










Servicios Personalizados
Articulo
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 no.2 Pretoria feb. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i2.16643
RESEARCH
Implementation of self-monitoring of blood glucose for patients with insulin-dependent diabetes at a rural non-communicable disease clinic in Neno, Malawi
T RudermanI, *; G FerrariII, III, *; F ValetaIV; M BotiV; K KumwendaV; P H ParkVI, VII, VIII; G NgogaIX, X, XI; E NdaramaXII; E ConnollyXIII, XIV, XV; G BukhmanXVI, XVII, XVIII, †; A AdlerXIX, †
IDO; Partners in Health, Neno, Malawi
IIMSN, MPH; NCD Synergies project, Partners in Health, Boston, Mass., USA
IIIMSN, MPH; Division of Global Health Equity, Brigham and Women's Hospital, Boston, Mass., USA
IVRN, MPH; Program in Global Noncommunicable Disease and Social Change, Department of Global Health and Social Medicine, Harvard Medical School, Boston, Mass., USA
VBSc; Program in Global Noncommunicable Disease and Social Change, Department of Global Health and Social Medicine, Harvard Medical School, Boston, Mass., USA
VIMD; NCD Synergies project, Partners in Health, Boston, Mass., USA
VIIMD; Division of Global Health Equity, Brigham and Women's Hospital, Boston, Mass., USA
VIIIMD; Program in Global Noncommunicable Disease and Social Change, Department of Global Health and Social Medicine, Harvard Medical School, Boston, Mass., USA
IXRN; NCD Synergies project, Partners in Health, Boston, Mass., USA
XRN; Noncommunicable Disease Program, Partners in Health, Rwanda
XIRN; Non-Communicable Diseases Division, Rwanda Biomedical Center, Kigali, Rwanda
XIIMBBS; Ministry of Health and Populations, Neno, Malawi
XIIIDO, MPH; Partners in Health, Neno, Malawi
XIVDO, MPH; Division of Pediatrics, University of Cincinnati College of Medicine, Ohio, USA
XVDO, MPH; Division of Hospital Medicine, Cincinnati Children's Hospital Medical Center, Ohio, USA
XVIMD, PhD; NCD Synergies project, Partners in Health, Boston, Mass., USA
XVIIMD, PhD; Division of Global Health Equity, Brigham and Women's Hospital, Boston, Mass., USA
XVIIID, PhD; Program in Global Noncommunicable Disease and Social Change, Department of Global Health and Social Medicine, Harvard Medical School, Boston, Mass., USA
XIXPhD; Division of Global Health Equity, Brigham and Women's Hospital, Boston, Mass., USA
ABSTRACT
BACKGROUND. Self-monitoring of blood glucose (SMBG) is a widely accepted standard of practice for management of insulin-dependent diabetes, yet is largely unavailable in rural sub-Saharan Africa (SSA). This prospective cohort study is the first known report of implementation of SMBG in a rural, low-income country setting.
OBJECTIVES. To evaluate adherence and change in clinical outcomes with SMBG implementation at two rural hospitals in Neno, Malawi.
Methods. Forty-eight patients with type 1 and insulin-dependent type 2 diabetes were trained to use glucometers and logbooks. Participants monitored preprandial glucose daily at rotating times and overnight glucose once a week. Healthcare providers were trained to evaluate glucose trends, and adjusted insulin regimens based on results. Adherence was measured as the frequency with which patients checked and documented blood glucose at prescribed times, while clinical changes were measured by change in glycated haemoglobin (HbA1c) over a 6-month period.
RESULTS. Participants brought their glucometers and logbooks to the clinic 95 - 100% of the time. Adherence with measuring glucose values and recording them in logbooks eight times a week was high (mean (standard deviation) 69.4% (15.7) and 69.0% (16.6), respectively). Mean HbA1c decreased from 9.0% (75 mmol/mol) at enrolment to 7.8% (62 mmol/mol) at 6 months (mean difference 1.2% (95% confidence interval (CI) 0.6 - 2.0; p=0.0005). The difference was greater for type 1 diabetes (1.6%; 95% CI 0.6 - 2.7; p=0.0031) than for type 2 diabetes (0.9%; 95% CI 0.1 - 1.9; p=0.0630). There was no documented increase in hypoglycaemic events, and no hospitalisations or deaths occurred.
CONCLUSION. SMBG is feasible for patients with insulin-dependent diabetes in a rural SSA population, and may be associated with improved HbA1c levels. Despite common misconceptions, all patients, regardless of education level, can benefit from SMBG. Further research on long-term retention of SMBG activities and the benefits of increasing frequency of monitoring is warranted.
Diabetes is a chronic non-communicable disease (NCD) of growing public health concern and with an increasing incidence worldwide. Africa has the fastest-growing prevalence of diabetes, with estimates predicting a 47.5% increase by 2030 to 28.6 million people.[1] Furthermore, the rural poor bear a disproportionate burden of NCDs without typical risk factors associated with urbanisation, such as obesity.[2,3] While it is unclear whether the aetiology of diabetes in the sub-Saharan African (SSA) setting differs from that in North America and Europe, cases are still typically classified as type 1 and type 2 diabetes.[4] In Malawi, 84% of the population lives in rural settings and 65% survive on less than USD1 per day.[5,6] While the national burden of diabetes in adults is estimated to be 1.4 - 3.0%,[1] a recent population-based study found that 41% of participants with diabetes were undiagnosed, suggesting that the actual burden may
be much higher.[7,8] Human insulin is procured by the Malawian government and provided free of charge to patients through public facilities, although availability can be limited.[9] Home glucometers and test strips must be purchased privately and are inaccessible and unaffordable to most patients living in rural communities.
