










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.113 n.1 Pretoria Jan. 2023
http://dx.doi.org/10.7196/SAMJ.2022.v113i1.16619
IN PRACTICE
Recovering from COVID lockdowns: Routine public sector PHC services in South Africa, 2019 - 2021
Y PillayI; H MuseririII; P BarronIII; T ZondiIV
IPhD; Division of Public Health and Health Systems, Department of Global Health, Facuty of Health Sciences, Stellenbosch University, Cape Town, South Africa
IIMPhil; Clinton Health Access Initiative, Pretoria, South Africa
IIIMB ChB; School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVMPH National Department of Health, Pretoria, South Africa
ABSTRACT
BACKGROUND. In a previous article on the impact of COVID-19, the authors compared access to routine health services between 2019 and 2020. While differential by province, a number of services provided, as reflected in the District Health Information System (DHIS), were significantly affected by the pandemic. In this article we explore the extent to which the third and fourth waves affected routine services.
OBJECTIVES. To assess the extent to which waves 3 and 4 of the COVID-19 pandemic affected routine health services in South Africa, and whether there was any recovery in 2021.
METHODS. Data routinely collected via the DHIS in 2019, 2020 and 2021 were analysed to assess the impact of the COVID-19 pandemic and extent of recovery.
RESULTS. While there was recovery in some indicators, such as number of children immunised and HIV tests, in many other areas, including primary healthcare visits, the 2019 numbers have yet to be reached - suggesting a slow recovery and continuing impact of the pandemic.
CONCLUSIONS. The COVID-19 pandemic continued to affect routine health services in 2021 in a number of areas. There are signs of recovery to 2019 levels in some of the health indicators. However, the impact indicators of maternal and neonatal mortality continued to worsen in 2021, and if interventions are not urgently implemented, the country is unlikely to meet the Sustainable Development Goals targets.
A 2021 publication[1] reflected the extent to which the COVID-19 pandemic affected routine primary healthcare services (PHC) in South Africa (SA) between 2019 and 2020. These routine services include healthcare for maternal and child health, women's health, including contraceptive care, management of common communicable diseases such as HIV and tuberculosis (TB) and management of chronic conditions such as hypertension, diabetes and mental health. The article compared a selected number of health indicators, e.g. immunisation coverage, antenatal early booking rates, maternal and neonatal deaths and mortality rates and HIV and TB testing rates using the District Health Information System (DHIS) between March and December 2019, relative to the same period in 2020. This 2021 article found that COVID-19 negatively impacted the number of people who visited health facilities, the number of children immunised, the number of women who received contraceptives and the number of people who were tested for HIV and TB. In addition, it found that maternal and neonatal mortality increased during the first year of COVID-19.
These findings were similar to those found in most other countries, including developed countries such as Germany, where there was a significant drop in cancer diagnoses[12] as well as in developing countries. In a review of over 500 facilities in 32 developing countries, a report from the Global Fund found that 'antenatal first care visits fell by 66% in facilities surveyed in seven countries across Asia, while consultations for under-5 services decreased by 74%'.[3] In its third pulse survey at the end of 2021,[4] the World Health Organization (WHO) found that 2 years into the COVID-19 pandemic, 90% of countries reported continued disruptions to routine health services, with little improvement relative to the pre-COVID period.
Disruptions were found in immunisation coverage, maternal and child health services, sexual and reproductive health services as well as HIV and TB services. In addition, 43% of countries reported that financial challenges that resulted from the impact of the pandemic also impacted negatively on their ability to provide services.'[5]
Low- and middle-income countries were expected to struggle to cope with the pandemic as a result of low levels of investment in health systems. However, the pandemic has shown that all health systems struggled to cope with the pandemic - even countries such as England struggled to cope with the scale of the pandemic, and elective services were scaled down, resulting in an increase of 38% (>6 million patients) now waiting for treatment.[6]
From March 2020 to December 2021, there were four COVID-19waves in SA. While the numbers of COVID-19 cases in the third and fourth waves in 2021 were as high as the second wave in 2020, hospitalisations and deaths in the third and fourth waves were much lower.
