










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.7 Pretoria Jul. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i7.16303
RESEARCH
Non-fatal injuries among boys and girls presenting to Red Cross War Memorial Children's Hospital, Cape Town
M PrinslooI, II; K HunterIII, IV; R MatzopoulosV, VI; E MillettVII; S van AsVIII, IX, X; E JordaanXI; M M PedenXII, XIII
IMPH, PhD; Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa
IIMPH, PhD; Institute for Lifecourse Development, Faculty of Education, Health and Human Sciences, University of Greenwich, London, UK
IIIMPH, PhD; The George Institute for Global Health Australia, Sydney, Australia
IVMPH, PhD; University of New South Wales, Sydney, Australia
VMPhil, PhD; Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa
VIMPhil, PhD; School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
VIIMSc, PhD (deceased); The George Institute for Global Health UK, Imperial College London, UK
VIIIMMed (Surgery), PhD; ChildSafe, Red Cross War Memorial Childrens Hospital, Cape Town, South Africa
IXMMed (Surgery), PhD; Division of Paediatric Surgery, Faculty of Health Sciences, University of Cape Town, South Africa
XMMed (Surgery), PhD; Department of Surgery, School of Medicine, University of Limpopo, South Africa
XIMSc (Statistics); Biostatistics Unit, South African Medical Research Council, Cape Town, South Africa
XIIBSc Med Hons (Epidemiology), PhD; University of New South Wales, Sydney, Australia
XIIIBSc Med Hons (Epidemiology), PhD; The George Institute for Global Health UK, Imperial College London, UK
ABSTRACT
BACKGROUND: In South Africa (SA), road traffic injuries, homicides and burns are the leading causes of injury-related deaths among children. Injury-related deaths are well documented for SA, but this is not the case for non-fatal injuries
OBJECTIVES: To describe the non-fatal injuries sustained among children aged 0-13 years, to identify any significant sex differences by age group, cause of injury, admission status and injury severity
METHODS: The trauma unit database from 1997 to 2016 at Red Cross War Memorial Childrens Hospital, Cape Town, was utilised for this analysis. The prevalence of injuries and the boy/girl ratios with 95% confidence intervals (CIs) were reported
RESULTS: Analysis indicated significant differences by sex for individual injury causes (transport, assault, burns, falls and other injuries), age group, injury severity and admission status. Moderately severe injuries were largely caused by burns, while severe injuries were mostly transport related. Boys had significantly higher proportions of all injury causes. The boy/girl ratio was lowest for assault (1:18), where significantly more girls aged 1-3 and 4-6 years were injured. Rape/sexual assault was 5.5 times higher for girls, with a significantly higher proportion of moderate-severity injuries (87%; 95% CI 84.7 - 89.4
CONCLUSION: The study findings call for a more targeted prevention response for boy and girl children. Interventions should be targeted at the prevention of burns, traffic collisions and interpersonal violence, in particular sexual assaults against girls
Paediatric injuries are a growing concern globally, especially in low-and middle-income countries (LMICs), where they are associated with significant morbidity and mortality[1] Injuries can also result in disability, with short-term or lifelong consequences. LMICs in the African region are affected by high rates of child injury mortality, particularly from road traffic crashes and violence.[2] Data to characterise the causes associated with childhood fatal and nonfatal injuries in these countries are very scarce, however, and sex disaggregation is not routinely undertaken during analysis.
Interpersonal violence and road traffic injuries are the 8th and 9th leading causes of death for all South Africans,[3] each with a rate of -35 per 100 000 population in 2012.[4] These injuries contribute greatly to premature mortality in South Africa (SA).[3,5-7] A 2014 child death review pilot study of two mortuaries in Western Cape and KwaZulu-Natal provinces for deaths < 18 years found that 42.6% of all childhood deaths were non-natural.[8] Most of these deaths are due to road traffic injuries, which were found to be the second leading cause of death after HIV for children aged 5-14 years.[5]
Analysis of a nationally representative study of injury mortality conducted in 2009[9] found a higher likelihood of unintentional injury deaths among children aged 0-14 years and significantly higher unintentional injury mortality rates among children aged 0-4 years in urban areas compared with rural areas.[10] However, reducing injury deaths is not likely to be a high priority for SA policy makers, as communicable diseases still lead the cause-of-death profile for children aged 0-4 years.[3,5] However, appropriate interventions are needed to reduce these preventable injuries and deaths.
