










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.7 Pretoria Jul. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i7.16258
RESEARCH
Treating urinary tract infections in public sector primary healthcare facilities in Cape Town, South Africa: A pharmaceutical perspective
N KeulerI; Y JohnsonII; R CoetzeeIII
IB Pharm, MClinPharm; School of Pharmacy, University of the Western Cape, Cape Town, South Africa
IIBPharm, MPH; Western Cape Government Health, Cape Town, South Africa
IIIMPharm, PharmD; School of Public Health, University of the Western Cape, Cape Town, South Africa
ABSTRACT
BACKGROUND: Antibiotic resistance is a global healthcare burden complicating the management of infections. Urinary tract infections (UTIs) are commonly treated in primary care. Managing UTIs appropriately in primary care can combat antibiotic resistance. The treatment practices for UTIs in primary care in Western Cape Province, South Africa, are not well described
OBJECTIVES: To describe treatment of UTIs in adults in primary care in the Cape Town metropole public sector of the Western Cape
METHOD: A retrospective multicentre medical records review of patients diagnosed with UTIs was conducted during 1 October 2020 -28 February 2021. Six public sector primary healthcare facilities were included in the study through random selection from three of the four substructures in the Cape Town metropole. Medical records of adult patients diagnosed with UTIs, through clinical diagnosis or microbiological testing, were identified via a selective sampling process. Data were collected from medical records using a standardised data collection tool
RESULTS: A total of 401 UTI episodes occurred in 383 patients during the study period. The majority of UTI episodes (84.3%) occurred in females, complicated UTIs (74.1%) were more common than uncomplicated UTIs, and nitrofurantoin (57.1%) was frequently prescribed, followed by ciprofloxacin (39.7%). Compliance with urine microscopy recommendations was low (6.7%), and antibiotics were appropriately selected in 75.0% of uncomplicated and 70.0% of complicated UTI episodes
CONCLUSION: Interventions are required to improve compliance with treatment recommendations as per the standard treatment guidelines, especially when selecting the appropriate antibiotic, duration of therapy and urine microscopy
Antibiotic resistance is one of the greatest global healthcare threats the world is facing.[1] Failure to respond with appropriate action may lead to a post-antibiotic era in which ordinary infections will be untreatable.[2] Irrational prescribing is one of the factors fuelling antibiotic resistance.[3,4] Approximately 80% of antibiotic prescribing occurs in the primary healthcare setting,[5] where almost 30% of prescribed antibiotics are unnecessary.[6] Antibiotic stewardship programmes have been identified as a key strategy to optimise antibiotic use in an attempt to reduce antibiotic resistance at both hospital and community level.[7] Low- and middle-income countries face various challenges to successfully implement antibiotic stewardship programmes.[8] Implementation of stewardship programmes in primary care in South Africa (SA) is still developing.[9,10] The Antimicrobial Resistance National Strategy Framework 2014 - 2024 was developed to support antibiotic stewardship in SA.[11]
In the Western Cape Province primary care setting at the time of the study, prescribing was guided by the 2018 Primary Healthcare Standard Treatment Guidelines and Essential Medicines List (PHC EML 2018).[12] In a study conducted by Gasson et al.,[13] adherence to the Standard Treatment Guidelines (STGs) for infections in primary care (2014 edition) was investigated. Urological infections accounted for 7.5% of infections, and compliance with primary care guidelines for treating urological infections was the lowest. In terms of treating urological infections, the duration of antibiotic therapy and antibiotic selection were inappropriate in 51.2% and 17.1% of the cases, respectively. Adherence to guideline recommendations for ciprofloxacin prescribing was poor.[13] Urinary tract infections (UTIs) are among the most commonly treated primary healthcare conditions requiring antibiotic therapy,[14,15] which may increase the healthcare burden as antibiotic resistance increases.[16] UTIs affect a patient's quality of life, and the sequelae of UTI complications may include urosepsis, recurrence, pyelonephritis, sepsis, renal damage, bacteraemia, preterm birth, and even Clostridioides difficile infections.[17,18] If asymptomatic bacteriuria in pregnancy remains untreated, it may lead to pyelonephritis, preterm birth and low birthweight.[19,20] The goals of UTI treatment are to eradicate the infection and prevent complications and recurrence, as well as limiting antibiotic resistance.[21]
Practising antibiotic stewardship in primary care can optimise patient health outcomes and reduce antibiotic resistance. Appropriate empirical therapy is vital to ensure treatment success and to prevent complications; however, antibiotics should be considered carefully in view of the current antibiotic resistance dilemma.[22,23] Local antimicrobial susceptibility patterns will assist in guiding empirical therapy for UTIs in the emerging setting of resistance.[22] A few surveillance studies have been conducted in SA,[22,24-26] and it is evident that surveillance data are area specific and that continuous monitoring is needed to recommend appropriate empirical therapy. Surveillance data in the Western Cape could guide prescription of the appropriate antibiotic therapy for treating UTIs. Classifying UTI in terms of complicated and uncomplicated infections requires standardisation[27] to promote rational antibiotic use and to optimise patient health outcomes.
