










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.12 Pretoria Dez. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i12.16552
RESEARCH
COVID-19 in pregnant women in South Africa: A retrospective review
S BhooraI, II; J ZampariniIII; N OdellIV, V; L MurrayVI; G BalieVII, VIII; N SanyikaIX; K MallX; T RamdinXI; A MahomedXII; L ChaukeXIII
IMB BCh, MSc; Department of Obstetrics and Gynaecology University of the Witwatersrand, Johannesburg, South Africa
IIMB BCh, MSc; Department of Obstetrics and Gynaecology, Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
IIIMB ChB, MMed (Int Med); Department of Internal Medicine, University of the Witwatersrand and Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
IVMB BCh, MMed (O&G); Department of Obstetrics and Gynaecology University of the Witwatersrand, Johannesburg, South Africa
VMB BCh, MMed (O&G); Department of Obstetrics and Gynaecology, Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
VIMB ChB, DPhil; Division of Infectious Diseases, Department of Internal Medicine, University of the Witwatersrand and Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
VIIMB ChB, MMed (O&G); Department of Obstetrics and Gynaecology University of the Witwatersrand, Johannesburg, South Africa
VIIIMB ChB, MMed (O&G); Department of Obstetrics and Gynaecology, Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
IXMBBS; Department of Internal Medicine, University of the Witwatersrand and Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
XMB ChB; Department of Internal Medicine, University of the Witwatersrand and Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
XIMB BCh, MMed (Paed); Department of Paediatrics and Child Health, University of the Witwatersrand and Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
XIIMB BCh, FCP (SA); Department of Internal Medicine, University of the Witwatersrand and Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
XIIIMMed (O&G), PhD; Department of Obstetrics and Gynaecology University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: The majority of maternal deaths in South Africa (SA) occur as a result of non-pregnancy-related infections (NPRI). Pregnancy is a known risk factor in severe COVID-19, increasing the burden of NPRI in SA. In this study, we describe the prevalence, profile and clinical outcomes of pregnant women with COVID-19 admitted to a tertiary facility
OBJECTIVES: To describe the prevalence, profile and clinical outcomes of pregnant women with COVID-19 admitted to a tertiary facility in Gauteng, SA
METHODS: We performed a retrospective review of all pregnant women with COVID-19 admitted to Charlotte Maxeke Johannesburg Academic Hospital between 6 March and 30 August 2020. Data collected included demographics, medical history, obstetric history, clinical findings and laboratory variables. Outcomes assessed were mortality, admission to intensive care unit (ICU), symptomatic v. asymptomatic disease, maternal and fetal outcome and mode of delivery
RESULTS: A total of 204 pregnant women were included in the study. Of these, 33 (16.2%) women were critically ill, with 21 (10.3%) admitted to the ICU and 3 (1.5%) deaths related to COVID-19. The median gestational age was 37 weeks and median birthweight 2 940 g. Sixty-seven women (33%) were HIV-positive, in keeping with national statistics regarding HIV in pregnancy. Caesarean section was the most common mode of delivery (n=105, 60%). However, no women underwent caesarean section for indications related to COVID-19
CONCLUSION: COVID-19-related mortality in our cohort was higher than that seen internationally, likely due to differences in background maternal mortality rates and difficulty in accessing care
South Africa (SA) is a low- to middle-income country (LMIC) and, despite having made significant progress over the past two decades, the maternal mortality rate (MMR) remains approximately 100/100 000, significantly higher than that seen in high-income countries.[1] The majority of maternal deaths in SA occur as a result of non-pregnancy-related infections, and pregnant women in SA have not been spared the burden of COVID-19.[1] A large SA study conducted at 36 hospitals across the country showed an overall high MMR (6.3%) in women infected with SARS-CoV-2. The MMR was even higher (14.7%) in those admitted primarily for COVID-19, as opposed to those with incidental or asymptomatic disease.[2] In addition, there was a 30% increase in maternal deaths in SA in the first 9 months of 2020, compared with the same time period in 2019.[3] While some of these deaths may have been directly due to COVID-19, it is assumed that the indirect effect of the COVID-19 pandemic on maternal health services also played a significant role.[3] SA has a population that is predominantly black African, with a high burden of HIV as well as non-communicable diseases such as obesity, which presents a unique scenario in the context of COVID-19 and pregnancy. While it is well known that pregnancy itself is a risk factor for severe COVID-19, the added burden of hypertension and obesity in SA may further increase the risk of severe COVID-19 in our pregnant population.[4,5] In addition, the high prevalence of HIV and the potential of severe disease in concomitant HIV and COVID-19 remains.[6-9]
While the majority of pregnant women with COVID-19 have mild to moderate symptoms,[10] it is clear that pregnant women have higher rates of intensive care unit (ICU) admission, endotracheal intubation and invasive ventilation.[11-14] SA studies on COVID-19 in pregnancy have yielded similar results: in the cohort investigated by Budhram et al.,[2] 32.3% of women admitted for COVID-19-related issues required admission to an ICU (as opposed to 8.6% in those with incidental COVID-19) and 20.3% required ventilation (compared with 2.6% in those with incidental COVID-19). COVID-19 may also result in poor pregnancy outcomes, with an increased risk of preterm delivery, miscarriage and neonatal admission to ICU.[15-17]
The risk of mortality in pregnant women with COVID-19 is significantly higher than in those without COVID-19, as has been shown in numerous cohorts across the globe. In addition, the risk of death in pregnant women with COVID-19 compared with their non-pregnant counterparts is approximately 70% higher, with a disproportionate number of deaths in black, Asian and mixed ethnicity (BAME) women compared with white women.[12,18,19]
In this study, we describe the prevalence, profile and clinical outcomes of pregnant women with COVID-19 admitted to a tertiary facility in SA.
