










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 n.3 Pretoria Mar. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i3.16761
RESEARCH
Clinical impact of plasma concentrations of first-line antituberculosis drugs
R PerumalI, II; K NaidooIII, IV; A NaidooV; N PadayatchiVI, VII
IMB ChB, MMed (Int Med); Centre for the AIDS Programme of Research in South Africa (CAPRISA), Nelson R Mandela School of Medicine, College of Health Sciences., University of KwaZulu-Natal, Durban, South Africa
IIMB ChB, MMed (Int Med); Medical Research Council-CAPRISA HIV-TB Pathogenesis and Treatment Research Unit, Doris Duke Medical Research Institute, University of KwaZulu-Natal, Durban, South Africa
IIIMB ChB, PhD; Centre for the AIDS Programme of Research in South Africa (CAPRISA), Nelson R Mandela School of Medicine, College of Health Sciences., University of KwaZulu-Natal, Durban, South Africa
IVMB ChB, PhD; Medical Research Council-CAPRISA HIV-TB Pathogenesis and Treatment Research Unit, Doris Duke Medical Research Institute, University of KwaZulu-Natal, Durban, South Africa
VMMedSc, PhD;Centre for the AIDS Programme of Research in South Africa (CAPRISA), Nelson R Mandela School of Medicine, College of Health Sciences., University of KwaZulu-Natal, Durban, South Africa
VIMB ChB, PhD;Centre for the AIDS Programme of Research in South Africa (CAPRISA), Nelson R Mandela School of Medicine, College of Health Sciences., University of KwaZulu-Natal, Durban, South Africa
VIIMB ChB, PhD;Medical Research Council-CAPRISA HIV-TB Pathogenesis and Treatment Research Unit, Doris Duke Medical Research Institute, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: The clinical significance of low antituberculosis (anti-TB) drug concentrations has not been fully elucidated
OBJECTIVES: To investigate the clinical consequences of first-line drug concentrations in adult patients with drug-susceptible pulmonary TB in South Africa (SA
METHOD: We conducted a pharmacokinetic study nested within the control arm of the Improving Treatment Success (IMPRESS) trial (NCT 02114684) in Durban, SA. During the first 2 months of treatment, participants received weight-based dosing of first-line anti-TB drugs (rifampicin, isoniazid, pyrazinamide and ethambutol), and had plasma drug concentrations measured at 2 and 6 hours after drug administration during the 8th week of treatment. Intermediate (8 weeks), end-of-treatment (6 months) and follow-up TB outcomes were assessed using World Health Organization criteria
RESULTS: We measured plasma drug concentrations on available samples in 43 participants. Peak drug concentrations were below the therapeutic range in 39/43 (90.7%) for rifampicin, 32/43 (74.4%) for isoniazid, 27/42 (64.3%) for pyrazinamide and 5/41 (12.2%) for ethambutol. At the end of the intensive phase of treatment (week 8), 20.9% (n=9/43) of participants remained culture positive. We did not find a relationship between the concentrations of first-line drugs and treatment outcomes at week 8. All participants were cured at the end of treatment, and there were no relapses during the 12-month follow-up period
CONCLUSION: Treatment outcomes were favourable despite low drug concentrations as defined by current reference thresholds
Tuberculosis (TB) is the leading cause of death from a curable infectious disease. In 2020, there were an estimated 10 million new cases of drug-sensitive TB, with almost half of the cases in southern Africa occurring in individuals with HIV co-infection.[1] Despite effective treatment, the global treatment success rate is 85% of reported cases. There is significant variability in success rates across regions, and the rate is considerably lower in settings with a high TB/HIV burden.[1] Despite the high global cure rate, much lower levels of treatment success have been reported in some parts of the world; only nine of the top 30 high TB burden countries reached or exceeded a 90% treatment success rate, and >1.5 million people experienced poor outcomes globally in 2020.[1] The End TB Strategy has set the ambitious goal of improving treatment success to >90% by 2025 and reducing TB mortality to <5%.[2] While the current multidrug regimen for TB has improved treatment success over the past decades, there have been few instructive pharmacokinetic-pharmacodynamic studies to guide optimisation of the regimen.[3] The highly variable pharmacokinetic-pharmacodynamic profile of first-line TB drugs has received much attention since the advent of modern molecular advances in pharmacokinetic-pharmacodynamic science and the application of therapeutic drug monitoring principles to TB.[4-13] However, the optimal plasma concentrations for these drugs have still not been established, which has raised questions about whether our current dosing strategies are optimal.[14-17]The emergence of acquired drug resistance, even in the context of well-functioning TB control programmes and high levels of adherence, has placed increased pressure on the scientific community to improve our understanding of the pharmacological challenges in the treatment of TB.[18] Additionally, the risks of therapeutic failure on one side and drug toxicities on the other continue to motivate the search for optimal pharmacokinetic-pharmacodynamic performance of these drugs. Recent modelling data that evaluated various novel rifampicin-susceptible or rifampicin-resistant TB regimens concluded that regimen efficacy alone had the greatest potential to reduce TB cases and deaths, concluding that maintaining the efficacy of existing regimens should be as important as research into novel regimens.[19]
Low concentrations of one or more anti-TB drugs have frequently been reported in both developed and developing countries; however, few studies were appropriately designed to investigate the clinical significance of low drug concentrations based on published reference ranges.[20-26]
In this prospective observational substudy of a randomised controlled trial, we investigated the clinical consequences of first-line drug concentrations in adult participants with drug-susceptible pulmonary TB in South Africa (SA).