In this article we explore whether the pandemic continued to negatively affect the indicators from the 2021 article, and the extent to which there was recovery to pre-pandemic levels by December 2021.
Methods
The DHIS is the repository of routine data from the public sector, which caters for ~85% of the total population.[7] In addition, aggregate TB testing data (polymerase chain reaction results, performed under the tradename GeneXpert) were provided by the National Health Laboratory Service (NHLS). We analysed routine data for selected indicators for the period March 2019 to December 2021. The rationale for using data from March to December of each year is:
(i) to align with when the first cases of COVID-19 were detected on 5 March 2020; and (ii) to ensure that we compare the same time periods in 2020 and 2021, to avoid any bias. Data were analysed per province as well as nationally.
The indicators measured were chosen as proxy indicators of access to PHC. The indicators actually measure utilisation of health services. Utilisation is itself a proxy for access to health services, which incorporates a number of elements including affordability, availability, accessibility, acceptability and accommodation of user's preferences.'8-
The indicators were:
• total number of PHC visits
• access to contraceptives
• access to antenatal care
• number of deliveries in public health facilities
• in-facility maternal, neonatal and children <5 years mortality
• immunisation coverage
• number of HIV tests
• number of TB screenings
• number of GeneXpert tests done, and number positive.
Results
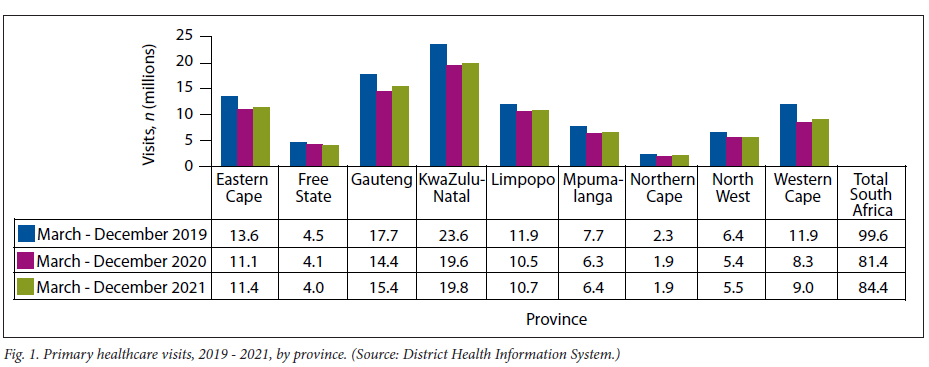
Number of PHC visits
Fig. 1 reflects the number of visits to PHC facilities between March 2019 and December 2021. Nationally, in 2019 there were 99.6 million visits. This declined to 81.4 million in 2020 (18.3% decline), with a slight rebound to 84.1 million in 2021. After big declines in 2020, there was some recovery in the provinces in 2021, but none recovered to their 2019 levels. The Free State was the only province with a further decline in number of PHC visits between 2020 and 2021.
Access to contraceptives
Nationally, the number of contraceptive years protected in 2021 were lower than those in 2019 by 4.1% (7.3 million in 2019 compared with 7 million in 2021; Fig. 2). Three provinces (Free State, Gauteng and KwaZulu-Natal) recovered to 2019 levels. Interestingly, two provinces (Eastern Cape and Northern Cape) had more contraceptive years protected in 2020 than 2021.
Number of antenatal visits
Nationally, the number of first antenatal visits increased by 3.2% between 2019 and 2020, and declined by 3.7% between 2020 and 2021 (Fig. 3). Between 2019 and 2021, antenatal visits declined by 0.6%. KwaZulu-Natal, Mpumalanga, Northern Cape and North West provinces recorded more antenatal visits in 2021 than 2019.
Public health facility births, 2019 - 2021
Fig. 4 reflects that nationally, the number of births in public facilities increased by 3.8% between 2019 and 2020, but declined by 1% between 2020 and 2021. Between 2019 and 2021, births increased on average by 2.8%. The only province with fewer births in 2021 than 2019 was the Western Cape.
