










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.12 Pretoria Dez. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i12.16410
RESEARCH
Risk factors and outcomes of sepsis-associated acute kidney injury in intensive care units in Johannesburg, South Africa
M D MweeneI; G A RichardsII; G PagetI; J BandaIII; C DickensIV
IMB ChB, MMed (Int Med); Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMMed (Int Med), PhD; Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIMMed (Int Med), PhD; Department of Medical Sciences, Faculty of Health Sciences, University of Namibia, Windhoek, Namibia
IVMSc, PhD; Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Sepsis-associated acute kidney injury (SA-AKI) has been shown to be a significant contributor to morbidity and mortality in both children and adults with critical illness. In sub-Saharan Africa, there is a lack of information on factors associated with development of SA-AKI and outcomes after intensive care unit (ICU) admission
OBJECTIVES: To assess the rate of SA-AKI, factors associated with its development, and predictors of mortality at 90 days in critically ill patients admitted to the ICU with sepsis
METHODS: This was a prospective observational study conducted at two of the biggest teaching hospitals in Johannesburg, South Africa, from 15 February 2016 to 15 February 2020. The study included consecutive patients with confirmed sepsis who were admitted to the ICU within 24 hours of admission to hospital. The primary outcome of the study was development of SA-AKI (defined according to Kidney Disease Improving Global Outcome (KDIGO) criteria), and secondary outcomes were risk factors for SA-AKI and predictors of mortality at 90 days. Multivariate logistic regression analysis was employed to determine the factors associated with SA-AKI and 90-day mortality
RESULTS: In total, 327 critically ill patients with sepsis admitted to the ICUs were included in the study. The median (interquartile range) age was 39 (30 - 52) years, and 185 patients (56.6%) developed SA-AKI. Of these patients, blacks and whites comprised 91.0% and 6.1%, respectively, and the prevalent comorbidities were HIV/AIDS (19.3%), hypertension (14.2%) and diabetes mellitus (10.1%). Patients with SA-AKI were likely to be older and of male gender, and to have cardiovascular disease, malignancies, hypotension and a low serum albumin level. In multivariate analysis, the predictors of SA-AKI were age >55 years (odds ratio (OR) 2.43; 95% confidence interval (CI) 1.27 - 4.65), inotropic support (OR 3.61; 95% CI 2.18 - 5.96) and a low serum albumin level (OR 2.93; 95% CI 1.40 - 6.13). SA-AKI and need for inotropic support were respectively associated with 1.9-fold and 1.7-fold increased mortality at 90 days after ICU admission
CONCLUSION: SA-AKI was found to be frequent in this study in two tertiary hospital ICUs in Johannesburg, and the need for inotropic support predicted mortality after ICU admission
Sepsis is a clinical condition in which the inflammatory response to an infection causes organ dysfunction distal to the primary site of infection.[1] Sepsis-associated acute kidney injury (SA-AKI) has been shown to cause significant morbidity and mortality in both children and adults with severe illness.[2,3] SA-AKI occurs in 35 - 70% of critically ill patients and increases both in-hospital morbidity and mortality.[4] In the USA, a 22-year retrospective analysis of hospitalised patients from discharge records of non-federal acute care hospitals found that sepsis occurred at an annual rate of 13.7% of hospital admissions.[5] In a single-centre retrospective cohort study in Asia in critically ill patients in the intensive care unit (ICU), the reported incidence of acute kidney injury (AKI) was nearly 55% and sepsis was the cause in 49% of cases.[6] In a study in South Africa (SA) in HIV-positive patients, sepsis was the most common cause of AKI, in 60% of the patients,[7] and in another study also conducted in SA in critically ill patients with AKI, ~41% of AKI was caused by sepsis. [8] There have been shown to be many risk factors for developing SA-AKI. In a meta-analysis that referenced 47 papers, it was noted that in patients diagnosed with sepsis or septic shock, hypertension, diabetes mellitus (DM), inotropic support and mechanical ventilation had 2.9-fold, 1.4-fold, 1.6-fold, 3.0-fold and 1.6-fold odds ratios, respectively, for developing SA-AKI.[9] In other studies, older age and low serum albumin levels (<35 g/L) were also found to be significant factors associated with SA-AKI.[6,10] There are very few studies from Africa, and those that are available focused on elucidating the causes of AKI in critically ill patients and included SA-AKI as one of these causes.[8,11]
For this reason, we conducted a study on SA-AKI in critically ill patients to determine the burden and associated risk factors in two tertiary centres in Johannesburg, SA. The study also investigated the influence of serum albumin, anaemia, underlying comorbidities and use of inotropes in critically ill patients admitted to ICUs in these two hospitals.
