










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.11b Pretoria Nov. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i11b.16844
CASE REPORT
Colonoscopy performed with selective use of sedation: A case report
M Tun
MMed (Surg), FACS; Department of General Surgery, Limpopo Academic Complex and School of Medicine, University of Limpopo, Polokwane, South Africa
ABSTRACT
Colonoscopy is the gold standard for diagnosis of colonic disease. We present a patient with chronic diarrhoea and a caecal tumour that was diagnosed with colonoscopy.
Colonoscopy is the visual examination of the inner lining of the large intestine with a camera on a flexible tube passed through the anus.[1] The most important indications for colonoscopy are evaluation of abnormalities observed on imaging studies, investigation of gastrointestinal (GI) bleeding, investigation of iron deficiency anaemia, investigation of unexplained diarrhoea, surveillance of patients with inflammatory diseases, and screening for and follow-up of colorectal cancer (CRC).[2,3]
Case report
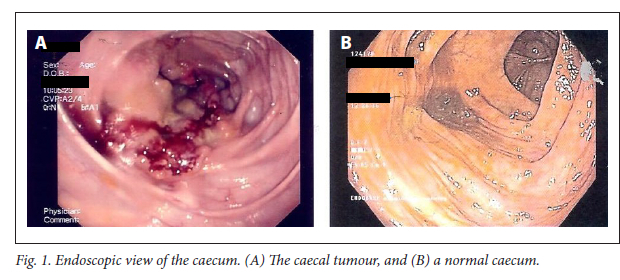
A 45-year-old woman was referred to our endoscopy unit for colonoscopy as a further work-up on her chronic diarrhoea. She reported that she did not have any other chronic medical diseases or a family history of CRC. She had taken bowel preparation medication. The procedure was explained to her in detail, including the sedation that would be used if necessary. The procedure-centred pain (PCP) score was used to assess the patient's requirement for sedation during the procedure. Colonoscopy revealed a malignant-looking lesion in the caecum (Fig. 1), and it was biopsied for histological diagnosis. No concomitant pathologies such as polyps or colitis were detected endoscopically. The patient did not require any sedation during the procedure, as her PCP score remained grade III. It was not possible to pass the colonoscope into the ileum owing to the lesion in the caecum, so the procedure was recorded as an incomplete colonoscopy. Histological examination of the biopsy specimen showed the lesion to be a moderately differentiated invasive adenocarcinoma.
Discussion
Colonoscopy is regarded as the gold standard for diagnosis of colonic diseases. It can detect both cancers and premalignant neoplasms by visualising the entire colon. It also offers the advantages of detection and removal of polyps, as well as diagnostic sampling of cancers.[1,4-7] In our case, the caecal lesion was diagnosed as a malignancy on colonoscopy, and this was confirmed on histological examination of a tissue sample.
GI endoscopic procedures, including colonoscopy, are widely accepted and performed globally. However, these procedures are invasive and often unpleasant. For this reason, procedural sedation has become a fundamental aspect of GI endoscopy to fulfil patients' expectation of a painless procedure without compromising on its quality. There are various options for sedation, ranging from light sedation (anxiolysis) to general anaesthesia, depending on the procedure being performed, the centre of expertise and the individual patient. The wide range of practices include endoscopist-directed sedation, nurse-administered sedation and monitored anaesthesia care (MAC), the use of which depends on individual countries and regions. All of these techniques have certain advantages and disadvantages in terms of utilisation of resources. There are also concerns regarding the safety of the various sedatives, especially the rapid progression from moderate sedation to general anaesthesia, the risk of cardiopulmonary adverse events, and the increased risk of bowel perforation.[8-10]
Our PCP score is conceptualised on the basis of patients' expectation of a painless, high-quality procedure. The score is intended to balance the quality of endoscopy with the risks of sedation, especially at institutions with limited healthcare resources.