Various communications[28,29] on the potential risks of fluoroquinolones led to the National Department of Health (NDoH) amending the STGs for UTIs in 2019, recommending that ciprofloxacin should not be used for uncomplicated UTIs (Circular H53/2019[30]). To our knowledge, treating UTIs and prescribing practices in the primary care setting of the Western Cape public sector has not been described.
The objectives of this study were to describe how UTIs are treated in primary healthcare and to determine compliance with current local guidelines.
Methods
Study design and setting
A retrospective multicentre medical records review of patients with UTIs was conducted in the primary healthcare setting of the Western Cape public sector for the period 1 October 2020 - 28 February 2021.
Study population and sampling
Adult outpatients (>18 years of age) diagnosed with UTIs, either clinically or with microbiological confirmation, at community day centres (CDCs) or community healthcare centres (CHCs) in the Cape metropole were included. These facilities were identified through a random selection process using Excel 2016 (Microsoft Corp., USA) to identify two facilities per substructure from the following three substructures in the Cape metropole: Northern/ Tygerberg, Klipfontein/Mitchell's Plain and Eastern/Khayelitsha. The fourth substructure had to be excluded owing to different operating procedures. For anonymity, the data presented in the manuscript would not be presented according to the substructures' specific names.
A prevalence was set at 50% to calculate the sample size.[31] Medical records were identified through a selective sampling process following a pragmatic approach. Pharmacists daily identified all folders of adult patients who presented with UTIs. Data were collected by the researcher (NK) on a continuous basis until a minimum of 100 records per substructure or a total of 400 records had been reviewed. Patients who were referred to a higher level of care were excluded from the study.
Collecting and analysing data
A data collection tool was designed by the research pharmacists and a physician to collect the following data from patient medical records: demographics, diagnosis, results of diagnostic investigations, antibiotic regimen prescribed, concurrent conditions, concurrent medicines prescribed, and dispensing data. The PHC EML 2018[12] and Circular H53/2019[30] were used to inform on the criteria for the data collection tool. To test the data collection tool and study process, a pilot study was conducted using 10 patient folders from a facility not included here. The pilot study followed the same procedures. Data were analysed using descriptive statistics and MS Excel 2016 (Microsoft Corp., USA).
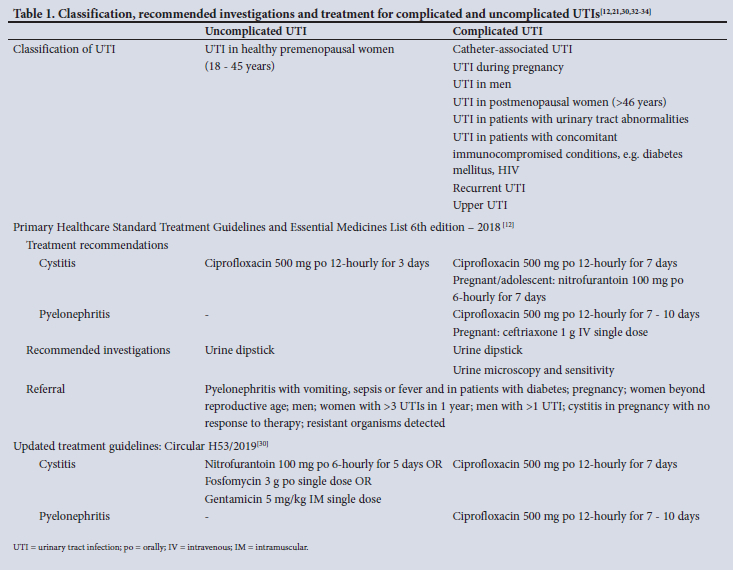
Current guidelines in place at the time of the study were used to assess appropriate management of UTIs, i.e. the PHC EML 2018[12] and Circular H53/2019,[30] which provided updated antibiotic treatment recommendations after notification of ciprofloxacin safety warnings. At primary healthcare level, it is expected that management of UTIs should predominantly conform to STGs.
