










Services on Demand
Article
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 n.2 Pretoria Feb. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i2.16510
RESEARCH
Factors associated with partner notification intentions among symptomatic sexually transmitted infection service attendees in South Africa
B Da Costa DiasI; T KufaII, III; R S KularatneIV, V
IBSc Hons, PhD; Centre for HIV and STIs, National Institute for Communicable Diseases, Johannesburg, South Africa
IIMB ChB, PhD; Centre for HIV and STIs, National Institute for Communicable Diseases, Johannesburg, South Africa
IIIMB ChB, PhD; School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVMMed (Micro), FC Path (SA) Micro Centre for HIV and STIs, National Institute for Communicable Diseases, Johannesburg, South Africa
VMMed (Micro), FC Path (SA) Micro Department of Clinical Microbiology and Infectious Diseases, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. In South Africa (SA), a client-initiated partner notification (PN) approach is implemented for the management of sexual partners of patients presenting with sexually transmitted infections (STIs) or STI syndromes.
OBJECTIVES. To explore the demographic, sexual behavioural and clinical characteristics associated with PN intentions among symptomatic STI service attendees at sentinel primary healthcare facilities in three SA provinces.
METHODS. We analysed cross-sectional data obtained from 1 293 adults enrolled into STI aetiological surveillance during 2019 - 2020 in Gauteng, KwaZulu-Natal and Western Cape provinces. Self-reported sexual practices, PN intentions and clinical data were collected using nurse-administrated questionnaires. We assessed gender-stratified factors associated with the index case's willingness to notify their sexual partners of their STI syndrome diagnosis. Univariable and multivariable Poisson regression models with robust error variance were used to determine factors associated with gender-stratified PN intentions.
RESULTS. The enrolled participants comprised 887 male (68.6%) and 406 female (31.4%) STI clients. Self-reported PN intentions were higher among women than men (83.5% v. 64.4%; p<0.001). Multivariable analyses revealed that casual sex partnerships during the preceding 3-month period and enrolment at the KwaZulu-Natal site were independent barriers to PN intent among male participants. For females, enrolment at the Gauteng site was independently associated with lower PN intentions, while presenting with genital ulcer syndrome was a motivator towards PN intent. The primary reasons cited for non-disclosure across both genders were casual sexual encounters, followed by geographically distant partnerships and fear of disclosure.
CONCLUSION. We show that demographic and behavioural characteristics, as well as relationship dynamics, may influence the PN intentions of STI service attendees in SA. Alternative PN strategies should be considered, based on the reported barriers, to increase overall STI notification, strengthen partner management and ultimately reduce STI incidence.
South Africa (SA) has a high burden of sexually transmitted infections (STIs), with an estimated incidence of 4.5 million cases of gonorrhoea and 5.8 million cases of chlamydia among adults aged 15 - 49 years in 2017.[1] In the public health sector alone during 2020, 288 778 new cases of male urethritis syndrome (MUS) were reported.[2] Partner notification (PN), the process of an index case informing sexual partners of their possible exposure to STIs and their need to seek treatment, is an integral component of STI management. Effective PN and the promotion of healthcare seeking for sexual contacts are critical in preventing reinfection of the index case as well as reducing community transmission. In SA, STIs are managed using a syndromic approach,[3] as routine STI testing (point of care or laboratory based) is not readily available at primary healthcare (PHC) facilities. In such settings, PN would contribute to a reduction in the community burden of STIs through the treatment of undiagnosed infections in asymptomatic sexual contacts.
There are a number of PN strategies in clinical practice. These include provider-orientated methods, where healthcare providers contact partners of index cases to arrange treatment, and a mixed or 'two-step' strategy in which clients are asked to refer their sexual contacts, failing which healthcare providers fulfil this role.[4] Expedited partner treatment (EPT) refers to a scenario in which index cases deliver medication to their sexual contacts, without the partner having to attend a healthcare facility and undergo medical examination.[4] However, owing to the resource and cost implications associated with the above strategies, a client-initiated PN approach is implemented in many developing countries.[5] In SA, sexual partner management at PHC facilities involves the use of anonymous 'contact slips' indicating the STI syndrome of the index case, which patients deliver to their sexual partners.[3,6]
As the client-orientated PN approach relies solely on the index case's willingness to communicate their STI diagnosis, an understanding of the perceived barriers to this approach is of the utmost importance. An SA study by Wood et al[7] demonstrated that these barriers may include inadequate knowledge regarding STI transmission and concerns regarding adverse partner reactions such as intimate partner violence and abandonment, as well as fear of accusations of infidelity and stigmatisation. These barriers are commonly cited in studies investigating PN in developing countries.[5]
There is a paucity of studies investigating PN intentions in SA. The few published studies have either been conducted in specific populations such as university students,[8] pregnant women[9] and men in the minibus transport industry,[10] or in a single province,[7,11-13] thereby limiting their generalisability. We sought to explore demographic, sexual behavioural and clinical characteristics associated with intention to notify sexual partners among symptomatic STI service attendees at sentinel PHC facilities in three SA provinces.