There are two forms of diabetes that require exogenous insulin administration. Type 1 diabetes is an autoimmune condition characterised by impaired secretion of insulin from pancreatic islet cells and is typically diagnosed in childhood or young adulthood. Type 2 diabetes is characterised by resistance to insulin and is typically diagnosed in adulthood. Although type 2 diabetes can initially be managed with lifestyle modifications and oral medications that increase insulin sensitivity or production, exogenous insulin administration is often required as the condition progresses.
Uncontrolled diabetes is common in SSA and leads to individual disability, mortality, and strain on health systems.[10] All patients who use insulin face an increased risk of severe hypoglycaemia and increased self-care challenges, including the necessity for frequent self-monitoring of blood glucose, multiple daily injections, and strict dietary management.[2,10,11]
Glycaemic control is an essential element of diabetes care and reduces the risk of short- and long-term complications.[12] While insulin is increasingly being considered an essential medicine and is supplied by health systems in many countries, access to blood glucose meters and test strips remains extremely limited.[13,14] Self-monitoring of blood glucose (SMBG) has been the standard of care for diabetes in high-income countries since the transition from self-monitoring of urinary glucose in the 1980s.[15]SMBG impacts on glycaemic control both by increasing patient awareness of blood glucose levels and by providing information to healthcare providers that enables more accurate titration of insulin doses. Monitoring blood glucose levels at home has proved to be feasible and acceptable in high-resource settings, and an increased frequency of SMBG is linked to lower levels of glycated haemoglobin (HbA1c).[12,16] Global guidelines emphasise the value of SMBG for ensuring safety, preventing complications, and promoting individual self-management in patients with diabetes, especially those using insulin.[16-18] Despite these clear guidelines, SMBG use remains infrequent in low-income rural settings. To our knowledge, there are no current data on adherence to and the clinical impact of SMBG for the rural poor living with diabetes in SSA, and this is the first study to measure adherence to and effectiveness of SMBG in rural low-income SSA.
Cost, access, patient literacy and adherence are all potential or perceived barriers to SMBG in low-resource settings. Previous research on SMBG in the African region has focused on urban or tertiary care facilities.[14,19-23] In Malawi, in a recent cross-sectional survey of adolescents with type 1 diabetes receiving care at tertiary hospitals, only 20% were using glucose meters.'24' Variability in criteria used to define adherence makes comparison across studies difficult. Studies focusing on glycaemic control in SSA have not been conclusive in demonstrating a correlation between SMBG and glycaemic control. However, these studies have primarily been carried out at urban medical centres, demonstrated low adherence to SMBG, and included patients with non-insulin-dependent type 2 diabetes.'19,25' The impact of SMBG on HbA1c has been shown to be stronger for type 1 than type 2 diabetes.'19,26' Studies based in urban medical centres may not be generalisable to rural populations, given the increased challenges of care provision and reduced literacy in the rural setting. A randomised controlled trial evaluating SMBG feasibility in rural patients with insulin-dependent type 2 diabetes in Rwanda is in progress.'27' As previous research on SMBG has not included patients in resource-limited rural communities and perceived barriers to quality care have not been examined, it is necessary to evaluate adherence to and the impact of SMBG for these patients. We present the findings of a cohort study examining adherence and clinical outcomes with introduction of SMBG to insulin-dependent patients in a rural district hospital clinic in Malawi.
Methods
Setting and population
Neno is a rural district with a population of 138 291 according to the Malawi census of 2018, located in the southern region of Malawi.[6] Most people in Neno rely on subsistence agriculture and fewer than 5% have access to electricity. The literacy rate, defined as being able to read and write a simple sentence, is 70%.[6] Neno's local health system is primarily public and comprises a district hospital in Neno centre, a smaller community hospital in the town of Lisungwi, and 12 additional healthcare centres distributed throughout the district. Partners in Health (PIH), a US-based non-governmental organisation known locally as Abwenzi Pa Za Umoyo, has partnered with the Ministry of Health (MoH) since 2007 in order to improve healthcare and socioeconomic development in Neno.
In Malawi, like many parts of SSA, it is difficult for patients in rural districts to receive care for severe NCDs, including type 1 and insulin-dependent type 2 diabetes, sickle cell disease and rheumatic heart disease, because most specialty clinics are at central referral hospitals. Most decentralised models of care, such as the World Health Organization (WHO) Package of Essential Non-communicable Disease Interventions (WHO PEN), focus on addressing common NCDs, such as hypertension and non-insulin-dependent type 2 diabetes, at primary healthcare centres.'28' In Neno, patients with common NCDs are treated at the Integrated Chronic Care Clinics, a unique model that provides longitudinal care for patients with HIV and NCDs.'29' At the same time, integrated services for more severe and complex NCDs, such as insulin-dependent diabetes, are provided through the PEN-Plus model. PEN-Plus is a strategy for providing outpatient treatment of chronic, severe NCDs at specialised clinics based in rural district hospitals.[3,30] This model builds on the WHO PEN approach and promotes decentralisation through structured training of nurses and other mid-level healthcare providers.[31-36]
Two PEN-Plus clinics, known locally as advanced NCD (aNCD) clinics, have been operating in Neno since November 2018. The clinics are run by clinical officers and nurses, with supervision by a doctor and a nurse mentor. Patients with diabetes who use insulin are seen at the clinics on a monthly basis. Insulin regimens are created and titrated based on clinical protocols that take into account multiple factors including patient symptoms, monthly fasting blood sugar levels taken at the clinic, and twice-yearly HbA1c levels. Most insulin regimens include a combination of intermediate-acting insulin (neutral protamine Hagedorn, NPH) and short-acting insulin (regular). Patients typically inject a fixed dose of intermediate- and short-acting insulin twice a day, before breakfast and before dinner. Oral regimens for patients with type 2 diabetes are adjusted as necessary.