Methods
Study design and setting
This was a retrospective analysis of all pregnant women, irrespective of gestational age, with COVID-19 confirmed by either reverse-transcriptase polymerase chain reaction (RT-PCR) or antigen testing admitted to the Charlotte Maxeke Johannesburg Academic Hospital (CMJAH) between 6 March and 30 August 2020. CMJAH is a large central hospital located in Johannesburg, SA, which directly services the inner city of Johannesburg and surrounding suburbs in addition to serving as a referral site to surrounding regional hospitals and midwife-led obstetric units. Approximately 9 500 deliveries occur annually, and more than 30 000 women are seen at the several high-risk antenatal clinics per year at the hospital.
Ethical approval to establish the CMJAH COVID-19 database was granted by the University of the Witwatersrand, Johannesburg Human Research Ethics Committee (Medical), HREC-M (ref. no. M200458), as well as hospital management at CMJAH. Approval to conduct this study was granted by the HREC-M (clearance certificate no. M201169) and the CMJAH management. The study was registered with the National Health Research Database.
Data collection
Patient data were captured on discharge or death from paper-based clinical files onto a digital database (REDCap version 12.1.1, Vanderbilt University, USA).[20,21] Data captured included demographics, medical history, clinical findings and laboratory variables, as well as routine antenatal data and laboratory tests (HIV status, syphilis serology and Rhesus serology). The outcome of the pregnancy, as well as birthweight and Apgar scores, and mode of delivery, including indication for caesarean delivery if done, were also collected.
Women were defined as being symptomatic for COVID-19 if one or more of the following symptoms were present: cough, dyspnoea, sore throat, rhinitis, ageusia, anosmia, diarrhoea, fatigue, malaise, fever and myalgia, and there was no other identifiable cause for these symptoms. The remaining women were considered asymptomatic and deemed as having 'incidental COVID-19' on universal screening, and therefore admitted for pregnancy-related indications. Although not yet validated for use in COVID-19, we assessed clinical severity using the modified early obstetric warning score (MEOWS) as per guidelines issued by the International Society for Infectious Diseases in Obstetrics and Gynaecology (ISIDOG).[22]
Routine laboratory investigations performed for asymptomatic women in our cohort included a full blood count (FBC) and urea, creatinine and electrolytes (U and E), as per hospital protocol. In addition to the FBC and U and E, routine laboratory tests for patients with symptomatic COVID-19 included C-reactive protein (CRP), D-dimer, lactate dehydrogenase, alanine aminotransferase, N-terminal pro-hormone B-type natriuretic peptide, high sensitivity troponin T, ferritin, differential count and procalcitonin (PCT). Women with known HIV or those newly diagnosed also had a CD4 count and HIV viral load done on admission, as per national guidelines for the prevention of mother-to-child transmission.[23]
An HIV viral load of <50 copies/mL was considered suppressed, in keeping with national guidelines.[23]
Statistical analysis
Data were exported from the REDCAP database into Excel (version 16.5.4, Microsoft Corp., USA) and Prism 9.3 (GraphPad Software Inc., USA) for analysis. Non-parametric tests were used for all analyses, as data were found to be non-normally distributed using the Shapiro-Wilk normality test. Continuous variables are presented as medians with interquartile ranges (IQR), 95% confidence intervals and standard deviations. Comparative statistics were performed using the Mann-Whitney U, Fisher's exact test and Spearman's rank correlation, where appropriate. We considered a p-value of <0.05 as statistically significant.
