather than of HIV markers, such as CD4 count, appeared to drive mortality risk in adjusted analyses. Furthermore, <10% of all deaths in HIV-infected patients were attributed to opportunistic infections, HIV-associated malignancies, or advanced HIV. Among HIV-infected patients, markers of more severe pericardial disease or disseminated TB, such as severe dyspnoea, hypotension and peripheral oedema, were predictive of death.
Our study had several limitations. This was a post-hoc analysis of the IMPI trial, and even though the HIV analyses were pre-specified, this study was not powered to identify differences in the compared subgroups, thus making the study hypothesis generating. The date of initiation of ART was not captured during the trial, but only whether or not patients were on treatment at a given study visit; this resulted in imprecision in the analyses related to ART. Although CD4 counts were available for two-thirds of HIV-infected patients at enrolment, the data were sparse for the subsequent visits over 6 months of treatment because these tests were not mandated by the trial protocol.'201 Autopsies were performed on very few deceased patients. Therefore, the causes of death were largely based on review of clinical notes and remain unknown for many patients, particularly those who died away from the hospital.
Conclusion
In conclusion, in the modern ART era, the case fatality rate for HIV-infected patients with TB pericarditis is similar to that of HIV-uninfected patients. Importantly, HIV-infected patients may be at lower risk for the most severe long-term complication, constriction.
Declaration. None.
Acknowledgements. The authors wish to acknowledge and thank all IMPI trial investigators.
Author contributions. FG, SP, JBN, ZK, VF, LT, MS and JB were investigators on the main IMPI trial that was led by SY, MN and BMM. FG, SP and GM conducted the analyses for this study and prepared the first draft of the manuscript. All authors provided feedback on the drafts towards finalisation of the manuscript.
Funding. IMPI trial was supported by grants from the Canadian Institutes of Health Research, the Canadian Network and Centre for Trials Internationally, the Population Health Research Institute, Cadila Pharma, the South African Medical Research Council, and the Lily and Ernst Hausmann Research Trust. GM was supported by the Wellcome Trust (098316 and 203135/Z/16/Z), the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation (NRF) of South Africa (Grant No 64787), NRF incentive funding (UID: 85858) and the South African Medical Research Council through its TB and HIV Collaborating Centres Programme with funds received from the National Department of Health (RFA# SAMRC-RFA-CC: TB/HIV/AIDS-01-2014).
The funders had no role in study design; collection, analysis, or interpretation of data; the writing of the report; or the decision to submit the paper for publication. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Conflicts of interest. None.
References
1. Murray CJL, Ortblad KF, Guinovart C, et al. Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014;384(9947):1005-1070. https://doi.org/10.1016/s0140-6736(14)60844-8 [ Links ]
2. Joint United Nations Programme on HIV/AIDS (UNAIDS). UNAIDS Data 2018. www.unaids.org/sites/default/files/media_asset/unaids-data-2018_en.pdf. Accessed 13 November 2018. Geneva: UNAIDS, 2018. [ Links ]
3. World Health Organization. Global Tuberculosis Report 2018. http://apps.who.int/iris/bitstream/handle/10665/259366/9789241565516-eng.pd£jsessionid=9B5AB592527079D4E42B715095E00688?sequence=1. Geneva: WHO, 2018 (accessed 13 November 2018). [ Links ]
4. Mayosi BM, Wiysonge CS, Ntsekhe M, et al. Clinical characteristics and initial management of patients with tuberculous pericarditis in the HIV era: the Investigation of the Management of Pericarditis in Africa (IMPI Africa) registry. BMC Infect Dis 2006;6:2. https://doi.org/10.1186/1471-2334-6-2 [ Links ]