Institutional maternal deaths, 2019 - 2021
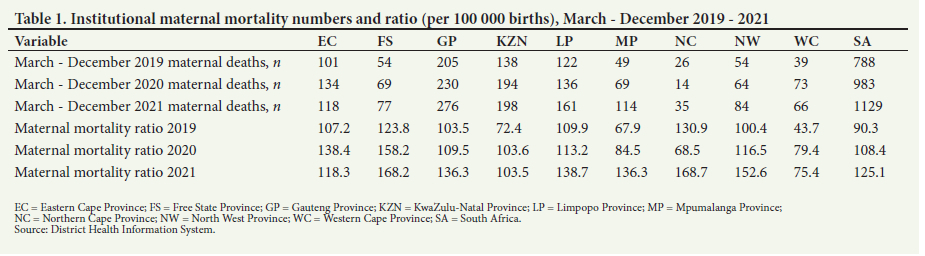
Between March and December 2019, there were 788 maternal deaths recorded in public facilities. This number increased to 983 during the same period in 2020, and increased further to 1 129 in 2021. This represents a 43.3% increase in maternal deaths between 2019 and 2021. All provinces reported increases in maternal deaths in 2021 compared with 2019. As reflected in Table 1, the institutional maternal mortality ratio increased from 90.3/100 000 live births in 2019 to 125.1 in 2021.
Institutional neonatal deaths
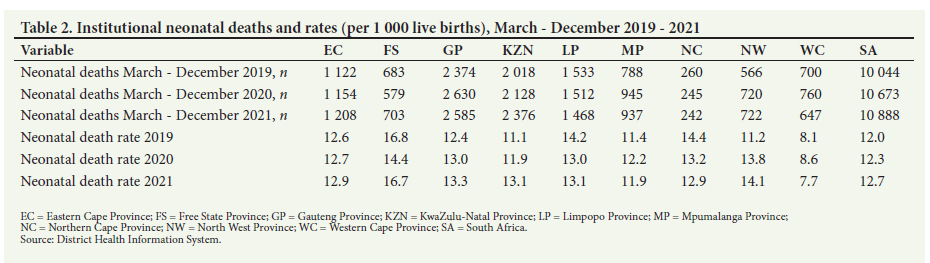
In 2019, 10 044 institutional neonatal deaths were recorded in the DHIS. This increased by 6.3% in 2020 and by a further 2% between 2020 and 2021, when 10 888 deaths were reported. Three provinces, Limpopo, Northern Cape and Western Cape, reported fewer neonatal deaths in 2021 than 2019, with the remaining six all showing increases. The neonatal mortality rate (Table 2) similarly increased from 12 per 1 000 births in 2019 to 12.7 per 1 000 in 2021.
Number of children fully immunised
In 2019, 800 242 children were fully immunised at 12 months (Fig. 5). The number of children fully immunised declined by 4.3% in 2020. There was a rebound in 2021, with more children immunised than in 2019. However, in the Eastern Cape, Limpopo, Northern Cape and North West provinces, fewer children were fully immunised in 2021 compared with 2019. After taking into account the 15% of the population who are on medical aid, the immunisation coverage rates for 2019 - 2021 are shown in Table 3. Most provinces showed a decrease in 2020, with a rebound in 2021. There are striking differences between North West and Limpopo provinces (~60%) and urban Gauteng (well above 90%).
Child under 5 in-facility deaths
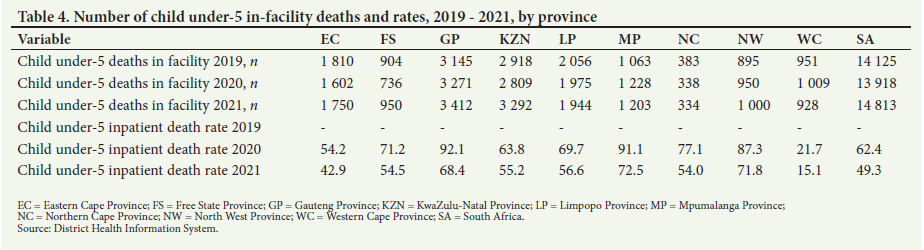
Fewer children <5 years old died in public health facilities in 2020 compared with 2019 (14 125 in March - December 2019, compared with 13 918 during the same period in 2020). However, the figure increased to 14 813 in 2021. The Free State, Gauteng, KwaZulu-Natal, Mpumalanga and North West had more deaths of children <5 years in 2021 than 2019. The under-5 in-facility death rates (per 1 000 children) for 2020 and 2021 are shown in Table 4. Clearly there were significant decreases in this rate across all provinces. Unfortunately, denominator data were not available for 2019 in order to calculate these death rates.