Study design
This was a prospective 6-month cohort study evaluating patient adherence and clinical outcomes with introduction of home SMBG among patients with insulin-dependent diabetes in a rural NCD clinic setting. Prior to SMBG implementation, patients used symptom monitoring while at home and received a fasting blood sugar check monthly during clinic visits. Data collection was done at the same time as site-wide implementation of SMBG for all patients with insulin-dependent diabetes. All insulin-dependent patients aged >18 years receiving care at the aNCD clinic were invited to participate in the study. Children were given the same standard of care but were not included in the study. Twenty-five adults with type 1 diabetes and 23 adults with insulin-dependent type 2 diabetes were eligible and attended their appointment to be enrolled in the study. The aNCD clinic is the only chronic care clinic in Neno treating patients with insulin-dependent diabetes, so all patients in the district were evaluated for enrolment.
Prior to study initiation, NCD clinicians and nurses were trained on the correct technique for using glucometers and providing patient education on glucometer use. Clinicians were further trained to use logbook data to inform insulin dosing decisions. At the start of the study, patients received a half-day training session led by
NCD nurses. They were taught how to use the glucometer, check blood glucose and document values in the logbook. Education also reinforced recognition and treatment of low blood glucose levels. However, the education did not instruct patients to self-adjust insulin dosing outside of clinic visits. This was decided on because there was concern about possible hypoglycaemia if insulin was adjusted based on one blood glucose measurement per day, particularly given that some patients faced inconsistent food availability. Patients were followed up at the aNCD clinic 2 weeks after initial training to ensure that the glucometers were being used appropriately and blood glucose values documented correctly. After the 2-week follow-up, patients returned monthly for regularly scheduled care, data collection, education and insulin titration. Additional patient education was provided as needed.
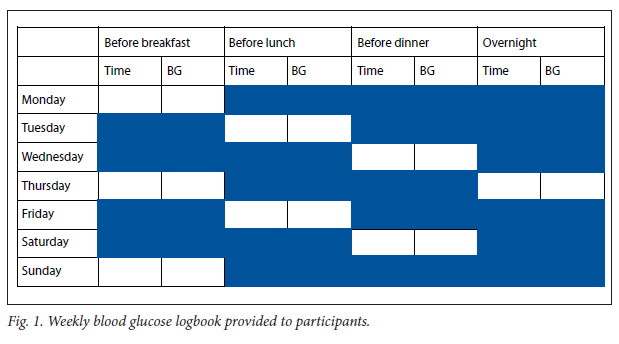
Glucometers, test strips and lancets were provided to all patients enrolled in the study. Logbooks were created to help guide the patients on when to check their blood sugar levels and record the results (Fig. 1). Participants were asked to check preprandial blood sugar once a day, rotating through breakfast, lunch and dinner. They were also asked to check one additional overnight blood glucose per week, resulting in a total of eight prescribed checks per week. HbA1c was measured at baseline and 6 months. Logbooks were used throughout the course of the study to help inform changes to insulin regimens.
Data collection
Demographic data were obtained from structured patient intake forms during enrolment. Point-of-care HbA1c was obtained at baseline and endline using a point-of-care device. Because the glucometers did not have capability to upload to a computer, study staff compared the time-stamped values from the glucometer with those recorded in the logbook, then manually entered glucometer values into an Excel spreadsheet, version 16 (Microsoft, USA). If blood glucose was checked more than once in a day, only the value within an hour of the prescribed time was recorded. At each visit, the interval since the previous visit was noted and all data since the previous visit were collected so that no data were missed if participants missed an appointment.
Outcomes of interest
Adherence was the primary outcome of interest, and was measured by the following variables: (i) whether patients brought their glucometers to the clinic; (ii) whether patients brought their logbooks to the clinic; (iii) the number of days the patients checked their blood glucose during the previous month; (iv) the number of days the patient entered the glucose value correctly in the logbook during the previous month; and (v) the number of days patients both correctly checked their glucose and entered the data into the logbook. HbA1c was the primary clinical outcome of interest. Glycaemic variability, the secondary clinical outcome of interest, was calculated by identifying the percentage of values in a visit interval <70 mg/dL, >180 mg/dL, and in range (70 - 180 mg/dL).
Statistical analysis
Data were analysed using Stata version 15.1 (StataCorp, USA). Owing to the low sample size, demographic variables were grouped into binary or three-tiered groups. For example, education level was grouped by binary groups of none or primary education and secondary or higher. Adherence to SMBG activities was calculated as a proportion by comparing the number of times an activity was completed correctly with the number of times that activity was
expected to have been completed. Change in HbA1c from baseline to endline at 6 months was calculated using a paired f-test.
Ethical considerations
All participants were instructed about the benefits and risks of the study and signed consent forms before starting. Participants were not compensated, because this cohort study was evaluating a new standard of care being implemented for all diabetes patients in the clinic. All patient data were kept secure by password encryption. Ethics approval was obtained from the Malawi National Health Sciences Research Committee (NHSRC) (ref. no. 19/05/2340) and the MoH-PIH Malawi Research Committee.