Methods
Study design
This was a cross-sectional STI aetiological surveillance study conducted by the National Institute for Communicable Diseases during 2019 - 2020.
Setting
The study was conducted in three sentinel PHC facilities located in three SA provinces: Gauteng Province (GP), KwaZulu-Natal (KZN) and Western Cape (WC). These are urban PHC facilities in the public health sector that were selected based on a patient load of at least 25 MUS cases per month, space availability for study surveillance officers (professional nurses), and clinic centrality for ease of sample logistics.
Participants
Consecutive adult (>18 years) male and female STI service attendees presenting with MUS, vaginal discharge syndrome (VDS) and/or genital ulcer syndrome (GUS) were invited to participate. Participants were enrolled following assessment of eligibility by trained surveillance officers, which included informed consent procedures for study participation as well as sample collection and storage for future research. Each participant was assigned a unique survey identification number that was used to link questionnaire and laboratory data, and personal identifiers were removed in order to maintain participant anonymity and confidentiality.
Data collection
Demographic, sexual behavioural and clinical characteristics were collected using both paper-based (2019) and electronic surveillance officer-administered questionnaires (2020). Participants self-reported their age, race and sexual orientation, and provided information regarding condom use at last sexual encounter, number of sexual partners during the preceding 3 months, and type (regular/casual) and place of residence (in or outside of enrolment province or SA) of their most recent sexual partners. Participants also self-reported their willingness to refer their most recent sexual partners for STI treatment, and associated reasons if they declined. These questions were phrased to assess general PN intentions for all sexual partners during the preceding 3-month period and were not asked separately for each partner or for different partner types.
Clinical variables included participants' knowledge of their HIV status, self-reported HIV status, self-reported treatment for STIs during the preceding 12 months, and self-reported non-resolution of STI symptoms despite treatment during the preceding 3 months.
Sample collection
A 10 mL venous blood sample was collected from each participant for serological testing.
Laboratory procedures Serological testing
Sera were tested for HIV (HIV Ag/Ab Combo Assay) using the Architect i1000SR system (Abbott GmbH, Germany).
Data analyses
Sample size considerations
The sentinel surveillance had a planned sample size of 150 males with MUS, 100 females with VDS and 100 participants with GUS per sentinel site. These sample sizes were calculated to measure: (i) Neisseria gonorrhoeae positivity of 70 - 80% among males with MUS and at least 100 viable gonococcal isolates for antimicrobial resistance testing; (ii) N. gonorrhoeae positivity of 10 - 20% among females with VDS; and (iii) ulcer-derived herpes simplex virus positivity of 60 - 70% among attendees with GUS, assuming an alpha level of 0.05 and power of 80%. Post hoc power calculations were performed to determine the power of the analyses done given the sample sizes.
Secondary data analyses
Data were extracted, cleaned and exported into Stata 14.2 (StataCorp, USA) for analysis. Continuous data were described using medians and interquartile ranges (IQRs), while proportions were used to describe categorical variables. PN intent was reported as a proportion with an estimated 95% confidence interval (CI). Factors associated with STI clients' willingness to notify their sexual partners of their diagnosis and refer them for STI treatment were investigated and further stratified by gender. Univariable and multivariable Poisson regression models with robust error variance were used to determine factors associated with participants' intent to notify sexual partners and were reported as relative risks (prevalence rate ratios) associated with PN intent with 95% CIs. Variables that had p-values <0.2 in univariable analyses were included in the multivariable analyses with age included a priori.
Ethical considerations
Ethics approval for STI surveillance was granted by the University of the Witwatersrand Human Research Ethics Committee (Medical) (ref. no. M160667).
