










Serviços Personalizados
Artigo
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 no.2 Pretoria Fev. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i2.16629
RESEARCH
Peritoneal dialysis outcomes in a tertiary-level state hospital in Johannesburg, South Africa: Ethnicity and HIV co-infection do not increase risk of peritonitis or discontinuation
M M SunnyrajI; M DaviesI, II; Z CassimjeeI, II
IMB BCh, MMed (Int Med); Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMB BCh, MMed (Int Med); Division of Nephrology, Helen Joseph Hospital, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Peritoneal dialysis (PD) is a valuable means to increase access to kidney replacement therapy in South Africa (SA). An increased rate of modality discontinuation related to an increased risk of peritonitis in patients of black African ethnicity, in those with diabetes and in those living with HIV has previously been suggested, which may lead to hesitancy in adoption of 'PD first' programmes.
OBJECTIVES. To analyse the safety of a PD-first programme in terms of 5-year peritonitis risk and patient and modality survival at the outpatient PD unit at Helen Joseph Hospital, Johannesburg.
METHODS. After exclusions, clinical data from 120 patients were extracted for analysis. The effects of patient age at PD initiation, ethnicity, gender, diabetes mellitus and HIV infection on patient and modality survival and peritonitis risk were analysed using Cox proportional hazards modelling and logistic regression analysis. Five-year technique and patient Kaplan-Meier survival curves for peritonitis and comorbidity groups were compared using the Cox-Mantel test. The Mann-Whitney (7-test and Fisher's exact test were used to compare continuous and categorical variables where appropriate.
RESULTS. Five-year patient survival was 49.9%. Black African ethnicity was associated with reduced mortality hazard (hazard ratio (HR) 0.33; 95% confidence interval (CI) 0.15 - 0.71; p=0.004), and patients with diabetes had poorer 5-year survival (19.1%; p=0.097). Modality survival at 5 years was 48.1%. Neither Black African ethnicity nor HIV infection increased the risk of PD discontinuation. Peritonitis was associated with increased modality failure (HR 2.99; 95% CI 1.31 - 6.87; p=0.009). Black African ethnicity did not increase the risk of peritonitis. HIV was not independently associated with an increased risk of peritonitis. Patient and PD survival were generally similar to other contemporaneous cohorts, and the peritonitis rate in this study was within the International Society for Peritoneal Dialysis acceptable range.
CONCLUSION. PD is a safe and appropriate therapy in a low socioeconomic setting with a high prevalence of HIV infection. Consideration of home circumstances and training in sterile technique reduce peritonitis risk and improve PD modality survival. Patients with diabetes may be at risk of poorer outcomes on PD.
Reduced costs, lower staff requirements, and independence from in-centre treatment render peritoneal dialysis (PD) a valuable kidney replacement therapy (KRT) for low- to middle-income countries such as South Africa (SA).[1,2] PD is therefore more likely than haemodialysis (HD) to be prescribed in the resource-limited public healthcare sector in this country,[3] which serves a historically socioeconomically disadvantaged population of predominantly black African ethnicity with a high prevalence of HIV infection[4] and diabetes.[5]
Available local literature has raised concern over the universal suitability of PD in this setting, with increased rates of PD modality discontinuation reported in patients of black African ethnicity~[6,7-PD-related peritonitis is the most important modifiable cause of PD discontinuation[8] and an important contributor to mortality.[9] An increased risk of peritonitis in patients of black African ethnicity[1°-and in people living with HIV (PLWH)[11] has been reported by local centres; comorbid diabetes has similarly been identified in some series as a risk factor for peritonitis.[12]
Lack of access to dialysis in the state sector limits individual modality selection, with many units pursuing a 'PD-first' policy. Poorer PD outcomes in this population create an ethical conundrum for prescribing nephrologists, who must seek to maximise the benefit of access to KRT while limiting the potential of harm to the individual arising from treatment complications. We describe the 5-year outcomes of PD at our institution, which demonstrate the safety of a modified PD-first programme in the state sector.