5. Damasceno A, Mayosi BM, Sani M, et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: Results of the sub-Saharan Africa survey of heart failure. Arch Int Med 2012;172:1386-1394. https://doi.org/10.1001/archinternmed.2012.3310 [ Links ]
6. Maher D, Harries AD. Tuberculous pericardial effusion: A prospective clinical study in a low-resource setting -Blantyre, Malawi. Int J Tuberc Lung Dis 1997;1(4):358-364. [ Links ]
7. Reuter H, Burgess LJ, Louw VJ, et al. The management of tuberculous pericardial effusion: Experience in 233 consecutive patients. Cardiovasc J S Afr 2007;18:20-25. [ Links ]
8. Mayosi BM, Wiysonge CS, Ntsekhe M, et al. Mortality in patients treated for tuberculous pericarditis in sub-Saharan Africa. S Afr Med J 2008;98:36-40. [ Links ]
9. Syed FF, Ntsekhe M, Gumedze F, et al. Myopericarditis in tuberculous pericardial effusion: Prevalence, predictors and outcome. Heart (British Cardiac Society) 2014;100(2):135-139. https://doi.org/10.1136/heartjnl-2013-304786 [ Links ]
10. Mayosi BM, Ntsekhe M, Bosch J, et al. Prednisolone and Mycobacterium indicuspranii in tuberculous pericarditis. N Engl J Med 2014;371(12):1121-1130. [ Links ]
11. Fine J, Gray R. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 1999;94:496-509. [ Links ]
12. Lawn SD, Bekker L-G, Middelkoop K, et al. Impact of HIV infection on the epidemiology of tuberculosis in a peri-urban community in South Africa: The need for age-specific interventions. Clin Infect Dis 2006;42(7):1040-1047. https://doi.org/10.1086/501018 [ Links ]
13. Raviglione MC, Narain JP, Kochi A. HIV-associated tuberculosis in developing countries: Clinical features, diagnosis, and treatment. Bull World Health Organ 1992;70(4):515-526. [ Links ]
14. Volberding PA, Levine AM, Dieterich D, et al. Anemia in HIV infection: Clinical impact and evidence-based management strategies. Clin Infect Dis 2004;38(10):1454-1463. https://doi.org/10.1086/383031 [ Links ]
15. Kerkhoff AD, Wood R, Cobelens FG, et al. The predictive value of current haemoglobin levels for incident tuberculosis and/or mortality during long-term antiretroviral therapy in South Africa: A cohort study. BMC Med 2015;13:70. https://doi.org/10.1186/s12916-015-0320-9 [ Links ]
16. Ntsekhe M, Wiysonge CS, Gumedze F, et al. HIV infection is associated with a lower incidence of constriction in presumed tuberculous pericarditis: A prospective observational study. PLoS ONE 2008;3:e2253. https://doi.org/10.1371/journal.pone.0002253 [ Links ]
17. Matthews K, Deffur A, Ntsekhe M, et al. A compartmentalised profibrotic immune response characterises pericardial tuberculosis, irrespective of HIV-1 infection. Am J Respir Crit Care Med 2015;192(12):1518-1521. https://doi.org/10.1164%2Frccm.201504-0683LE [ Links ]
18. Mutevedzi PC, Newell ML. Review: The changing face of the HIV epidemic in sub-Saharan Africa. Trop Med Int Health 2014;19(9):1015-1028. https://doi.org/10.1111/tmi.12344 [ Links ]
19. World Health Organization. March 2014 supplement to the 2013 consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: Recommendations for a public health approach. 2014; http://www.who.int/hiv/pub/guidelines/arv2013/arvs2013upplement_march2014/en/ (accessed 20 June 2016). [ Links ]
20. Mayosi BM, Ntsekhe M, Bosch J, et al. Rationale and design of the Investigation of the Management of Pericarditis (IMPI) trial: A 2 X 2 factorial randomised double-blind multicenter trial of adjunctive prednisolone and Mycobacterium w immunotherapy in tuberculous pericarditis. Am Heart J 2013;165(2):109-115.e103. https://doi.org/10.1016/j.ahj.2012.08.006 [ Links ]
 Correspondence:
Correspondence:
G Meintjes
graemein@mweb.co.za
* Deceased


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}