Results
Demographic and sexual behavioural characteristics
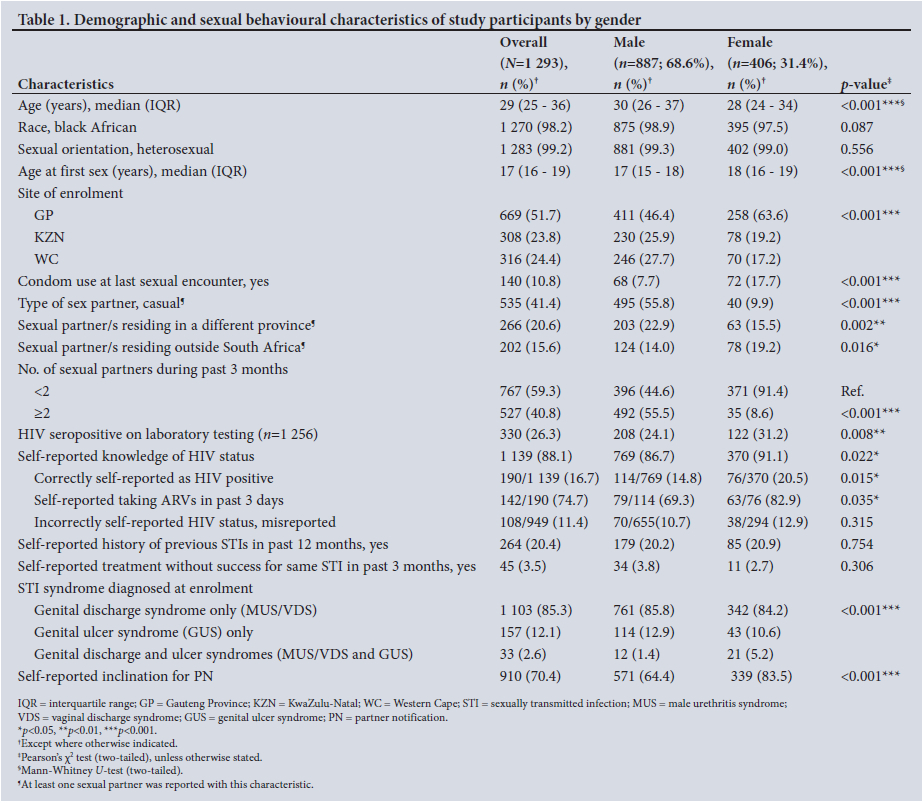
A total of 1 293 STI service attendees were enrolled during the surveillance period. They comprised 887 (68.6%) male and 406 (31.4%) female attendees.
The demographic, behavioural and clinical characteristics of male and female participants are presented in Table 1. The median (IQR) age for males was 30 (26 - 37) years, compared with 28 (24 - 34) years for females. The age of sexual debut also differed by gender and was higher among females compared with males (Table 1). The majority of the participants were enrolled at the Gauteng site (n=669; 51.7%).
Sexual behavioural factors differed significantly by gender, with a significantly lower proportion of male participants compared with females reporting condom use at their last sexual encounter (7.7% v. 17.7%; p<0.001), and higher proportions of males reporting casual relationships (55.8% v. 9.9%; p<0.001) and multiple sexual partners (>2) during the past 3 months (55.5% v. 8.6%; p<0.001). Female participants were more likely to have sexual partners residing in another country, while a higher proportion of men reported sexual partners residing in another SA province.
For 1 256 participants in whom HIV serological testing was performed, the overall HIV seroprevalence was 26.3%, with HIV seropositivity significantly higher in adult females presenting with STIs compared with males (31.2% v. 24.1%; p=0.008). The majority of participants self-reported knowledge of their HIV status (88.1%), with women demonstrating notably superior self-reported knowledge compared with men (91.1% v. 86.7%; p=0.022), and higher proportions of women correctly self-reporting as HIV seropositive (20.5% v. 14.8%; p=0.015) and initiating and adhering to antiretroviral therapy (ART) (82.9% v. 69.3%; p=0.035) (Table 1). Among the participants without self-reported knowledge of their HIV status, the majority (n=118/154; 76.7%) were men (data not shown). The proportion of participants self-reporting STI treatment during the preceding 12 months or treatment without success for the same syndrome during the previous 3 months did not differ by gender.