Methods
Helen Joseph Hospital (HJH) is a tertiary-level public hospital that provides KRT to residents of the western areas of Johannesburg. In line with government policy, KRT is only offered to those patients in whom evaluation reveals no overt contraindication to transplantation; evaluation includes assessment of cardiovascular risk. The hospital pursues a modified policy of 'PD first': patients are preferably initiated onto KRT via PD provided that a nurse practitioner deems their home circumstances to be suitable for PD. Key criteria assessed during the home visit by the nurse practitioner are the presence of a nearby source of running water to facilitate sterilisation, an area that can be made sterile for PD indwell, and adequate storage space for dialysate. Patients living in informal housing are not excluded from the programme provided these criteria are met. PLWH are not required to demonstrate virological control and immunological recovery prior to PD initiation. While all PLWH are initiated onto antiretroviral therapy (ART) before PD is started, late presentation with advanced kidney failure and previously undiagnosed HIV infection result in many patients requiring optimisation of their ART regimen following the start of dialysis.
All new PD initiates receive inpatient training by nurse practitioners following Tenckhoff catheter insertion, emphasising sterile self-administration of dialysate. Nurse practitioners undertake follow-up home visits to monitor patient compliance with sterile technique.
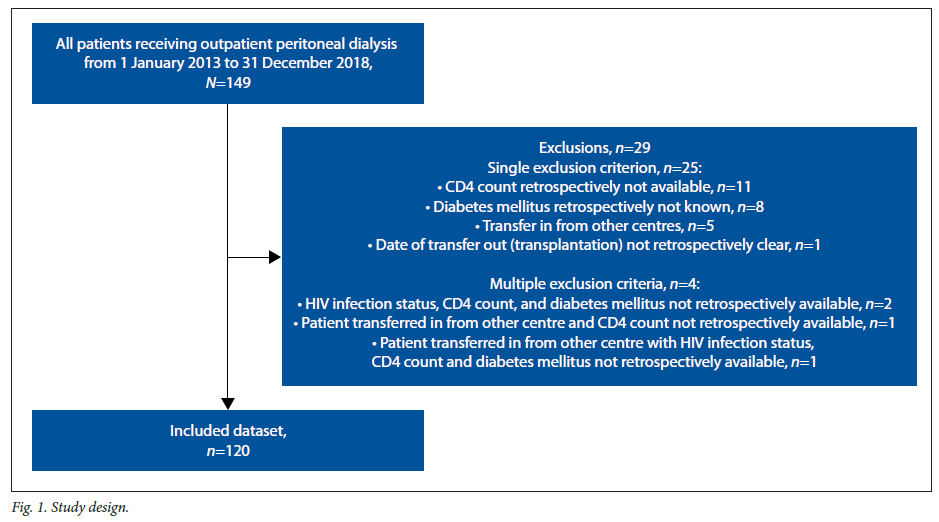
Permission to conduct this study was obtained from the Human Research Ethics Committee of the University of the Witwatersrand (ref. no. M190703). A retrospective review of the case records of all patients receiving outpatient PD for the management of kidney failure at HJH from 1 January 2013 to 31 December 2018 was undertaken. Of 149 patients, 29 were excluded from analysis owing to retrospectively incomplete data (Fig. 1). During the course of the study, 5 patients transferred to other PD units and 3 patients received a kidney transplant. The effects of patient age at dialysis initiation, ethnicity, gender and comorbidity with either diabetes mellitus or HIV on patient survival, PD discontinuation and peritonitis risk were analysed. For the purposes of this study, PD discontinuation was defined as formal acceptance for permanent transfer to HD or HD for >3 months' duration. Hazard ratios (HRs) for patient and modality outcomes were determined using Cox proportional hazards modelled over the first 5 years from PD initiation, and logistic regression analysis was used to evaluate the odds of developing peritonitis. Five-year technique and patient survival curves for peritonitis and comorbidity groups were fitted using the Kaplan-Meier method. The Cox-Mantel test was used to compare survival between groups.
Results
Baseline characteristics of the study cohort are shown in Table 1. The median (interquartile range) time on PD was 13.2 (5.7 - 27.5) months. Median age (42.4 v. 45.8 years) and sex ratios (male/female 1:1 and 3:2) were statistically similar between black African and non-black African ethnic groups (p=0.130 and p=0.343, respectively); however, heterogeneity in median distance of the patient's home from the PD centre (14.3 v. 7 km; p<0.001), HIV seropositivity (34.6 v. 7.1%; p<0.001) and comorbid diabetes mellitus (23.1 v. 40.5%; p=0.037) were observed. Patients with diabetes were older than non-diabetics (median age at PD initiation 49.9 years and 42.3 years, respectively; p=0.022).