Classification of UTIs is not clear in the literature, and for the purpose of this study, UTIs were categorised into complicated and uncomplicated infections based on national and international guidelines. [12,21,32,33] Table 1 provides a summary of the classification, recommended investigations and treatment of complicated and uncomplicated UTIs. UTIs in healthy, premenopausal, non-pregnant females (18 - 45 years of age) were categorised as uncomplicated, and all other UTIs were categorised as complicated.[21]
Ethical considerations
Approval was granted by the University of the Western Cape's Biomedical Research Ethics Committee (ref. no. BM20/5/17) and Western Cape Government Health (ref. no. WC_202006_038). This was a retrospective medical record review and data were anonymised before analysis, so no informed consent was required from patients.
Results
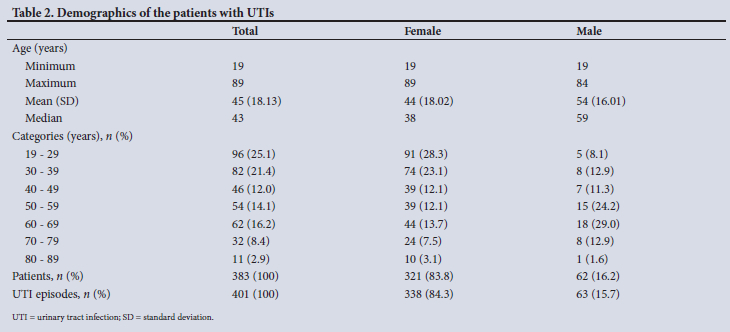
A total of 401 UTI episodes from 383 patients were reviewed from six primary care facilities across three substructures in the Cape metropole. Facilities comprised CDCs (n=5/6; 83.3%; 323 UTI episodes, 80.5%) and CHCs (n=1/6; 16.7%; 78 UTI episodes; 19.5%). The majority of UTI episodes occurred in females (n=338/401; 84.3%). Seventy-five pregnant women (n=75/321; 23.4%) presented with 84 UTI episodes during the study period. In terms of age, UTIs occurred more frequently in younger premenopausal women (18 - 39 years age category) compared with men (50 - 69 years age category). Table 2 provides more details.
Fifty-two patients (n=52/383; 13.6%), 44 females and 8 males, had been exposed to an antibiotic during the preceding 90 days. Penicillin (41.1%), nitrofurantoin (20.5%) and ciprofloxacin (19.2%) were the most common antibiotics patients had been exposed to previously.
Allergy status was reported in the majority of patient folders (88.3%). Hypertension (37.6%) and diabetes mellitus (16.7%) were common comorbid conditions. Analgesics were the most frequent medicines prescribed concurrently (Table 3). The study included 8 wheelchair-bound patients (2.1%), 1 patient with tetraplegia due to a spinal injury (0.3%), and 5 patients with a catheter (1.3%). A urine alkaliser was prescribed in 53 UTI episodes and concurrently with ciprofloxacin in 22 episodes.

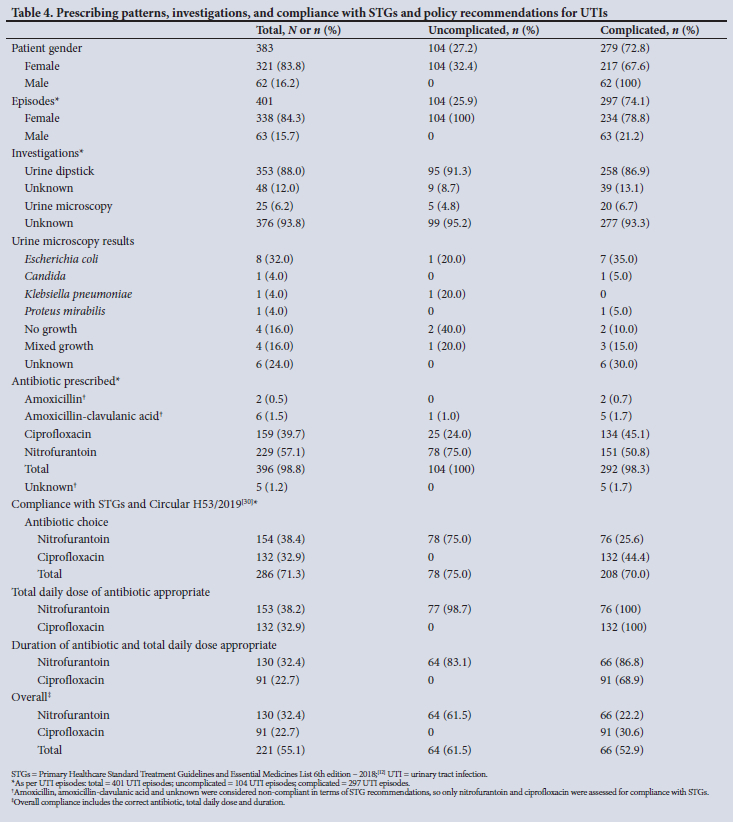
The majority of UTI episodes occurred in females (84.3%), and 74.1% of all episodes were complicated. Antibiotics were prescribed in all male and 98.5% of female episodes, and in all uncomplicated episodes and in 98.3% of complicated episodes. Of the 729 nitrofurantoin issues recorded on the electronic dispensing system during the study period, 229 nitrofurantoin prescriptions from patient records were reviewed. Similarly, 4 fosfomycin issues were recorded; however, no prescriptions were reviewed for the study period. Nitrofurantoin was prescribed in the majority of UTI episodes (57.1%), followed by ciprofloxacin (39.7%). Nitrofurantoin was more frequently prescribed in uncomplicated (75.0%) than complicated (50.8%) UTI episodes, and in episodes in women (63.9%). Ciprofloxacin