Injury-related deaths are quite well documented in SA, but this is not the case for non-fatal injuries. Furthermore, sex disaggregation is not routinely conducted or linked to prevention activities. This article therefore aims to describe the injury profile for boys and girls, by age and severity, for the main causes of injuries sustained over two decades (1997 - 2016). Using the Red Cross War Memorial Childrens Hospital (RCWMCH) database for childhood injuries, we hope to answer the question 'who is injured' using a gender lens, and glean how this information can be used to build more specific intervention strategies to reduce the high rates of injuries in children.[11-14]
Methods
Data source and variables
Data from 1997 to 2016 were sourced from RCWMCH, a state-funded paediatric tertiary-level hospital affiliated to the University of Cape Town. RCWMCH primarily treats children aged 0-13 years and serves suburbs in the southern part of Cape Town. It also receives severely injured children referred from further afield. The hospital's database is managed by ChildSafe (https://www.childsafe.org.za/), a non-governmental organisation focusing on child injury research, advocacy, community education and cause-specific injury prevention programmes. Ethical approval was obtained from the University of Cape Town Human Research Ethics Committee (ref. no. HREC/REf:085/2010 (amendment)) and the University of Oxford Tropical Research Ethics Committee (ref. no. OxTREC: 530-18).
A routine trauma unit record form is used to capture age, sex, cause and mechanism of injury, place of occurrence, clinical presentation, severity, anatomy (i.e. brain, face, thorax, hand, etc.), pathology (concussion, laceration, pneumothorax, fracture, etc.), admission status (not admitted, admitted to trauma unit, admitted to ward/intensive care unit (ICU)) and treatment (dressings, clean and suture, open operation, etc.) for all injured children aged 0-13 years who present to the hospital accident and emergency unit.
For the injury cause categories, the related mechanisms include the following: transport, comprising motor vehicle passenger and pedestrian injuries, and bicycle- and motorcycle-related injuries; assault, comprising blunt objects, sharp (penetrating) objects, rape/ sexual assault, and other mechanisms such as human bite; burn-related injuries, comprising flame, fluid, heat contact, electrical, chemical, explosion and other burns; falls, comprising falls from beds, stairs, attendants' arms, playground equipment, mobiles and other heights and levels; and other injuries, comprising injuries arising from being struck by or against an object or caught between objects, sharp (penetrating) instruments, firearms, machinery, dog and other bites, immersion/drowning, suffocation, food and other foreign body ingestion, and other mechanisms not specified. The injury severity categories were coded numerically, for minor, moderate, severe and death (1 - 4), on the trauma unit record form and selected by each patient's attending doctor. The level of severity was recorded for a maximum of the four most severe injuries, according to the anatomy and pathology of the recorded injury.
Each record is de-identified, and the data are captured into an Excel spreadsheet, version 2016 (Microsoft Corp., USA), by volunteers at ChildSafe. For the purposes of analysis, cases were stratified into age groups that delineate important developmental stages and target groups for cause-specific injury prevention programmes and policies, viz. <1 year, 1-3 years, 4-6 years, 7-9 years and 10-13 years.
Statistical analysis
The prevalence of injuries, 95% confidence intervals (CIs) and boy/ girl ratios with 95% CIs were reported by sex. Results were reported by age group, cause of injury, mechanism of injury, injury severity admission status, and combinations thereof. Where the injury severity score was missing for the primary injury, the missing values were substituted with the severity score of the second most severe injury for analysis. We conducted a post hoc analysis of assault and sex, because sex differences for assault were different from all other injury mechanisms when examined by age group. Univariate and bivariate analysis for selected combinations of age, cause, severity admission status, and assault type were undertaken.
The responses for the various outcomes (cause, severity, assault mechanism, admission status) were modelled using a generalised linear model (GENMOD procedure) in SAS 9.4 (SAS Institute Inc., USA). The distribution of the response was binomial and was specified in the form of a ratio of two variables denoting injuries/total number in the subgroup for each sex. A log link was used to obtain the injury prevalence by subgroup and sex, and the reference category for all models was girls, to report the ratio for boys v. girls.
