










Services on Demand
Article
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 n.2 Pretoria Feb. 2023
http://dx.doi.org/10.7196/SAMJ.2023.v113i2.16798
IN PRACTICE
HEALTHCARE DELIVERY
What are health policy and systems research priorities for universal health coverage in South Africa?
H SchneiderI; T KredoII; W A OdendaalIII; F AbdullahIV
IMMed (Comm Health), PhD ; School of Public Health, University of the Western Cape, Cape Town, South Africa; Health Services to Systems Research Unit, South African Medical Research Council, Cape Town, South Africa
IIMMed (Clin Pharmacol), PhD; South African Cochrane Centre, South African Medical Research Council, Cape Town, South Africa
IIIBA, MA; HIV and Other Infectious Diseases Research Unit, South African Medical Research Council, Cape Town, South Africa; Department of Psychiatry, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
IVMB ChB, FCPHM; Office of AIDS and TB Research, South African Medical Research Council, Cape Town, South Africa; Division of Infectious Diseases, School of Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
ABSTRACT
We report here on the process and findings of a research prioritisation exercise for universal health coverage (UHC) in South Africa, conducted during the course of 2019. As plans to roll out National Health Insurance (NHI) gather momentum and we transition into a pandemic recovery phase, we believe that it is now time to revisit these priorities, while recognising that experiences with the COVID-19 pandemic have revealed new system challenges and strengths and introduced new priorities. The UHC research priority-setting methodology followed a stepwise process of collation of evidence, expert brainstorming and the development of a survey completed by 68 members of the Public Health Association of South Africa. Themes related to leadership and governance were ranked most highly, and with other priorities generated, provide an initial road map of knowledge needs that could guide individual institutions and commissioning by funding bodies. We further reflect on the importance of researcher-decision-maker dialogue and strengthening the contribution of health policy and systems research to policy and practice, especially as new reforms are implemented.
As South Africa (SA) transitions to a pandemic recovery phase, the core underlying health system preoccupations and priorities of the pre-COVID era are coming back into focus. Legislative and policy processes linked to National Health Insurance (NHI)[1] are gathering momentum, and a new generation of 'NHI pilots' at provincial and district level are being prepared. In the years just prior to the first COVID-19 lockdowns, several widely canvassed and comprehensive reviews of SA's health system were conducted.[1-3] Key among these were the 2018 Presidential Health Summit (resulting in a Presidential Health Compact[3]) and the Health Market Inquiry of the Competition Commission South Africa, which published its provisional and final reports in 2018 and 2019, respectively.[4
In response to these developments and the publication of the NHI Bill in 2018,[1] a group of health policy and system (HPS) researchers initiated a process of research priority setting for universal health coverage (UHC) in SA under the umbrella of the South African Medical Research Council (SAMRC). This culminated in a 2-day National Dialogue on UHC in November 2019, jointly hosted by the National Department of Health and the SAMRC and bringing together a wide range of players - academics, decision-makers and civil society -from across the country.[5] We reflect here on the methods, findings and implications of the UHC research priority-setting exercise conducted over the course of 2019, which informed the UHC Dialogue.
We believe that it is now time to revisit the priorities identified, and more broadly, the recommendations on strengthening SA's health system from these various processes, recognising that experiences with the COVID-19 pandemic have introduced new ways of thinking and new imperatives.
Process of priority setting
The priority-setting exercise adopted UHC, the governing idea on health systems in the Sustainable Development Goals, as its overall frame. UHC is the global reference point for the NHI policy, but is a concept wider than NHI, which focuses specifically on financing and resource allocation. According to the World Health Organization (WHO), the presence of UHC 'means that all individuals and communities receive the health services they need without suffering financial hardship. It includes the full spectrum of essential, quality health services, from health promotion to prevention, treatment, rehabilitation, and palliative care across the life course.'[6]
The priority-setting process began with a 1-day workshop in early 2019, attended by 25 HPS researchers from the SAMRC and academic institutions across the country. Participants were presented with summaries of the 2018 Presidential Health Summit[3] and the (then provisional) Health Market Inquiry reports,[4] organised into a conceptual framework (Fig. 1). This framework broadly followed the WHO health system 'building blocks' approach,[7] with additional cross-cutting functions (implementation, learning health system). Taking these as their starting inputs, workshop participants broke into groups to generate priority research themes on each of eight health system domains (the vertical blue bars in Fig. 1). Using a structured brainstorming methodology (nominal group techniques), they identified and ranked a set of priority health policy and systems research (HPSR) themes for each domain.