was mostly prescribed in episodes in men (79.4%) and in complicated episodes (45.1%). A urine dipstick test was performed in the majority of episodes (88.0%), while urine microscopy was conducted in only 6.7% of complicated episodes. In terms of complying with STG recommendations, nitrofurantoin was appropriately selected in 75.0% of uncomplicated episodes. However, for complicated UTIs, compliance in terms of antibiotic choice was better for ciprofloxacin (44.4%) than for nitrofurantoin (25.6%). An appropriate total daily dose of the selected antibiotic was ordered for ~99% of prescriptions of nitrofurantoin and ciprofloxacin, while appropriate duration of antibiotic with correct total daily dose were lower. In complicated UTIs, appropriate duration of antibiotic and total daily dose were lowest for ciprofloxacin (68.9%). Overall compliance in prescribing was greater for uncomplicated UTIs (61.5%) than for complicated UTIs (52.9%). Overall compliance in uncomplicated UTIs was greater with nitrofurantoin, but for complicated UTIs, compliance was greater with ciprofloxacin. Failure to comply with STG recommendations was mostly due to inappropriate antibiotic selection for complicated UTIs and duration of therapy (Table 4).
Four females were diagnosed with asymptomatic bacteriuria. Of these, two pregnant women were treated with antibiotics, amoxicillin-clavulanic acid and nitrofurantoin; an elderly patient with diabetes was treated with ciprofloxacin; and choice of antibiotics was unknown in one patient. Eighteen recurrent UTI episodes occurred in 17 patients during the 5-month study period. Fifteen women and one man experienced two UTI episodes, and one woman experienced three episodes. Urine microscopy was only conducted in three recurrent episodes. Nitrofurantoin was mostly prescribed in the first (70.6%) and second (58.8%) episodes.
Twenty-five urine samples were sent for urine microscopy and culture sensitivity analysis, with Escherichia coli being the most common organism identified (32.0%). It was unknown whether urine microscopy was conducted in 93.3% of complicated UTI episodes.
Discussion
We aimed to describe treatment of UTIs at primary healthcare level and to determine compliance with STG recommendations. This pragmatic study provides novel information and a broad overview on the treatment of UTIs at primary healthcare level in the Western Cape metropole public sector. Areas for improvement to optimise compliance with local guidelines and rational antibiotic use were identified.
According to the Pharmacy Information System, electronic data indicated that 729 prescriptions of nitrofurantoin and 4 prescriptions of fosfomycin were dispensed over the study period for all six facilities. This study had a good representative sample, including approximately a third (n=229/729; 31.4%) of nitrofurantoin prescriptions.
In previous SA studies,[22,24-26] E. coli was the most common causative organism (54.2 - 79.6%). Although urine cultures could only be analysed for 11 of our urine samples, E. coli was the most common organism detected (32.0%).