Results
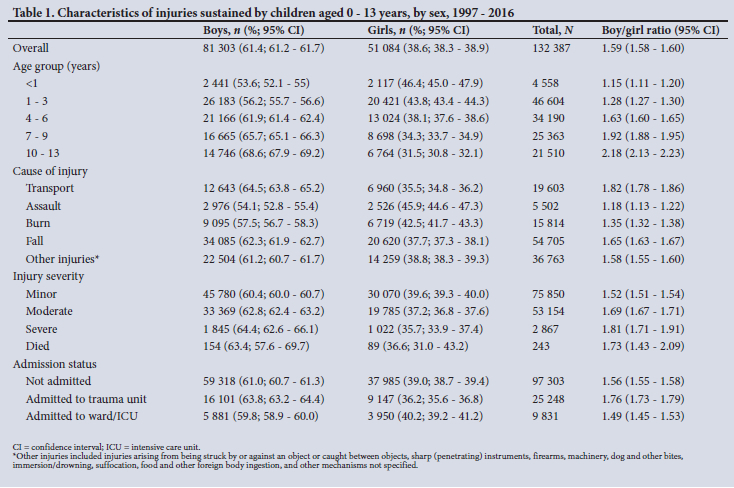
Between 1997 and 2016, there were 132 387 injury cases recorded Falls were the leading cause of injury, followed by other injuries, transport, burns and assault. The highest caseloads were observed among 1 - 3-year olds (n=46 604 cases), followed by the 4 - 6-year old group (n=34 190 cases). There were significant differences in injury characteristics by sex (Table 1). Overall, the boy/girl ratio was 1.59 (95% CI 1.58 - 1.60). The boy/girl ratio increased with each age group from 1.15 (95% CI 1.11 - 1.20) among children <1 year of age to 2.18 for children aged 10-13 years, where more than two-thirds of injuries were among boys (68.6%; 95% CI 67.9 -69.2).
Boys had significantly higher risk than girls across all age groups, injury causes, severity levels and admission status (Table 1). The largest boy/girl risk ratio (2.18) was in the oldest age group (10 -13 years), and the risk ratio was smallest (1.15) in children aged <1 year. For cause of injury, the boy/girl risk ratio was lowest for assault (1.18) and burns (1.35). Boys had significantly more moderate, severe and fatal injuries than girls. Most injuries were minor: most children were seen and discharged. Fewer than one-fifth were admitted to the trauma unit, 7.4% were admitted to a ward or ICU, and only <0.2% died of their injuries.
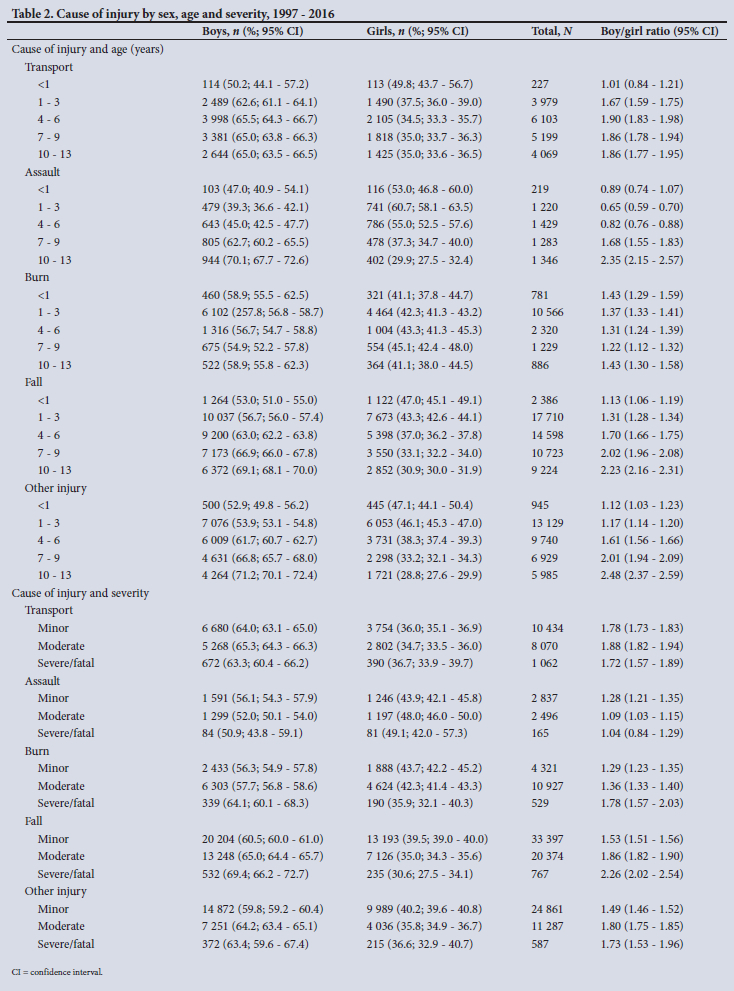
Stratified analysis by age group indicated that falls were the leading cause of injury across all age groups (Table 2). Boys were at significantly higher risk for transport-related injuries, burns, falls and other injuries in the 1-3- and 4 - 6-year age groups. However, the assault risk for girls was higher than for boys in the younger age groups <1, 1 - 3 and 4-6 years. This finding was significant for girls in the 1 - 3-year (60.7%; 95% CI 58.1 - 63.5) and 4 - 