










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 n.11b Pretoria Nov. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i11b.16835
RESEARCH
Profile of burn patients at Mankweng Hospital, Polokwane, Limpopos Province, South Africa
L M Leso-RangwatoI; M M Z U BhuiyanII; T T NetshiongolweIII
IMB ChB; Department of General Surgery, Limpopo Academic Health Complex and School of Medicine, University of Limpopo, Polokwane, South Africa
IIPRCS (Glasg), MMed (Surg) ; Department of General Surgery, Limpopo Academic Health Complex and School of Medicine, University of Limpopo, Polokwane, South Africa
IIIMMed (Plast Surg), FC Plast Surg (SA); Department of Plastic and Reconstructive Surgery, Limpopo Academic Health Complex and School of Medicine, University of Limpopo, Polokwane, South Africa
ABSTRACT
BACKGROUND. Burn injuries are a common cause of preventable morbidity and mortality. In all societies, burns continue to constitute a medical, psychological and economic problem. Burn wounds are one of the most common surgical emergencies leading to hospitalisation.
OBJECTIVES. To understand the profile of patients with burn injuries presenting to Mankweng Hospital in Polokwane, Limpopo Province, South Africa.
METHODS. This was a retrospective study using a descriptive quantitative design to analyse the profile of all patients admitted consecutively to the Mankweng Hospital burns unit from 1 January 2018 to 31 December 2020.
RESULTS. During the study period, a majority of males (n=412; 56.7%) were admitted, indicating a significant sex difference.
CONCLUSION. Children aged <5 years were found to be more affected than any other age group. Males were more affected than their female counterparts. Scalds and flame burns were the most common burn injuries.
Burn injuries are a common cause of preventable morbidity and mortality.[1-4] In all societies, burns continue to constitute a medical, psychological and economic problem.[5] Burns are one of the most common surgical emergencies leading to hospitalisation.[6] Burns are not only life-threatening emergencies, but also have long-term effects.[6,7] Apart from physical consequences that are functionally important, cosmetic and psychological factors also play a significant role, and patients with extensive burns are likely to suffer long-term effects of this trauma.[6] The severity of burn injury varies from mild to severe, depending on the cause and the duration of exposure to the inciting agent.[2] In scald burn injuries, the temperature of the injuring agent determines the severity of the injury.[2] Other types of burn injuries include flame, chemical and electrical burns. Scald and flame burns are the most common types of burns.[6] Scald burns constitute the majority of cases (71.1%), with 53% attributable to hot liquids related to cooking, including coffee and tea.[1] As unintentional burn injuries account for the majority of morbidity in the paediatric population,[1,3,7] prevention of burns is crucial.[2] Treatment of burns should be focused on wound care to prevent infection and minimise further fluid loss,[2] and a multidisciplinary team forms an integral part of managing patients with burn injuries to achieve optimal outcomes.
The burns unit at Mankweng Hospital in Polokwane serves as the only referral unit for burn patients in the remote province of Limpopo in South Africa, serving a population of ~6 million people. The province has five districts, namely Capricorn, Vhembe, Mopani, Sekhukhune and Waterberg, and patients are referred from all these districts to our centre. The burns unit has a total capacity of only 19 beds (8 paediatric beds, 4 female beds, 3 male beds and 4 high-care beds), and patients from all districts have to share this limited number of beds.
There is a paucity of information on the profile of patients with burn injuries presenting to Mankweng Hospital. The main objective of this study was to understand this profile, including determination of: (i) the most common mechanism of burns; (ii) the most affected gender; (iii) the age group most commonly affected by burns; and (iv) the peak burns season. We hope that the results presented will enable healthcare professionals to adequately allocate resources to improve the management of patients with burn injuries in Limpopo. In addition, we hope that the results will educate clinicians in referral hospitals and people in the communities to be aware of the most common causes of burn injuries, so that the communities can form part of both prevention and early intervention strategies to tackle the scourge of these injuries. Awareness will enable the hospital staff to better manage and allocate the limited bed spaces available.