PN intentions of STI service attendees
Among male attendees, the achieved sample size provided 96% power to detect willingness to refer most recent sexual partners of 65% ± 3%, assuming α=0.05, while among females the achieved sample size provided 89% power to detect willingness to refer most recent sexual partners of 83% ± 3%.
Self-reported PN intentions were higher among women than among men (83.5% v. 64.4%; p<0.001) (Table 1). A trend towards lower PN intent was observed in HIV-positive participants who self-reported being HIV positive but had not yet initiated ART (data not shown).
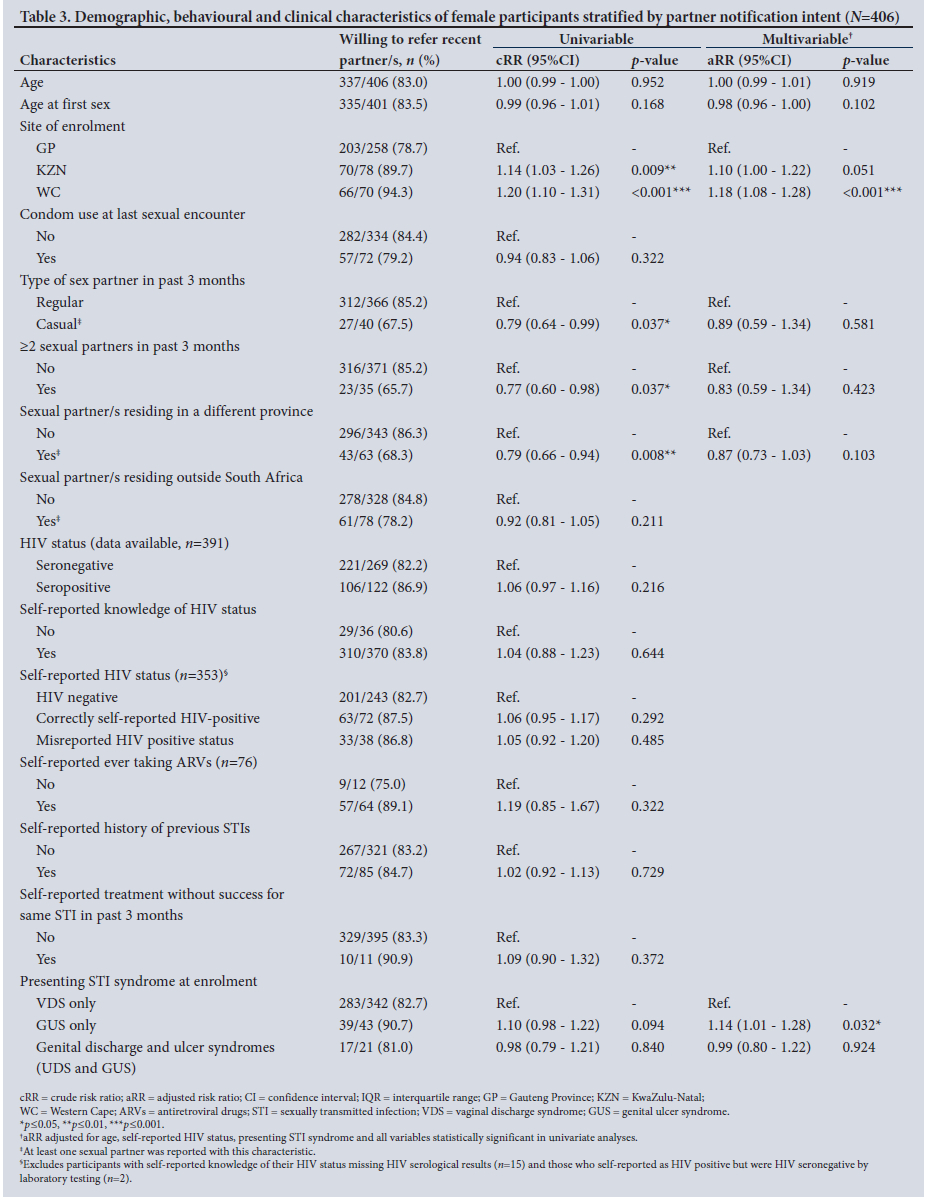
We further stratified our analyses of PN intent by participant gender. Univariable analyses (Tables 2 and 3) revealed that non-regular (casual) sexual partners, as well as having >2 sexual partners during the preceding 3 months, were factors consistently associated with partner non-referral across both genders.