6-year (55.0%; 95% CI 52.5 - 57.6) age groups. For the 7-9- and 10 - 13-year age groups, boys were at significantly higher risk for all injury cause groups. The boy/girl risk ratio was most pronounced for assault in the oldest age group. Analysis for severity of injury by cause indicated that, of all the injury cause categories, transport-related injuries had the most severe/fatal injuries among both sexes. For assault, unlike every other cause category, there was no significant difference in fatality risk between boys and girls.
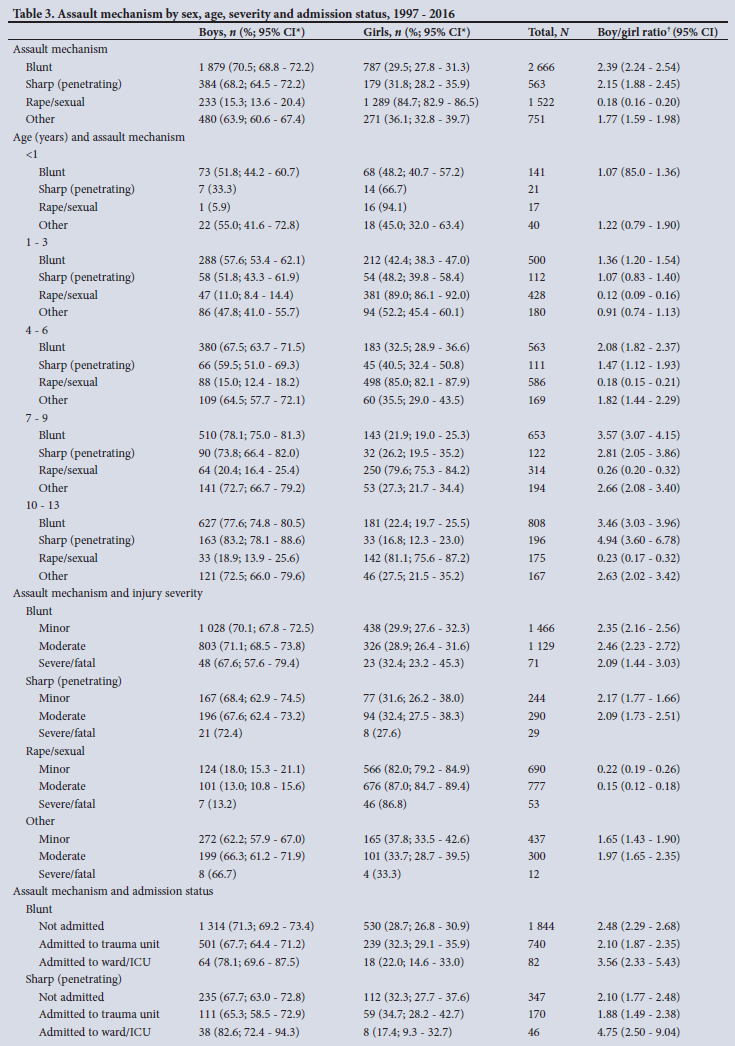
These sex differences are also reflected in the analysis of injury severity and admission status by the specific mechanism of assault (Table 3). Boys had significantly more blunt-force injuries (70.5%; 95% CI 68.8 - 72.2) than girls (29.5%; 95% CI 27.8 - 31.3). This was followed by rape/sexual assault, where girls (84.7%; 95% CI 82.9 - 86.5) had significantly more injuries than boys (15.3%; 95% CI 13.6 - 20.4). This higher magnitude of rape/sexual assault for girls persisted from the ages of 1 to 13 years. When considering assault mechanism and injury severity, boys had significantly more blunt assaults of minor severity (70.1%; 95% CI 67.8 - 72.5) and moderate severity (71.1%; 95% CI: 68.5 - 73.8) and more severe/ fatal assaults (67.6%; 95% CI: 57.6 - 79.4) than girls. However, girls had significantly more injuries associated with rape/sexual assault of minor severity (82.0%; 95% CI 79.2 - 84.9) and moderate severity (87.0%; 95% CI 84.7 - 89.4) than boys. In addition, girls had more severe or fatal rape/sexual assault injuries. Analysis of assault mechanism by admission status indicated that significantly more girls who had injuries associated with rape/sexual assault (88.1%; 95% CI 85.7 - 90.5) were admitted to the trauma unit compared with boys (11.9%; 95% CI 9.7 - 14.6).