Methods
This was a retrospective study using a descriptive quantitative design to analyse the profile of all patients admitted consecutively to the Mankweng Hospital burns unit over the 3-year period 1 January 2018 - 31 December 2020. The data were collected by scrutinising the admission books for all patients admitted to our unit as a study frame. Patients who were seen and treated in and discharged from the accident and emergency unit, as well as those who were admitted to wards other than the burns unit, were excluded from the study. The data collected were documented in a data collection sheet comprising gender, the mechanisms of burn injuries, age at the time of injury, seasonal variations, total body surface area (TBSA) of burn, and burn injuries from each district in Limpopo as variables of the study. A total of 726 patients were included. Data were analysed using descriptive and inferential statistics. Descriptive statistics entailed measures of central tendencies and means, frequencies and percentages, and inferential statistics applied one-way analysis of variance with an F-test to assess the level of significance in the number of patients with burn injuries over the 3-year period. A p-value of 0.05 was used to test the level of significance. The Statistical Package for the Social Sciences (SPSS) version 28.0 (IBM Corp., USA) was used for data analysis.
Ethical approval was obtained from the Pietersburg-Mankweng Research Ethics Committee (ref. no. PMREC 17 FEBRUARY 2021/A) and the provincial Department of Health (ref. no. LP_2021-03-007).
Results
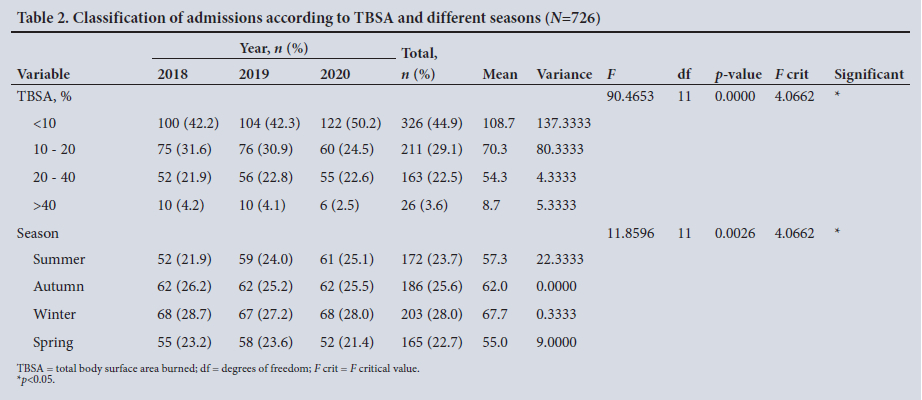
Detailed results of the study are reflected in Tables 1, 2 and 3. A total of 726 patients were admitted to the burns unit over the 3-year study period. During this period, 237 patients were admitted in 2018, 246 in 2019 and 243 in 2020, indicating a consistent average yearly admission rate. The majority of patients admitted were male (n=412 (56.7%), v. n=314 (43.3%) female) (Table 1), the results indicating a significant difference (F=46.62; p=0.0024<0.05). Of the patients, 472 (65.0%) were discharged and 174 (24.0%) were stepped down to other wards with the aim of creating more bed availability in the burns unit. Patients who were stepped down were those who had minor burn injuries, those who were healing well, and those waiting to be discharged who were subsequently discharged. The results further showed that 68 patients (9.4%) died, 11 (1.5%) signed RHT (refusal of hospital treatment) and 1 (0.1%) absconded. There was a significant difference in outcome between patients who were discharged, died, stepped down to other wards, signed RHT and absconded. The majority of patients were discharged compared with other outcomes (F=384.05; p<0.0001). Of the patients admitted, 361 (49.7%) were from Capricorn district, 111 (15.3%) from Vhembe, 93 (12.8%) from Waterberg, 81 (11.2%) from Sekhukhune and 78 (10.7%) from Mopani, while 2 patients (0.3%) were transferred from Mpumalanga Province (Table 1). The majority of the patients were from Capricorn district, with an average over the study period that differed significantly from the other districts (F=189.45; p<0.0001). Most of the burn patients admitted were aged 1 - 5 years (n=336; 46.3%) (Table 1). Hot water was the the most common mechanism of burn injury (61.4%), followed by open fire burns at 22.9% (Table 3). Most burns (44.9%) involved <10% of TBSA, which differed significantly from other categories (F=90.46; p<0.0001) (Table 2). Seasonal variations were observed, with most admissions of burn patients (28.0%) in winter, which differed significantly from the other seasons (F=11.85; p=0.0026), and the lowest number of admissions in spring (22.7%) (Table 2).