In the univariable analysis, male participants in KZN and WC were 38% and 25% less willing, respectively, to refer their partners compared with men enrolled in GP. Interestingly, self-reported knowledge of HIV status among male attendees was associated with lower PN intent (p=0.021). Furthermore, men self-reporting STI diagnosis and treatment during the preceding 12 months were also 22% less likely to be willing to inform their sexual partners of their current STI diagnosis compared with men not self-reporting a previous STI diagnosis.
Self-reported PN intent was higher among men with sexual partners residing outside SA, as well as among men presenting with genital ulcers compared with those presenting with urethral discharge (Table 2). Multivariable analyses, adjusted for age, presenting STI and self-reported HIV status as well as all variables shown to be significant on univariate analyses, revealed that partner non-referral in male service attendees was independently associated with enrolment at the KZN site, as well as with having casual sex partners during the past 3 months (Table 2).
Univariate analysis of data from female participants revealed that those enrolled in GP were less likely to inform their sexual partners compared with those in KZN and WC (Table 3). PN intentions were also 21% lower for women with sexual partners residing in a different SA province. In contrast to the results observed for men, STI diagnosis and treatment during the preceding 12 months and self-reported HIV status did not influence PN intent among female participants (Table 3). After adjusting for age, age at first sex, site of enrolment, presenting STI syndrome and casual partner type, multiple sexual partners and sexual partners residing in a different province during the past 3 months, enrolment at the GP site was independently associated with lower PN intentions among female participants. The presence of genital ulcers was shown to be an independent motivator towards PN intent among female service attendees.
Reasons for partner non-referral
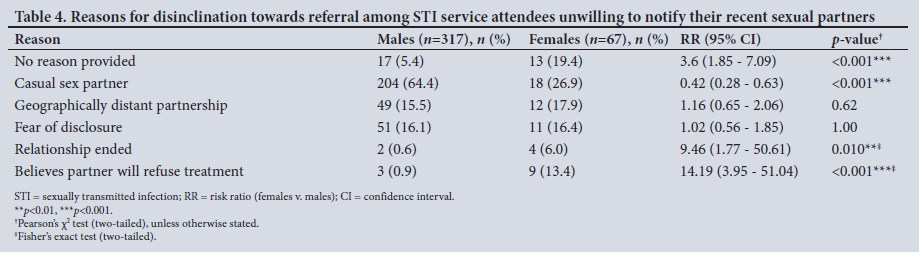
Of the 384 STI service attendees who did not intend to disclose their STI diagnosis and inform their sexual partners, female participants were more likely than males to not provide a reason for non-referral.
The primary reason associated with a lack of PN intent among both men and women was the casual nature of the sexual relationship, followed by geographical distance between partners and fear of disclosure. Compared with male STI service attendees, women were significantly more likely to report termination of the relationship, as well as the belief that their partner would not seek treatment, as motives for their inclination not to refer (Table 4).
Discussion
In this study we investigated the demographic, sexual behavioural and clinical characteristics that serve as either facilitators or barriers to PN among STI service attendees in SA. We found that a large proportion of adults (64.4% of males and 83.5% of females) presenting to PHC facilities with STI syndromes were reportedly willing to refer their recent sexual partners for STI treatment. We found that female participants had a greater willingness to notify their partners than their male counterparts, a finding consistent with previous reports from SA[12,14] and other sub-Saharan African countries,[15] which has been attributed to awareness of their partner's concurrent relationships with other women and the importance of PN to prevent their own reinfection.[7]
Our data reveal that the greatest behavioural barrier to PN among both men and women was engaging in casual sex partnerships. The reduced likelihood of referring casual partners has been reported regularly,[11,16] and was independently associated with non-referral among male STI service attendees in our study. This finding may be attributed to difficulties in contacting these sexual partners or lack of concern for the wellbeing of a non-regular partner.[5,17] Kalichman et al.[16] failed to find an association between number of sexual partners and intentions of STI service attendees in Cape Town to notify their partners. This is in keeping with our data, where, after adjusting for other factors in the multivariable model, having multiple sex partners was not associated with PN decisions among both men and women with symptomatic STIs.