Most of the blunt assaults and rape/sexual assaults occurred inside and around their home for both boys and girls (Fig. 1). Blunt assaults at school/daycare centres and public places were more prevalent for boys. Rape/sexual assault inside other peoples homes was more prevalent for girls.

Discussion
Our study indicates significant sex differences by age group, cause of injury and severity among injured children presenting to RCWMCH in Cape Town. Although boys had significantly higher risks across all age groups and causes than girls, higher severity of rape/sexual assault was seen among young girls.
These results have policy and practice implications that need to be addressed in order for SA to meet a number of the Sustainable Development Goal (SDG) targets, including a reduction in the number of deaths/injuries from road traffic crashes (SDG 3.6). eliminating all forms of violence against women and girls (SDG 5.2), and ending abuse and all forms of violence and torture of children (SDG 16.2)by2030.[15]
As with previous analyses, most injuries sustained by children presenting to RCWMCH were related to falls.[12,13] Significantly more boys presented than girls, and those aged 1-3 and 4-6 years were the most common attendees, which is not unexpected because this is the age at which children tend to start to socialise as toddlers and participate in higher-risk behaviour. Falls are, however, very amendable to several proven prevention strategies. Increasing supervision for the 4 - 6-year age group is essential, alongside establishing playground safety standards, maintaining equipment and surface material and legislating for window guards.[16-18] Low-cost modifications of these interventions should be possible, even in LMICs. Other interventions such as supportive home visitation,
education for at-risk families and mass media campaigns[1,19] should also be introduced.
Transport injuries were more common among boys than girls across all age ranges and were associated with the highest number of severe and fatal injuries, probably because, as has been documented previously, most children were injured as pedestrians or unrestrained passengers.[20] In SA many children are transported to school in minibus taxis or on the back of 'bakkies' (pick-up trucks), neither of which are equipped with appropriate safety restraints. In addition, many children seen at RCWMCH come from low-income suburbs where there are few amenities for them to play safely, and many of them also walk to school unaccompanied on busy streets. Prevention strategies should therefore focus on these two high-risk groups by implementing, for example, a maximum speed limit in residential areas or near schools and play areas[21] restraining young passengers with child restraint seats, and adult supervision.[22] The authors propose that the age limitation for child car restraints and booster seats be increased from <3 years up to the age of 7 years,[23] and that the documented barriers to the uptake of child restraints in the city, and factors that would facilitate them, be addressed by local government.[24]
Boys sustained significantly more burn-related injuries than girls for all age groups, with 1 - 3-year-old boys accounting for most cases. This is possibly related to young boys being more likely than girls to explore their surroundings as they become mobile. More than two-thirds of burn-related injuries were of moderate severity, which can cause scarring and disability, leading to lifelong physical and psychological consequences. These injuries usually result in long hospital stays with costly treatment regimens to aid physical and emotional functioning. Burn-related injuries are preventable, but are strongly associated with poverty in Cape Town and throughout SA.