PCP is scored as follows:
• The patient is told the nature of the procedure and that some discomfort can be expected. If the patient is still anxious after this explanation, PCP is scored as grade IV, and it is recommended that endoscopist-directed light sedation (anxiolysis) be provided.
• If the complete procedure can be performed without sedation and with only minimal patient discomfort, PCP is scored as grade I.
• If the patient suffers severe discomfort, but this resolves with adjustments in endoscopic manoeuvres, PCP is scored as grade II.
• If the patient suffers severe discomfort and this does not resolve with adjustments in endoscopic manoeuvres, but the discomfort resolves when the endoscope is completely withdrawn and the procedure is able to proceed again, PCP is scored as grade III.
• If the patient suffers severe discomfort even after the endoscope is withdrawn, but the discomfort resolves with endoscopist-directed light sedation (anxiolysis), PCP is scored as grade IV.
• If the patient suffers severe discomfort even after endoscopist-directed light sedation has been provided, PCP is scored as grade V and MAC is highly recommended to assist in monitoring the patient and excluding procedure-related complications.
We did not use any sedation for our patient, as her PCP score was grade III.
There is a need for more qualified endoscopists worldwide to meet patients' expectations of high-quality lower GI endoscopy. There are many training methods in endoscopy: simulators, animal models, and computerised or virtual reality devices. However, colonoscopy training largely remains an apprenticeship on real patients, and this can involve many challenges for the trainees in terms of acquisition of skills.[2] We follow a colonoscopy technique that was acquired and modified from the techniques of Prof. G J Oettle (University of the Witwatersrand) and Prof. F Seow-Choen (National University of Singapore). The skills are acquired by means of apprentice-model training. In this technique, there are 12 essential steps to perform a safe and high-quality colonoscopy:
• Keep the scope straight during the procedure. Always keep the lumen at 12 o'clock and target at 6 o'clock.
• There are only two fixed points in colonoscopy, the anus and the caecum. If the scope reaches the caecum within 75 cm from the anus, the procedure is almost always painless.
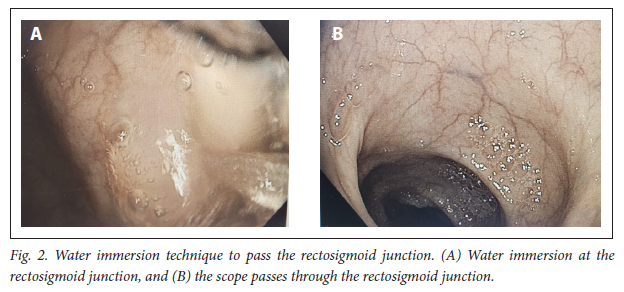
• Only minimal air insufflation should be used, to prevent the so-called balloon effect. Always use water immersion to pass the kinked areas of the colon (Fig. 2).
• Friction at the perineum, stretching the mesentery with scope loops, massive air insufflation and bowel perforation are causes of a painful procedure.
• A painless procedure does not preclude complications, especially in a patient with a difficult splenic flexure.
• Always withdraw the scope as you proceed. Always change the patient's position to take advantage of gravity on mobile bowel.
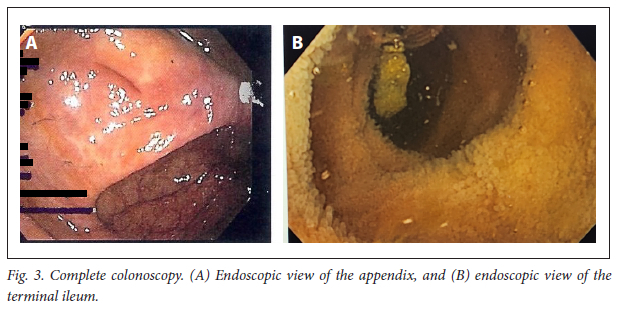
• Always identify the appendix orifice after passing over the ileocaecal valve. Only cannulation of the terminal ileum means a complete colonoscopy (Fig. 3).