We also report, for the first time in SA, differences in PN intentions among STI service attendees based on the province of enrolment of the index case. Men enrolled outside GP had lower PN intentions, with those enrolled in KZN being least likely to notify their sexual partners. It is noteworthy to add that at the GP surveillance site a male counsellor is employed in addition to the female surveillance officer, while only female professional nurses are employed at the KZN and WC sites. It has been shown that men prefer PN counselling offered by male healthcare workers,[17] and the presence of a male counsellor may have improved PN intentions of men enrolled in GP. Conversely, willingness to refer sexual partners by female participants enrolled in GP was lower than at the other sites. This finding may be ascribed to the fact that the majority of women who reported sexual partners residing in a different province (n=61/63; 96.8%) or another country (n=76/78; 97.4%) (data not shown) were enrolled in GP. Geographically distant partnerships were associated with lower PN intent among females, while this factor appeared to be a facilitator to PN among men, again highlighting gender-based differences. The hesitancy associated with referral of partners who live far away may be partially attributed to the fact that face-to-face notification is repeatedly described as the preferred STI PN method for long-term partners among SA individuals.[7,18] Women in Botswana have similarly reported delayed PN as a consequence of not wanting to disclose their STI diagnosis by telephonic communication.[19] Further research is warranted to understand additional factors (societal, cultural and healthcare associated) that may account for the disparate PN intentions observed across provinces. Women were also more likely than men to cite the dissolution of relationships as well as their partners' aversion to seeking healthcare in explanation of their PN hesitancy, although relatively few participants reported these reasons. This finding aligns with other studies, in one of which female university students in SA showed a trend towards non-referral of ex-partners compared with their male counterparts (56.5% v. 50.2%; p=0.099),[8] while pregnant women in Botswana similarly revealed that their partner's reluctance to access healthcare would hinder PN and treatment efforts.[19]
Other personal barriers to PN have been described, including financial dependence on sexual partners and fears that disclosure would result in loss of material support, as well as not wanting extramarital relationships to be revealed.[5] Healthcare-associated barriers may also hinder patient-intiated strategies through the inconsistent provision of 'contact slips'. A national evaluation of STI service delivery in primary PHC facilities in SA revealed that only 70.2% of standardised patient actors were offered these slips or counselling, with female service attendees significantly less likely to be offered these services.[6] Although not communicated by participants in our study, these factors may still be relevant to our setting and should be considered in strategies to improve PN outcomes.
Our observation that female participants presenting with genital ulcers were more likely to intend to refer their sexual partners compared with those with genital discharge syndrome is in keeping with univariate data from female STI attendees in Cape Town[11] and may be due to the conspicuous and painful nature of these lesions, as has been described previously.[17]
In SA, few studies have investigated provider-initiated notification approaches, but when offered, these methods were rarely requested (n=1/350; 0.3%).[20] A recent systematic review revealed the limited acceptability by STI clients of electronic PN via e-cards or text messaging, owing to their anonymous and impersonal nature.[21] Text messaging has been shown to have some level of acceptability among SA university students[8] and highly mobile men in the minibus transport industry,[10] although the actual uptake of these services for PN was not assessed in these studies. EPT has been shown to have limited acceptability by STI patients in Botswana,[22] while uptake was high among HIV-negative female STI service attendees in KZN (87%)[23] and Kenyan women accessing HIV pre-exposure prophylaxis (94%).[24] The acceptability and uptake of EPT by heterosexual men in sub-Saharan Africa has yet to be comprehensively investigated. Support for a dual-referral approach has been reported in SA,[18] in which STI patients inform their partners of their STI exposure, followed by telephonic confirmation and emphasis on the importance of treatment by a healthcare provider.
Overall, these studies suggest that PN strategies may need to be tailored for different populations. Based on the data we present here, alternative approaches such as electronic technologies and provider-assisted strategies should be considered for casual and geographically distant sex partners, as well as for index cases who cite fear of disclosure or partner hesitancy as barriers to partner referral. Such strategies would bolster efforts at reducing the incidence of STIs through intensified PN, as outlined in the 2017 - 2022 South African National Strategic Plan for HIV, TB and STIs[25l and the World Health Organization's Strategic Direction 2.[4
Our study had several limitations. Many of the outcomes assessed were based on self-reporting, and social desirability bias may have resulted in inflated STI PN intentions for our cohort. Data were not collected at an individual partner level, so distinct notification intentions for specific partner types or numbers could not be explored. Furthermore, successful PN and treatment rates were not recorded or quantified. Our questionnaire did not include other behavioural variables such as participant education and employment status, substance (alcohol and drug) use or HIV-serodiscordant partnerships, and we did not assess self-perceived risk, knowledge of STI symptoms and mode of transmission among participants, which have been described as influencing PN intentions.[9,1U2,15,161 Additionally, our findings are only a reflection of the urban population and may differ from those for STI service attendees in rural settings. Furthermore, as our study was limited to STI service attendees enrolled at three sentinel sites, we cannot assume that the findings presented here can be generalised to the broader population of adults seeking STI treatment services in SA.