According to Wattengel et al.,[35] prescription of antibiotics for UTIs was suboptimal. Their retrospective analysis showed that 68% of patients treated for UTIs were treated inappropriately. Incorrect duration (50.9%) was the most common error, followed by inappropriate choice of antibiotics (35.1%) and incorrect dosing (12.4%).[35] An SA study by Gasson et al.[13] found that the duration of therapy was most often inappropriate (in 51.2% of urological infections), with inappropriate antibiotic selection in 17.1% of infections. The present study showed greater compliance in terms of overall antibiotic selection; however, antibiotic selection for treating complicated UTIs was mostly inappropriate, which was concerning in view of UTI complications and antibiotic resistance. Similar to the findings of Gasson et al.,[13] compliance with guideline recommendations for ciprofloxacin was poor. With regard to total daily dose of appropriately selected antibiotics, compliance was very high (98.7 - 100%); however, compliance was not as good for duration of treatment with appropriate antibiotics selected and total daily dose. Overall, compliance with STG recommendations was poor.
In a 2008 study by Bosch et al.[22] in Bloemfontein, the most common antibiotic prescribed for uncomplicated UTIs was found to be amoxicillin-clavulanic acid (36%), while ciprofloxacin was most commonly prescribed for complicated UTIs. In a Gauteng study conducted in 2011,[26] ciprofloxacin was the most common antibiotic prescribed (50.3%). The REWIND study,[36] conducted in Brazil, Belgium, Italy and Russia during 2016 - 2017, found that fosfomycin (21.6 - 39.7%) was the most common antibiotic prescribed, followed by ciprofloxacin (9.6 - 24.6%). In the present study, nitrofurantoin and ciprofloxacin were frequently prescribed. It is evident that antibiotic treatment selection varies, and it is therefore important to survey data to inform local STGs that recommend appropriate management of UTIs and to limit emerging resistance.
UTIs in male patients are categorised as 'complicated', and the recommended therapy is fluoroquinolones.[12,32] In the present study, 20.6% of male UTI episodes were treated with nitrofurantoin. There is conflicting evidence with regard to the use of nitrofurantoin in men.[37,38]
According to a Cochrane review,[39] there is insufficient evidence to recommend urinary alkalisers for symptomatic relief of uncomplicated UTIs. The PHC EML 2018 recommends against the use of alkalising agents.[12] Citro-Soda, a urinary alkaliser, was prescribed in 13.2% of UTI episodes in the present study. In 41.5% of these episodes, ciprofloxacin was concurrently used - the urinary alkaliser interfering with the effectiveness of ciprofloxacin.[40]
According to various guidelines, asymptomatic bacteriuria should not be treated in the elderly or in diabetic patients;[20,32] however, one elderly patient in the present study was prescribed antibiotic therapy for asymptomatic bacteriuria. Asymptomatic bacteriuria during pregnancy was appropriately treated with antibiotics. Therapy was unknown in one patient.
Antimicrobial resistance surveillance is a critical weapon in the fight against antibiotic resistance. Urine microscopy and sensitivity analysis could strengthen surveillance and guide empirical therapy. According to the PHC EML 2018 recommendations,[12] urine microscopy is recommended in complicated and recurrent UTIs, UTIs in men and pregnant women, and upper UTIs. In the present study, urine microscopy was conducted in 20 complicated UTI episodes (6.7%), 7.9% of episodes in men, and 7.1% of episodes during pregnancy. Urine microscopy frequency was relatively low in view of the STG recommendations; reasons for this should therefore be considered, as well as access to urine microscopy services.
Recurrent UTIs are defined as UTI occurring at least three times during a period of 12 months or at least twice during a period of 6 months. Recurrent UTIs can be caused by reinfection or relapse.[21,32] It was not possible to determine true recurrence in our study, or to differentiate between reinfection and relapse. However, during the study period 16 patients experienced two UTI episodes and one female experienced three. Nitrofurantoin was the most frequently prescribed antibiotic during the first and second UTI episodes. In the case of the female with three UTI episodes, nitrofurantoin was prescribed for all three episodes. As stated above, urine microscopy frequency was low in recurrent UTI episodes.
This study identified recommendations for the multidisciplinary team for practice and future research to promote rational antibiotic prescribing and use. Interviews with pharmacists and prescribers would assist in understanding the knowledge on antibiotic use and prescribing to identify targeted interventions.
Recommendations
Differentiating between complicated and uncomplicated UTIs is critical, as it influences diagnostic investigations and antibiotic therapy. This differentiation must be clearly described in the evidence-based guidelines of the NDoH (e.g. STGs) to optimise antibiotic therapy. Also, recommendations for managing asymptomatic bacteriuria should be explicitly described.
Considering the antibiotic resistance crisis, it is important to monitor resistance of uropathogens to nitrofurantoin and ciprofloxacin. Future research is needed to investigate and address the low compliance with urine microscopy to consider feasible and appropriate recommendations.