Although the South African Bureau of Standards (SABS) enacted a national standard for the safe use of paraffin stoves in 2006, the quality of the manufacturing of these stoves does not appear to be strictly monitored.[25] The key feature of the SABS-approved stove is a self-extinguishing mechanism if the appliance is tilted, but this is reported to malfunction. Suggested intervention strategies for this
environment include greater enforcement of home appliance standards and support from government to purchase safer, but more costly, liquefied petroleum gas for cooking and heating.[25,26] Additional burn prevention strategies could include setting and enforcing laws on smoke alarms and hot-water temperatures and providing first-aid training on how to treat burns.[1]
Significantly more girls than boys aged 1 - 3 and 4-6 years were assaulted, and this often occurred inside/outside homes, at schools/daycare centres and in public places. A national survey to estimate child maltreatment in SA[27] reported that 44.6% of 15 - 17-year-old respondents had experienced some form of child maltreatment in their lives. This included witnessing family violence, physical and emotional violence, neglect and sexual violence, with 15 -17-year-old girls reporting higher lifetime prevalence than boys. National estimates for child homicide[28,29] indicated that sexual assault and abuse-related homicides were most common among girls in the 1 - 4-year age group,[28] which corresponds to the findings of the present study. Interventions to prevent sexual assault are needed at an early age, as national evidence shows that it may lead to substance misuse, high-risk sexual behaviour, post-traumatic stress disorder, and depression and anxiety in adolescence.[30] Prevention strategies that have been put forward include substance abuse interventions, caregiver support to develop warm and caring relationships with children, and non-violent approaches to managing children's behaviour.[30] Putting such strategies into place would require enhanced intersectoral co-ordination in SA, particularly with regard to reporting, medical treatment, psychosocial support to victims, and timely prosecution of offenders.[28] The World Health Organizations handbook on selecting, implementing and monitoring effective violence prevention policies and programmes[31] should be used as a guide to respond to violence against children in SA.
Study limitations
RCWMCH only treats children aged <13 years who seek treatment at a public hospital. The results are therefore not representative of the entire Cape Town population, or even subdistricts of the hospitals catchment area. We could therefore not calculate population-based rates. However, although hospital-based data remain the most robust data to study sex differences among injured children in SA, there is still a need to improve the granularity of the current database. For instance, while information on restrained and unrestrained children is recorded, the data do not clarify whether an appropriate restraint was used and whether the child was correctly and securely strapped. Likewise, more specific details about assault cases could be captured in order to better target prevention strategies. Finally, the injury severity scoring system used at RCWMCH is not internationally recognised and therefore cannot be used to compare with many other studies that use the Abbreviated Injury Scale or the Injury Severity Score (ISS). With this in mind, the trauma form is currently being modified to a digital version, which will include the internationally recognised ISS, to record the injury severity based on six different body regions.[32]
Conclusion
This analysis reiterates the importance of conducting sex analysis on data, as it can uncover important biases and inequities that could have an impact on the policies and practices implemented in resource-poor settings[33] to prevent childhood injuries and to alleviate the burden on clinical staff. It has highlighted the need to develop interventions targeted at the prevention of burns, interpersonal violence and transport injuries among boys and sexual assaults among girls. In addition, it has highlighted priority age groups for these interventions. The importance of understanding the factors driving the differences for sexual assault among children is an area that warrants further in-depth investigation.
Declaration. None.
Acknowledgements. The authors thank the RCWMCH medical staff, and the members of ChildSafe who capture the data on an annual basis.
Author contributions. SvA provided the data. EM, MP and MMP cleaned the data. EM, MP and EJ provided analysis with input from MMP, KH and RM. MP, MMP, KH, RM and EJ drafted the manuscript, with review and final approval by all contributors, except for EM, who passed away on 10 March 2019.
Funding. A small grant from The George Institute's Global Womens Health Program Research Funding Grant (2018).
Conflicts of interest. None.