Methods
We conducted a prospective pharmacokinetic study nested within the Improving Treatment Success (IMPRESS) open-label randomised controlled trial (NCT 02114684) in Durban, SA. Participants randomised to the control arm of the study, receiving the World Health Organization (WHO) standardised first-line four-drug regimen, provided informed consent to be included in the pharmacokinetic substudy. Blood samples were collected for pharmacokinetic analysis at predefined time points. All participants recruited into the study were > 18 years of age, had a history of pulmonary TB in the previous
3 years, and had been diagnosed with drug-susceptible pulmonary TB. During the first 2 months (intensive phase) of treatment weight-based dosing of fixed-dose combination (FDC) tablets was as follows: participants weighing 38 - 54 kg received rifampicin 450 mg, isoniazid 225 mg, pyrazinamide 1 200 mg and ethambutol 825 mg those weighing 55 - 70 kg received rifampicin 600 mg, isoniazid 300 mg, pyrazinamide 1 600 mg and ethambutol 1 100 mg; and those weighing >70 kg received rifampicin 750 mg, isoniazid 375 mg, pyrazinamide 2 000 mg and ethambutol 1 375 mg. During the subsequent 4 months (continuation phase), the same weight-based dosing of rifampicin and isoniazid was continued.
Sputum samples were collected for smears and culture at baseline, fortnightly for 8 weeks, monthly until the end of treatment, and then on alternate months until the end of 18 months after randomisation. Clinical and safety evaluations were performed every 2 months for the first 6 months and as clinically indicated thereafter, until the end of the 12-month follow-up period. Demographic, clinical and laboratory data previously reported to influence plasma concentrations of first-line anti-TB drugs were recorded: age, sex, ethnicity, body weight, haemoglobin, albumin, HIV infection, diabetes mellitus, smoking and alcohol exposure. Concomitant drug exposures were recorded on case report forms at baseline and follow-up.
The study pharmacokinetic assessment was scheduled at the end of the intensive phase of treatment, ~8 weeks after the start of TB treatment. The daily FDC dose was administered under direct observation and under fasting conditions. All drugs with potential for drug-drug interaction with first-line anti-TB drugs were rescheduled for 4 hours before or after TB treatment dosing. Venous blood was drawn at 2 hours and 6 hours after anti-TB drug ingestion. Plasma, collected in ethylenediaminetetra-acetic acid-coated tubes, was centrifuged at 3 000 rpm, placed on ice, and stored in cryovials at -80°C within 1 hour of collection. Rifampicin, isoniazid, pyrazinamide and ethambutol concentrations were quantified in clinical plasma samples using validated high-performance liquid chromatography tandem mass spectrometry at the KwaZulu-Natal Research Institute for Tuberculosis and HIV (KRITH) pharmacology laboratory. The higher of the two measured values for each drug was defined as the estimated maximum plasma concentration (Cmax).[27-30] Low plasma concentrations were defined using published reference ranges: rifampicin <8 mg/L, isoniazid <3 mg/L, pyrazinamide <35 mg/L and ethambutol <2 mg/L.[31] Very low plasma concentrations were defined as rifampicin <4 mg/L, isoniazid < 1.5 mg/L, pyrazinamide <20 mg/L and ethambutol <1 mg/L.[31] No dose adjustments were performed on the basis of these results. Standard WHO TB outcome definitions were used.[32]
The study was approved by the Biomedical Research Ethics Committee of the University of KwaZulu-Natal (ref. no. BFC029/13) and the Medicines Control Council of South Africa (ref. no. MCC 20130510).