Prescribing patterns should be monitored on a continuous basis through collaboration between NDoH stakeholders and the Medicine Use Evaluation Committee, as this will highlight areas for improvement. Subsequent to this study (in 2020), the UTI recommendations were amended again.[41] Through this process, adoption of guidelines can be monitored and improved. Pharmacists form an integral part of the antibiotic stewardship programmes in primary healthcare.[42] The pharmacist's role in antibiotic stewardship includes, but is not limited to, educating and training other healthcare professionals as well as the public, reviewing antibiotic prescriptions on a daily basis, and determining compliance with STGs and evidence-based medicine recommendations.[13,42] The present study has shown that a collaborative, pharmacist-led investigation exposed inappropriate use of antibiotics and highlighted areas for improvement in managing UTIs, reflecting the important role pharmacists can fulfil at primary healthcare level in addressing antimicrobial stewardship.
Study strengths and limitations
This was a multicentre study with a reasonable sample size (power 80%) and limited missing data. Facilities were identified through a random selection process and objective measures were used for assessment. The study was conducted at six primary healthcare facilities, in the urban setting only, across three of the four substructures in the public sector of the Cape metropole in the Western Cape, and could not be generalised to rural and private settings. It was not possible to differentiate between cystitis and pyelonephritis owing to the inconsistent documented diagnoses in patient medical folders. Documented diagnoses varied; the researchers therefore categorised and analysed UTIs according to complicated and uncomplicated categories based on national and international guidelines and societies.[12,21,32,33] However, this classification did not compromise our assessment of compliance with UTI STG recommendations.
Conclusion
Interventions are required to improve compliance with prescribing antibiotics as per guideline recommendations, specifically selecting the appropriate antibiotic, duration of therapy and urine microscopy.
Declaration. The research for this study was done in partial fulfilment of the requirements for NK's MClinPharm degree at the University of the Western Cape.
Acknowledgements. The authors acknowledge all healthcare staff involved in assisting with access to patient medical folders.
Author contributions. NK, YJ and RC developed the study. NK collected and analysed the data and wrote the initial draft of the manuscript. YJ and RC reviewed and edited the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. O'Neil J. Antimicrobial resistance: Tackling a crisis for the health and wealth of nations. London: Review on Antimicrobial Resistance, 2014. https://wellcomecollection.org/works/rdpck35v (accessed 20 June 2021). [ Links ]
2. Chandra P, Unnikrishnan MK, Vandana KE, et al. Antimicrobial resistance and the post antibiotic era: Better late than never effort. Expert Opin Drug Saf 2021;20(11):1375-1390. https://doi.org/10.1080/14740338.2021.1928633 [ Links ]
3. Shapiro DJ, Hicks LA, Pavia AT, Hersh AL. Antibiotic prescribing for adults in ambulatory care in the USA, 2007 - 09. J Antimicrob Chemother 2014;69(1):234-240. https://doi.org/10.1093/jac/dkt301 [ Links ]
4. Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010 - 2011. JAMA 2016;315(17):1864-1873. https://doi.org/10.1001/jama.2016.4151 [ Links ]
5. Department of Health Standing Medical Advisory Committee, UK. The path of least resistance: Report of Sub-group on Antimicrobial Resistance. London: Department of Health, 1998. [ Links ]
6. Centers for Disease Control and Prevention, USA. Measuring outpatient antibiotic prescribing. 2019. https://www.cdc.gov/antibiotic-use/community/programs-measurement/measuring-antibiotic-prescribing.html (accessed 15 July 2021). [ Links ]
7. World Health Organization. Global Action Plan on Antimicrobial Resistance. 2015. https://apps.who.int/iris/handle/10665/193736 (accessed 30 June 2021). [ Links ]