Methods
Study design, setting and population
This was a prospective observational study conducted in the ICUs of two tertiary teaching hospitals (Charlotte Maxeke Johannesburg Academic Hospital (CMJAH) and Chris Hani Baragwanath Academic Hospital (CHBH)) in Johannesburg from 15 February 2016 to 15 February 2020. Ethical approval was obtained from the University of the Witwatersrand Human Research Ethics Committee (ref. no. #M160901), and the study was conducted according to the Declaration of Helsinki. We recruited consecutive patients who were admitted to the multidisciplinary ICUs with a diagnosis of sepsis within 24 hours of admission to hospital. The inclusion criteria were adult patients aged >18 years with sepsis, and we excluded those with preexisting kidney disease and those who did not give consent. CMJAH and CHBH are two of the largest hospitals in SA and are also the main teaching hospitals for the Faculty of Health Sciences, University of the Witwatersrand, Johannesburg.
Study procedures
We evaluated the medical records and examined participants for risk factors for SA-AKI. Baseline information included age, gender, ethnicity, concomitant illness, including the Acute Physiology and Chronic Health Evaluation version II (APACHE II) score, need for assisted ventilation and inotropic support, and urine output. Baseline laboratory investigations that were recorded included a full blood count, kidney function, C-reactive protein and albumin levels and HIV status. Serum creatinine was analysed using Jaffe's reaction method and the estimated glomerular filtration rate using the modification of diet in renal disease equation.[12]
Study definition and outcomes
Sepsis was defined according to the 2012 Surviving Sepsis guidelines,[13] while SA-AKI was defined according to Kidney Disease Improving Global Outcomes (KDIGO) criteria.[14] The primary outcomes of the study were the development of SA-AKI, the identification of associated risk factors, and 90-day mortality. The presence of hypertension, DM, malignancies and HIV was extracted from the patients' files, as was the APACHE II score.[15] Hypoalbuminaemia was defined as a serum albumin level <35 g/L.
Statistical analysis
Data were analysed using Stata version 13 (StataCorp, USA).
Continuous variables were expressed as means with standard deviations if normally distributed, and otherwise as medians with interquartile ranges (IQRs). Categorical variables were reported as percentages of the number of cases. The association of categorical variables with SA-AKI or mortality was performed using the x2 test. A Wilcoxon-Mann-Whitney test was employed to compare medians. Multivariate logistic regression analysis was employed to determine risk factors associated with development of SA-AKI and 90-day mortality. All factors that were significant at p<0.1 in bivariate analyses were considered in a multivariate logistic regression analysis. The stepwise backward likelihood ratio variable selection method was used, with an enter probability of 0.05 and removal of 0.051. The unadjusted and adjusted odds ratios (ORs) and their 95% confidence intervals (CIs) were reported.