Results
Study population
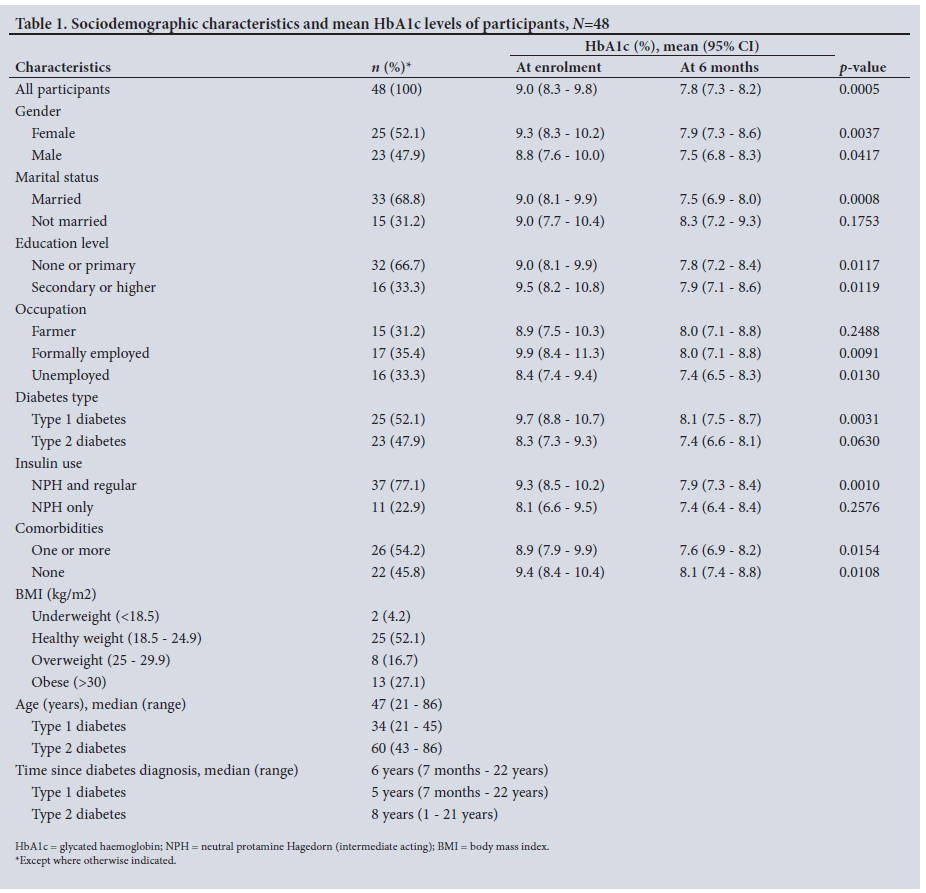
A total of 48 participants were enrolled in and completed the study (Table 1). About half (52.1%; n=25) had type 1 diabetes and the other half (47.9%; n=23) had insulin-dependent type 2 diabetes. The median patient age was 47 years (range 21 - 86), and 52.1% (n=25) of participants were female. Most participants were married (68.8%; n=33) and had no or only primary education (66.7%; n= 32). Participant occupation was evenly divided between subsistence farmer (31.2%; n=15), formal employment (35.4%; n=17) and unemployment (33.3%; n=16). The mean time since diabetes diagnosis was 5 years (range 7 months - 22 years) for participants with type 1 diabetes and 8 years (range 1 - 21 years) for those with type 2 disease. Most participants were using intermediate-acting (NPH) and short-acting (regular) insulins to manage their diabetes (77.1%; n=37), while the remainder were using intermediate-acting insulin only (22.9%; n=11). Twelve patients (25.0%) were also taking metformin. Fifty-four percent of participants (n=26) had one or more comorbidities, the most common being hypertension, while 45.8% (n=22) had no comorbidities (Table 1).
Adherence
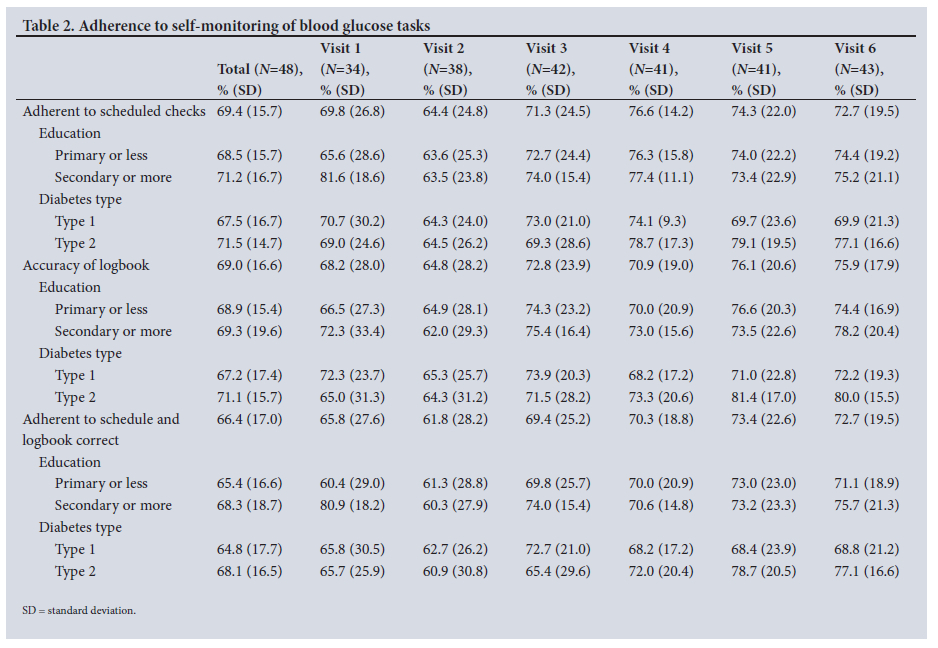
Most patients brought their glucometers and logbooks to the clinic, ranging from 94% to 100% at each visit, with an overall average of 98%. For monthly adherence to scheduled glucose checks, accuracy of logbooks and both these variables, mean (standard deviation) percentages of participants were 69.4% (15.7), 69.0% (16.6) and 66.4% (17.0), respectively (Table 2). Trends highlighted by stratification by education and diabetes type show that participants with primary or no education and those with type 2 diabetes had improved adherence to scheduled checks and accuracy of logbooks over time; however, owing to high levels of variability, these trends were not statistically significant (Table 2).
