










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.11b Pretoria Nov. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i11b.16837
CASE REPORT
A rare case of follicular thyroid carcinoma with metastasis to the scalp
T GviliaI; M TunII
IMD, PhD; Department of General Surgery, Limpopo Academic Complex and School of Medicine, University of Limpopo, Polokwane, South Africa
IIMMed (Surg), FACS; Department of General Surgery, Limpopo Academic Complex and School of Medicine, University of Limpopo, Polokwane, South Africa
ABSTRACT
Follicular thyroid carcinoma accounts for 10% of thyroid carcinomas. Cutaneous metastases are rare and usually indicate an advanced tumour stage. We present a case of follicular thyroid carcinoma with scalp metastases.
Thyroid cancer is the most common malignant disease of the endocrine system. Follicular thyroid carcinoma accounts for 10% of thyroid carcinomas and is rare in young populations. It is most common in iodine-deficient areas and tends to occur in an older age group than papillary thyroid cancer.[1] Follicular thyroid cancer has a propensity to spread haematogenously to bone, lung or liver.[2] Cutaneous metastases are rare and usually indicate an advanced tumour stage. Scalp metastases are a rare presentation, seen in 2.5 - 5.8% of follicular thyroid carcinomas.[3]
Case report
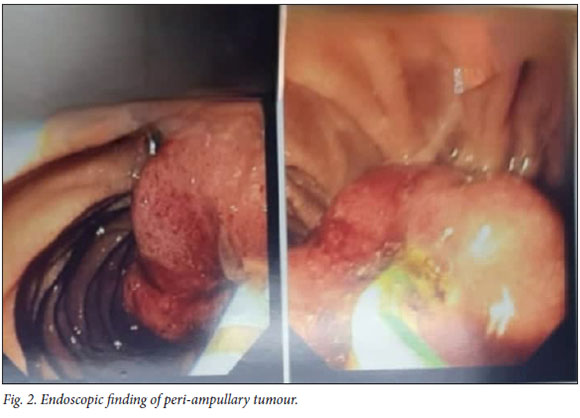
A 60-year-old woman was referred to our department by a neurosurgeon. She had a newly developed scalp tumour, suspected to be of metastatic origin from a thyroid gland. It was a parieto-occipital mass ~7 χ 5 cm in size, and the patient's forehead veins were very distended (Fig. 1). There was no significant anterior neck swelling, or history of dysphagia or voice changes. An excisional biopsy specimen from the mass had features of an underlying neoplastic infiltrate. The patient underwent full metastasis work-up. The results of thyroid function tests were within normal limits. A thyroid ultrasound scan showed multinodular goitre (TIRADS 5), and fine-needle aspiration of the gland showed features of follicular neoplasm. A computed tomography scan showed thyroid carcinoma with skeletal and pulmonary metastases (T3b, N1b, Ml) as well as dilated biliary ducts. She developed obstructive jaundice while awaiting further surgical treatment. Liver function test results confirmed the clinical suspicion of obstructive jaundice. Subsequently, endoscopic retrograde cholangiopancreatography (ERCP) was performed and the patient was found to have a peri-ampullary tumour that was causing obstructive cholangiopathy. A biliary stent was inserted to relieve obstruction, and biopsy of the tumour showed it to be benign (Fig. 2).

The patient's jaundice subsided clinically and biochemically after the ERCP, and she underwent elective thyroidectomy. The thyroid gland was hard, deeply extended to the trachea and left recurrent laryngeal nerve. A near-total thyroidectomy was performed, leaving a small amount of thyroid tissue to avoid damage to the vital cervical structures. There were no postoperative complications and the patient's recovery was uneventful. She was discharged and referred to our nuclear medicine department for further management with radioactive iodine therapy.
Discussion
Metastatic thyroid carcinoma of the scalp can be a diagnostic challenge. Scalp metastases of thyroid carcinoma appear as solitary or multiple reddish nodules. In a world literature review, only 38 cases of scalp metastases from thyroid carcinoma were reported.[4] The most common histological type was follicular carcinoma (46%). A follicular neoplasm is potentially malignant, but it is impossible to differentiate cytologically between a follicular adenoma and carcinoma.[5] The treatment of patients with scalp metastases includes total thyroidectomy and excision of the scalp lesion, followed by administration of radioiodine therapy.
Conclusion
We present a rare case of metastatic follicular thyroid carcinoma. Any slowly growing scalp nodule should raise the suspicion of a metastatic thyroid carcinoma.
Declaration. None.
Acknowledgements. We thank all staff of the Department of General Surgery, Limpopo Academic Complex, for their contributions to surgical services. Without them, this article could not have been written. We also thank Mr C M Aung for his help formatting the figures.
Author contributions. Equal contributions.
Funding. None.
Conflicts of interest. None.
References
1. Tuttle RM. Follicular thyroid cancer (including Hurthle cell cancer). UpToDate, last updated 24 August 2021. uptodate.com/contents/follicular-thyroid-cancer-including-hurthle-cell-cancer?source=history_widget (accessed 22 July 2022). [ Links ]
2. Bucher BT, Moley JF. Endocrine surgery. In: Klingensmit ME, Aziz A, Bharat A, Fox AC, Porembka MR, eds. The Washington Manual of Surgery. 6th ed. Philadelphia: Lippincott Williams & Wilkins, 2011:466-494. [ Links ]
3. Kumar M, Singh A, Mishra S. Scalp metastasis from follicular thyroid carcinoma diagnosed by fine needle aspiration cytology: A case series. Thyroid Res Pract 2016;13(2):80-82. https://doi.org/10.4103/0973-0354.159529 [ Links ]
4. Arslan S, Arslan E. Scalp metastases from thyroid carcinomas: Review of clinical and pathological features. J Med Updates 2014;4(2):71-76. https://doi.org/10.2399/jmu.2014002010 [ Links ]
5. Arora D, Singh N, Doda V. Lytic skull metastasis from follicular carcinoma of thyroid: A case diagnosed on cytology. J Fam Community Med 2018;25(2):129-130. https://doi.org/10.4103/jfcm.JFCM_97_17 [ Links ]
 Correspondence:
Correspondence:
M Tun
drmyinttun@outlook.com
Accepted 21 September 2022