• Palpate the patient's abdomen frequently during the procedure.
• Use clockwise torque to prevent a loop at the sigmoid colon, as well as to shorten the scope.
• There must be a one-to-one ratio of scope movements, inside and outside the abdomen.
• The duration of scope withdrawal must be at least the same as the duration of scope insertion. Every mucosal fold must be checked during scope insertion as well as during scope withdrawal.
• Always perform a digital rectal examination before starting the procedure, and always check the anal canal with a retroflexed scope before completing the procedure.
In our patient, a caecal tumour was diagnosed endoscopically and confirmed by subsequent histological examination of a tissue sample. The patient did not require any sedation and was therefore not exposed to any sedation risks.
Conclusion
In our opinion, sedation is not a substitute for performing poor-quality endoscopy. We share our experience with the PCP score and our colonoscopy technique, both of which can be applied to endoscopic procedures at medical institutions with limited resources.
Declaration. None.
Acknowledgements. We thank all staff of the Department of General Surgery, Limpopo Academic Complex, for their contributions to endoscopy services. Without them, this article could not have been written. We also thank Mr C M Aung for his help formatting the figures.
Author contributions. Sole author.
Funding. None.
Conflicts of interest. None.
References
1. Hafner S, Zolk K, Radaelli F, Otte J, Rabenstein T, Zolk O. Water infusion versus air insufflation for colonoscopy. Cochrane Database Syst Rev 2015, Issue 5. Art. No. CD009863. https://doi.org/10.1002/14651858.CD009863.pub2 [ Links ]
2. Papanikolaou IS, Karatzas PS, Varytimiadis LT, et al. Effective colonoscopy training techniques: Strategies to improve patient outcomes. Adv Med Educ Pract 2016;7:201-210. https://doi.org/10.2147/AMEP.S99617 [ Links ]
3. Appropriate use of gastrointestinal endoscopy. Gastrointest Endosc 2000;52(6 Pt 1):831-837. [ Links ]
4. Häfner M. Conventional colonoscopy: Technique, indications, limits. Eur J Radiol 2007;61(3):409-414. https://doi.org/10.1016/j.ejrad.2006.07.034 [ Links ]
5. Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. Gastrointest Endosc 2015;81(1):31-53. https://doi.org/10.1016/j.gie.2014.07.058 [ Links ]
6. Smith RA, Manassaram-Baptiste D, Brooks D, et al. Cancer screening in the United States, 2015: A review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J Clin 2015;65(1):30-54. https://doi.org/10.3322/caac.21261 [ Links ]
7. Lieberman DA, Rex DK, Winawer SJ, Giardiello FM, Johnson DA, Levin TR. Guidelines for colonoscopy surveillance after screening and polypectomy: A consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2012;143(3):844-857. https://doi.org/10.1053/j.gastro.2012.06.001 [ Links ]
8. Ferreira AO, Cravo M. Sedation in gastrointestinal endoscopy: Where are we at in 2014? World J Gastrointest Endosc 2015;7(2):102-109. https://doi.org/10.4253/wJge.v7.i2.102 [ Links ]
9. Metzner J, Domino KB. Risks of anesthesia or sedation outside the operating room: The role of the anesthesia care provider. Curr Opin Anaesthesiol 2010;23(4):523-531. https://doi.org/10.1097/ACO.0b013e32833b7d7c [ Links ]
10. McCain JD, Stancampiano FF, Bouras EP, et al. Creation of a score to predict risk of high conscious sedation requirements in patients undergoing endoscopy. Gastrointest Endosc 2020;91(3):595-605. https://doi.org/10.1016/j.gie.2019.11.015 [ Links ]
 Correspondence:
Correspondence:
M Tun
drmyinttun@outlook.com
Accepted 3 October 2022


{kind=link}
{kind=link}
{kind=link}