Factors associated with low or normal plasma Cmax of isoniazid, rifampicin, ethambutol and pyrazinamide were identified using Fisher's exact tests (categorical factors) and t-tests (continuous factors). Differences in the plasma Cmax and the proportions of patients with low or very low plasma concentrations by 8-week culture outcome were assessed using the Wilcoxon rank-sum test and Fisher's exact test, respectively. Poisson regression analysis with robust variance, adjusting for sex, HIV status and presence of cavitation on baseline chest radiograph, was used to measure the association between 8-week culture outcome and C of each drug, where plasma Cmax was measured on a continuous scale. In order to determine whether selection bias was present in the sample, the characteristics of the study participants were compared with the characteristics of patients who refused or could not be part of the study (results not shown). All analyses were performed in SAS version 9.4 (SAS Institute, USA).
Results
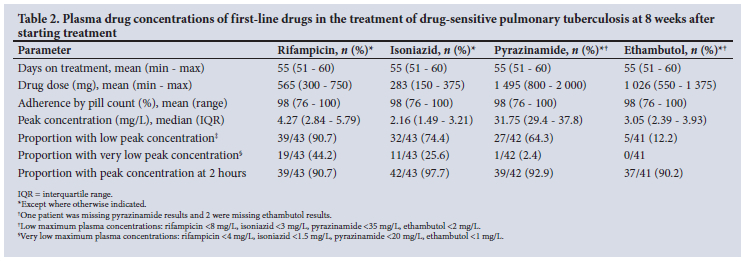
A total of 43/98 eligible patients with drug-sensitive pulmonary tuberculosis consented to participate in this pharmacokinetic substudy. The mean age of the participants was 34.5 years, and 60.5% were male (Table 1); 79.1% were HIV infected, with a mean CD4 count of 291 cells/uL. Almost a third (30.2%) of participants were former or current smokers. The mean time from treatment initiation to drug concentration assessment was 51 days, and mean doses were 565 mg (9.76 mg/kg) for rifampicin, 283 mg (4.89 mg/ kg) for isoniazid, 1 495 mg (25.8 mg/kg) for pyrazinamide and 1 026 mg (17.7 mg/kg) for ethambutol (Table 2). Mean adherence by pill count was 98% (range 76 - 100%) for all drugs. Plasma concentrations were below the therapeutic range in 39/43 (90.7%) of participants for rifampicin, 32/43 (74.4%) for isoniazid, 27/42 (64.3%) for pyrazinamide and 5/41 (12.2%) for ethambutol (Table 2 and Fig. 1). Plasma concentrations were very low (less than half of the lower limit of the therapeutic range) in 19/43 (44.2%) of participants for rifampicin, 11/43 (25.6%) for isoniazid and 1/42 (2.4%) for pyrazinamide. Correspondingly, the overall median peak concentrations for rifampicin, isoniazid and pyrazinamide were below the therapeutic range (Table 3). All participants were cured at the end of treatment, and there were no relapses during the 12-month follow-up period. However, for the intermediate treatment outcome of sputum culture conversion at 8 weeks, 9/43 (20.9%) of participants failed to achieve conversion (Table 3). Overall, low plasma concentrations in three or more drugs were found in 25/43 participants (58.1%): 7/9 participants (77.8%) who failed to culture convert by week 8, and 18/34 participants (52.9%) who were culture negative by week 8 (p=0.46).
The multivariable Poisson regression model with robust variance showed no significant relationship between the concentrations of any of the four drugs and sputum culture conversion at week 8, adjusting for sex, HIV status and cavitation on baseline chest radiograph (Table 4).