References
1. Peden M, Oyegbite K, Ozanne-Smith J, et al. eds. World report on child injury prevention. Geneva. World Health Organization, 2008. https://apps.who.int/iris/bitstream/handie/10665/43851/9789241563574_engpdf.jsessionid=ACAB4555C26AB9175C71E423323DEBC6?sequence=1 (accessed 14 September 2017). [ Links ]
2. Peden M, Hyder AA. Time to keep African kids safer. S Afr Med J 2009;99(1):36-37. [ Links ]
3. Piliay-van Wyk V, Msemburi W, Laubscher R, et al. Mortality trends and differentials in South Africa from 1997 to 2012. Second National Burden of Disease Study. Lancet Glob Health 2016;4(9):642-e653. https://doi.org/10.1016/S2214-109X(16)30113-9 [ Links ]
4. Piliay-van Wyk V, Msemburi W, Laubscher R, et al. Supplementary appendix. Mortality trends and differentials in South Africa from 1997 to 2012. Second National Burden of Disease Study. Lancet Glob Health 2016;(9):e642-e653. https://www.thelancet.com/cms/10.1016/S2214-109X(16)30113-9/attachment/ab7b9b9e-cc63-4bda-9ef3-6b6182e64029/mmc1.pdf (accessed 28 March 2019). [ Links ]
5. Msemburi W, Piliay-van Wyk V, Dorrington RE, et al. Second National Burden of Disease Study for South Africa. Cause-of-death profile for South Africa, 1997 - 2012. Cape Town. South African Medical Research Council, 2016. https://www.samrc.ac.za/sites/default/files/files/2016-12-08/SouthAfrica2012.pdf (accessed 14 September 2017). [ Links ]
6. Bradshaw D, Nannan N, Laubscher R, et al. South African National Burden of Disease Study 2000. Estimates of provincial mortality. Cape Town. South African Medical Research Council, 2004. https://www.samrc.ac.za/sites/defauit/files/fiies/2017-07-03/estimate.pdf (accessed 14 September 2014). [ Links ]
7. Norman R, Matzopouios R, Groenewald P, et al. The high burden of injuries in South Africa. Bull World Health Organ 2007;85(9):695-702. https://doi.org/10.2471/blt.06.037184 [ Links ]
8. Mathews S, Martin LJ, Coetzee D, et al. The South African child death review pilot. A multiagency approach to strengthen healthcare and protection for children. S Afr Med J 2016;106(9):895-899. https://doi.org/10.7196/SAMT.2016.vl06i9.11234 [ Links ]
9. Matzopouios R, Prinsloo M, Piliay-van Wyk V, et al. Injury-related mortality in South Africa. A retrospective descriptive study of post-mortem investigations. Bull World Health Organ 2015;93(5):303-313. https://doi.org/10.2471/BLT.14.145771 [ Links ]
10. Prinsloo M. Estimating injury mortality in South Africa and identifying urban-rural differences. DPhiJ thesis. Cape Town. University of Cape Town, 2019. https://open.uct.acza/bitstream/handle/11427/30083/thesis_hsf_2018_prinsloo_megan.pdf?sequence=l&isAliowed=y (19 August 2020). [ Links ]
11. Van As AB, van Niekerk A. Prevention of childhood injuries. S Afr Med J 2017;107(3):182. https://doi.org/10.7196/SAMT.2017.vl07i3.12364 [ Links ]
12. Campbell NM, Colvilie JG, van der Heyde Y, et al. Firearm injuries to children in Cape Town; South Africa. Impact of the 2004 Firearms Control Act. S Afr J Surg 2013;51(3):92-96. https://doi.org/10.7196/SATS.1220 [ Links ]
13. Wesson HKH, Bachani AM, Mtambeka P, et al. Changing state of pediatric injuries in South Africa. An analysis of surveillance data from a pediatric emergency department from 2007 to 2011. Surgery 2017;162(S6):S4-S11. https://doi.org/10.1016/j.surg.2017.03.019 [ Links ]
14. Wesson HKH, Bachani AM, Mtambeka P, et al. Pediatric burn injuries in South Africa. A 15-year analysis of hospital data. Injury 2013;44(11):1477-1482. https://doi.org/10.1016/j.injury.2012.12.017 [ Links ]
15. United Nations. Transforming our world. The 2030 Agenda for Sustainable Development. 25 September 2015. http://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/l&Lang=E (accessed4 March 2017). [ Links ]
16. Spiegel CN, Lindaman FC. Children can't fly. A program to prevent childhood morbidity and mortality from window falls. Am J Public Health 1977;67(12):1143-1147. https://doi.org/10.2105/ajph.67.12.1143 [ Links ]