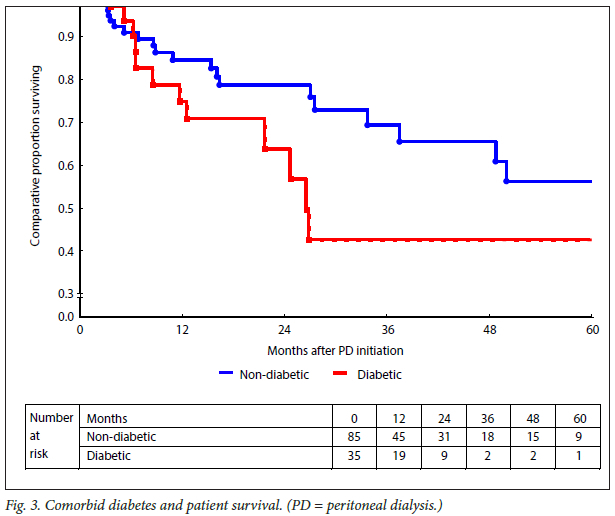
Thirty-two patients (26.7%) died during the course of this study. Cumulative survival censored for follow-up at 1, 2, 3 and 5 years was 82.2%, 74.6%, 61.1% and 49.9%. Mortality was directly attributable to peritonitis in 6 patients; Gram-negative bacteria were the most frequent isolates in this group (n=3 cases). Black African ethnicity was associated with lower mortality (HR 0.33; 95% confidence interval (CI) 0.15 - 0.71; p=0.004) (Fig. 2). Age at PD initiation (p=0.991), sex (p=0.485), comorbid diabetes (p=0.387) or HIV (p=0.268), and peritonitis (p=0.123) were not associated with increased mortality hazard during the 60 months of follow-up of the study period (Table 2), although poorer cumulative survival at 1, 2, 3 and 5 years was observed in patients with diabetes (77.1%, 66.8%, 38.2% and 19.1%, respectively) compared with non-diabetics (84.4%, 77.9%, 68.9% and 54.4%; p=0.097) (Fig. 3).
PD discontinuation occurred in 33 patients (27.5%) and was directly attributable to antecedent peritonitis (failure within 1 month of diagnosis of peritonitis or during inpatient treatment) in 21 cases (61.8% of technique failures). Gram-negative bacilli were the most frequently cultured organism in cases of peritonitis directly associated with discontinuation (n=8 cases). PD modality survival censored for duration of follow-up at 1, 2, 3 and 5 years was 83.3%, 74.5%, 58.9% and 48.1%, respectively. Peritonitis increased the risk of PD discontinuation (HR 2.99; 95% CI 1.31 - 6.87; p=0.009); recurrent episodes of peritonitis further increased this risk (HR 3.06; 95% CI 1.32 - 7.10; p=0.019) (Fig. 4). Age at PD initiation (p=0.885), sex (p=0.919), ethnicity (p=0.142) and comorbid diabetes (p=0.446) or HIV (p=0.607) did not affect risk of PD discontinuation (Table 2). PD modality survival rates at 5 years were non-significantly better in patients of black African ethnicity compared with other ethnic groups (48.6% and 38.9%, respectively; p=0.185).
One hundred and two episodes of peritonitis were recorded among 55 patients during the study period; the peritonitis rate was 0.51 episodes per patient-year (ppy). Gram-positive bacteria accounted for the majority of peritonitis cases (n=41; 40.2%), followed by Gram negatives (n=31 cases), with culture-negative peritonitis accounting for 24 cases. Tuberculous and fungal peritonitis were rare in this series (n=3 cases each). Age at PD initiation (p=0.633), sex (p=0.499), ethnicity (p=0.777) and comorbid diabetes (p=0.078) or HIV (p=0.328) were not associated with increased odds of peritonitis (Table 2), although the peritonitis rate was higher in PLWH than in those who were HIV negative (0.69 v. 0.45 ppy).