Number of HIV rapid tests done
Nationally, >15.4 million HIV tests were done between March and December 2019. This decreased to 12 million in 2020 (22% decline). The number of HIV tests done in 2021 increased to >14.8million (Fig. 6). While there is some recovery, the 2021 figure is still 4.3% lower than in 2019. Two provinces, Gauteng and North West, reported more tests done in 2021 than in 2019. Denominator data were not available to calculate rates.
TB screening and tests
The number of TB GeneXpert tests conducted by the NHLS decreased from 2.1 million in 2019 to 1.60 million in 2020 (22.7% decline). There was an increase in GeneXpert testing reported by the NHLS in 2021 to 2.0 million; however, this is still a decrease of 5.9% relative to 2019. The number of positive tests showed a similar picture, as shown in Table 5. This equates to high positivity rates of 10.0%, 9.7% and 8.9%.
Discussion
This study sought to show whether access to routine health services during the third and fourth COVID-19 waves, compared with the first and second waves, showed a rebound relative to the year preceding the start of the COVID-19 pandemic, namely March -December 2019. The number of PHC visits increased by 3.4% (from 84.1 million visits in 2021 compared with the 81.4 million visits in 2020). While this increase suggests a marginal recovery in 2021, none of the nine provinces reached the number of visits that they reported in the year before the pandemic. This suggests that some of the factors that mitigate against the use of the public sector (e.g. lack of transport availability, fear of contracting COVID-19) were in place in 2021. It is suggested that provinces should have a communication strategy encouraging people who rely on the public health sector that facilities are open for business, that it is safe to visit PHC facilities and that they should not delay seeking care.
Across the various health programmes, some provinces recovered to levels of access reported pre COVID-19. Four provinces increased the contraceptive years protected to pre-COVID-19 levels. However, in three provinces, the number of contraceptive years protected in 2021 was lower than in 2020. It is critical that all provinces increase access to contraceptives, especially to adolescents. A recently published article[9] reported an increase in pregnancies and deliveries in 10 -19-year-olds, with a 48% increase in 10 - 14 and a 17% increase in 15 -19-year-olds between 2017 and 2021. In addition, there have been numerous reports of stock-outs of contraceptive medicines at facility level, with a range of pragmatic recommendations for provinces to focus on improving basic PHC services.[10,11]
The provision of good-quality antenatal care is critical for good maternal and neonatal outcomes beyond survival, meaning that its impact extends to thriving as well.[12] KwaZulu-Natal and Mpumalanga provinces have been able to reach antenatal visits in 2021 comparable with those in 2019. It is noteworthy that six provinces have lower numbers of antenatal visits in 2021 than 2020. Provinces with these lower numbers of visits need to explore the reasons for the decreases. All provinces except the Western Cape reported more in-facility births in 2021 than 2019.
In-facility maternal mortality was in decline in SA up to 2019, when the lowest number of maternal deaths was recorded, at 788. It is of great concern that over the last 2 years, the number of in-facility maternal deaths increased 43.3%, and the maternal mortality ratio showed a similar increase of 38.5%. The lowest increase in the number of maternal deaths between 2019 and 2021 was in the Eastern Cape (16.8%), and the highest was in Mpumalanga (132.7%). These increases are reflected in the national maternal mortality ratio increasing from 90.3/100 000 live births in 2019 to 125.1/100 000 in 2021. These data reflect other recently published data,[13] noting that the small differences between these data and data reported in this article are related to the former using calendar-year data, whereas this article uses data from March to December in each year. There is evidence that decreased access to public health facilities, as well as the direct impact of COVID-19 on pregnant women, contributed to the increase in maternal mortality over the past 2 years.[13] Every effort must be made to reverse this increasing trend if the country is to reach the Sustainable Development Goal (SDG) target of no more than 70 maternal deaths per 100 000 deliveries.