On the basis of a detailed workshop report, the co-authors then developed an anonymous online survey, tested internally in the SAMRC and then posted on the listserv of the Public Health Association of South Africa HPSR Special Interest Group (PHASA HPSR-SIG). PHASA HPSR-SIG is a network of practitioners, decision-makers, researchers, students and academics from a variety of backgrounds - governmental, non-governmental, civil society and research - in SA. During the course of September and October 2019, a total of 68 SIG members completed the survey. The domains in the survey were further discussed in an organised session of the annual PHASA conference held during this period.
The survey asked respondents to first rank eight health system domains (governance and leadership, human resources for health, financing, information systems, service delivery, infrastructure, equipment and supply chains) in order of importance, and then to select which domains they wished to rank further. For each individual domain, respondents were asked to rank six listed priorities from 1 (most important) to 6 (least important). Respondents were permitted to skip domains for which they did not feel able to judge priorities, which explains the variable response rate by domain. Ample space was provided for comments on the domains and priorities.
The 68 respondents came from six provinces, but were mostly (96%) from Gauteng, Western Cape and KwaZulu-Natal (Fig. 2). They included researchers (based in a mix of higher-education institutions, government and civil society organisations), with policy-makers and managers contributing nearly a third of responses (n=20; 29%).
Scores were assigned to ranks (the item ranked first in each domain was assigned a score of 6, the item ranked second a score of 5, and so on, down to a score of 1 for the last-ranked item), and totals were calculated for each domain and theme within the domain. Qualitative responses to open-ended questions and notes from the PHASA-organised session were also grouped thematically.
Priorities identified
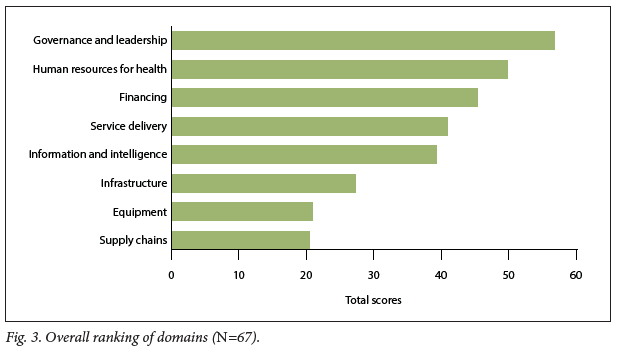
Fig. 3 presents the participants' overall ranking of the eight health system domains. Knowledge generation on health system governance and leadership was ranked highest, followed by human resources for health, financing, and then service delivery.
Table 1 summarises the ranking of priority themes within the domains. Highly ranked themes were leadership/management capacity, accountability (performance, financial and public/patient), use of information, quality improvement, and learning health systems. 'Hardware' aspects of health systems such as information infrastructure, regulation and technology, although featuring as priorities, were generally ranked below the knowledge needs on the relational, 'software' dimensions.
These emphases were also reflected in the additional comments of respondents, who pointed out the need for research on:
-
Issues of implementation (the how) that transcend building blocks, e.g. operational and change management, the role of complexity science in shaping implementation and 'scale-up', and bottom-up implementation strategies
-
The NHI policy process itself, including processes of agenda setting, stakeholder interests and political factors
-
Health system organisational culture, relationships and social dynamics, collaborative action and trust
-
Values of equity and access, while paying attention to efficiency and affordability Positioning quality and quality improvement and learning health systems as a cross-cutting theme rather than just being linked to one domain
-
Foregrounding action on the social determinants of health and multisectoral collaboration, seen as missing from the NHI policy debates.
It is important to note that these themes remained at a general level, i.e. they are not specific research questions, and many could simultaneously be considered priorities for research and policy/practice.
Implications
The findings of the research prioritisation exercise should not be regarded as scientifically valid or representative in a conventional sense. Nevertheless, the frameworks developed and HPSR themes generated provide an initial road map of knowledge needs that could guide the priorities of individual institutions and commissioning by funding bodies. Research prioritisation is especially important as new reform initiatives such as NHI are implemented.