Results
Demographics
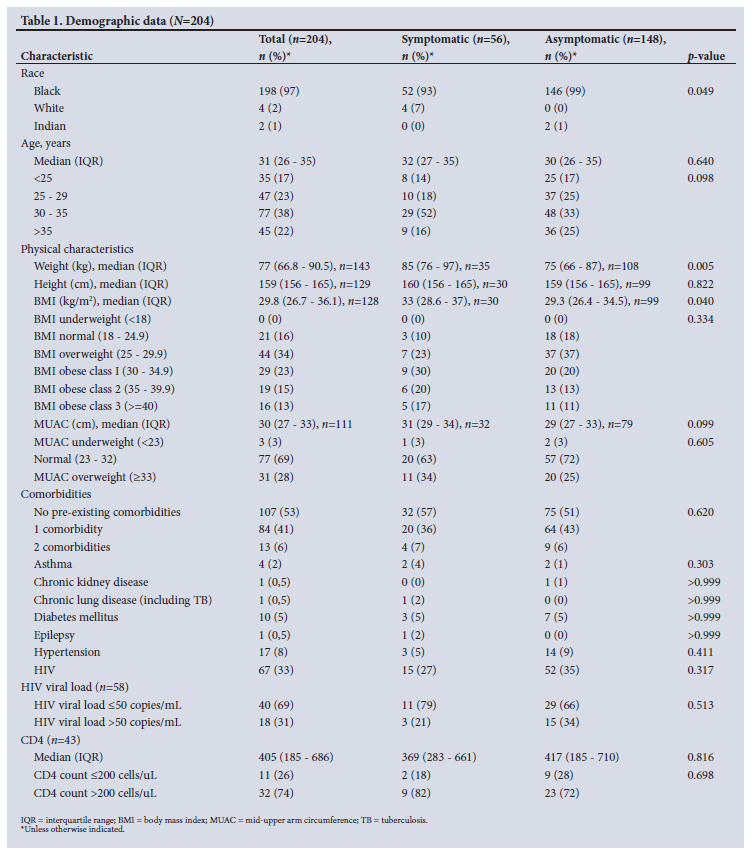
At the time of analysis, the CMJAH COVID-19 database included 236 pregnant women with COVID-19, of whom 32 had incomplete data, resulting in a final cohort of 204 pregnant women for analysis. The majority of the women in our cohort were black (n=198, 97%), with a median age of 31 years. There were 7 adolescent pregnancies (3.4%), and 57 women (28%) were of advanced maternal age (aged >35 years). Body mass index (BMI) data were missing for 75 women in the cohort (37%). However, in those with BMI available, 44 (34%) were in the overweight range and 64 (51%) considered obese by BMI. The majority of the women in our cohort had no previously documented comorbid disease (n=107, 52%), with 84 (41%) and 13 (6%) women affected by 1 comorbidity and >1 comorbidity, respectively. Sixty-seven women (33%) were HIV-positive, in keeping with national statistics regarding HIV in pregnancy. HIV viral loads were available for 58 of the 67 women with HIV (87%), with only 40 women (69%) virologically suppressed at the time of delivery. For those with a CD4 count available (n=43, 64%), 32 (74%) had a CD4 count >200 cells/uL. Demographic data are presented in Table 1.
Symptoms
Women with asymptomatic COVID-19 made up the majority of our study cohort (n=148, 73%). These women were admitted for obstetric indications as opposed to COVID-19-related illness. The remaining 56 women (27%) presented with symptoms typical of COVID-19 including cough, dyspnoea and headache in 18 (9%), 12 (6%) and 8 (4%) women, respectively. Fever was not documented in any of our cohort and only 5 women (2.5%) were found to have an oxygen saturation <94% on room air. However, during the initial part of the study period, the admission protocol for obstetric patients did not include routine monitoring of oxygen saturation, therefore it was recorded in only 128 women. There was no statistically significant difference in the presence of comorbidities in symptomatic women (24% v. 32%, p=0.43), nor was there a strong correlation between severity of illness and BMI (r=-0.14). Patients with pre-eclampsia were significantly more likely to have severe disease than not (20% v. 8%, p<0.0001). However, it was not clear whether it was the pre-eclampsia or the COVID-19 that drove the severity in these women. Symptom, vital and severity data are presented in Table 2 and Fig. 1.