Discussion
This prospective evaluation of first-line drug concentrations, nested within a randomised controlled trial, identified a high prevalence of low drug concentrations in participants with a previous history of TB, the majority of whom were HIV co-infected. Low peak plasma concentrations were demonstrated for rifampicin (90.7%), isoniazid (74.4%), pyrazinamide (64.3%) and ethambutol (12.2%) after 2 months of treatment in a cohort of participants with excellent adherence. The overwhelming majority of participants did not achieve therapeutic concentrations of either rifampicin or isoniazid, and 58.1% of participants (n=25/43) had low concentrations of at least three drugs after 8 weeks of uninterrupted treatment. In this study, low drug concentrations occurred independently of HIV co-infection, smoking status and body mass index (BMI). Although not statistically significant, there was a pattern of lower weight and BMI in patients with low drug concentrations, which is probably a consequence of weight-based dosing. All participants received drugs as part of an approved and registered FDC that was dosed according to the WHO-recommended weight-based schedule.[33] The mean doses of all drugs were found to be within the acceptable range (9.8 mg/kg for rifampicin, 4.9 mg/kg for isoniazid, 25.8 mg/kg for pyrazinamide and 17.7 mg/kg for ethambutol), and adherence rates measured by pill count were excellent.
The finding of a high prevalence of low drug concentrations has been widely reported, and pooled estimates for low drug concentrations generated by meta-analysis were 67% (95% confidence interval (CI) CI 60 - 74) for rifampicin, 43% (95% CI 32 - 55) for isoniazid, 12% (95% CI 7 - 19) for pyrazinamide and 27% (95% CI 17 - 38) for ethambutol.[34] Similar to our study, a meta-analysis of first-line drug concentrations did not identify HIV, diabetes mellitus, weight or dosing strategy to be important predictors of low drug concentrations.[34] While there has been extensive reporting of drug concentrations, there is a paucity of studies evaluating the impact of low drug concentrations on treatment outcomes.[20-28,35-39]
Despite the high prevalence of low concentrations of first-line drugs in the present study, treatment outcomes were uniformly good. All participants were cured, and there were no relapses during the 12 months of follow-up after treatment completion.
Assessing the intermediate outcome of sputum culture conversion at the end of the intensive phase of treatment (week 8), 20.9% of participants (n=9/43) remained culture positive. Overall, we did not find a relationship between the concentrations of first-line drugs and treatment outcomes, whether at week 8, at the end of treatment, or at the 12-month post-treatment follow-up. While men who failed to culture convert by week 8 tended towards low concentrations of isoniazid, pyrazinamide and ethambutol, this relationship did not reach statistical significance in a univariate model (not shown).
In contrast, women who failed to culture convert by week 8 showed a tendency towards lower rifampicin concentrations. These sex-specific trends were independent of body weight and BMI, and although this study was not powered to detect differences in drug concentrations and outcome between sexes, this signal warrants further empirical evaluation.
A prospective observational study of 225 outpatients in Botswana reported a greater risk (adjusted relative risk 3.3; 95% CI 1.84 - 6.22) for poor final treatment outcome in patients with a low pyrazinamide concentration.[25] A prospective observational cohort study of 32 inpatients and outpatients in a high-income country with a low TB and HIV burden demonstrated a significantly lower mean isoniazid concentration in patients with poor treatment outcomes compared with those with good outcomes (mean isoniazid Cmax 1.0 v. 2.6 mg/L; p=0.004).[21] While a prospective observational cohort study of 142 hospitalised patients in a high TB burden setting did not find an association between TB drug concentrations and treatment outcomes, the authors presented a novel statistical approach, classification and regression tree analysis to evaluate the role of the full first-line drug pharmacokinetic curve on treatment outcomes.[22] Using this method, the authors identified new area under the curve (AUC) thresholds for rifampicin, isoniazid and pyrazinamide that were predictive of a poor end-of-treatment outcome. The drug thresholds predictive of poor outcome were a 24-hour AUC of 363 mg.h/L for pyrazinamide, 13 mg.h/L for rifampicin and 52 mg.h/L for isoniazid. The odds ratio (OR) for poor outcome with an AUC of at least one drug below these derived thresholds compared with patients without any drug AUC below the thresholds was 14.14 (95% CI 4.08 - 49.08). In addition, patients with a pyrazinamide or rifampicin AUC below the threshold values had significantly increased odds of relapse (OR 51.9; 95% CI 3.04 - 886). In a large prospective study of drug concentrations and treatment outcomes in 1 912 patients with TB in India, lower rifampicin concentration was independently associated with risk of an unfavourable treatment outcome.[20] In a cohort of 268 TB/HIV-co-infected patients in Uganda, patients with both low rifampicin and low isoniazid concentrations had a significantly increased risk for an unfavourable treatment outcome.[29] We did not find a relationship between first-line drug concentrations and treatment outcomes, irrespective of whether we examined drug concentrations as median concentration, proportion below reference cut-offs, or a continuous variable (Table 3 and Fig. 1). In addition, unlike several other studies, the combination of low rifampicin and isoniazid concentrations did not predict a poor outcome in our cohort. However, it is possible that our study was underpowered to detect these associations.