Results
Baseline characteristics
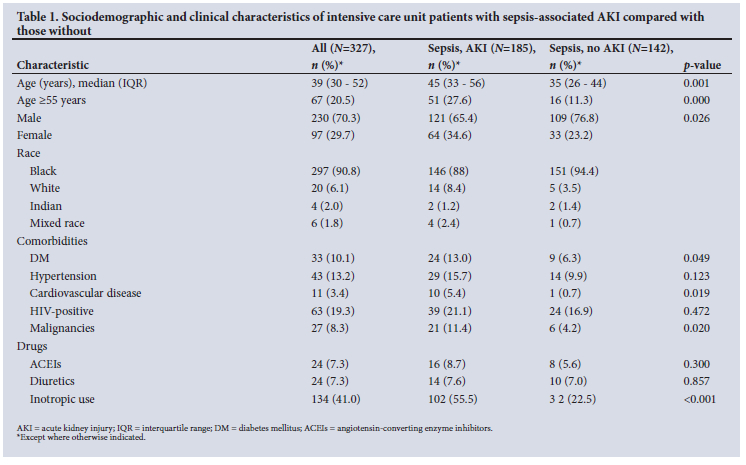
After excluding 10 patients, 327 participants with sepsis were included in the study, and their characteristics are reported in Table 1. The median (IQR) age was 39 (32 - 52) years, 90.8% were black and 6.1% white, and 70.3% were male. The commonest underlying comorbidities were HIV/AIDS (19.3%), hypertension (13.2%) and DM (10.1%).
Rate of sepsis-associated AKI and associated factors
In total, 185 patients in the study (56.6%) developed SA-AKI.
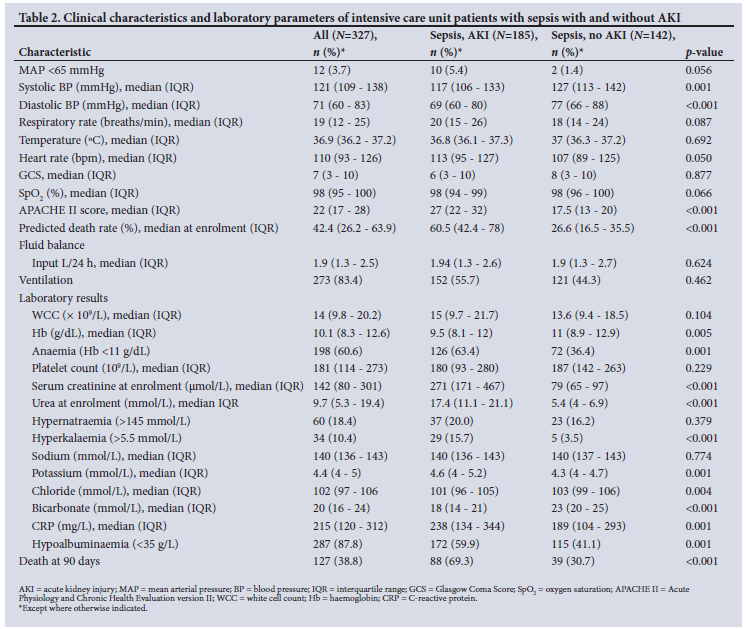
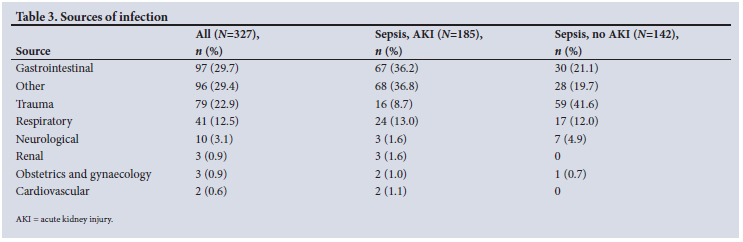
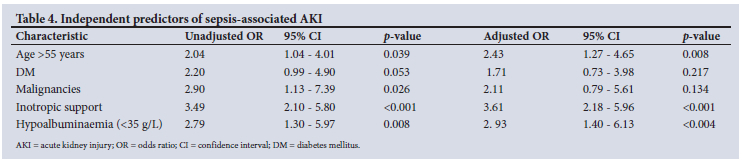
Patients with SA-AKI were likely to be male, to have DM, and to have underlying cardiovascular disease or a malignancy. Furthermore, they were likely to have a high APACHE II score, to be anaemic or hyperkalaemic, and to have a reduced bicarbonate level (Table 2). The sources of infections are shown in Table 3. In unadjusted analysis, age >55 years, male gender, inotropic support, DM, underlying malignancy, anaemia and hypoalbuminaemia (<35 g/L) were found to be significantly associated with SA-AKI. In adjusted analysis, we found that age >55 years (OR 2.43; 95% CI 1.27 - 4.65; p=0.008), use of inotropes (OR 3.61; 95% CI 2.18 - 5.96; p<0.001) and the presence of hypoalbuminaemia (OR 2.93; 95% CI 1.40 - 6.13; p=0.004) increased the likelihood of SA-AKI, as shown in Table 4.