Obstetric and fetal outcomes
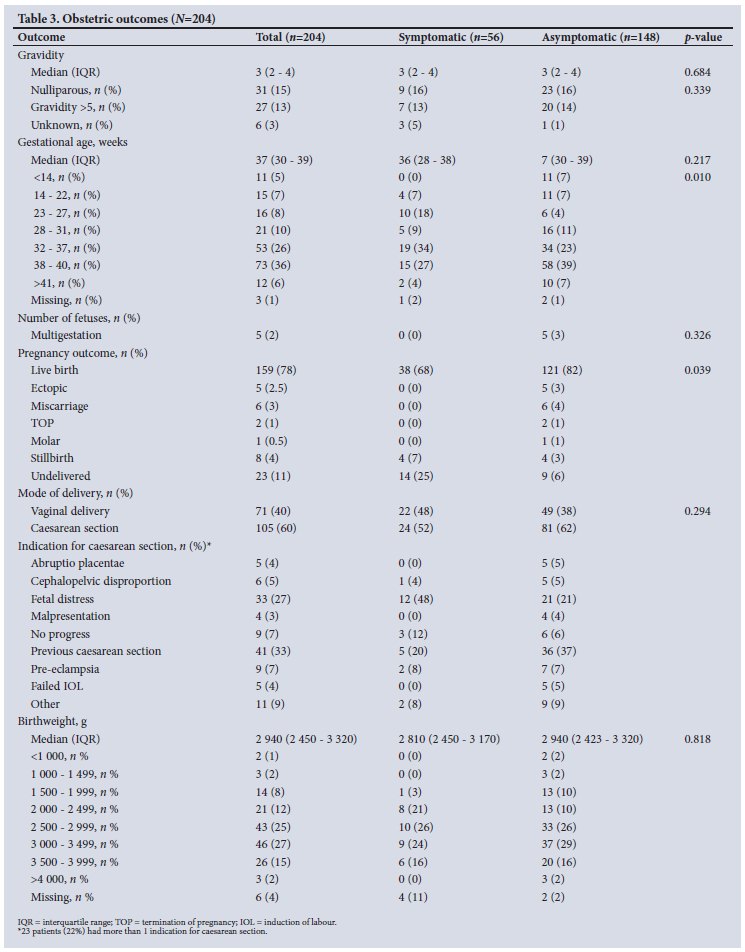
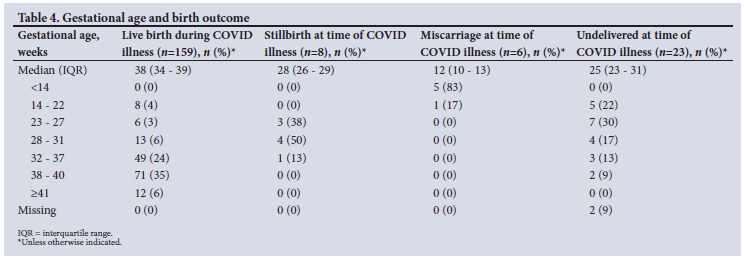
The median (IQR) gestational age for women in our cohort was 37 (30 - 39) weeks. Eighty-five women (42%) presented at a gestational age of 38 weeks or later, with 11 women (5%) in the first trimester at the time of admission. Thirty-one women (15%) were nulliparous and 27 (13%) were pregnant for the fifth time or more. Twenty-three patients (11%) were undelivered at the time of discharge and 159 delivered during their admission, with 164 live infants born, including 5 sets of twins. Caesarean section was the most common mode of delivery (n=105, 60%), with the indication for caesarean section being a previous operative delivery in one-third of these women and fetal distress the indication in 33 (27%). No women underwent caesarean section for indications related to COVID-19. The median (IQR) birthweight for the infants born alive was 2 940 (2 450 - 3 320) g; 19 infants (11%) were born weighing <2 000 g and 3 (2%) weighed >4 000 g. Neonates were only tested for COVID-19 if they required admission, and of those admitted only 1 was positive for COVID-19. The remaining pregnancy outcomes are presented in Table 3. Eight pregnancies ended in stillbirths (4%), of which 3 occurred in women who had not received any antenatal care prior to admission, 3 were as a result of chorioamnionitis, 1 occurred in a woman with confirmed syphilis and 1 in a woman admitted to ICU with an inferior vena cava thrombosis, with COVID-19 a likely contributing factor. The median gestational age at time of stillbirth was 28 weeks. There were 6 miscarriages (3%) occurring at a median gestational age of 18 weeks. Data for gestational age and birth outcomes are shown in Table 4.
Laboratory results
In those patients with a CRP done, median levels were elevated at 41 mg/L, as was PCT at 0.095 ng/mL. There was no significant difference in laboratory results in those who did and did not require ICU, nor was there a difference in laboratory results in symptomatic v. asymptomatic patients. Laboratory results are presented in Table 5.
Maternal outcomes
There was an overall mortality rate of 1.5% (n=3). All women who died had severe COVID‑19 and required admission to ICU.
Two women had concomitant severe preeclampsia and one was HIV-positive; however, she had a CD4 of 369 cells/uL and was virally suppressed at the time of death. Twenty-one women (10%) were admitted to an ICU, of which 3 (1%) required invasive ventilatory support and 8 (4%) non-invasive ventilation via continuous positive airway pressure. While there was no significant difference in pulse rate or temperature among women admitted to ICU, there was a statistically significant increase in respiratory rate compared with those who did not require ICU admission (20 v. 18 breaths per minute, p=0.002). There was no relationship found between HIV status and likelihood of ICU admission (p=0.22).