The varying findings regarding the relationship between drug concentrations and treatment outcomes require evaluation through further prospective long-term follow-up studies. The existing evidence does not provide a convincing answer to this question, one way or the other. While it is possible that larger studies are needed to evaluate the relationship between drug concentrations and treatment outcome, this is largely because unfavourable outcomes are uncommon, and treatment outcomes are reasonably good despite widely reported low first-line drug concentrations. Nonetheless, there remains heterogeneity in treatment outcomes, as treatment success rates of between 34% and 76% have been reported in high TB/HIV burden settings, even under research conditions.[40,41] This finding lends credence to the possibility that optimal concentrations may be higher than can be achieved using current dosing guidelines, and there is accumulating evidence to suggest that higher doses of rifampicin, and correspondingly increased plasma concentrations, may be able to safely close the treatment success gap.[17]
While there has been concern that low drug concentrations may increase the risk of acquired drug resistance and disease relapse, we did not encounter any cases of acquired drug resistance or relapse. In a study of 413 patients with TB in Korea, recurrence with drug-resistant TB occurred in 4 patients, 3 of whom had low isoniazid drug concentrations during treatment of the initial drug-sensitive TB episode.[23] A meta-analysis of isoniazid and rifampicin pharmacokinetics and acquired drug resistance demonstrated that the pharmacokinetic variability of isoniazid, led primarily by acetylator status, was associated with acquired drug resistance.[14]
The present study has a number of important strengths, including that it was a prospective study nested within a randomised controlled trial, using a pharmacokinetic protocol under standardised conditions. Directly observed drug administration in the starved state, and timed blood draws with careful sample handling, storage and processing, all contributed to high-quality drug concentration data. Despite the small sample size, this is one of only a few studies investigating drug concentrations in a setting of high TB/HIV co-infection, exclusively in patients with a previous history of TB. An 18-month follow-up allowed for evaluation of the important ancillary outcome of relapse, which is only infrequently reported on in the existing literature. Nonetheless, some important limitations must be noted. The sample size is small and was largely limited by the costs associated with pharmacokinetic studies performed under strict research conditions. In addition, the absence of unfavourable outcomes in this study may reflect the high levels of retention and adherence that were obtained partly through the intensive retention strategies of the randomised controlled trial and inclusion of the adherence-promoting activity of pill counting. While we estimated Cmax using a limited-sampling strategy, it is possible that first-line TB drugs may have a more demonstrable dose response when represented by the AUC. However, measuring the AUC is impractical in clinical settings, and previous studies have shown that the Cmax values of rifampicin, isoniazid, pyrazinamide and ethambutol correlate well with the respective AUC derived from intensive sampling.[31,42] Furthermore, it is possible that pathogen factors such as the minimum inhibitory concentration (MIC) may intervene in the relationship between drug concentrations and treatment outcome. The absence of a pharmacodynamic parameter such as the MIC in this study limits its ability to make any strong conclusions regarding microbiological outcome.
Conclusion
This prospective study using a pharmacokinetic protocol demonstrated a high prevalence of low plasma drug concentrations in a cohort of patients with recurrent TB in a high TB/HIV burden setting. Despite this finding, treatment outcomes were good, and we found no relationship between the concentrations of any of the first-line anti-TB drugs and treatment outcomes. Notwithstanding the absence of evidence demonstrating the effect of drug concentrations on treatment outcome in this study, the idea of optimising drug concentrations is still worthy of consideration, as it may help to achieve the goals of shortening treatment duration, reducing acquired drug resistance, and improving long-term treatment outcomes.
Declaration. None.
Acknowledgements. We thank the following laboratories and laboratory staff for their assistance with handling, processing and analysing specimens for the pharmacokinetic analysis of first-line TB drugs: the CAPRISA Laboratory (Mrs Natasha Samsunder and her laboratory staff) and the KRITH Pharmacology Core (Dr John Adamson and Ms Katya Govender).