Discussion
This study provides evidence for the safety of a modified PD-first programme in the state sector among patients living in low socioeconomic settings and in populations with significant rates of comorbid diabetes mellitus and HIV infection. The study provides further demonstration of the importance of peritonitis in limiting the longevity of PD. Of note, these data appear to refute previous reports of increased risk of peritonitis and modality discontinuation in patients of black African ethnicity receiving PD, with superior patient survival being observed in this group.
Patient survival in this cohort was similar to that reported by contemporaneous international series, but poorer than that reported in the local literature (Table 3). A greater proportion of patients with diabetes in the present cohort (29.2%) compared with previous local studies (Davidson et al.[6] 9.8%, Isla et al.[13] 9.9%, Kapembwa et al.[7] 0.5%) and diverging survival outcomes for these patients, as observed in this study and reported by others,[17,18] may partially account for this discrepancy. Patients in our cohort were on average older (median age at PD initiation 44.3 years) than in contemporaneous local cohorts (Davidson et al.[6] 39.7 years, Isla et al.[13] 37.5 years, Kapembwa et al.[7] 36 years). Older age, particularly in patients with diabetes, has been associated with increasing mortality risk on PD,[19] which may further explain the poorer overall survival in our series.
Overall modality survival in this study was similar to that reported in other series (Table 3). Consistent with local[7,13,20] and international[8] experience, peritonitis contributed a significant risk to PD discontinuation; peritonitis was directly responsible for PD discontinuation in 61.8% of cases. Interventions to reduce peritonitis risk therefore offer a useful means to improve PD longevity.
In comparison with previous local series[6,7] and US data,[21] no effect was observed for ethnicity on modality survival. In SA as well as in the USA, ethnicity is often a determinant of socioeconomic status, which is an important factor in PD modality success.[21,22] A similar lack of effect for ethnicity on PD discontinuation has been noted in earlier reports from Johannesburg,[20] where census data suggest higher rates of integration and less socioeconomic disparity between ethnic groups.[23] The reliance on assessment of home circumstances as an entry criterion to this unit's PD programme is likely to have further homogenised socioeconomic status between ethnicities and abrogated the apparent effect of ethnicity on PD discontinuation.
The peritonitis rate recorded in our cohort (0.51 episodes ppy) is within range of that accepted by the International Society for Peritoneal Dialysis (ISPD),[24] but above the global mean rate of 0.31 - 0.35 episodes ppy reported for the study period.[25] Local units have reported contemporaneous peritonitis rates of 0.87 (Cape Town),[6] 0.82 (Polokwane)[13] and 1.45 (Bloemfontein).[26] Exit site care and sterile connection technique are important modifiable factors in decreasing infection risk,[8] and frequent monitoring of these parameters at clinical follow-up may reduce the rate of peritonitis and hence PD discontinuation.[20] The lower rate of peritonitis in this cohort may reflect centre-specific practices, including pre-admission assessment of home circumstances, inpatient training on sterile technique, and follow-up home visits. Such interventions are also likely to have reduced the effect of ethnic discrepancies in socioeconomic status and to account for the lack of effect of ethnicity on peritonitis risk observed.
Although the peritonitis rate in HIV-positive patients in this series was higher than that of HIV-negative patients, HIV seropositivity was not independently associated with an increased risk of developing peritonitis. The risk of peritonitis in the setting of HIV is partly dependent on severity of immunocompromise as evidenced by CD4 count at dialysis initiation, with those patients with a CD4 count <200 cells/mL being at particularly increased risk.[11] The median CD4 count in this series was 339 cells/mL, with only 9 patients having a CD4 count <200 cells/mL. Universal access to ART and improved CD4 counts at PD initiation are likely to have reduced the risk of peritonitis in this series.
There are limitations to this study. Level of education and income were not retrospectively available for all patients and were therefore not analysed. Type of housing (for example, residence in informal settlements) was also not included as a variable in the analyses. Previous local studies have failed to show a significant effect for these factors on the patient or PD outcomes assessed in the present work.[13,20] Pre-initiation assessment of home circumstances, and extensive inpatient training in sterile technique, are likely to have controlled for any discrepancies in housing state or education level in this cohort.