8. Cox JA, Vlieghe E, Mendelson M, et al Antibiotic stewardship in low- and middle-income countries: The same but different? Clin Microbiol Infect 2017;23(11):812-818. https://doi.org/10.1016/j.cmi.2017.07.010 [ Links ]
9. Chetty S, Reddy M, Ramsamy Y, Naidoo A, Essack S. Antimicrobial stewardship in South Africa: A scoping review of the published literature. JAC Antimicrob Resist 2019;1(3):dlz060. https://academic.oup.com/jacamr/article/1/3/dlz060/5645376 [ Links ]
10. Peters SM, Werner J, Willems B. Antimicrobial stewardship in the Western Cape: A situational analysis of existing facility-level initiatives. S Afr Med J 2021;111(5):421-425. https://doi.org/10.7196/SAMJ.2021.v111i5.14645 [ Links ]
11. National Department of Health, South Africa. Antimicrobial Resistance National Strategy Framework 2014 - 2024. 2014. https://health-e.org.za/wp-content/uploads/2015/09/Antimicrobial-Resistance-National-Strategy-Framework-2014-2024.pdf (accessed 14 June 2021). [ Links ]
12. National Department of Health, South Africa. Primary Healthcare Standard Treatment Guidelines and Essential Medicines List 6th edition - 2018. Pretoria: NDoH, 2018. https://www.knowledgehub.org.za/elibrary/primary-healthcare-standard-treatment-guidelines-and-essential-medicines-list-6th-edition (accessed 20 January 2021). [ Links ]
13. Gasson J, Blockman M, Willems B. Antibiotic prescribing practice and adherence to guidelines in primary care in the Cape Town metro district, South Africa. S Afr Med J 2018;108(4):304-310. https://doi.org/10.7196/SAMJ.2017.v108i4.12564 [ Links ]
14. Medina M, Castillo-Pino E. An introduction to the epidemiology and burden of urinary tract infections. Ther Adv Urol 2019:11:1756287219832172. https://doi.org/10.1177/1756287219832172 [ Links ]
15. Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis 2011;52(5):103-120. https://doi.org/10.1093/cid/ciq257 [ Links ]
16. World Health Organization. Global Antimicrobial Resistance Surveillance System (GLASS) Report: Early implementation 2016 - 2017. Geneva: WHO, 2017. https://www.who.int/docs/default-source/searo/amr/global-antimicrobial-resistance-surveillance-system-(glass)-report-early-implementation-2016-2017.pdfsfvrsn=ea19cc4a_2 (accessed 10 July 2021). [ Links ]
17. Öztürk R, Murt A. Epidemiology of urological infections: A global burden. World J Urol 2020;38(11):2669-2679. https://doi.org/10.1007/s00345-019-03071-4 [ Links ]
18. Chu CM, Lowder JL. Diagnosis and treatment of urinary tract infections across age groups. Am J Obstet Gynecol 2018;219(1):40-51. https://doi.org/10.1016/j.ajog.2017.12.231 [ Links ]
19. Smaill FM, Vazquez JC. Antibiotics for asymptomatic bacteriuria in pregnancy. Cochrane Database Syst Rev 2019, Issue 11. Art. No.: CD000490. https://doi.org/10.1002/14651858.CD000490.pub4 [ Links ]
20. Nicolle LE, Gupta K, Bradley SF, et al. Clinical practice guideline for the management of asymptomatic bacteriuria: 2019 update by the Infectious Diseases Society of America. Clin Infect Dis 2019;68(10):e83-e110. https://doi.org/10.1093/cid/ciy1121 [ Links ]
21. Fernandez J, Coyle E. Urinary tract infections and prostatitis. In: DiPiro J, Yee GC, Posey LM, Haines ST, Nolin TD, Ellingrod V, eds. Pharmacotherapy: A Pathophysiological Approach. 11th ed. New York: McGraw-Hill Education, 2019. [ Links ]
22. Bosch FJ, van Vuuren C, Joubert G. Antimicrobial resistance patterns in outpatient urinary tract infections - the constant need to revise prescribing habits. S Afr Med J 2011;101(10):328-331. [ Links ]
23. Nzalie RN-T, Gonsu HK, Koulla-Shiro S. Bacterial etiology and antibiotic resistance profile of community-acquired urinary tract infections in a Cameroonian city. Int J Microbiol 2016;2016:3240268. https://doi.org/10.1155/2016/3240268 [ Links ]
24. Bhola P, Mvelase NR, Balakrishna Y, Mlisana KP, Swe-Han KS. Antimicrobial susceptibility patterns of uropathogens isolated from pregnant women in KwaZulu-Natal Province: 2011 - 2016. S Afr Med J 2020;110(9):872-876. https://doi.org/10.7196/SAMJ.2020.v110i9.14468 [ Links ]