The consultative process of priority setting was also an opportunity for raising awareness on the need for HPSR capacity to advance UHC in SA. There is a considerable body of research on SA's health system, developed over the decades since the political transition in this country. However, this knowledge base is fragmented or forgotten. Systematic programmes of evidence synthesis could play an important role in harnessing accumulated knowledge and making it available in accessible formats and repositories. Synthesised and accessible information could provide immediate actionable intelligence for policy and practice, while identifying gaps in knowledge that are translatable into specific research questions.
As pointed out in the 2013 World Health Report[8] on research for UHC, there is a need to pay attention to both the content of research and the way it is conducted. Approaches such as co-production, embedded research and multidisciplinary approaches are key to nurturing a learning culture in the health system. The National Dialogue on UHC convened by the SAMRC in November 2019 provided a significant initial platform for exchange between policymakers, researchers and practitioners. There was overwhelming agreement on the need for more such opportunities, extending to provincial and local levels, and the momentum lost during the COVID-19 pandemic needs to be regained.
Finally, research prioritisation is not a once-off event. The COVID-19 pandemic and recent environmental disasters (such as droughts and floods) have foregrounded new priorities and a growing orientation towards whole-of-society approaches. Formally mandated bodies such as the National Health Research Committee provide the vehicle for updating priorities.[9] Our methodology has shown that when approached in a systematic fashion, achieving consensus on HPSR priorities for UHC in SA is feasible, and provides meaningful evidence-based contributions to health reform choices being contemplated by public and private sector decision-makers.
Declaration. None.
Acknowledgements. We gratefully acknowledge the 25 HPSR researchers who attended the initial workshop to generate priorities, and the PHASA HPSR-SIG members who participated in the organised session and responded to the survey.
Author contributions. The authors collectively steered the priority-setting process. HS drafted the manuscript, which was commented on and approved by all authors.
Funding. HS holds a Department of Science and Innovation/National Research Foundation South African Research Chair in Health Systems Governance. TK is partly funded by the Research, Evidence and Development Initiative (READ-It) (project no. 3003420104). READ-It is funded by UK aid from the UK government; however, the views expressed do not necessarily reflect the UK government's official policies.
Conflicts of interest. None.
References
1. National Department of Health, South Africa. National Health Insurance Bill, 2018. Government Gazette No. 41725:635, 21 June 2018. https://www.gov.za/sites/default/files/gcis_document/201806/41725gon635s.pdf (accessed 26 August 2022). [ Links ]
2. South African Lancet National Commission. Confronting the right to ethical and accountable quality health care in South Africa: A consensus report. Pretoria: National Department of Health, 2019. https://bhekisisa.org/wp-content/uploads/2019/07/620a9eb9-final-sa-lnc-report.pdf (accessed 26 August 2022). [ Links ]
3. The Presidency. Presidential Health Summit 2018: Strengthening the health system towards an integrated and unified health system. 19 - 20 October 2018. https://www.gov.za/sites/default/files/gcis_document/201902/presidential-health-summit-report.pdf (accessed 26 August 2022). [ Links ]
4. Competition Commission South Africa. Healthcare Market Inquiry: Final findings and recommendations report. September 2019. https://www.compcom.co.za/healthcare-inquiry/ (accessed 26 August 2022). [ Links ]
5. South African Medical Research Council. Universal health coverage: National dialogue: Harnessing knowledge for the design and implementation of universal health coverage, November 2019. Cape Town: SAMRC, 2020. http://uhcs.samrc.ac.za/UHCReport.pdf (accessed 26 August 2022). [ Links ]
6. World Health Organization. Universal health coverage (UHC). https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc) (accessed 26 August 2022). [ Links ]
7. World Health Organization. Everybody's business: Strengthening health systems to improve health outcomes: WHO's framework for action. Geneva: WHO, 2007. https://apps.who.int/iris/handle/10665/43918 (accessed 26 August 2022). [ Links ]
8. World Health Organization. The World Health Report 2013: Research for universal health coverage. Geneva: WHO, 2013. https://www.who.int/publications/i/item/9789240690837 (accessed 28 December 2022). [ Links ]
9. National Department of Health, South Africa. National Health Research Strategy: Research priorities for South Africa, 2021 - 2024. https://health.gov.za/wp-content/uploads/2021/04/NATIONAL-HEALTH-RESEARCH-STRATEGY-2021-2024.pdf (accessed 26 August 2022). [ Links ]
 Correspondence:
Correspondence:
H Schneider
hschneider@uwc.ac.za
Accepted 27 September 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}