MEOWS score
We used the MEOWS score, as presented in the ISIDOG guidelines,[22] to classify severity of disease in our patients on admission. A total of 128 women (63%) had a MEOWS score of 0 and were considered stable, while 33 (16%) had a MEOWS score of ≥6 and were considered critical on admission. Our data only included the MEOWS score on admission, and we are unable to report on the change in score during admission. This is evident as 16 (76%) of the women admitted to ICU had a MEOWS score of <6 on admission, indicating that they decompensated during the course of admission. Similarly, two of the women who died had a MEOWS score of 0 on admission. However, of those with a MEOWS score of >6 on admission, 28 (85%) required admission to ICU, arguing for the use of this score in pregnant women with COVID-19.
Discussion
In this study we report on 204 pregnant women with SARS-CoV-2 infection, with an overall mortality rate of 1.5%. This is lower than that seen in a large SA study (6.3%),[2] but similar to that seen in the INTERCOVID study (1.6%),[11] both of which ran over the same time period. We note a higher mortality rate, however, when compared with similar cohorts from the USA (0.15%)[12] and UK (0.7%).[24] All three women who died in our cohort required ICU admission, and two of them had severe pre-eclampsia, which we believe contributed to their deaths. Noting the higher mortality rate when compared with the USA and UK, we believe that this is in keeping with the vastly different background maternal mortality rate in SA compared with these two countries, with late access to care contributing significantly. Limited access to ICU may also have played a role.
Women who were asymptomatic at the time of admission accounted for 73% of our cohort, similar to the findings in another SA study,[2] but in contrast to data from the UK for a similar time period, where 63% of women were symptomatic.[24] Our institution, as well as many others in SA, undertook routine screening for all admitted patients from early on in the pandemic, and this may explain the higher number of asymptomatic cases. In addition, over the time period in question, new cases in SA peaked at 13 944 per day (218.25 cases per million people on 24 July 2020), whereas the peak in the UK was half that number at 6 201 cases per day (69.39 cases per million people on 1 May 2020), which may indicate a higher level of community spread in SA.[25-27]
In keeping with the finding of milder disease, only 5 women (2.5%) were hypoxaemic and 16 (8.1%) tachypnoeic, with the majority of our patients (63%) classified as 'stable' according to the MEOWS score. We noted a significant association between tachypnoea and ICU admission in our cohort. While the use of this scoring system in COVID-19 has not yet been validated, it has been recommended for use by ISIDOG as well as a number of National Health Service trusts in the UK for use in COVID-19, owing to its ease of use and its ability to detect subtle changes early. A similar tool has been advocated for by the National Committee on Confidential enquiries into Maternal Deaths, and is a component of the proposed maternity record; however, it is limited to the postpartum period.[1] Further research is needed on the use of scoring systems to triage pregnant women with COVID-19.
A significant number of women in our cohort were considered obese by BMI, with 51% of those with a BMI available considered obese and 34% overweight. This number is higher than the 36% SA estimate for rates of obesity in pregnancy.[4] Data have shown a link between obesity and COVID-19 infection in pregnancy: 48.6% of women with COVID-19 were obese compared with 40.2% without COVID-19 in the INTERCOVID study.[11] In addition, our centre is a referral site for complicated pregnancies, and women with obesity may have additional comorbidities requiring specialist input.
Adolescent pregnancies accounted for 3.4% (n=7) of our cohort, the youngest being 14 years old at the time of delivery, highlighting both the global and national burden of adolescent pregnancy, something not spared by the COVID-19 pandemic. Data from SA show that 9% of women aged 15 - 17 years old have begun childbearing, a number that increases to 16% if the age range is increased to 15 - 19 years.[28] Furthermore, there was a 60% increase in adolescent pregnancies in Gauteng Province, where our facility is based, between April 2020 and March 2021, a phenomenon driven by lack of access to condoms and other contraceptives during the lockdowns associated with COVID-19.[29] Globally, ~12 million women aged 15 - 19 give birth in developing countries.[30] Reassuringly, none of this age group in our cohort experienced severe COVID-19 disease, nor did any require ICU admission or die.