Discussion
This 3-year retrospective, consecutive study analysed data from all patients admitted to our burns unit from 1 January 2018 to 31 December 2020. During this period, the unit treated a total of 726 acutely burned patients, with no significant variation between the years: 237 patients were admitted in 2018, 246 in 2019 and 243 in 2020. Males were more affected than females (n=412; 56.7% v. n=314; 43.3%, respectively), which is a significant difference (p=0.0024<0.05). This finding is in contrast to a study by Hemeda et al.[5] in Egypt, in which females (53.1%) were found to be more vulnerable to burns than males (46.8%), but is in line with other studies that found males to be more commonly affected than females in all age groups (p<0.0001).[3,7] There were seasonal variations, with a peak of burn admissions during winter that significantly differed from the other seasons (p=0.0026<0.05). We assume that this peak was due to an increased need for hot water in winter and more fires burning to keep the household warm. Other studies have also found seasonal variations with peaks in winter.[3,5,6,8] The literature indicates that most burns of females occurred in the home (mostly housewives and female children), while most males sustained burns at outdoor locations.[3-5] A study by Fernandes-Morales et al.[9] in Spain found that 65.8% of burn accidents occurred in the home. Children were mainly reported to be victims of scalds and flame burns.[3.5,6] In the present study, the most commonly affected age group was 1 - 5 years. Almost half of the total number of patients fell into this age group (n=336; 46.3%), a significant difference (p<0.0001). In keeping with our observation, Frans et al[6] reported that most burned patients in their study were in the age group 0 - 4 years. Lee et al.[1] found that 73.2% of all burn patients were between the ages of 0 and 6 years. In younger children, a 'bib pattern' burn distribution is sustained when the child pulls a container of hot liquid down from a higher surfaced3,4,5-Institution of preventive measures is therefore very important. Some of the steps that can be taken to prevent these injuries are setting the hot water heater to a maximum of 49°C to limit scald injuries from bathing, and keeping children out of the kitchen while cooking, microwaving or using the oven.[2]
Scalds and flame burns were the burn injuries most commonly seen in the Mankweng Hospital burns unit, accounting for a significant 70.8% and 22.9%, respectively (p<0.0001). In line with this observation, Lee et al.[1] reported figures of 71.1% for scalds and 20.8% for flame burns, while Frans et al.[6] found that the most common cause of burns was scalds (47.9%), followed by flame (22.3%). Among all the scald burns in the present study, the most common cause was hot water (61.4%). Hemeda et al.[5] and Sahu et al.[3] found that scalds were mostly associated with partial (36.8%) rather than full-thickness (10%) injuries.[5] Flame burns may result from household fires or fires from a motor vehicle accident. Lee et al.[1] found that in the teenage group, flame burns were the most common (53.8%). Data from hospitalised burn patients worldwide reveal incidence rates for assault by fire and scalds ranging from 3% to 10%.[10]
Most of the burn injuries in the present study had a positive outcome, with a significant 646 eventual hospital discharges (89.0%), but our mortality rate was 9.4%. The proportions of patients who were discharged and who died differed significantly over the study period (p<0.0001). The results further indicated that 44.9% of patients admitted had sustained minor burn injuries involving <10% of TBSA, which was associated with positive outcomes and reduced length of hospital stay. The reason for admitting such patients was the admission criteria adopted from the American Burn Association.[11] These outcomes are comparable with the study by Frans et al.,[6] in which 42.4% of the patients had burns involving <10% of TBSA. Shields et al}7] found that 66.5% of burn injuries were <10% TBSA, whereas Hemeda et al.[5] found that the most common TBSA was 25 - 59%.[5] Peck et al.[10] found that the average proportion of TBSA burned in an assault by fire or scalds was ~20%. In US burn centres from 1999 to 2008, 2% of admissions were due to assault by burning (including child abuse), and <1% due to self-harm or attempted suicide.[10,12] The distribution of burn injuries according to district in Limpopo showed that Capricorn had the most admissions (n=361; 49.7%), which differed significantly from other districts in the province (Vhembe n=111 (15.3%), Waterberg n=93 (12.8%), Sekhukhune n=81 (11.2%), Mopani n=78 (10.7%), and transfers from Mpumalanga n=2 (0.3%)) (p<0.0001). The most likely reason for the finding that Capricorn district had the largest number of admissions is that Mankweng Hospital is located in Capricorn, and most of these patients would have arrived as self-referrals.