25. Fourie JL, Claassen FM, Myburgh JJ. Causative pathogens and antibiotic resistance in community-acquired urinary tract infections in central South Africa. S Afr Med J 2021;111(2):124-128. https://doi.org/10.7196/SAMJ.2021.v111i2.14905 [ Links ]
26. Lewis DA, Gumede LY, van der Hoven LA, et al. Antimicrobial susceptibility of organisms causing community-acquired urinary tract infections in Gauteng Province, South Africa. S Afr Med J 2013;103(6):377-381. https://doi.org/10.7196/SAMJ.6722 [ Links ]
27. Wagenlehner FME, Johansen TEB, Cai T, et al. Epidemiology, definition and treatment of complicated urinary tract infections. Nat Rev Urol 2020;17(10):586-600. https://doi.org/10.1038/s41585-020-0362-4 [ Links ]
28. European Medicines Agency. Quinolone- and fluoroquinolone-containing medicinal products. 2018. https://www.ema.europa.eu/en/medicines/human/referrals/quinolone-fluoroquinolone-cont aining-medicinal-products (accessed 12 June 2021). [ Links ]
29. US Food and Drug Administration. FDA drug safety communication: FDA warns about increased risk of ruptures or tears in the aorta blood vessel with fluoroquinolone antibiotics in certain patients. 2018. https://www.fda.gov/drugs/drug-safety-and-availability/fda-warns-about-increased-risk-ruptures-or-tears-aorta-blood-vessel-fluoroquinolone-antibiotics (accessed 28 July 2021). [ Links ]
30. National Department of Health, South Africa. Circular H53/2019 Notice: Risk of serious adverse effects associated with fluoroquinolones. 2019. [ Links ]
31. Naing L, Winn T, Rusli B. Practical issues in calculating the sample size for prevalence studies. Arch Orofac Sci 2006;1:9-14. [ Links ]
32. Bonkat G, Pickard R, Bartoletti R, et al. EAU Guidelines on Urological Infections. 2018. https://uroweb.org/wp-content/uploads/EAU-Guidelines-on-Urological-Infections-2018-large-text.pdf (accessed 10 June 2021). [ Links ]
33. Sabih A, Leslie S. Complicated urinary tract infections. In: StatPearls [Internet]. Treasure Island, Fla.: StatPearls Publishing, 2022. https://pubmed.ncbi.nlm.nih.gov/28613784/ (accessed 10 June 2021). [ Links ]
34. National Department of Health, South Africa. Circular H74/2020: Antibiotic selection and dosing for empiric treatment of urinary tract infections. 2020. [ Links ]
35. Wattengel B, DiTursi S, Schroeck J, Sellick J, Mergenhagen K. Outpatient antimicrobial stewardship: Targets for urinary tract infections. Am J Infect Control 2020;48(9):1009-1012. https://doi.org/10.1016/j.ajic.2019.12.018 [ Links ]
36. Cai T, Palagin I, Brunelli R, et al. Office-based approach to urinary tract infections in 50 000 patients: Results from the REWIND study. Int J Antimicrob Agents 2020;56(1):105966. https://doi.org/10.1016/j.ijantimicag.2020.105966 [ Links ]
37. Ingalsbe M, Wojciechowski A, Smith K, Mergenhagen K. Effectiveness and safety of nitrofurantoin in outpatient male veterans. Ther Adv Urol 2015;7(4):186-193. https://doi.org/10.1177/1756287215581556 [ Links ]
38. Wolterink I, Verheij T, Platteel T, et al. Nitrofurantoin failure in elderly men: A retrospective observational study. Antibiotics 2020;9(5):3-7. https://doi.org/10.3390/antibiotics9050211 [ Links ]
39. O'Kane DB, Dave SK, Gore N, et al. Urinary alkalisattion for symptomatic uncomplicated urinary tract infection in women. Cochrane Database Syst Rev 2016, Issue 4. Art. No.: CD010745. https://doi.org/10.1002/14651858.CD010745.pub2 [ Links ]
40. Bayer HealthCare Pharmaceuticals Inc. CIPRO (ciprofloxacin hydrochloride). 2016. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/019537s086lbl.pdf (accessed 1 July 2021). [ Links ]
41. National Department of Health, South Africa. Primary Healthcare Standard Treatment Guidelines and Essential Medicines List for South Africa - 2020. 7th ed. Pretoria: NDoH, 2020. https://www.knowledgehub.org.za/elibrary/primary-healthcare-phc-standard-treatment-guidelines-and-essential-medicines-list-soul (accessed 20 January 2021). [ Links ]
42. Garau J, Bassetti M. Role of pharmacists in antimicrobial stewardship programmes. Int J Clin Pharm 2018;40(5):948-952. https://doi.org/10.1007/s11096-018-0675-z [ Links ]
 Correspondence:
Correspondence:
N Keuler
nnkeuler@uwc.ac.za
Accepted 29 March 2022


{kind=link}
{kind=link}
{kind=link}