Clinical data
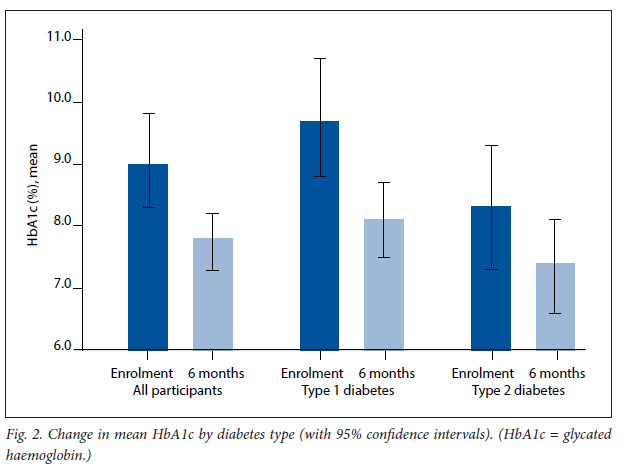
Change in HbA1c was the primary clinical outcome of interest. Mean HbA1c for the cohort decreased from 9.0% (75 mmol/ mol) at enrolment to 7.8% (62 mmol/mol) at 6 months (mean difference 1.2%; 95% confidence interval (CI) 0.6 - 2.0; p=0.0005). Enrolment mean HbA1c was consistent with HbA1c levels of insulin-dependent patients at the clinic over the previous year, which averaged 9.3% (78 mmol/mol) from January to June 2019 (n=18) and 8.8% (73 mmol/ mol) from July to December 2018 (n=8). The mean difference between baseline and endline was greater for patients with type 1 diabetes (1.6%; 95% CI 0.6 - 2.7; p=0.0031) than for those with type 2 disease (0.9%; 95% CI 0.1 - 1.9; p=0.0630) (Fig. 2). When stratified, a significant decrease was seen from baseline to endline for all education levels (Table 1).
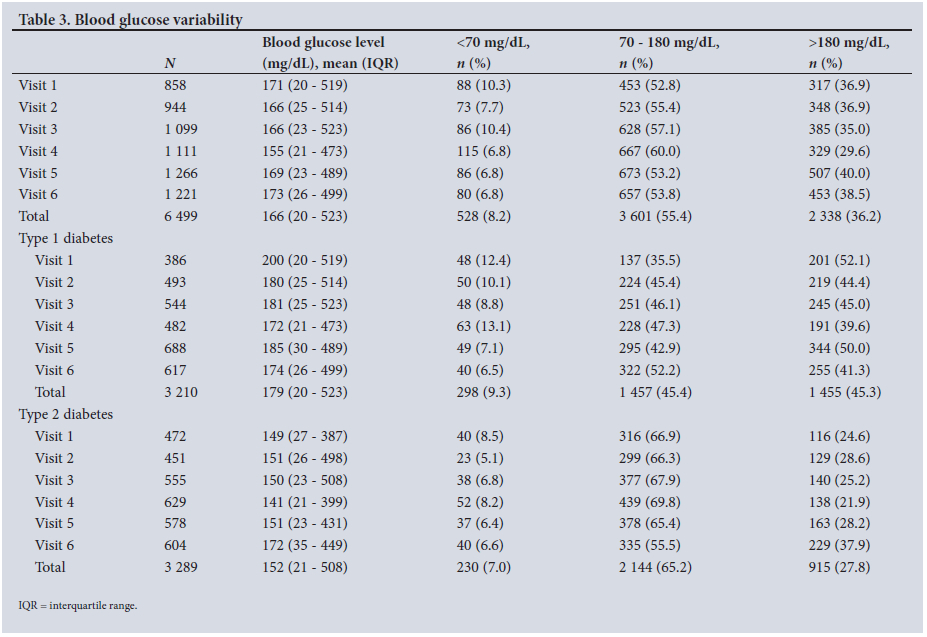
Description of any change in glucose variability from initiation to completion of the intervention was a secondary clinical outcome of interest. Glucose levels ranged from 20 mg/dL to 523 mg/dL over the 6 months of data collection (Table 3). For both type 1 and type 2 diabetes, the percentage of low values (<70 mg/dL) remained consistent, between 6.8% and 10.3%. The percentage of values >180 mg/dL increased slightly for type 2 diabetes (24.6% v. 36.9%), although it remained below the overall mean for type 1 diabetes (45.3%). The percentage of values in range (70 - 180 mg/dL) increased for type 1 diabetes from 35.5% to 52.2%, although this was not statistically significant and remained below the overall mean for type 2 diabetes (65.2%) (Table 3). There were no adverse events (hospitalisation or death) during the 6 months of data collection.
Discussion
This is the first study conducted on SMBG for type 1 diabetes in a rural, low-income setting. Our cohort study demonstrated that SMBG is feasible in a rural SSA setting. Participants enrolled in this study demonstrated a reduction of HbA1c over 6 months, and showed good adherence to SMBG, particularly as the study progressed. Overall adherence to SMBG was high, with a total of 69.4% of prescribed checks completed and 69.0% of checks accurately transcribed from glucometers to logbooks. Initially there in participants with limited literacy and numeracy. During the first months of the study, participants with primary school or no education had lower adherence than those with secondary or higher education. However, with close follow-up and re-education, adherence levels became the same in both groups. Cumulatively, these findings suggest that with sustained patient education and a patient-centred approach, all patients can benefit from SMBG technology regardless of education levels.
Previous studies conducted in SSA have used different methodologies to measure adherence. One study measured adherence to seven blood glucose checks per week and had 15.1% of participants meet this criterion,[21] and another measured adherence as >80% of blood glucose checks completed, with 34% of participants meeting the criterion.[22] We found it difficult to make direct comparisons with these studies because we collected data differently. Our analysis measured the number of prescribed checks completed (69.4%) and the number of checks accurately transcribed from glucometers to logbooks (69.4%). While comparison with published studies is difficult without an established metric or cut-off, the data suggest that our study achieved higher adherence.