Conclusion
This study contributes to the body of evidence demonstrating that demographic (gender, province of residence) and behavioural (sexual partner type) characteristics as well as relationship dynamics (geographical distance and power imbalance) may influence the PN intentions of STI service attendees in SA.
Declaration. None.
Acknowledgements. The authors thank the surveillance officers Ms Valencia Kekana, Mr Alex Vezi, Ms Zukiswa Mithani and Ms Nokuthula Nzuza, as well as Ms Thabitha Mathega for data entry and management.
Author contributions. RSK conceptualised the study. BDCD and TK performed the statistical analyses. BDCD drafted the manuscript. All authors contributed to the review and editing of the manuscript and approved the final version.
Funding. None.
Conflicts of interest. None.
References
1. Kularatne RS, Niit R, Rowley J, et al. Adult gonorrhea, chlamydia and syphilis prevalence, incidence, treatment and syndromic case reporting in South Africa: Estimates using the Spectrum-STI model, 1990 - 2017. PLoS ONE 2018;13(10):e0205863. https://doi.org/10.1371/journal.pone.0205863 [ Links ]
2. National Integrated District Health Information System. https://za.dhis.dhmis.org/dhis-web-commons/security/login.action (accessed 8 October 2021). [ Links ]
3. National Department of Health, South Africa. Sexually transmitted infections: Management guidelines 2018. https://www.health.gov.za/wp-content/uploads/2020/11/sti-guidelines-27-08-19.pdf (accessed 8 October 2021). [ Links ]
4. World Health Organization. Global health sector strategy on sexually transmitted infections, 2016 - 2021. 3 October 2016. https://www.who.int/publications/i/item/WHO-RHR-16.09 (accessed 8 October 2021). [ Links ]
5. Alam N, Chamot E, Vermund SH, Streatfield K, Kristensen S. Partner notification for sexually transmitted infections in developing countries: A systematic review. BMC Public Health 2010;10:19. https://doi.org/10.1186/1471-2458-10-19 [ Links ]
6. Kohler PK, Marumo E, Jed SL, et al. A national evaluation using standardised patient actors to assess STI services in public sector clinical sentinel surveillance facilities in South Africa. Sex Transm Infect 2017;93(4):247-252. https://doi.org/10.1136/sextrans-2016-052930 [ Links ]
7. Wood JM, Harries J, Kalichman M, et al. Exploring motivation to notify and barriers to partner notification of sexually transmitted infections in South Africa: A qualitative study. BMC Public Health 2018;18:980. https://doi.org/10.1186/s12889-018-5909-4 [ Links ]
8. Mokgatle MM, Madiba S, Cele L. A comparative analysis of risky sexual behaviors, self-reported sexually transmitted infections, knowledge of symptoms and partner notification practices among male and female university students in Pretoria, South Africa. Int J Environ Res Public Health 2021;18(11):5660. https://doi.org/10.3390/ijerph18115660 [ Links ]
9. Green H, Taleghani S, Nyemba D, Myer L, Davey DJ. Partner notification and treatment for sexually transmitted infections among pregnant women in Cape Town, South Africa. Int J STD AIDS 2020;31(13):1282-1290. https://doi.org/10.1177/0956462420949789 [ Links ]
10. Mokgatle MM, Madiba S. Risky sexual behaviour amidst predicament of acceptable sexually transmitted infection partner notification modalities: A cross-sectional survey amongst minibus taxi drivers in Gauteng Province, South Africa. S Afr Fam Pract 2020;62(1):e1-e6. https://doi.org/10.4102/safp.v62i1.5165 [ Links ]
11. Mathews C, Kalichman MO, Laubscher R, et al. Sexual relationships, intimate partner violence and STI partner notification in Cape Town, South Africa: An observational study. Sex Transm Infect 2018;94(2):144-150. https://doi.org/10.1136/sextrans-2017-053434 [ Links ]
12. Meyer-Weitz A, Reddy P, van den Borne B, Kok G, Pietersen J. Determinants of communication between partners about STD symptoms: Implications for partner referral in South Africa. S Afr Fam Pract 2006;48(7):17-17d. https://doi.org/10.1080/20786204.2006.10873421 [ Links ]