Nevertheless, taken together, these data demonstrate the role of pre-initiation assessment ofindividual patient socioeconomic circumstances and of ongoing nurse practitioner support in achieving acceptable peritonitis rates and potentially increasing PD longevity. Pre-initiation assessment should further include consideration of comorbidities including the treatment status of HIV infection, and caution should be exercised in prescribing PD for older patients with diabetes.
Conclusion
This study confirms the safety of use of PD as initial dialysis in a low socioeconomic community with high rates of HIV comorbidity. Peritonitis remains the most significant limitation to PD technique survival, and attention to patient home circumstances in the allocation of patients to PD, with ongoing patient training by nurse practitioners in infection prevention strategies, may assist in reducing the risk of this complication to ISPD acceptable levels. Patients with diabetes may be at increased risk of poorer overall survival, and are likely to benefit from careful cardiovascular risk evaluation if selected for PD.
Declaration. The research for this study was done in partial fulfilment of the requirements for MMS's MMed (Int Med) degree at the University of the Witwatersrand.
Acknowledgements. The authors gratefully acknowledge the nursing staff of the Helen Joseph Hospital Peritoneal Dialysis Unit, whose expertise and dedication are evident in the outcomes reported in this article.
Author contributions. MMS, MD and ZC contributed to the design of this study. Data collection was performed by MMS with assistance from MD. Data analysis was undertaken by MD. Manuscript preparation was by MD with assistance from ZC and MMS.
Funding. None.
Conflicts of interest. None.
References
1. Wearne N. Kilonzo K, Effa E, et al Continuous ambulatory peritoneal dialysis: Perspectives on patient selection in low- to middle-income countries. Int J Nephrol Renovasc Dis 2017;10:1-9. https://doi.org/10.2147/IJNRD.S104208 [ Links ]
2. Makhele L, Matlala M, Sibanda M, et al. A cost analysis of haemodialysis and peritoneal dialysis for the management of end-stage renal failure at an academic hospital in Pretoria, South Africa. Pharmacoeconom Open 2019;3(4):631-641. https://doi.org/10.1007/s41669-019-0124-5 [ Links ]
3. Davids MR, Jardine T, Marias N, et al. South African Renal Registry Annual Report 2017. Afr J Nephrol 2019;22(1):60-71. https://doi.org/10.21804/22-1-3810 [ Links ]
4. Mabaso M, Makola L, Naidoo I, Mlangeni LL, Jooste S, Simbayi L. HIV prevalence in South Africa through gender and racial lenses: Results from the 2012 population-based national household survey. Int J Equity Health 2019;18(1):167. https://doi.org/10.1186/s12939-019-1055-6 [ Links ]
5. Stokes A, Berry KM, Mchiza Z, et al Prevalence and unmet need for diabetes care across the care continuum in a national sample of South African adults: Evidence from the SANHANES-1, 2011 - 2012. PLoS ONE 2012;12(1):e0184264. https://doi.org/10.1371/journal.pone.0184264 [ Links ]
6. Davidson B, Crombie K, Manning K, Rayner B, Wearne N. Outcomes and challenges of a PD-first program, a South-African perspective. Perit Dial Int 2018;38(3):179-186. https://doi.org/10.3747/pdi.2017.00182 [ Links ]
7. Kapembwa KC, Bapoo NA, Tannor EK, Davids MR. Peritoneal dialysis technique survival at Tygerberg Hospital in Cape Town, South Africa. Afr J Nephrol 2017;20(1):25-33. https://doi.org/10.21807/20-1-1917 [ Links ]
8. Ersoy FF. Improving technique survival in peritoneal dialysis: What is modifiable? Perit Dial Int 2009;29(Suppl 2):S74-S77. [ Links ]
9. Ye H, Zhou Q, Fan L, et al The impact of peritoneal dialysis-related peritonitis on mortality in peritoneal dialysis patients. BMC Nephrol 2017;18(1):186. https://doi.org/10.1186/s12882-017-0588-4 [ Links ]
