










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.11b Pretoria Nov. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i11b.16839
CASE REPORT
Unilateral congenital nasal pyriform aperture stenosis and unilateral choanal atresia - a novel finding: A case report
J A KhosaI; A B (Sebastian) van AsII
IFCORL (SA), MMed (ORL); Department of Ear, Nose and Throat Surgery, Pietersburg Hospital, Limpopo Academic Health Complex, and School of Medicine, University of Limpopo, Polokwane, South Africa
IIMMed (Surg), PhD; Division of Surgery, Pietersburg Hospital, Limpopo Academic Health Complex, and School of Medicine, University of Limpopo, Polokwane, South Africa
ABSTRACT
Congenital nasal pyriform aperture stenosis (CNPAS) is a rare cause of upper airway obstruction in infants, with an incidence of 1 in 25 000 live births. Choanal atresia (CA) is a more common cause of upper airway obstruction, with an incidence of 1 in 5 000 - 8 000 live births. These two conditions often occur independently of each other. Radiologists frequently misinterpret CNPAS as CA. We present a case in which unilateral CNPAS and unilateral CA occurred in the same patient on opposite sides of the nose. The patient had none of the associated craniofacial abnormalities or syndromes. The CNPAS was successfully treated with a sub-labial approach and drilling of the stenotic pyriform aperture, while the CA was dilated with Lister dilators.
Infants are obligate nasal breathers during the first few months of life, so congenital nasal obstructions are life threatening. In diagnosing these potentially lethal conditions, it is important to distinguish between the various types of nasal obstruction. The very rare congenital nasal pyriform aperture stenosis (CNPAS) can easily be confused with choanal atresia (CA), which is more common. Other causes of nasal obstruction include nasal hypoplasia, septal dislocation, meningocele and dermoid cysts. It is important to detect any nasal obstruction at an early stage as it can lead to potentially fatal respiratory failure or asphyxia.
Case report
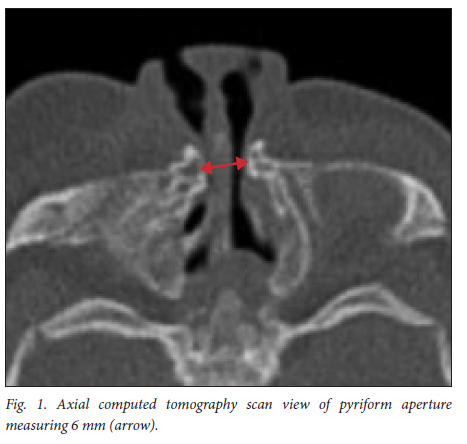
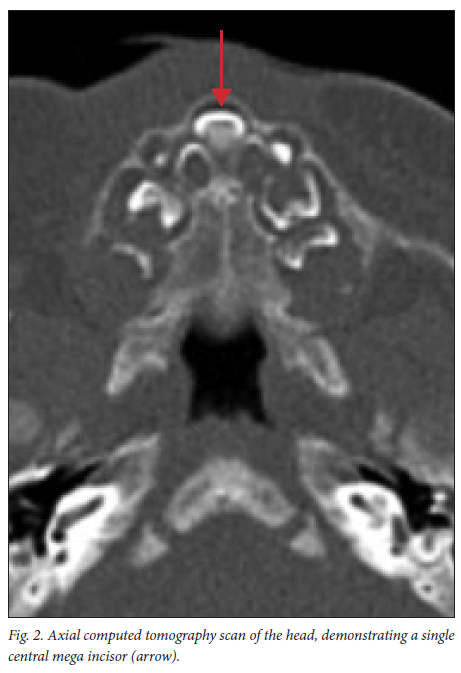
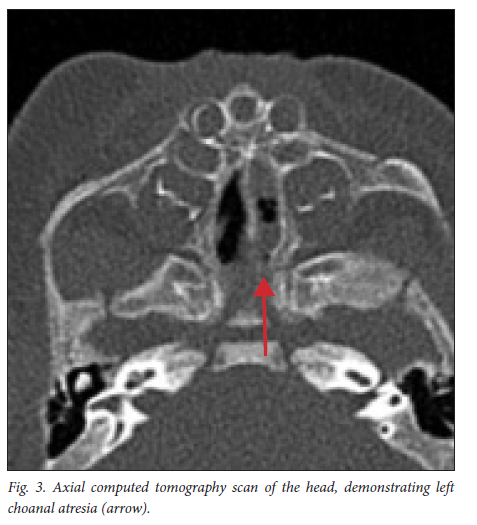
A 1-month-old male infant with a diagnosis of bilateral nasal obstruction, difficulty in breathing, noisy breathing and bilateral discharge of thick white nasal mucus was referred from Malamulele Hospital to the Department of Ear, Nose and Throat Surgery at Pietersburg Hospital in Polokwane, Limpopo Province, South Africa. He had difficulty suckling from his mother's breasts and was failing to thrive. He had been born at term to a 25-year-old primípara via a normal vaginal delivery, with a birth weight of 3 300 g. On arrival at our unit, he had an oropharyngeal airway secured to his mouth with Elastoplast and a feeding tube on the side. He weighed 3 200 g (less than his birth weight). Stertorous breathing with suprasternal and subcostal recessions were noted. His oxygen saturation was 94% with nasal prongs at 1 L/min. Echocardiography of the chest showed no structural abnormalities other than hyperdynamic left ventricular dysfunction. The radiologist reported the presence of left CA, but missed the right pyriform aperture stenosis. The pyriform aperture diameter measured 6.2 mm. A single central mega incisor was present, with a triangular hard palate (Figs 1 - 3). A magnetic resonance imaging scan did not identify any findings to suggest a holoprosencephaly phenotype. The hypothalamic infundibular axis appeared normal.