SA-AKI and mortality
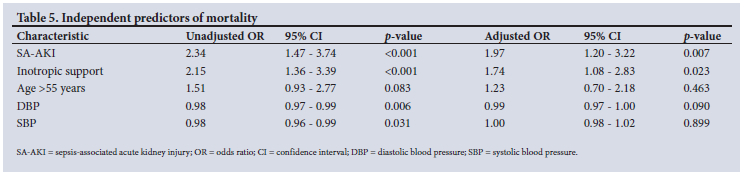
The overall mortality at 90 days after ICU admission was 38.8%. In multivariate analysis, SA-AKI and inotropic support were associated with mortality at 90 days (OR 1.97; 95% CI 1.20 - 3.22; p=0.007 and OR 1.74; 95% CI 1.08 - 2.83; p=0.023, respectively), as shown in Table 5.
Discussion
Our study assessed the burden of SA-AKI and related risk factors and outcomes in the ICUs at two of the largest hospitals in SA. The study showed a high rate of SA-AKI in patients with sepsis at 56.6%, and the predictors were age >55 years, inotropic support, and the presence of low serum albumin (<35 g/L). The predictors of 90-day mortality were SA-AKI and need for inotropic support.
The rate of SA-AKI in the ICU patients in our study was higher than that reported in previous studies.[16] In a retrospective study of 19 579 patients conducted in Beijing, the rate of SA-AKI in patients with sepsis was 48.1%.[17] Additionally, a review of ICU patients from Australia and New Zealand found a rate of 42.1%.[18] A recent analysis of ICU data on patients with sepsis from the Medical Information for Intensive Care III (MIMIC-III) study in the USA found a rate of 40.0%.[19] The high rate of SA-AKI in our study may be explained by the frequency of underlying comorbidities and the fact that almost three-quarters of the patients with SA-AKI were aged >55 years. Another relevant factor could be that a lack of resources relative to the developed world may mean that sicker patients are admitted. Critically ill patients are generally exposed to invasive monitoring devices and catheters and are frequently mechanically ventilated, both of which may predispose them to sepsis and therefore SA-AKI. Previous studies have also reported a positive link between SA-AKI and older age.[17,20]
In the present study, age >55 years correlated positively with SA-AKI, and this finding was comparable to previous studies.[21,22] An analysis of 39 938 ICU patients in a large tertiary care university hospital system in the USA found that older patients had a higher incidence of AKI compared with those aged <55 years.[23] In this study, patients aged >75 years had a rate of AKI 20% higher than those aged <55 years.[23] The probable reason for this finding is that older age is associated with a greater likelihood of underlying comorbidities, as evidenced in the present study, where nearly 55% had comorbidities. Furthermore, there is evidence that elderly patients are more likely to have underlying age-related kidney damage.[10]
The presence of a low serum albumin level had a positive association with development of SA-AKI in our study, a result consistent with previous studies.[24,25] In patients undergoing coronary artery bypass grafting, the AKI group had slightly lower albumin levels compared with controls (39 g/L v. 40 g/L, respectively), and 45% of the patients with low albumin developed AKI.[26] Similarly, in the MIMIC-III study of critically ill patients with sepsis, low albumin (<30 g/L) was associated with 1.33-fold increased odds of SA-AKI.[19] The explanation is probably that albumin is a negative acute-phase reactant that correlates with severity of sepsis, and critically ill patients develop capillary leak with loss of albumin into the interstitium.[27-29]