HIV-positive women accounted for 33% of our cohort, a similar number to that seen by Budhram et al.,[2] and in keeping with the estimated national prevalence of 30%.[31] However, only 69% were virologically supressed. Despite being in keeping with the rate of HIV viral suppression in national estimates, the rate of viral suppression of 69% in our study is concerning given SA's aim to reach the Joint United Nations Programme on HIV and AIDS target of 95% viral suppression by 2030.[32] Nevertheless, we were reassured by the fact that only one HIV-positive woman died (1.5%), with no difference in mortality between HIV-positive and HIV-negative women (1.5% v. 1.4%, p=0.964). Furthermore, there was no difference in severity of disease nor an increased rate of ICU admission in HIV-positive women compared with HIV-negative women (6% v. 12%, p=0.22). These findings are similar to a non-pregnant cohort of HIV-positive patients from our hospital.[7]
We report a caesarean section rate of 60%, with one-third of these women undergoing caesarean section due to a previous operative delivery, and no women undergoing caesarean for COVID-19-related indications. While the rate of caesarean section in our cohort is higher than the SA rate of 28.6%, and far higher than the 'ideal rate' of 10% - 15% recommended by the World Health Organization, we believe the high number of caesarean deliveries is likely due to the level of care provided by our institution as a referral centre for the province.[1,33] Furthermore, in keeping with our setting as a referral centre for high-risk pregnancies, we report a higher rate of preterm deliveries (39%) than that seen in other studies. Similarly, we report 12 miscarriages (5.9%) and 8 (3.9%) stillbirths, rates not increased when compared with pre-pandemic studies, although it is unclear if COVID-19 had any effect on these outcomes.[34,35]
In keeping with findings from other studies, pre-eclamptic women in our cohort were significantly more likely to have severe COVID-19 disease. It is unclear whether this was a 'pre-eclampsia-like syndrome' induced by COVID-19, as reported by Mendoza et al.,[36] or de novo pre-eclampsia. Our facility does not have access to sFlt-1/PlGF testing, and uterine artery doppler indices were not recorded in the clinical records of the women included in our study.
Our cohort was made up mostly of women of black ethnicity, in keeping with the demographics of the population served by our facility, which gives further insight into COVID-19 in women of BAME groups. Data from the USA and UK have shown worse outcomes among pregnant women in this group, as well as increased rates of infection when compared with pregnant women of white ethnicity. Internationally this is attributed to a number of factors, including differences in socioeconomic status. However, SA data on differences amongst racial groups are limited. Notably, the proportion of black patients in this cohort was significantly higher than in two previously published cohorts of patients with COVID-19 from our centre (99% v. 79%'371 and 84%'71), even when corrected for age (99% v. 85%).
Notably, the majority of women in our cohort (78%) were in the third trimester of pregnancy, and those at earlier gestational ages who remained undelivered were not followed up. Neonatal outcome might correlate with timing of viral load/exposure during pregnancy and severity of maternal outcome, so more data are needed on COVID-19 exposure in early pregnancy and maternity outcomes.[38]
Strengths and limitations
Our study was limited by missing data owing to its retrospective nature. Data such as oxygen saturation and COVID-19-specific laboratory tests were not performed on all patients, especially those with asymptomatic disease. We were also unable to follow up on women discharged from our institution undelivered, and therefore outcome data are not available in these women who were lost to follow-up.
In terms of strengths, our study was the first to include the MEOWS score to identify severity of COVID-19 in pregnancy, highlighting the possible importance of scoring systems in risk stratification of COVID-19 in pregnancy. Additionally, we have been able to report on outcomes of COVID-19 in adolescents who are pregnant. The single-centre nature of our cohort is also a strength in that all women received the same standard of care and treatment protocols, reducing confounding factors related to mortality and ICU admission.
Conclusion
COVID-19 in pregnancy is a continuously evolving entity, and our study provides valuable insight into the profiles of pregnant women with COVID-19, especially in a LMIC setting. Future research into the interactions between HIV and COVID-19 in pregnancy, as well as the use of scoring systems such as the MEOWS score in COVID-19 in pregnancy, is needed.
Declaration. None.
Acknowledgements. The authors wish to acknowledge the staff of the COVID-19 Unit in the Department of Obstetrics and Gynaecology at Charlotte Maxeke Johannesburg Academic Hospital.
Author contributions. SB conceived the study and wrote the first draft of the manuscript. SB, JZ, NO, GB, NS, KM and TR assisted with data collection. JZ performed the statistical analysis. All authors contributed to the writing of the final manuscript.
Funding. None.
Conflicts of interest. None.