Conclusion
Burn injuries are one of the most common surgical emergencies in Limpopo. Children aged <5 years were found to be affected more than any of the other age groups. Males were more affected than their female counterparts. Scalds and flame burns were the most common burn injuries. There were seasonal variations, with burn admissions peaking in winter, followed by autumn.
This study was the first to determine the epidemiology of burn injuries in Limpopo. The results and findings will provide a basis for recommendations to the Department of Health to educate the communities about burns, especially scald and flame burns, and preventive measures to reduce the frequency of burns and burn-related deaths.
Declaration. None.
Acknowledgements. The authors thank Ms Livhuwani (Mphaphuli) Nedzingahe, chartered statistician, for her contribution to the statistical analysis.
Author contributions. Data gathering and literature search: LML-R, MMZUB, TTN; study design: LML-R, MMZUB, TTN; obtaining ethical approval: MMZUB; initial writing of manuscript: LML-R; final writing and editing: MMZUB, TTN.
Funding. None.
Conflicts of interest. None.
References
1. Lee CJ, Mahendraraj K, Houng A, et al. Pediatric burns: A single institution retrospective review of incidence, etiology, and outcomes in 2273 burn patients (1995 - 2013). J Burn Care Res 2016;37(6):e579-e585. https://doi.org/10.1097/BCR.0000000000000362 [ Links ]
2. Yin S. Chemical and common burns in children. Clin Pediatr (Phila) 2017;56(5_suppl):8S-12S. https://doi.org/10.1177/0009922817706975 [ Links ]
3. Sahu SA, Agrawal K, Patel PK. Scald burn, a preventable injury: Analysis of 4306 patients from a major tertiary care center. Burns 2016;42(8):1844-1849. https://doi.org/10.1016/j.burns.2016.06.022 [ Links ]
4. Strobel AM, Fey R. Emergency care of pediatric burns. Emerg Med Clin North Am 2018;36(2):441-458. https://doi.org/10.1016/j.emc.2017.12.011 [ Links ]
5. Hemeda M, Maher A, Mabrouk A. Epidemiology of burns admitted to Ain Shams University Burns Unit, Cairo, Egypt. Burns 2003;29(4):353-358. https://doi.org/10.1016/s0305-4179(03)00044-5 [ Links ]
6. Frans FA, Keli SO, Maduro AE. The epidemiology of burns in a medical center in the Caribbean. Burns 2008;34(8):1142-1148. https://doi.org/10.1016/j.burns.2008.05.013 [ Links ]
7. Shields BJ, Comstock RD, Fernandez SA, Xiang H, Smith GA. Healthcare resource utilisation and epidemiology of pediatric burn-associated hospitalisations, United States, 2000. J Burn Care Res 2007;28(6):811-826. https://doi.org/10.1097/BCR.0b013e3181599b51 [ Links ]
8. El-Badawy A, Mabrouk AR. Epidemiology of childhood burns in the burn unit of Ain Shams University in Cairo, Egypt. Burns 1998;24(8):728-732. https://doi.org/10.1016/S0305-4179(98)00097-7 [ Links ]
9. Fernández-Morales E, Gálvez-Alcaraz L, Fernández-Crehuet-Navajas J, Gómez-Gracia E, Salinas-Martínez JM. Epidemiology of burns in Malaga, Spain. Burns 1997;23(4):323-332. https://doi.org/10.1016/S0305-4179(96)00136-2 [ Links ]
10. Peck MD. Epidemiology of burns throughout the world. Part II: intentional burns in adults. Burns 2012;38(5):630-637. https://doi.org/10.1016/j.burns.2011.12.028 [ Links ]
11. American Burn Association. Burn center referral criteria. http://ameriburn.org/public-resources/burn-center-referral-criteria/ (accessed 16 June 2022). [ Links ]
12. American Burn Association. National Burn Repository: Report of data from 1999 - 2008. Version 5.0. Chicago, Ill.: ABA, 2009. [ Links ]
 Correspondence:
Correspondence:
M Bhuiyan
bhuiyanmirza@gmail.com
Accepted 19 September 2022


{kind=link}
{kind=link}
{kind=link}