10. Zent R, Myers JE, Donald D, Rayner BL. Continuous ambulatory peritoneal dialysis: An option for the developing world? Perit Dial Int 1994;14(1):48-51. [ Links ]
11. Ndlovu KCZ, Sibanda W, Assounga A. Peritonitis outcomes in patients with HIV and end-stage renal failure on peritoneal dialysis: A prospective cohort study. BMC Nephrol 2017;18(1):48. https://doi.org/10.1186/s12882-017-0466-0 [ Links ]
12. Chow KM, Szeto CC, Leung BC, Kwan BC-H, Law MC, Li PK-T. A risk analysis of continuous ambulatory peritoneal dialysis-related peritonitis. Perit Dial Int 2005;25(4):374-379. https://doi.org/10.1177/089686080502500413 [ Links ]
13. Isla RAT, Mapiye D, Swanepoel C, Rozumyk N, Hubahib JE, Okpechi IG. Continuous ambulatory peritoneal dialysis in Limpopo province, South Africa: Predictors of patient and technique survival. Perit Dial Int 2014;34(5):518-525. https://doi.org/10.3747/pdi.2013.00334 [ Links ]
14. Li PK-T, Chow KM, van de Luitgaarden MWM, et al. Changes in the worldwide epidemiology of peritoneal dialysis. Nat Rev Nephrol 2017;13(2):90-103. https://doi.org/10.1038/nrneph.2016.181 [ Links ]
15. United States Renal Data System. 2020 Annual Data Report. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases, 2020. https://adr.usrds.org/2020 (accessed 22 April 2022). [ Links ]
16. Canadian Institute for Health Information. Treatment of end-stage organ failure in Canada. Canadian Organ Replacement Register, 2010 - 2019: End-stage kidney disease and kidney transplants. Ottawa, ON: CIHI, 2020. https://www.cihi.ca (accessed 22 April 2022). [ Links ]
17. Guo A, Mujais S. Patient and technique survival on peritoneal dialysis in the United States: Evaluation in large incident cohorts. Kidney Int 2003;64(Suppl 88):S3-S12. https://doi.org/10.1046/j.1523-1755.2003.08801.x [ Links ]
18. Yang X, Yi C, Liu X, et al. Clinical outcome and risk factors for mortality in Chinese patients with diabetes on peritoneal dialysis: A 5-year cohort study. Diabetes Res Clin Pract 2013;100(3):354-361. https://doi.org/10.1016/j.diabres.2013.03.030 [ Links ]
19. Bieber SD, Mehrotra R. Patient and technique survival of older adults with ESRD treated with peritoneal dialysis. Perit Dial Int 2015;35(6):612-617. https://doi.org/10.3747/pdi.2015.00050 [ Links ]
20. Katz I, Sofianou L, Hopley M. An African community-based chronic ambulatory peritoneal dialysis programme. Nephrol Dial Transplant 2001;16(12):2395-2400. https://doi.org/10.1093/ndt/16.12.2395 [ Links ]
21. Nadeau-Fredette A-C, Bargman JM. Characteristics associated with peritoneal dialysis failure: Are we asking the right questions? Am J Kidney Dis 2019;74(6):586-588. https://doi.org/10.1053/j.ajkd.2019.07.002 [ Links ]
22. Li PK-T, Chow KM. Peritoneal dialysis patient selection: Characteristics for success. Adv Chronic Kidney Dis 2009;16(3):160-168. https://doi.org/10.1053/j.ackd.2009.02.001 [ Links ]
23. Parry K, van Eeden A. Measuring racial residential segregation at different geographic scales in Cape Town and Johannesburg. S Afr Geogr J 2015;97(1):31-49. https://doi.org/10.1080/03736245.2014.924868 [ Links ]
24. Li PK-T, Szeto CC, Piraino B, et al. ISPD peritonitis recommendations: 2016 update on prevention and treatment. Perit Dial Int 2016;36(5):481-508. https://doi.org/10.3747/pdi.2016.00078 [ Links ]
25. Marshall MR. A systematic review of peritoneal dialysis-related peritonitis rates over time from national or regional population-based registries and databases. Perit Dial Int 2022;42(1):39-47. https://doi.org/10.1177/0896860821996096 [ Links ]
26. Musoke J, Bisiwe F, Natverlal A, et al. The prevalence and bacterial distribution of peritonitis amongst adults undergoing continuous ambulatory peritoneal dialysis at Universitas Hospital. S Afr J Infect Dis 2020;35(1):a104. https://doi.org/10.4102/sajid.v35i1.104 [ Links ]
 Correspondence:
Correspondence:
M Davies
malcolm.davies@wits.ac.za
Accepted 4 October 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}