We also acknowledge the contributions of Dr Rochelle Adams, Dr Razia Hassan-Moosa, and CAPRISA nursing and support staff.
Author contributions. All authors contributed to the design and implementation of the study. RP and AN performed the data analysis and drafted the manuscript. All authors reviewed and approved the manuscript.
Funding. This work was supported by the European and Developing Countries Clinical Trials Partnership, which provided funding for the trial (TA.2011.40200.044).
Conflicts of interest. None.
References
1. World Health Organization. Global tuberculosis report 2020. Geneva. WHO, 2020. https://www.who.int/publications/i/item/9789240013131 (accessed 21 August 2021). [ Links ]
2. World Health Organization. The End TB Strategy. Global strategy and targets for tuberculosis prevention, care, and control after 2015. Geneva. WHO, 2015. https://www.who.int/publications/i/item/WHO-HTM-TB-2015.19 (accessed 23 August 2021). [ Links ]
3. Gumbo T, Angulo-Barturen I, Ferrer-Bazaga S. Pharmacokinetic-pharmacodynamic and dose-response relationships of antituberculosis drugs. Recommendations and standards for industry and academia. J Infect Dis 2015;21l(Suppl 3):S96-S106. https://doi.org/10.1093/infdis/jiu610 [ Links ]
4. Wilkins JJ, Savic RM, Karlsson MO, et al. Population pharmacokinetics of rifampin in pulmonary tuberculosis patients, including a semi mechanistic model to describe variable absorption. Antimicrob Agents Chemother 2008;52(6):2138-2148. https://doi.org/10.1128/aac.00461-07 [ Links ]
5. Wilkins JJ, Langdon G, McIUeron H, Pillai GC, Smith PJ, Simonsson US. Variability in the population pharmacokinetics of pyrazinamide in South African tuberculosis patients. Eur J Clin Pharmacol 2006;52(9):727-735. https://doi.org/10.1007/s00228-006-0141-z [ Links ]
6. Wilkins JJ, Langdon G, McIUeron H, Pillai G, Smith PJ, Simonsson US. Variability in the population pharmacokinetics of isoniazid in South African tuberculosis patients. Br J Clin Pharmacol 2011;72(1):51-62. https://doi.org/10.1111/j.l365-2125.2011.03940.x [ Links ]
7. Tappero JW, Bradford WZ, Agerton TB, et al. Serum concentrations of antimycobacterial drugs in patients with pulmonary tuberculosis in Botswana. Clin Infect Dis 2005;41(4):461-469. https://doi.org/10.1086/431984 [ Links ]
8. Peloquin CA. Tuberculosis drug serum levels. Clin Infect Dis 2001;33(4):584-585. https://doi.org/10.1086/322706 [ Links ]
9. Peloquin CA. Therapeutic drug monitoring in antituberculosis chemotherapy. Ther Drug Monit 1999;21(4):426-427. https://doi.org/10.1097/00007691-199908000-00008 [ Links ]
10. Peloquin CA. Serum concentrations of the antimycobacterial drugs. Chest 1998;113(5):1154-1155. https://doi.org/10.1378/chest.ll3.5.1154 [ Links ]
11. McIUeron H, Wash P, Burger A, Norman J, Folb PI, Smith P. Determinants of rifampin, isoniazid, pyrazinamide, and ethambutol pharmacokinetics in a cohort of tuberculosis patients. Antimicrob Agents Chemother 2006;50(4):l170-1177. https://doi.org/10.1128/aac.50.4.1170-1177.2006 [ Links ]
12. McIUeron H, Rustomjee R, Vahedi M, et al. Reduced antituberculosis drug concentrations in HIV-infected patients who are men or have low weight. Implications for international dosing guidelines. Antimicrob Agents Chemother 2012;56(6):3232-3238. https://doi.org/10.1128/aac05526-11 [ Links ]
13. Gumbo T, Louie A, Deziel MR, et al. Concentration-dependent Mycobacterium tuberculosis killing and prevention of resistance by rifampin. Antimicrob Agents Chemother 2007;51(11):3781-3788. https://doi.org/10.1128/aac01533-06 [ Links ]