Maternal complications, including maternal deaths, are also associated with poor perinatal outcomes, including neonatal death.[14] It is therefore not surprising that neonatal deaths during the past 2 years increased in tandem with maternal mortality. Deaths in both mothers and their neonates are also related to inadequate antenatal care. There was an 8.3% increase in in-facility neonatal deaths between 2019 and 2021. The highest increase in neonatal mortality between 2019 and 2021 was in North West Province (27.6%) followed by Mpumalanga (18.9%), with the Western Cape recording the largest decline (7.6%). The national in-facility neonatal mortality rate increased from 12/1 000 deliveries in 2019 to 12.7% in 2021. The SDG target is 12/1 000 and this increasing rate in the past 2 years needs to be rapidly reversed if SA is to meet the SDG target. Previous reviews of neonatal mortality in SA have made recommendations such as improved quality of care (helping babies breathe), adequate training of staff and engaged provincial leadership with adequate monitoring and oversight, as well as better use of community health workers (CHWs).[15] These recommendations are as pertinent, if not more so, following COVID-19.
Nationally, the number of children fully immunised increased marginally between 2019 and 2021. However, it is of concern that four provinces immunised fewer children in 2021 than 2019. This situation is significantly worse in rural areas, such as in Limpopo and North West provinces. Possibilities exist for better use of CHWs, who have been shown to improve immunisation coverage.[16] Missed opportunities for vaccination (MOV) were a concern pre-COVID-19.'17] The 2016 SA Demographic Survey found 42% MOV.[18] Clearly, the COVID-19 pandemic has made this situation worse.
To reduce under-5 mortality, every effort needs to be made to ensure that every child is fully immunised. There was a 4.9% increase of under-5 deaths in 2021 relative to 2019. The largest percentage increase in in-facility child mortality between 2019 and 2021 was in Mpumalanga (13.2%), followed by KwaZulu-Natal (12.8%) and North West (11.7%). The main causes of child deaths in SA are diarrhoea and pneumonia. DHIS data suggest that deaths in children under 5 from diarrhoea declined by 17.4% between 2019 and 2021. Similarly, deaths due to pneumonia declined by 12.6% during the same period. It has been suggested that the reduction in deaths from diarrhoea and pneumonia can be attributed to the hand hygiene and physical distancing measures imposed by government. [19]
While the number of HIV tests done in 2021 has increased relative to 2020, it is still lower than the number of tests done in 2019. Testing people for HIV is critical, not only to know one's status but to initiate those who test positive on antiretrovirals, to protect the health of the individual as well as to prevent the spread of HIV. While two provinces (Gauteng and North West) increased the number of people tested for HIV in 2021 relative to 2019, the other seven provinces did not, including the province with the largest HIV burden, KwaZulu-Natal. Similarly, the number of TB screenings in 2021 did not reach 2019 levels in any of the nine provinces. While the Western Cape comes closest (0.4% decline) in the number of screenings in 2021 compared with 2019, the Free State (26.6% decline), KwaZulu-Natal (12.3%), North West (12.1%), Eastern Cape (11.1%) and Mpumalanga (9.8%) were the worst performers. Data from the NHLS shows that the number of GeneXpert tests done increased in 2021 relative to 2020 and has reached within 5.9% of the number of tests done in 2019. While this is positive, there is a larger problem that predates the COVID-19 pandemic, as according to the TB coverage survey, an estimated 150 000 people with TB are not diagnosed or on treatment annually.[20]
The WHO's South East Asia region adopted a series of recommendations for countries to implement to secure essential health services.[21]- These recommendations apply equally to SA, and include: (i) increasing investment to strengthen PHC services to address health emergencies and to achieve universal health coverage; (ii) strengthening availability of essential medicines, human resources for health and infrastructure to ensure delivery of essential health services, including during emergencies; and (iii) strengthening partnerships, including the private sector, to increase the capacity of the system to respond to emergencies and to ensure that services are delivered to everyone. A framework including 10 recommendations similar to the above was also made by Geerts et al.,[22] and included the crucial issue of providing regular communication to build trust in society. This is important given the increasing lack of trust in a government that is responsible for providing more than 85% of people in the country with health services.