Surgical management
The upper gingival sulcus and nasal floor were injected with lidocaine 1% and epinephrine 1:100 000. A 2 cm sub-labial incision was made down to the maxillary bone, taking care not to disrupt any tooth buds. A sub-periosteal flap was raised to expose the anterior nasal spine and the floor of the nose. On the right, the floor was raised sufficiently to insert a 2 mm diamond burr, which was used to widen the pyriform aperture laterally and medially. Care was taken to avoid injury to the tooth buds inferiorly and the nasolacrimal duct laterally. Drilling was deemed adequate when a 3.5 mm endotracheal tube (ETT) could easily pass through. The incision was closed in a multi-layered fashion. For the CA on the left, Lister dilators of various sizes were used. A 3.5 mm ETT was left in place for 2 weeks to prevent re-stenosis. At the time of writing, the patient has been followed up for 3 months postoperatively. He continues to have patent nares bilaterally, and his suckling has improved.
Discussion
CNPAS was first described by Brown et al.[1] in 1989 and is a rare cause of airway obstruction in infants. It is estimated to occur in only ~1 in 25 000 live births.'21 As infants are obligate nasal breathers until the age of 4 months, nasal obstruction may lead to respiratory and feeding difficulties and can be potentially life-threatening. Stenosis of the pyriform aperture occurs secondary to bony overgrowth of the nasal processes of the maxilla.[2] A pyriform aperture measuring <11 mm on radiographic imaging is considered stenotic. Furthermore, radiological findings of a central mega-incisor, which is present in approximately 60% of cases, help confirm the diagnosis.[3] One theory is that CNPAS is a form of holoprosencephaly resulting in anomalies of the forebrain and facial midline.[4]
CA, on the other hand, is congenital narrowing or obstruction of the posterior nasal apertures, leading to failure of the posterior nasal cavity to communicate with the nasopharynx. Its incidence is 1 in 5 000 - 8 000 live births. The developmental deformity consists of an enlarged vomer and medialisation of the pterygoid plates and lateral nasal walls. CA was first described by Johann George Roederer in 1755 (in Ha and Vijayasekaran[5]). CA is far more common than CNPAS. The pyriform aperture is a pear-shaped opening bounded by nasal bone superiorly, the nasal process of the maxilla laterally and the maxillary horizontal process inferiorly. A literature search by Ha and Vijayasekaran'51 on Medline, Embase and PubMed databases did not show any study in which CA and CNPAS coexisted. They were the first to report presence of the two conditions in one patient. Their patient appeared to have bilateral nasal pyriform aperture stenosis (NPAS), whereas in our case the NPAS was unilateral, with CA on the contralateral side. In our case, conservative management by the paediatricians at the referring hospital failed, and the infant was failing to thrive, was on supplemental oxygen to maintain his saturation, and was in obvious constant respiratory distress. We therefore decided that operative management was indicated.
Because CNPAS is such a rare condition, radiologists frequently miss the diagnosis and typically incorrectly report the airway obstruction in newborns as CA. This happened in our case, where the radiologist reported only the CA on the left side and missed the NPAS on the right. It is therefore very important for otolaryngologists to be able to read their own scans.
Conclusion
We report a case of unilateral pyriform aperture stenosis together with a contralateral CA in the same patient that to the best of our knowledge, after performing an extensive literature review, has not yet been described. In addition, since NPAS can be missed by radiologists, we consider that otolaryngologists should be clinically astute and able to accurately read their own CT scans, so that they do not miss the diagnosis and are able to manage their patients appropriately.
Declaration. None.
Acknowledgements. None.
Author contributions. Equal contributions.
Funding. None.
Conflicts of interest. None.
References
1. Brown OE, Manning SC, Myer CM. Congenital nasal pyriform aperture stenosis. Laryngoscope 1989;99(1):86-91. https://doi.org/10.1288/00005537-198901000-00016 [ Links ]
2. Rajan R, Tunkel DE. Choanal atresia and other neonatal nasal anomalies. Clin Perinatol 2018;45(4):751-767. https://doi.org/10.1016/j.clp.2018.07.011 [ Links ]
3. Angulo C, Jayawardena ADL, Caruso PA, et al. Congenital nasal piriform aperture atresia: A case report and novel finding. Int J Pediatr Otorhinolaryngol 2020;135:110124. https://doi.org/10.1016/j.ijporl.2020.110124 [ Links ]
4. Tate JR, Sykes J. Congenital nasal pyriform aperture stenosis. Otolaryngol Clin North Am 2009;42(3):521-525. https://doi.org/10.1016/j.otc.2009.03.006 [ Links ]
5. Ha J, Vijayasekaran S. Congenital choanal atresia and pyriform aperture stenosis. Int J Pediatr Otorhinolaryngol Extra 2011;6(4):265-268. https://doi.org/10.1016/j.pedex.2010.11.010 [ Links ]
 Correspondence:
Correspondence:
J A Khosa
jennefer.mansoor@gmail.com
Accepted 25 September 2022