14. Pasipanodya JG, Srivastava S, Gumbo T. Meta-analysis of clinical studies supports the pharmacokinetic variability hypothesis for acquired drug resistance and failure of antituberculosis therapy. Clin Infect Dis 2012;55(2):169-177. https://doi.org/10.1093/cid/cis353 [ Links ]
15. Mitchison DA. Pharmacokinetic/pharmacodynamic parameters and the choice of high-dosage rifamycins. Int J Tuberc Lung Dis 2012;16(9):1186-1189. https://doi.org/10.5588/ijtld.l1.0818 [ Links ]
16. Milstein M, Lecca L, Peloquin C, et al. Evaluation of high-dose rifampin in patients with new, smear-positive tuberculosis (HIRIF). Study protocol for a randomised controlled trial. BMC Infect Dis 2016;16(1):453. https://doi.org/10.1186/sl2879-016-1790-x [ Links ]
17. Boeree MJ, Diacon AH, Dawson R, et al. A dose-ranging trial to optimise the dose of rifampin in the treatment of tuberculosis. Am J Respir Crit Care Med 2015;191(9):1058-1065. https://doi.org/10.1093/cid/cizl071 [ Links ]
18. Calver AD, Falmer AA, Murray M, et al. Emergence of increased resistance and extensively drug-resistant tuberculosis despite treatment adherence, South Africa. Emerg Infect Dis 2010;16(2):264-271. https://doi.org/10.3201/eidl602.090968 [ Links ]
19. Kendall E A, Shrestha S, Cohen T, et al. Priority-setting for novel drug regimens to treat tuberculosis. An epidemiologic model. PLoS Med 2017;14(l):el002202. https://doi.org/10.1371/journal.pmed.1002202 [ Links ]
20. Ramachandran G, Agibothu Kupparam HK, Vedhachaiam C, et al. Factors influencing tuberculosis treatment outcome in adult patients treated with thrice-weekly regimens in India. Antimicrob Agents Chemother 2017;61(5):e02464-16. https://doi.org/10.1128/aac.02464-16 [ Links ]
21. Prahl JB, Johansen IS, Cohen AS, Frimodt-MoUer N, Andersen AB. Clinical significance of 2 h plasma concentrations of first-line anti-tuberculosis drugs. A prospective observational study. J Antimicrob Chemother 2014;69(10):2841-2847. https://doi.org/10.1093/jac/dku210 [ Links ]
22. Pasipanodya JG, McUleron H, Burger A, Wash PA, Smith P, Gumbo T. Serum drug concentrations predictive of pulmonary tuberculosis outcomes. J Infect Dis 2013;208(9):1464-1473. https://doi.org/10.1093/infdis/jit352 [ Links ]
23. Park JS, Lee JY, Lee YJ, et al. Serum levels of antituberculosis drugs and their effect on tuberculosis treatment outcome. Antimicrob Agents Chemother 2015;60(1):92-98. https://doi.org/10.1128/aac.00693-15 [ Links ]
24. Maze MJ, Paynter J, Chiu W, Hu R, Nisbet M, Lewis C. Therapeutic drug monitoring of isoniazid and rifampicin during anti-tuberculosis treatment in Auckland, New Zealand. Int J Tuberc Lung Dis 2016;20(7):955-960. https://doi.org/10.5588/ijtld.l5.0792 [ Links ]
25. Chideya S, Winston CA, Peloquin CA, et al. Isoniazid, rifampin, ethambutol, and pyrazinamide pharmacokinetics and treatment outcomes among a predominantly HIV-infected cohort of adults with tuberculosis from Botswana. Clin Infect Dis 2009;48(12):1685-1694. https://doi.org/10.1086/599040 [ Links ]
26. Burhan E, Ruesen C, Ruslami R, et al. Isoniazid, rifampin, and pyrazinamide plasma concentrations in relation to treatment response in Indonesian pulmonary tuberculosis patients. Antimicrob Agents Chemother 2013;57(8):3614-3619. https://doi.org/10.1128/aac.02468-12 [ Links ]
27. Requena-Mendez A, Davies G, Ardrey A, et al. Pharmacokinetics of rifampin in Peruvian tuberculosis patients with and without comorbid diabetes or HIV Antimicrob Agents Chemother 2012;56(5):2357-2363. https://doi.org/10.1128/aac06059-11 [ Links ]
28. S ekaggya-Wiltshire C, Lamorde M, Kiragga AN, et al. The utility of pharmacokinetic studies for the evaluation of exposure-response relationships for standard dose anti-tuberculosis drugs. Tuberculosis (Edinb) 2018;108:77-82. https://doi.org/10.1016/j.tube.2017.11.004 [ Links ]