Study limitations
A limitation of this article is the use of the DHIS and NHLS as the data sources. These sources only record information from the public sector - hence this analysis has no data from the private health sector. In addition, the data are descriptive, and no specific attributions are possible. It should also be noted that the DHIS data are updated by provinces periodically, and small changes between different times when data are drawn are typical. We were not able to obtain data on some relevant denominators, which inhibited our ability to calculate more comparable rates than absolute numbers. Finally, as in Pillay et al.,[1] data on non-communicable diseases (NCDs) were omitted because of the poor and unreliable quality of the routinely collected NCD data.
Conclusions
This article builds on the 2021 article by Pillay et al.,[1] and explores the extent to which there was recovery to pre-COVID levels in selected health indicators. There has been some recovery on some indicators and in some provinces. Of concern is that PHC visits have not returned to pre-COVID levels. Unless communities dependent on the public health sector feel safe enough to seek care, none of the indicators analysed are likely to improve. Everything possible needs to be done to build the population's confidence in the public health system.
Declaration. None.
Acknowledgements. None.
Author contributions. YP conceptualised and wrote the first draft. HM and TZ provided the data, and all authors redrafted and edited the article.
Funding. None.
Conflicts of interest. None.
References
1. Pillay Y, Pienaar S, Barron P, Zondi T. Impact of COVID-19 on routine primary healthcare services in South Africa. S Afr Med J 2021;111(8):714-719. https://doi.org/10.7196/SAMJ.2021.v111i8.1578 [ Links ]
2. Jacob L, Kalder M, Kostev K. Decrease in the number of patients diagnosed with cancer during the COVID-19 pandemic in Germany. J Cancer Res Clin Oncol 2022;148:3117-3123. https://doi.org/10.1007/s00432-022-03922-5 [ Links ]
3. The Global Fund. The impact of COVID-19 on HIV, TB and malaria services and systems for health, April 2021. Geneva: TGF, 2021. https://www.theglobalfund.org/media/10776/covid-19_2020-disruption-impact_report_en.pdf (accessed 22 April 2022). [ Links ]
4. World Health Organization. Essential health services face continued disruption during COVID-19 pandemic. Geneva: WHO, 7 February 2022. https://www.who.int/news/item/07-02-2022-essential-health-services-face-continued-disruption-during-covid-19-pandemic (accessed 23 April 2022). [ Links ]
5. United Nations Children's Fund. COVID-19 continues to disrupt essential health services in 90 per cent of countries. New York: UNICEF, 2021. https://www.unicef.org/press-releases/covid-19-continues-disrupt-essential-health-services-90-cent-countries (accessed 23 April 2022). [ Links ]
6. Nuffield Trust. Health system recovery from COVID-19: International lessons for the NHS. Epsom: Nuffield Trust, 2022. https://www.nuffieldtrust.org.uk/research/health-system-recovery-from-covid-19-international-lessons-for-the-nhs (accessed 24 April 2022). [ Links ]
7. Coovadia H, Jewkes R, Barron P, Sanders D, McIntyre D. The health and health system of South Africa: Historical roots of current public health challenges. Lancet 2009:374(9692):817-834. https://doi.org/10.1016/S0140-6736(09)60951-X [ Links ]
8. McLaughlin C, Wyszewianski L. Access to care: Remembering old lessons. Health Services Res 2002;37(6):1441-1443. https://doi.org/10.1111%2F1475-6773.12171 [ Links ]
9. Barron P, Subedar H, Letsoko M, Makua M, Pillay Y. Teenage births and pregnancies in South Africa, 2017 - 2021 - a reflection of a troubled country: Analysis of public sector data. S Afr Med J 2022;112(4):252-258. https://doi.org/10.7196/SAMJ.2022.v112i4.16327 [ Links ]