The need for inotropic support predicted SA-AKI and mortality in the present study. This finding has also been observed in a meta-analysis that included 42 studies of patients with sepsis,[10] in which administration of vasopressor therapy was associated with a 3-fold increase in the odds of developing SA-AKI.[10] This finding is likely to be related to the fact that patients on inotropes have had hypotensive episodes and have had more severe disease. In other studies, vasopressor use was also associated with an increased odds of mortality (OR 1.75).[16] Studies have also shown that patients with sepsis who develop AKI are more likely to have required inotropic support compared with those with sepsis who have not developed AKI.16,22,30]
In the present study, SA-AKI was associated with mortality at least twice as high at 90 days as in patients with sepsis only (69.3% v. 30.7%), and SA-AKI was also associated with a 1.9-fold increase in the odds of death at 90 days. This finding is consistent with previous studies that have examined SA-AKI and its outcomes. In a multicentre retrospective review of data from the Australia and New Zealand Intensive Care Society Adult Patient Database, Bagshaw et al.[18] observed a high ICU and hospital mortality rate in patients with SA-AKI at 30.0% and 20.0%, respectively, compared with those with AKI from other causes at 22.0% and 13.4%, and 13.0% and 7.5% in those with sepsis only.[18] A study in SA that was limited to critically ill ICU patients also showed increased mortality in those with AKI v. those without (20.5% v. 2.3%).[31]
This prospective study has shown important confirmatory findings relevant to a tertiary hospital in Africa. Although the sample size was adequate, there are some limitations. The sample was drawn from mixed ICUs at only two centres, which may mean that the data are not representative of other centres in Africa. Similarly, outcomes could have been influenced by specific management practices. Thirdly, vital information on renal replacement therapy and its mode and intensity was not collected, and dialysis could have had an influence on outcomes.
Conclusion
We have demonstrated that the rate of SA-AKI was high in our critically ill population, and that development of SA-AKI was associated with older age (>55 years), hypoalbuminaemia and need for inotropic support. SA-AKI has previously been shown to be a risk factor for mortality. There is, however, a need to find new biomarkers that will identify patients at risk of developing SA-AKI, so that appropriate measures can be instituted early to improve outcomes. There is also a need for more studies from Africa to investigate and categorise the prevalence of SA-AKI in critically ill patients.
Declaration. The research for this study was done in partial fulfilment of the requirements for MDM's PhD degree in nephrology at the University of the Witwatersrand.
Acknowledgements. The authors thank the patients attending CMJAH and CHBAH who participated in this study, and the staff at the both facilities. MDM thanks the International Society of Nephrology, the University of the Witwatersrand and the Zambian Ministry of Health for supporting his training. He also acknowledges his supervisors and research team for their guidance and support.
Author contributions. MDM: conceptualised the research, collected data, participated in data analysis and write-up; CD, GP and GAR participated in conceptualisation, supervision, editing and review; JB: was involved in formal analysis, write-up and review of the research. Funding. The study was funded by research funds contributed by research collaborators (Prof. Saraladevi Naicker) and a grant from the University of the Witwatersrand Faculty Research Committee (individual research grant no. 001,401). Conflicts of interest. None.