Clinical impact was measured primarily by change in HbA1c, with a mean decrease of 1.2% (p<0.005) from baseline to endline. This difference was greater in participants with type 1 diabetes than in those with type 2 disease (1.6%; p<0.005), which may reflect the higher baseline HbA1c in this population and increased complexity of insulin regimens and disease management. Consistency of baseline HbA1c with clinical data from the past year implies that this change was not due to potential confounding factors such as seasonality, which can affect food security and therefore diabetes management. Charity et al.[22] found a similar mean decrease in HbA1c (1.2%; 95% CI 0.8 - 1.7) 6 months after implementation of an SMBG programme in western Kenya. The post-intervention average HbA1c level of 7.8% (62 mmol/mol), while not meeting target levels of 7.0% (53 mmol/ mol), demonstrates remarkable improvement in control compared with previous studies in the region. An assessment of youth with type 1 diabetes at a central hospital in Malawi found a mean HbA1c level of 13.2% (121 mmol/mol),[37] while a cohort of type 1 and 2 diabetes patients at PEN-Plus clinics in Rwanda had a median HbA1c of 8.6% (70 mmol/mol) 24 months after entry into care.[32]
Importantly, no severe adverse events (defined as hospitalisation or death) occurred during the study. One serious concern with lower HbA1c is increased hypoglycaemia, especially in a setting with limited monitoring capability. Prior to the initiation of this study, there were no data on the severity or frequency of hypoglycaemia in rural SSA. Over the course of the study, neither participants with type 1 nor those with type 2 diabetes had a statistically significant change in the percentage of values <70 mg/dL recorded, suggesting that increased glycaemic control and lower HbA1c were obtained without increasing the risk of hypoglycaemia in this population. However, the presence of values <50 mg/dL during all 6 months of the study remains a critical finding. Some of these values may have been due to transcription errors when transferring values from glucometers to data collection tools. Nevertheless, it is likely that some of these are true values <50 mg/dL and further support the need for increasing SMBG for patients using insulin, since some patients were probably experiencing undetected symptomatic or asymptomatic hypoglycaemia at home prior to initiation of the study. Further research using increased SMBG or continuous glucose monitoring would be valuable to assess the true extent of previously undetected hypoglycaemia in this population.
The most significant limitation to this study was the small sample size. The number of patients on insulin in the aNCD clinic limited the ability for more detailed analysis into predictors and for analysing subgroups of the population. However, despite this limitation, there was still a significant improvement in mean HbA1c in the population. Additionally, the primary outcome of assessing adherence to prescribed variables was able to be met.
The cohort design of the study was influenced by the clinical goal of providing SMBG to all patients. There was a statistically significant improvement in HbA1c before SMBG and after 6 months, but external factors could have influenced the results given the cohort design. The 6 months of data collection do not allow for conclusions on whether the observed clinical and behavioural changes can be sustained over time. Furthermore, because the glucometers were not able to upload directly to a computer for analysis, data were manually transcribed from logbook data and cross-checked with the glucometers. This process may have led to transcription errors (e.g. 20 mg/dL range instead of 200 mg/dL range).
While this study found significant clinical improvement with a model using one glucose test strip per day, best practice and previous research have shown that increasing glucose checks per day is correlated with lower HbA1c.[16,17] While cost was not an outcome of this study, it is a primary barrier to use of SMBG in SSA.[1319-23] Neno is the first district in Malawi to provide glucometers to all patients on insulin, but the cost of test strips limited testing to once per day. Although multiple glucose checks per day is the optimal treatment strategy for patients on insulin, this study shows that testing once a day is associated with blood sugar control to near-normal levels.
We therefore believe that testing blood sugar daily is a reasonable monitoring strategy until resources allow patients to have enough test strips to check blood sugar multiple times per day.
Free provision of glucometers and strips to participants for the duration of the study is likely to have influenced the higher levels of adherence seen in these results compared with previous studies in SSA. Further research would be valuable to understand the feasibility and document the cost-effectiveness of increasing the number of glucose checks per day in this setting. As continuous glucose monitors become cheaper and more widely utilised in high-income settings, comparative studies with current SMBG models evaluating cost, feasibility, and clinical impact in low-resource settings are warranted.
Our findings suggest that use of SMBG with one strip per day at rotating times is an effective strategy to improve glycaemic control for patients with insulin-dependent diabetes in low-resource, rural populations in SSA. Low literacy and numeracy should not be reasons to avoid use of SMBG, although clinics planning to implement it should take care to provide frequent follow-up, patient support and re-education. Further research would be helpful to evaluate the effect on long-term adherence and the impact and cost-effectiveness of increasing the number of glucose checks per day. This study adds to the growing body of literature and global guidelines supporting integration of SMBG as a minimum health system requirement for patients with insulin-dependent diabetes.
Conclusion
SMBG with one glucose check per day, at rotating times, is feasible in rural SSA. Despite common misconceptions, all patients, regardless of education level, can benefit from SMBG. Implementation of SMBG is associated with a decrease in the mean HbA1C level. Further research, including randomised controlled trials with larger sample sizes, is warranted to define a causal relationship between SMBG and improved clinical outcomes in this setting, and to understand long-term retention of SMBG activities, and the benefits of increasing frequency of monitoring.
Declaration. None.
Acknowledgements. None.