13. Kalichman S, Banas E, Kalichman M, et al. Brief enhanced partner notification and risk reduction counseling to prevent sexually transmitted infections, Cape Town, South Africa. Sex Transm Dis 2021;48(3):174-182. https://doi.org/10.1097/olq.0000000000001295 [ Links ]
14. Chitneni P, Beksinska M, Dietrich JJ, et al. Partner notification and treatment outcomes among South African adolescents and young adults diagnosed with a sexually transmitted infection via laboratory-based screening. Int J STD AIDS 2020;31(7):627-636. https://doi.org/10.1177/0956462420915395 [ Links ]
15. Taleghani S, Joseph-Davey D, West SB, et al. Acceptability and efficacy of partner notification for curable sexually transmitted infections in sub-Saharan Africa: A systematic review. Int J STD AIDS 2019;30(3):292-303. https://doi.org/10.1177/0956462418803983 [ Links ]
16. Kalichman SC, Mathews C, Kalichman M, Lurie MN, Dewing S. Perceived barriers to partner notification among sexually transmitted infection clinic patients, Cape Town, South Africa. J Public Health 2017;39(2):407-414. https://doi.org/10.1093/pubmed/fdw051 [ Links ]
17. Moyo W, Chirenje ZM, Mandel J, et al. Impact of a single session of counseling on partner referral for sexually transmitted disease treatment, Harare, Zimbabwe. AIDS Behav 2002;6(3):237-243. https://doi.org/10.1023/A:1019891808383 [ Links ]
18. National Department of Health, South Africa. A national evaluation of sexually transmitted infection services in public sector clinical sentinel surveillance facilities, in South Africa. October 2015. https://www.go2itech.org/wp-content/uploads/2017/07/STI-Services-reportLC_7-2017.pdf (accessed 8 October 2021). [ Links ]
19. Wynn A, Moucheraud C, Moshashane N, et al. Using partner notification to address curable sexually transmitted infections in a high HIV prevalence context: A qualitative study about partner notification in Botswana. BMC Public Health 2019;19:606. https://doi.org/10.1186/s12889-019-6813-2 [ Links ]
20. Mathews C, Lombard C, Kalichman M, et al. Effects of enhanced STI partner notification counselling and provider-assisted partner services on partner referral and the incidence of STI diagnosis in Cape Town, South Africa: Randomised controlled trial. Sex Transm Infect 2021;97(1):38-44. https://doi.org/10.1136/sextrans-2020-054499 [ Links ]
21. Pellowski J, Mathews C, Kalichman MO, et al. Advancing partner notification through electronic communication technology: A review of acceptability and utilisation research. J Health Commun 2016;21(6):629-637. https://doi.org/10.1080/10810730.2015.1128020 [ Links ]
22. Hansman E, Wynn A, Moshashane N, et al. Experiences and preferences with sexually transmitted infection care and partner notification in Gaborone, Botswana. Int J STD AIDS 2021;32(13):1250-1256. https://doi.org/10.1177/09564624211033231 [ Links ]
23. Garrett NJ, Osman F, Maharaj B, et al. Beyond syndromic management: Opportunities for diagnosis-based treatment of sexually transmitted infections in low- and middle-income countries. PLoS ONE 2018;13(4):e0196209. https://doi.org/10.1371/journal.pone.0196209 [ Links ]
24. Omollo V, Bukusi EA, Kidoguchi L, et al. A pilot evaluation of expedited partner treatment and partner HIV self-testing among adolescent girls and young women diagnosed with Chlamydia trachomatis and Neisseria gonorrhoeae in Kisumu, Kenya. Sex Transm Dis 2021;48(10):766-772. https://doi.org/10.1097/olq.0000000000001430 [ Links ]
25. South Africa. National Strategic Plan for HIV, TB and STIs 2017 - 2022. 2016. https://www.gov.za/sites/default/files/gcis_document/201705/nsp-hiv-tb-stia.pdf (accessed 8 October 2021). [ Links ]
 Correspondence:
Correspondence:
B Da Costa Dias
biancad@nicd.ac.za
Accepted 12 September 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}