17. MacKay M, Vincenten J, Brussoni M, et al. Child safety good practice guide. Good investments in unintentional child injury prevention and safety promotion. Amsterdam. European Child Safety Alliance (EuroSafe), 2006. https://www.childsafetyeurope.org/publications/goodpracticeguide/info/good-practice-guide.pdf (accessed 21 August 2020). [ Links ]
18. Mitchell R, Sherker S, Cavanagh M, et al. Falls from playground equipment. Will the new Australian playground safety standard make a difference and how will we tell? Health Promot J Austr 2007;18(2):98-104. https://doi.org/10.1071/he07098 [ Links ]
19. Rehmani R, LeBlanc JC. Home visits reduce the number of hazards for childhood home injuries in Karachi, Pakistan. A randomised controlled trial. Int J Emerg Med 2010;3:333-339. https://doi.org/10.1007/s12245-010-0238-0 [ Links ]
20. Ferreira Y, van As AB. Promote buckling up and save a child's life. S Afr Med J 2017;107(4):292-294. https://doi.org/10.7196/SAMT.2017.vl07i4.12433 [ Links ]
21. Cairns J, Warren J, Garthwaite K, et al. Go slow. An umbrella review of the effects of 20 mph zones and limits on health and health inequalities. J Public Health 2015;37(3):515-520. https://doi.org/10.1093/pubmed/fdu067 [ Links ]
22. World Health Organization. Save LIVES. A road safety technical package. Geneva. WHO, 2017. https://www.who.int/publications/i/item/save-lives-a-road-safety-technical-package (accessed 21 August 2020). [ Links ]
23. Janmohammed A, Attwood P, Mtambeka P, et al. The need for stronger child restraint laws. S Afr Med J 2019;109(8):545. https://doi.org/10.7196/SAMJ.2019.vl09i8.14118 [ Links ]
24. Hunter K, Bestman A, Dodd M, et al. Overloaded and unrestrained. A qualitative study with local experts exploring factors affecting child car restraint use in Cape Town, South Africa. Int J Environ Res Public Health 2020;17(14):4974. https://doi.org/10.3390/ijerphl7144974 [ Links ]
25. Kimemia DK, van Niekerk A. Energy poverty, shack fires and childhood burns. S Afr Med J 2017;107(4):289-291. https://doi.org/10.7196/SAMJ.2017.v107i4.12436 [ Links ]
26. Kimemia D, van Niekerk A. Cookstove options for safety and health. Comparative analysis of technological and usability attributes. Energy Policy 2017;105:451-457. https://doi.org/10.1016/j.enpol.2017.03.022 [ Links ]
27. Artz L, Burton P, Ward CL, et al. Sexual victimisation of children in South Africa. Final report of the Optimus Foundation Study. Zurich. UBS Optimus Foundation, 2016. https://www.saferspaces.org.za/uploads/files/08_cjcp_report_2016_d.pdf (accessed 2 May 2018). [ Links ]
28. Abrahams N, Mathews S, Martin LJ, et al. Gender differences in homicide of neonates, infants, and children under 5 y in South Africa. Results from the Cross-Sectional 2009 National Child Homicide Study. PLoS Med 2016;13(4):e1002003. https://doi.org/10.1371/journal.pmed.l002003 [ Links ]
29. Mathews S, Abrahams N, Jewkes R, et al. Child homicide patterns in South Africa. Is there a link to child abuse? Cape Town. South African Medical Research Council, 2012. http://www.mrc.ac.za/policybriefs/child homicide.pdf (accessed 9 March 2016). [ Links ]
30. Ward CL, Artz L, Leoschut L, et al. Sexual violence against children in South Africa. A nationally representative cross-sectional study of prevalence and correlates. Lancet Glob Health 2018;6(4):e460-e468. https://doi.org/10.1016/S2214-109X(18)30060-3 [ Links ]
31. World Health Organization. INSPIRE. Seven strategies for ending violence against children. Geneva. WHO, 2016. https://www.who.int/publications/i/item/inspire-seven-strategies-for-ending-violence-against-children (accessed 22 June 2020). [ Links ]
32. Baker SP, O'Neili B, Haddon W, et al. The injury severity score. A method for describing patients with multiple injuries and evaluating emergency care. J Trauma 1974;14(3):187-196. [ Links ]
33. Peters SAE, Norton R. Sex and gender reporting in global health. New editorial policies. BMJ Glob Health 2018;3:e001038. https://doi.org/10.1136/bmjgh-2018-001038 [ Links ]
 Correspondence:
Correspondence:
M Prinsloo
megan.prinsloo@mrc.ac.za
Accepted 7 April 2022


{kind=link}
{kind=link}
{kind=link}