References
1. National Committee on the Confidential Enquiries into Maternal Deaths. Saving Mothers 2017-2019: Seventh triennial report on confidential enquiries into maternal deaths in South Africa. Pretoria: National Department of Health, 2020. [ Links ]
2. Budhram S, Vannevel V, Botha T, et al. Maternal characteristics and pregnancy outcomes of hospitalised pregnant women with SARS-CoV-2 infection in South Africa: An International Network of Obstetric Survey Systems-based cohort study. Int J Gynecol Obstetr 2021;155(3):455-465. https://doi.org/10.1002/ijgo.13917 [ Links ]
3. Soma-Pillay P, Moodley J, Pattinson R, et al. The effect of the first wave of Covid-19 on use of maternal and reproductive health services and maternal deaths in South Africa. Obstetrics and Gynaecology Forum. 2020 Dec 1;30(4):38-46. https://doi.org/10.10520/ejc-medog-v30-n4-a10 [ Links ]
4. Basu JK, Jeketera CM, Basu D. Obesity and its outcomes among pregnant South African women. Int J Gynaecol Obstet 2010;110(2):101-104. https://doi.org/10.1016/j.ijgo.2010.02.020 [ Links ]
5. Guan W, Ni Z, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. New Eng J Med 2020;382(18):1708-1720. https://doi.org/10.1056/NEJMoa2002032 [ Links ]
6. Statistics South Africa. South Africa Demographic and Health Survey 2016. Key indicator report. Pretoria: StatsSA, 2017. https://www.statssa.gov.za/publications/Report%2003-00-09/Report%2003-00-092016.pdf (accessed 16 November 2022). [ Links ]
7. Venturas J, Zamparini J, Shaddock E, et al. Comparison of outcomes in HIV-positive and HIV-negative patients with COVID-19. J Infection 2021;83(2):217-227. https://doi.org/10.1016/j.jinf.2021.05.020 [ Links ]
8. Jassat W, Cohen C, Tempia S, et al. Risk factors for COVID-19-related in-hospital mortality in a high HIV and tuberculosis prevalence setting in South Africa: A cohort study. Lancet HIV 2021;8(9):e554-567. https://doi.org/10.1016/S2352-3018(21)00151-X [ Links ]
9. Western Cape Department of Health in collaboration with the National Institute for Communicable Diseases, South Africa. Risk Factors for Coronavirus Disease 2019 (COVID-19) Death in a Population Cohort Study from the Western Cape Province, South Africa. Clin Infect Dis. 2021 Oct 5;73(7):e2005-15. https://doi.org/10.1093/cid/ciaa1198 [ Links ]
10. Pastick KA, Nicol MR, Smyth E, et al. A Systematic Review of Treatment and Outcomes of Pregnant Women With COVID-19-A Call for Clinical Trials. Open Forum Infect Dis. 2020 Aug 13;7(9):ofaa350. https://doi.org/10.1093/ofid/ofaa350 [ Links ]
11. Villar J, Ariff S, Gunier RB, et al. Maternal and neonatal morbidity and mortality among pregnant women with and without COVID-19 infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatrics 2021;175(8):817-826. https://doi.org/10.1001/jamapediatrics.2021.1050 [ Links ]
12. Zambrano LD, Ellington S, Strid P, et al. Update: Characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status - United States, January 22 - October 3, 2020. Morb Mortal Weekly Rep 2020;69(44):1641-1647. https://doi.org/10.15585/mmwr.mm6944e3 [ Links ]
13. Allotey J, Stallings E, Bonet M, et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020;370:m3320. https://doi.org/10.1136/bmj.m3320 [ Links ]
14. Badr DA, Mattern J, Carlin A, et al. Are clinical outcomes worse for pregnant women at >20 weeks' gestation infected with coronavirus disease 2019? A multicenter case-control study with propensity score matching. Am J Obstet Gynecol 2020;223(5):764-768. https://doi.org/10.1016/j.ajog.2020.07.045 [ Links ]
15. Kyle MH, Glassman ME, Khan A, et al. A review of newborn outcomes during the COVID-19 pandemic. Semin Perinatol 2020;44(7):151286. https://doi.org/10.1016/j.semperi.2020.151286 [ Links ]
16. Dashraath P, Wong JLJ, Lim MXK, et al. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. Am J Obstet Gynecol 2020;222(6):521-531. https://doi.org/10.1016/j.ajog.2020.03.021 [ Links ]
17. Gale C, Quigley MA, Placzek A, et al. Characteristics and outcomes of neonatal SARS-CoV-2 infection in the UK: A prospective national cohort study using active surveillance. Lancet Child Adolesc Health 2021;5(2):113-121. https://doi.org/10.1016/S2352-4642(20)30342-4. [ Links ]
18. Jering KS, Claggett BL, Cunningham JW, et al Clinical characteristics and outcomes of hospitalized women giving birth with and without COVID-19. JAMA Intern Med 2021;181(5):714-717. https://doi.org/10.1001/jamainternmed.2020.9241 [ Links ]
19. Knight M, Bunch K, Vousden N, et al. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: national population based cohort study BMJ 2020;369:m2107. https://doi.org/10.1136/bmj.m2107 [ Links ]