Author contributions. TR created the research protocol, obtained local NHSRC approval, managed the research and co-wrote the manuscript. GF organised training, analysed data and co-wrote the manuscript. FV conducted patient training, collected data and reviewed the manuscript. MB and KK were the primary clinicians for the project and reviewed the manuscript. PHP and GN helped develop the research concept and reviewed the manuscript. EN supervised the research from the MoH and reviewed the manuscript. EC provided administrative support, helped develop the research and reviewed the manuscript. GB provided administrative support, secured funding and reviewed the manuscript. AA provided research oversight and mentorship and reviewed the manuscript.
Funding. Funding for this study was provided by the Helmsley Charitable Trust (G-2105-04638).
Conflicts of interest. None.
References
1. International Diabetes Federation. IDF Diabetes Atlas. 9th ed. Brussels, Belgium: IDF, 2019. http://diabetesatlas.org/atlas/ninth-editioni (accessed 11 February 2020). [ Links ]
2. Bukhman G, Bavuma C, Gishorna C, et al Endemic diabetes in the world's poorest people. Lancet Diabetes Endocrinol 2015;3(6):402-403. https://doi.org/10.1016/S2213-8587(15)00138-2 [ Links ]
3. Bukhman G, Mocumbi A, Atun R, et al. The Lancet NCDI Poverty Commission: Bridging a gap in universal health coverage for the poorest billion. Lancet 2020;396(10256):991-1044. https://doi.org/10.1016/s0140-6736(20)31907-3 [ Links ]
4. Bavuma C, Sahabandu D, Musafiri S, Danquah I, McQuillan R, Wild S. Atypical forms of diabetes mellitus in Africans and other non-European ethnic populations in low- and middle-income countries: A systematic literature review. J Glob Health 2019;9(2):020401. https://doi.org/10.7189/jogh.09.020401 [ Links ]
5. World Bank. World Development Indicators 2014. http://hdl.handle.net/10986/18237 (accessed 11 February 2020). [ Links ]
6. Government of Malawi, National Statistical Office. 2018 Malawi Population and Housing Census report. May 2019. http://nsomalawi.mw/index.php?option=com_content&view=article&id=226:2018-malawi-population-and-housing-census&catid=8:reports&Itemid=6 (accessed 11 February 2020). [ Links ]
7. Price AJ, Crampin AC, Amberbir A, et al Prevalence of obesity, hypertension, and diabetes, and cascade of care in sub-Saharan Africa: A cross-sectional, population-based study in rural and urban Malawi. Lancet Diabetes Endocrinol 2018;6(3):208-222. https://doi.org/10.1016/S2213-8587(17)30432-1 [ Links ]
8. Ministry of Health, Malawi. Malawi National STEPwise Survey for Non-Communicable Diseases Risk Factors 2017 report (STEPS 2017). 21 January 2020. https://extranet.who.int/ncdsmicrodata/index.php/catalog/629 (accessed 11 February 2020). [ Links ]
9. Gupta N, Coates M, Bekele A, et al Availability of equipment and medications for non-communicable diseases and injuries at public first-referral level hospitals: A cross-sectional analysis of service provision assessments in eight low-income countries. BMJ Open 2020;10(10):e038842. https://doi.org/10.1136/bmjopen-2020-038842 [ Links ]
10. Atun R, Davies J, Gale E, et al Diabetes in sub-Saharan Africa: From clinical care to health policy. Lancet Diabetes Endocrinol 2017;5(8):622-667. https://doi.org/10.1016/s2213-8587(17)30181-x [ Links ]
11. Mbanya JCN, Motala A, Sobngwi E, Assah F, Enoru S. Diabetes in sub-Saharan Africa. Lancet 2010;375(9733):2254-2266. https://dolorg/10.1016/S0140-6736(10)60550-8 [ Links ]
12. Nathan DM, Genuth S, Lachin J, et al The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329(14):977-986. https://doi.org/10.1056/NEJM199309303291401 [ Links ]
13. Klatman EL, Jenkins A, Ahmedani M, Ogle G. Blood glucose meters and test strips: Global market and challenges to access in low-resource settings. Lancet Diabetes Endocrinol 2019;7(2):150-160. https://doi.org/10.1016/S2213-8587(18)30074-3 [ Links ]
14. Klatman EL, McKee M, Ogle G. Documenting and visualising progress towards universal health coverage ofinsulin and blood glucose test strips for people with diabetes. Diabetes Res Clin Pract 2019;157:107859. https://doi.org/10.1016/j.diabres.2019.107859 [ Links ]
15. Bergman M, Felig P. Self-monitoring of blood glucose levels in diabetes: Principles and practice. Arch Intern Med 1984;144(10):2029-2034. https://doi.org/10.1001/archinte.1984.04400010149024 [ Links ]
16. Miller KM, Beck R, Bergenstal R, et al. Evidence of a strong association between frequency of self-monitoring of blood glucose and hemoglobin A1c levels in T1D exchange clinic registry participants. Diabetes Care 2013;36(7):2009-2014. https://doi.org/10.2337/dc12-1770 [ Links ]
17. American Diabetes Association. Glycemic targets: Standards of medical care in diabetes - 2020. Diabetes Care 2020;43(Suppl 1):S66-S76. https://doi.org/10.2337/dc20-S006 [ Links ]
18. Czupryniak L, Barkai L, Bolgarska S, et al. Self-monitoring of blood glucose in diabetes: From evidence to clinical reality in Central and Eastern Europe - recommendations from the International Central-Eastern European Expert Group. Diabetes Technol Ther 2014;16(7):460-475. https://doi.org/10.1089/dia.2013.0302 [ Links ]