10. Ritshidze. Eastern Cape: State of health. Ritshidze, September 2021. https://ritshidze.org.za/eastern-cape-state-of-health/ (accessed 22 April 2022). [ Links ]
11. Ritshidze. Free State: State of health. Ritshidze, September 2021. https://ritshidze.org.za/wp-content/uploads/2021/09/Ritshidze-State-of-Health-Free-State-2021.pdf (accessed 23 April 2022). [ Links ]
12. Tunçalp Ö, Pena-Rosas JP, Lawrie T, et al. WHO recommendations on antenatal care for a positive pregnancy experience-going beyond survival. BJOG 201;124(6):860-862. https://doi.org/10.1111/1471-0528.14599 [ Links ]
13. Vogel JP, Souza IP, Mori R, et al. Maternal complications and perinatal mortality: Findings of the World Health Organization Multicountry Survey on Maternal and Newborn Health. BJOG 2014;121(1):76-88. https://doi.org/10.1111/1471-0528.12633 [ Links ]
14. Pattinson R, Fawcus S, Bebhardt S, Soma-Pillay P, Niit R, Moodley J. The impact of COVID-19 on use of maternal and reproductive health services and maternal and perinatal mortality. In: Govender K, George G, Padarath A, Moeti T (editors). South African Health Review, 2021: Health Sector Responses to COVID-19. Durban: Health Systems Trust, 2021. [ Links ]
15. Rhoda N, Velaphi S, Gebhardt G, Kauchali S, Barron P. Reducing neonatal deaths in South Africa: Progress and challenges. S Afr Med J 2018;108(Suppl 1):S9-S16. https://doi.org/10.7196/SAMJ.2018.v108i3.12804 [ Links ]
16. Nzioki JM, Ouma J, Ombaka JH, Onyango RO. Community health worker interventions are key to optimal infant immunisation coverage, evidence from a pretest-posttest experiment in Mwingi, Kenya. Pan Afr Med J 2017;28:21. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5680999/ (accessed 23 April 2022). [ Links ]
17. Nnaji CA, Wiysonge CS, Lesosky M, Mahomed H, Ndwandwe D. COVID-19 and the gaping wounds of South Africa's suboptimal immunisation coverage: An implementation research imperative for assessing and addressing missed opportunities for vaccination. Vaccines 2021;9(7):691. https://doi.org/10.3390/vaccines9070691 [ Links ]
18. Shung-King M, Lake L, Hendricks M, et al. The impact of COVID-19 on children: Insights from the Western Cape experience. In: Govender K, George G, Padarath A, Moeti T (editors). South African Health Review, 2021: Health sector responses to COVID-19. Durban: Health Systems Trust, 2021. [ Links ]
19. Bradshaw D, Dorrington RE, Laubsher R, Moultrie TA, Groenewald P. Tracking mortality in near to real time provides essential information about the impact of the COVID-19 pandemic in South Africa in 2020. S Afr Med J 2021;111(8):732-740. https://doi.org/10.7196/SAMJ.2021.v111i8.15809 [ Links ]
20. Pillay Y, Mvusi L, Mametja, L, Dlamini S. What did we learn from South Africa's first-ever tuberculosis prevalence survey? S Afr Med J 2021;111(5):402-404. https://doi.org/10.7196/SAMJ.2021.v111i5.15662 [ Links ]
21. Regional Office for South-East Asia. COVID-19 and measures to 'build back better' essential health services to achieve UHC and the health-related SDGs. Geneva: WHO, 2021. https://apps.who.int/iris/bitstream/handle/10665/343752/sea-rc74-3-eng.pdf?sequence=1&isAllowed=y (accessed 24 April 2022). [ Links ]
22. Geerts JM, Kinnair D, Taheri P, et al. Guidance for health care leaders during the recovery stage of the COVID-19 pandemic: A consensus statement. JAMA Netw Open 2021;4(7):e2120295. https://doi.org/10.1001/jamanetworkopen.2021.20295 [ Links ]
 Correspondence:
Correspondence:
Y Pillay
ygpillay@gmail.com
Accepted 12 September 2022.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}