References
1. Zarjou A, Agarwal A. Sepsis and acute kidney injury. J Am Soc Nephrol 2011;22(6):999-1006. https://doi.org/10.1681/asn.2010050484 [ Links ]
2. Alobaidi R, Basu RK, Goldstein RL, Bagshaw SM. Sepsis-associated acute kidney injury. Semin Nephrol 2015;35(1):2-11. https://doi.org/10.1016/j.semnephrol.2015.01.002 [ Links ]
3. Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S. Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 2005:294(7):813-818. https://doi.org/10.1001/jama.294.7.813 [ Links ]
4. Lopes JA, Fernandes P, Jorge S, et al. Long-term risk of mortality after acute kidney injury in patients with sepsis: A contemporary analysis. BMC Nephrol 2010;11(9):1471-2369. https://doi.org/10.1186/1471-2369-11-9 [ Links ]
5. Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med 2003;348(16):1546-1554. https://doi.org/10.1056/nejmoa022139 [ Links ]
6. Shum HP, Kong HH, Chan KC, Yan WW, Chan TM. Septic acute kidney injury in critically ill patients - a single-center study on its incidence, clinical characteristics, and outcome predictors. Ren Fail 2016;38(5):706-716. https://doi.org/10.3109/0886022x.2016.1157749 [ Links ]
7. Vachiat AI, Musenge E, Wadee S, Naicker S. Renal failure in HIV-positive patients - a South African experience. Clin Kidney J 2013;6(6):584-589. https://doi.org/10.1093/ckj/sft128 [ Links ]
8. Aylward RE, van der Merwe E, Pazi S, et al. Risk factors and outcomes of acute kidney injury in South African critically ill adults: A prospective cohort study. BMC Nephrol 2019;20(1):460. https://doi.org/10.1186/s12882 [ Links ]
9. Liu J, Xie H, Ye Z, Li F, Wang L. Rates, predictors, and mortality of sepsis-associated acute kidney injury: A systematic review and meta-analysis. BMC Nephrol 2020;21(1):318. https://doi.org/10.1186/s12882-020-01974-8 [ Links ]
10. Yokota LG, Sampaio BM, Rocha EP, et al. Acute kidney injury in elderly patients: Narrative review on incidence, risk factors, and mortality. Int J Nephrol Renovasc Dis 2018;11:217-224. https://doi.org/10.2147/ijnrd.s170203 [ Links ]
11. Khuweldi MA, Skinner DL, de Vasconcellos K. The incidence and outcomes of patients with acute kidney injury in a multidisciplinary intensive care unit in Durban, South Africa. South Afr J Crit Care 2020;36(2):80-85. https://doi.org/10.7196/SAJCC.2020.v36i2.426 [ Links ]
12. Madero M, Sarnak MJ. Creatinine-based formulae for estimating glomerular filtration rate: Is it time to change to chronic kidney disease epidemiology collaboration equation? Curr Opin Nephrol Hypertens 2011;20(6):622-630. https://doi.org/10.1097/mnh.0b013e32834ba210 [ Links ]
13. Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med 2013;39(2):165-228. https://doi.org/10.1007/s00134-012-2769-8 [ Links ]
14. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int 2012;2(Suppl 1):1-138. https://kdigo.org/wp-content/uploads/2016/10/KDIGO-2012-AKI-Guideline-English.pdf (accessed 9 November 2022). [ Links ]
15. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: A severity of disease classification system. Crit Care Med 1985;13(10):818-829 https://doi.org/10.1097/00003246-198510000-00009 [ Links ]
16. Wang X, Jiang L, Wen Y, et al. Risk factors for mortality in patients with septic acute kidney injury in intensive care units in Beijing, China: A multicenter prospective observational study. Biomed Res Int 2014;2014:172620. https://doi.org/10.1155/2014/172620 [ Links ]