19. Abdelgadir M, Elbagir M, Eltom M, Berne C. The influence of glucose self-monitoring on glycaemic control in patients with diabetes mellitus in Sudan. Diabetes Res Clin Pract 2006;74(1):90-94. https://doiorg/10.1016/j.diabres.2006.03.003 [ Links ]
20. Mbanya JC, Aschner P, Chan JCN, Gagliardino JJ, Saji J. Self-monitoring of blood glucose (SMBG) and glycaemic control in Cameroon: Results of the International Diabetes Management Practices Study (IDMPS). Diabetes Res Clin Pract 2017;126:198-201. https://dolorg/10.1016/j.diabres.2016.11.029 [ Links ]
21. Dedefo MG, Ejeta B, Wakjira G, Mekonen G, Labata B. Self-care practices regarding diabetes among diabetic patients in West Ethiopia. BMC Res Notes 2019;12(1):212. https://doi.org/10.1186/s13104-019-4258-4 [ Links ]
22. Charity KW, Kumar AMV, Hinderaker SG, Chinnakali P, Pastakia SD, Kamano J. Do diabetes mellitus patients adhere to self-monitoring of blood glucose (SMBG) and is this associated with glycemic control; Experiences from a SMBG program in western Kenya. Diabetes Res Clin Pract 2016;112:37-43. https://doi.org/10.1016/j.diabres.2015.11.006 [ Links ]
23. Ugwu ET, Orjioke CJG, Young EE. Self monitoring of blood glucose among patients with type 2 diabetes mellitus in eastern Nigeria: Need for multi-strategic interventions. Curr Diabetes Rev 2018;14(2):175-181. https://doi.org/10.2174/1573399812666161014111618 [ Links ]
24. Phiri EC, Msiska G, Kululanga L, Mbakaya B. Patient's knowledge assessment on diabetes and self care practices among older adolescents with type 1 diabetes mellitus in Malawi. Eur Sci J 2017;13(33):429. https://doi.org/10.19044/esj.2017.v13n33p429 [ Links ]
25. Iwuala SO, Olamoyegun MA, Sabir AA, Fasanmade OA. The relationship between self-monitoring of blood glucose and glycaemic control among patients attending an urban diabetes clinic in Nigeria. Ann Afr Med 2015;14(4):182-187. https://doi.org/10.4103/1596-3519.155992 [ Links ]
26. Khowaja K, Waheed H. Self-glucose monitoring and glycaemic control at a tertiary care university hospital, Karachi, Pakistan. J Pak Med Assoc 2010;60(12):1035-1038. http://ecommons.aku.edu/pakistan_fhs_mc_med_diabet_endocrinol_metab/7 (accessed 16 January 2023). [ Links ]
27. NgAng'a L, Ngoga G, Dusabeyezu S, et al Implementation ofblood glucose self-monitoring among insulin-dependent patients with type 2 diabetes in three rural districts in Rwanda: 6 months open randomised controlled trial. BMJ Open 2020;10(7):e036202. https://doi.org/10.1136/bmjopen-2019-036202 [ Links ]
28. World Health Organization. Global action plan for the prevention and control of NCDs 2013 - 2020. 14 November 2013. https://www.who.int/publications/i/item/9789241506236 (accessed 11 February 2020). [ Links ]
29. Wroe EB, Kalanga N, Mailosi B, et al. Leveraging HIV platforms to work toward comprehensive primary care in rural Malawi: The integrated chronic care clinic. Healthc (Amst) 2015;3(4):270-276. https://doiorg/10.1016/j.hjdsi.2015.08.002 [ Links ]
30. World Health Organization Regional Office for Africa. WHO PEN and integrated outpatient care for severe, chronic NCDs at first referral hospitals in the African region (PEN-Plus): Report on regional consultation 29 July - 1 August 2020. https://www.afro.who.int/publications/who-pen-and-integrated-outpatient-care-severe-chronic-ncds-first-referral-hospitals (accessed 11 February 2020). [ Links ]
31. Bukhman G, Kidder A, The PIH guide to chronic care integration for endemic non-communicable diseases. Boston, Mass.: Partners in Health, 2011:168-195 [ Links ]
32. Tapela N, Habineza H, Anoke S, et al. Diabetes in rural Rwanda: High retention and positive outcomes after 24 months of follow-up in the setting of chronic care integration. Int J Diabetes Clin Res 2016;3(2). https://doi.org/10.23937/2377-3634/1410058 [ Links ]
33. Tapela NM, Bukhman G, Ngoga G, et al. Treatment of non-communicable disease in rural resource-constrained settings: A comprehensive, integrated, nurse-led care model at public facilities in Rwanda. Lancet Glob Health 2015;3:S36. https://doi.org/10.1016/s2214-109x(15)70155-5 [ Links ]
34. Ndayisaba A, Harerimana E, Borg R, et al. A clinical mentorship and quality improvement program to support health center nurses manage type 2 diabetes in rural Rwanda. J Diabetes Res 2017;2017:2657820. https://doi.org/10.1155/2017/2657820 [ Links ]
35. Eberly LA, Rusingiza E, Park P, et al. 10-year heart failure outcomes from nurse-driven clinics in rural sub-Saharan Africa. J Am Coll Cardiol 2019;73(8):977-980. https://doi.org/10.1016/j.jacc.2018.12.028 [ Links ]
36. Eberly LA, Rusingiza E, Park P, et al Nurse-driven echocardiography and management of heart failure at district hospitals in rural Rwanda. Circ Cardiovasc Qual Outcomes 2018;11(12):e004881. https://doi.org/10.1161/circoutcomes.118.004881 [ Links ]
37. Msekandiana A, Chigayo G, Chiume S, et al Complications and glycaemic control of type 1 diabetes mellitus amongst children aged 5 to 19 years attending diabetic clinic at Kamuzu Central Hospital in Malawi. Int J Diabetes Clin Res 2020;7(1). https://doi.org/10.23937/2377-3634/1410117 [ Links ]
 Correspondence:
Correspondence:
T Ruderman
truderman@pih.org
Accepted 4 October 2022
* Authors contributing equally
† Authors contributing equally


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}