20. Harris PA, Taylor R, Minor BL, et al The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95:103208. https://dolorg/10.1016/j.jbl2019.103208 [ Links ]
21. Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42(2):377-381. https://doi.org/10.1016/j.jbi.2008.08.010 [ Links ]
22. Donders F, Lonnée-Hoffmann R, Tsiakalos A, et al. ISIDOG recommendations concerning COVID-19 and pregnancy. Diagnostics 2020;10(4):243. https://doi.org/10.3390/diagnostics10040243 [ Links ]
23. National Department of Health, South Africa. 2019 ART clinical guidelines for the management of HIV in adults, pregnancy, adolescents, children, infants and neonates. Pretoria: NDoH, 2020. https://www.knowledgehub.org.za/elibrary/2019-art-clinical-guidelines-management-hiv-adults-pregnancy-adolescents-children-infants (accessed 16 November 2022). [ Links ]
24. Vousden N, Bunch K, Morris E, et al. The incidence, characteristics and outcomes of pregnant women hospitalized with symptomatic and asymptomatic SARS-CoV-2 infection in the UK from March to September 2020: A national cohort study using the UK Obstetric Surveillance System (UKOSS). PLoS One 2021;16(5):e0251123. https://doi.org/10.1371/journal.pone.0251123. [ Links ]
25. UK Government. Coronavirus (COVID-19) in the UK. London: gov.uk, 2022. https://coronavirus.data.gov.uk/details/cases (accessed 8 February 2022). [ Links ]
26. National Institute for Communicable Diseases. Weekly epidemiological brief. NICD, 2021. https://www.nicd.ac.za/diseases-a-z-index/disease-index-covid-19/surveillance-reports/weekly-epidemiological-br (accessed 8 February 2022). [ Links ]
27. Ritchie H, Mathieu E, Rodés-Guirao L, et al. Coronavirus pandemic (COVID-19). Our World in Data 2020. https://ourworldindata.org/covid-cases (accessed 27 June 2022). [ Links ]
28. Statistics South Africa. South Africa Demographic and Health Survey 2016: Report. Pretoria: StatsSA, 2016. https://dhsprogram.com/pubs/pdf/FR337/FR337.pdf#page=103 (accessed 2 February 2022). [ Links ]
29. Reliefweb Press Release. Teen pregnancies in South Africa jump 60% during COVID-19 pandemic - South Africa. ReliefWeb, 23 August 2021. https://reliefweb.int/report/south-africa/teen-pregnancies-south-africa-jump-60-during-covid-19-pandemic (accessed 2 February 2022). [ Links ]
30. World Health Organization. Adolescent pregnancy. Geneva: WHO, 2021. https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnancy (accessed 2 February 2022). [ Links ]
31. Woldesenbet SA, Lombard C, Manda S, et al. The 2019 National Antenatal Sentinel HIV Survey, South Africa. Pretoria: National Department of Health, 2021 https://www.nicd.ac.za/wp-content/uploads/2021/11/Antenatal-survey-2019-report_FINAL_27April21.pdf (accessed 2 February 2022). [ Links ]
32. Abuogi LL, Humphrey JM, Mpody C, et al Achieving UNAIDS 90-90-90 targets for pregnant and postpartum women in sub-Saharan Africa: Progress, gaps and research needs. J Virus Erad 2018;4:33-39. https://doi.org/10.1016/S2055-6640(20)30343-5 [ Links ]
33. World Health Organization. WHO statement on caesarean section rates. Geneva: WHO, 2015. http://www.who.int/reproductivehealth/publications/maternal_perinatal_health/cs-statement/en/ (accessed 7 February 2022). [ Links ]
34. DeSisto CL, Wallace B, Simeone RM, et al. Risk for stillbirth among women with and without COVID-19 at delivery hospitalisation - United States, March 2020 -September 2021. Morbidity Mortality Weekly Rep 2021;70(47):1640-1645. https://doi.org/10.15585/mmwr.mm7047e1 [ Links ]
35. Madhi SA, Briner C, Maswime S, et al. Causes of stillbirths among women from South Africa: A prospective, observational study. Lancet Glob Health 2019;7(4):e503-512. https://doi.org/10.1016/S2214-109X(18)30541-2 [ Links ]
36. Mendoza M, Garcia-Ruiz I, Maiz N, et al. Pre-eclampsia-like syndrome induced by severe COVID-19: A prospective observational study. BJOG 2020;127(11):1374-1380. https://doi.org/10.1111/1471-0528.16339 [ Links ]
37. Zamparini J, Venturas J, Shaddock E, et al. Clinical characteristics of the first 100 COVID-19 patients admitted to a tertiary hospital in Johannesburg, South Africa. Wits J Clin Med 2020;2(2):51. https://doi.org/10.18772/26180197.2020.v2n2a1 [ Links ]
38. Wong SF, Chow KM, Leung TN, et al. Pregnancy and perinatal outcomes of women with severe acute respiratory syndrome. Am J Obstetr Gynecol 2004;191(1):292-297. https://doi.org/10.1016/j.ajog.2003.11.019 [ Links ]
 Correspondence:
Correspondence:
S Bhoora
shastra.bhoora@wits.ac.za
Accepted 19 August 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}