17. Wang H, Ji X, Wang AY, et al Epidemiology of sepsis-associated acute kidney injury in Beijing, China: A descriptive analysis. Int J Gen Med 2021;14:5631-5649. https://doi.org/10.2147/ijgm.s320768 [ Links ]
18. Bagshaw SM, George C, Bellomo R. Early acute kidney injury and sepsis: A multicentre evaluation. Crit Care 2008;12(2):R47. https://doi.org/10.1186/cc6863 [ Links ]
19. Yang S, Su T, Huang L, Feng L-H, Liao T. A novel risk-predicted nomogram for sepsis associated-acute kidney injury among critically ill patients. BMC Nephrol 2021;22(1):173. https://doi.org/10.1186/s12882-021-02379-x [ Links ]
20. Alobaidi R, Basu RK, Goldstein SL, Bagshaw SM. Sepsis-associated acute kidney injury. Semin Nephrol 2015;35(1):2-11. https://doi.org/10.1016/j.semnephrol.2015.01.002 [ Links ]
21. Bagshaw SM, George C, Dinu I, Bellomo R. A multi-centre evaluation of the RIFLE criteria for early acute kidney injury in critically ill patients. Nephrol Dial Transplant 2008;23(4):1203-1210. https://doi.org/10.1093/ndt/gfm744 [ Links ]
22. Hoste EA, Lameire NH, Vanholder RC, Benoit DD, Decruyenaere JM, Colardyn FA. Acute renal failure in patients with sepsis in a surgical ICU: Predictive factors, incidence, comorbidity, and outcome. J Am Soc Nephrol 2003;14(4):1022-1030. https://doi.org/10.1097/01.asn.0000059863.48590.e9 [ Links ]
23. Kane-Gill SL, Sileanu FE, Murugan R, Trietley GS, Handler SM, Kellum JA. Risk factors for acute kidney injury in older adults with critical illness: A retrospective cohort study. Am J Kidney Dis 2015;65(6):860-869. https://doi.org/10.1053Zj.ajkd.2014.10.018 [ Links ]
24. Dos Santos RP, Carvalho ARdS, Peres LAB. Incidence and risk factors of acute kidney injury in critically ill patients from a single centre in Brazil: A retrospective cohort analysis. Sci Rep 2019;9(1):18141. https://doi.org/10.1038/s41598-019-54674-1 [ Links ]
25. Yu M-y, Lee SW, Baek SH, et al. Hypoalbuminemia at admission predicts the development of acute kidney injury in hospitalized patients: A retrospective cohort study. PLoS ONE 2017;12(7):e0180750. https://doi.org/10.1371/journal.pone0180750 [ Links ]
26. Aksoy R, Adademir T, Yilmaz E, et al Is hypoalbuminemia a predictor for acute kidney injury after coronary bypass grafting in diabetes mellitus patients? Braz J Cardiovasc Surg 2019;34(5):565-571. https://doi.org/10.21470/1678-9741-2018-0291 [ Links ]
27. Ranzani OT, Zampieri FG, Forte DN, Azevedo LC, Park M. C-reactive protein/albumin ratio predicts 90-day mortality of septic patients. PLoS ONE 2013;8(3):e59321. https://doi.org/10.1371/journal.pone.0059321 [ Links ]
28. Wiedermann CJ, Joannidis M. Nephroprotective potential of human albumin infusion: A narrative review. Gastroenterol Res Pract 2015;2015:1-8. https://doi.org/10.1155/2015/912839 [ Links ]
29. Wiedermann CJ. Hypoalbuminemia as surrogate and culprit of infections. Int J Mol Sci 2021;22(9):4496. https://doi.org/10.3390/ijms22094496 [ Links ]
30. Bagshaw SM, Uchino S, Bellomo R, et al. Septic acute kidney injury in critically ill patients: Clinical characteristics and outcomes. Clin J Am Soc Nephrol 2007;2(3):431-439. https://doi.org/10.2215/cjn.03681106 [ Links ]
31. Aylward R, Merwe E, Pazi S, et al. Risk factors and outcomes of acute kidney injury in South African critically ill adults: A prospective cohort study. BMC Nephrol 2019;20(1):460. https://doi.org/10.1186/s12882-019-1620-1627 [ Links ]
 Correspondence:
Correspondence:
M D Mweene
dimakweenda@yahoo.com
Accepted 2 August 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}