29. S ekaggya-Wiltshire C, von Braun A, Lamorde M, et al. Delayed sputum conversion in tuberculosis-human immunodeficiency virus-co-infecte d patients with low isoniazid and rifampicin concentrations. Clin Infect Dis 2018;67(5):708-716. https://doi.org/10.1093/cid/ciyl79 [ Links ]
30. Semvua HH, Mtabho CM, Fillekes Q, et al. Efavirenz,tenofovir and emtricitabine combined with first-line tuberculosis treatment in tuberculosis-HIV-coinfected Tanzanian patients. A pharmacokinetic and safety study. Antivir Ther 2013;18(1):105-113. https://doi.org/10.3851/imp2413 [ Links ]
31. Alsultan A, Peloquin CA. Therapeutic drug monitoring in the treatment of tuberculosis. An update. Drugs 2014;74(8):839-854. https://doi.org/10.1007/s40265-014-0222-8 [ Links ]
32. World Health Organization. Definitions and reporting framework for tuberculosis. Geneva. WHO, 2013. https://www.who.int/publications/i/item/9789241505345 (accessed 25 August 2021). [ Links ]
33. World Health Organization. Treatment of tuberculosis. Guidelines. 4th ed. Geneva. WHO, 2010. https://www.ncbi.nlm.nih.gov/books/NBK138748/#!po=16.6667 (accessed 15 July 2020). [ Links ]
34. Mota L, Al-Efraij K, Campbell JR, Cook VJ, Marra F, Johnston J. Therapeutic drug monitoring in antituberculosis treatment. A systematic review and meta-analysis. Int J Tuberc Lung Dis 2016;20(6):819-826. https://doi.org/10.5588/ijtld.15.0803 [ Links ]
35. Babalik A, Mannix S, Francis D, Menzies D. Therapeutic drug monitoring in the treatment of active tuberculosis. Can Respir J 2011;18(4):225-229. https://doi.org/10.1155/2011/30715C [ Links ]
36. Kayhan S, Akgunes A. Therapeutic monitoring of isoniazid, rifampicin, ethambutol and pyrazinamide serum levels in the treatment of active pulmonary tuberculosis and determinants of their serum concentrations. Afr J Pharm Pharmacol 2011;5(17):2035-2041. https://doi.org/10.5897/AJPP11.511 [ Links ]
37. Meloni M, Corti N, Muller D, et al. Cure of tuberculosis despite serum concentrations of antituberculosis drugs below published reference ranges. Swiss Med Wkly 2015;145.w14223. https://doi.org/10.4414/smw.2015.14223 [ Links ]
38. Ruslami R, Nijland HM, Alisjahbana B, Parwati I, van Crevel R, Aarnoutse RE. Pharmacokinetics and tolerability of a higher rifampin dose versus the standard dose in pulmonary tuberculosis patients. Antimicrob Agents Chemother 2007;51(7):2546-2551. https://doi.org/10.1128/aac.01550-06 [ Links ]
39. Van Crevel R, Alisjahbana B, de Lange WC, et al. Low plasma concentrations of rifampicin in tuberculosis patients in Indonesia. Int J Tuberc Lung Dis 2002;6(6):497-502. https://doi.org/10.5588/09640569513002 [ Links ]
40. Abdool Karim SS, Naidoo K, Grobler A, et al. Timing of initiation of anti retroviral drugs during tuberculosis therapy. N Engl J Med 2010;362(8):697-706. https://doi.org/10.1056/nejmoa0905848 [ Links ]
41. Volmink J, Garner P. Directly observed therapy for treating tuberculosis. Cochrane Database Syst Rev 2007, Issue 4. Art. No. CD003343. https://doi.org/10.1002/14651858.cd003343.pub3 [ Links ]
42. Akkerman OW, van Altena R, Bolhuis MS, van der Werf TS, Alffenaar JW. Strategy to limit sampling of antituberculosis drugs instead of determining concentrations at two hours postingestion in relation to treatment response. Antimicrob Agents Chemother 2014:58(1):628. https://doi.org/10.1128/aac.01535-13 [ Links ]
 Correspondence:
Correspondence:
R Perumal
rubeshanperumal@gmail.com
Accepted 4 October 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}