










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.8 Pretoria Ago. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i8.16695
EDITORIAL
https://doi.org/10.7196/samj.2022.v112i8.16695
A third-line antiretroviral therapy register to track patient clinical and virological outcomes
In 2021, South Africa (SA) had an estimated 7.8 million people living with HIV, of whom 5.6 million were receiving antiretroviral therapy (ART),[1] with 3.4 million on first-line ART, 145 000 on second-line ART (SLART) and >700 on third-line ART (TLART).[2,3] Access to TLART in SA's public healthcare sector is available to patients with confirmed virological failure on a second-line protease inhibitor (PI) regimen and documented PI resistance, defined as a genotype resistance Stanford score >15.[4] TLART access is managed nationally through expert clinical review committees that operate virtually via email consensus.[2] The TLART committees are responsible for recommending an individualised TLART regimen based on the patient's clinical history and genotype resistance profile (TLART National Secretary, personal communication, 12 June 2022). The recommendation goes to the applicant and facility's pharmacist, who then procures the relevant medicine(s).
In resource-limited public sector settings, the options for salvage therapy and last-resort options for patients failing SLART are extremely limited. Published data emanating from SA estimate that ~25% of the ~145 000 people receiving SLART experience treatment failure within 1 year as a result of treatment non-adherence, subtherapeutic ART, delayed switching, and accumulation of PI-resistant mutations.[2,5,6] Although these data are from the pre-dolutegravir (DTG) era, the growing pool of patients urgently needing TLART requires innovative systems to ensure that patients receiving TLART are alive, engaged in care, and virologically suppressed for the duration of their treatment.
The estimated annual cost for TLART is ~ZAR16 486 per patient for a commonly used regimen such as darunavir with ritonavir, DTG and two nucleoside reverse transcriptase inhibitors, considerably higher than first-line (tenofovir, emtricitabine and efavirenz or tenofovir, lamivudine and dolutegravir) and second-line ART (zidovudine, lamivudine, and lopinavir or atazanavir boosted with ritonavir) at ZAR1 649 and ZAR13 140 per patient per year, respectively.[7]
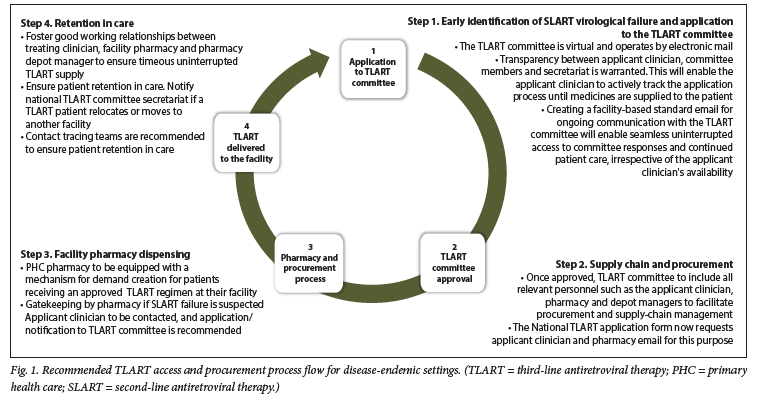
Owing to the substantially higher costs of second- and third-line regimens compared with first-line ART, targeted interventions to boost engagement and retention of TLART patients in health facilities will help to ensure that the goals of AIDS-free survival through ART access are met. Recommendations to improve current TLART access and procurement processes include early identification of SLART failure with an application to the TLART committee for consideration, implementation of optimised systems for TLART procurement and supply-chain management, enabling facility pharmacy dispensing of TLART, and systems to ensure long-term retention in care (Fig. 1). A confidential named-patient register maintained at facility, district, provincial and national levels may be an important administrative tool to potentially strengthen TLART care and complement the work of a holistic HIV care team. A TLART registry should be a systematic collection of patient demographic information, clinical parameters at initiation of TLART, treatment regimens and therapy escalation, and outcomes (e.g. virological, immune response and clinical outcomes), monitored and recorded at regular intervals through clinical audits (Table 1).
Ideally the TLART register would serve as a customised database to enhance tracking of patients initiated on TLART, their retention in care, and updates on their clinical outcomes. Initial data for the register could be accessed from the TLART application package, which would offer a collated clinical and virological summary by the treating clinician. Register maintenance should be done at least monthly at a single point in the process, preferably managed by the district pharmacist in collaboration with the facility, as all the patients will feed through this unit.
Maintenance would include when the TLART application was made, recommendation received, when the patient received their medication, and status of the patient. Certain outcome measures such as reporting of adverse drug reactions and therapy escalation with accompanying reason could also assist with overall pharmacovigilance. All relevant personnel involved in the patient's TLART management, including the treating clinician, the TLART secretariat and pharmaceutical services, should ideally have login access to the register/database. Register records could ultimately be compared with pharmaceutical depot records for consolidation of patient numbers, future forecasting needs, and input into the provincial budget.
Globally, the use of patient-centred registries has become increasingly adopted in treatment programmes for cancer, cardiovascular disease, diabetes and autoimmune diseases in developed countries, to monitor patient progress and outcomes.[8] Advantages stemming from patient registries include timeous up-referral, real-time clinical monitoring and immediate medical action, all contributing to improved clinical outcome. The major disadvantage of any type of registry is maintenance, audits and quality checks to ensure that the most accurate and up-to-date information is available.
The adoption of a TLART register by geographical area could map movement of patients within facilities and promote retention-in-care strategies to ensure ongoing engagement of TLART patients through outreach support. Comparing baseline clinical information with current viral load, by treatment regimen, would provide useful clinical information on effectiveness of TLART regimens for these patients, and offer a triage mechanism when more effective drugs or regimens become available. A third-line register has the potential to strengthen planning and provision of TLART in relation to treatment stockouts, provider/supply-chain challenges, or patient challenges such as frequent pill pick-up delays, to ensure optimal use of resources. The future of registries will be shaped by technological advances, and linking a TLART register/database to other electronic data sources, such as prescription and laboratory services, would reduce the need for intensive chart audits and provide the opportunity for real-time decision-making for this vulnerable group of patients. The register then becomes a quality improvement register, where patient outcomes are tracked for feedback to experts to provide efficient input on management of TLART patients.
With almost two decades of ART programmatic roll-out, an escalating burden of PI resistance and a fast-growing number of patients accessing TLART, innovative strategies to manage TLART better and mitigate the risk of HIV drug resistance are warranted in sub-Saharan Africa. Developing and maintaining a TLART register will complement patient services and help promote clinical governance to establish a process of accountability and excellence in HIV clinical care.
Kogieleum Naidoo
Centre for the AIDS Programme of Research in South Africa (CAPRISA), Durban, South Africa; MRC-CAPRISA HIV-TB Pathogenesis and Treatment Research Unit, Doris Duke Medical Research Institute, University of KwaZulu-Natal, Durban, South Africa. kogie.naidoo@caprisa.org
Jenine Ramruthan
Centre for the AIDS Programme of Research in South Africa (CAPRISA), Durban, South Africa
Millidhashni Reddy
Essential Medicine Consulting, Durban, South Africa
Ruth Lancaster
Essential Drugs Programme, Affordable Medicines Directorate, National Department of Health, Pretoria, South Africa
References
1. Joint United Nations Programme on HIV/AIDS (UNAIDS). Global HIV & AIDS statistics - fact sheet 2021. https://www.unaids.org/en/resources/fact-sheet#:~:text=GLOBAL%20HIV%20STATISTICS,infected%20with%20HIV%20in%202020 (accessed 13 July 2022). [ Links ]
2. Moorhouse M, Maartens G, Venter WDF, et al. Third-line antiretroviral therapy program in the South African public sector: Cohort description and virological outcomes. J Acquir Immune Defic Syndr 2019;80(1):73-78. https://doi.org/10.1097/QAI.0000000000001883 [ Links ]
3. Venter W, Kaiser B, Pillay Y, et al. Cutting the cost of South African antiretroviral therapy using newer, safer drugs. S Afr Med J 2017;107(1):28-30. https://doi.org/10.7196/SAMJ.2016.v107.i1.12058 [ Links ]
4. National Department of Health, South Africa. National consolidated guidelines for the management of HIV in adults, adolescents, children and infants and prevention of mother-to-child transmission. 2020. https://www.knowledgehub.org.za/elibrary/national-consolidated-guidelines-management-hiv-adults-adolescents-children-and-infants (accessed 13 July 2022). [ Links ]
5. Fox MP, Berhanu R, Steegen K, et al. Intensive adherence counselling for HIV-infected individuals failing second-line antiretroviral therapy in Johannesburg, South Africa. Trop Med Int Health 2016;21(9):1131-1137. https://doi.org/10.1111/tmi.12741 [ Links ]
6. Kouamou V, Manasa J, Katzenstein D, McGregor AM, Ndhlovu CE, Makadzange AT. Drug resistance and optimizing dolutegravir regimens for adolescents and young adults failing antiretroviral therapy. AIDS 2019;33(11):1729-1737. https://doi.org/10.1097/QAD.0000000000002284 [ Links ]
7. National Department of Health, South Africa. Master Health Product List, January 2019. https://www.health.gov.za/tenders/ (current version, 1 July 2022). [ Links ]
8. Gliklich RE, Dreyer NA, Leavy MB, eds. Registries for evaluating patient outcomes: A user's guide. 3rd ed. Rockville, Md.: Agency for Healthcare Research and Quality, 2014. Report No. 13(14)-EHC111. PMID: 24945055. [ Links ]


{kind=link}
{kind=link}