










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 n.5b Pretoria May. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i5b.16063
RESEARCH
Governing a pandemic: A case study of South Africa's coordination and management structures used to respond to the COVID-19 pandemic
D MoonasarI, II; E LeonardIII; R NaidooIV; Y PillayV, VI; N GovenderVII; P ChitukuVIII; R MorewaneIX; W RamkrishnaX; T FurumeleXI; O P RamadanXII; A PillayXIII; N MayetXIV
IDrPH; National Department of Health Malaria, Vector and Zoonotic Diseases, Pretoria, South Africa
IIDrPH; University of Pretoria, School of Health Systems and Public Health, South Africa
IIIBEng; Clinton Health Access Initiative South Africa, Pretoria, South Africa
IVMSc (Med); National Department of Health, Department of Emergency Medical Services, Pretoria, South Africa
VPhD; Clinton Health Access Initiative South Africa, Pretoria, South Africa
VIPhD; Division of Health Systems and Public Health, Stellenbosch University, South Africa
VIIMSc; National Institute for Communicable Diseases, Division of the National Health Laboratory Service, Johannesburg, South Africa
VIIIMPH; Clinton Health Access Initiative South Africa, Pretoria, South Africa
IXMDev (Pol), BDentT, BTech; National Department of Health, Department of Primary Health Care, Pretoria, South Africa
XMPH; National Department of Health Malaria, Vector and Zoonotic Diseases, Pretoria, South Africa
XIMPH; National Department of Health Malaria, Vector and Zoonotic Diseases, Pretoria, South Africa
XIIMBChB, MPH; World Health Organisation, Emergency preparedness and Response (EPR), Nairobi, Kenya
XIIIPhD; National Department of Health, Health Regulation, and Compliance, Pretoria, South Africa
XIVMB ChB, MPhil; National Institute for Communicable Diseases, Division of the National Health Laboratory Service, Johannesburg, South Africa
ABSTRACT
During a public health emergency, coordination and management are essential for ensuring timeous, decisive, and harmonised leadership. In this paper, the governance structures utilised in South Africa (SA) during the COVID-19 pandemic are recorded and the key strengths and weaknesses of response in the country are discussed. A qualitative methodology is used for the case study and comprises insights from stakeholders who were at the forefront of SA's response as well as from documentation that was used to guide the response. Structured, transparent, science-based and agile coordination and management systems are necessary to gain the public's trust during a public health emergency. This case study contributes to the literature on governing a pandemic and shares lessons learned from the COVID-19 response. The lessons learned by the stakeholders within the SA governance structures can be leveraged in future public health emergencies within SA and other low- and middle-income countries.
The Director-General of the World Health Organization (WHO) declared the 2019 SARS-CoV-2 outbreak a public health emergency of international concern on 30 January 2020, under the ambit of the International Health Regulations (IHR) (2005), following advice from the Emergency Committee.[1] After the initial issuing of temporary recommendations for China and other countries to scale up preparedness, the WHO released the initial Strategic Preparedness and Response Plan for member states on 6 February 2020.[2] The plan outlined priority actions for scaling up a country's preparedness and response operations; one of which was to strengthen coordination.[2,3] The COVID-19 pandemic has emphasised the importance of strong coordination mechanisms in a country's health system.[4] Furthermore, a multi-sectoral approach is key to efficiently and effectively mitigating and containing a pandemic. In addition to the health coordination mechanisms, coordination mechanisms need to be in place for a whole country (multi-sectoral) and a whole of society response.
Epidemic preparedness and response capacity in South Africa (SA) is mandated by the National Health Act and the National Disaster Management Act. In addition, as a WHO Member State, the country has obligations under the International Health Regulations (IHR) 2005 to have systems in place for the early detection and response to public health threats. SA also has regional and global commitments in the African Union, Southern African Development Community, WHO, and neighbouring countries, to support international efforts in preventing, detecting public health events, and sharing information and resources. The objective of this case study is to demonstrate how SA used and adapted the acts, regulations, guidelines, and commitments to coordinate and respond to the COVID-19 pandemic and to analyse the strengths and weaknesses of the coordination mechanisms.
Methods and data sources
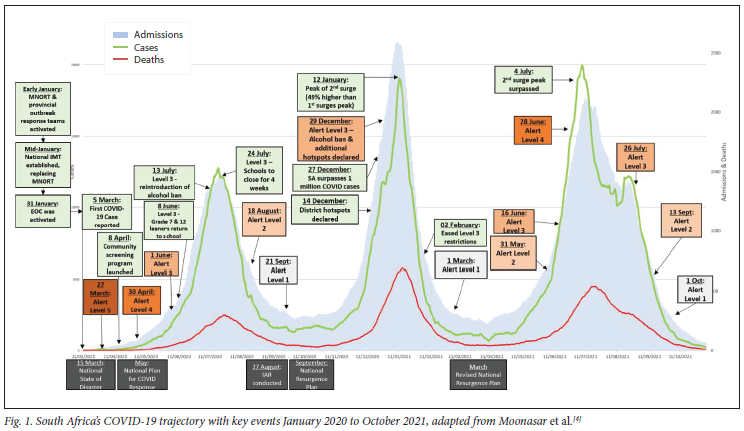
The methodology followed in this paper is a qualitative case study, defined as empirical inquiry into real-life phenomena.[5] The phenomenon investigated in this paper are pandemic governance structures within the real-life context of SA. The time frame covered in this case study is between January 2020 and October 2021. Fig 1 provides an overview of the key events that occurred during this period. The alert levels described in Fig 1 refer to the risk-adjusted strategy which was used to mitigate the impact of COVID-19 on the health system. Alert Level 5 consists of the most stringent restrictions and Alert Level 1 consists of the least stringent restrictions.
To perform the case study, data were collected from a variety of sources including insights from stakeholders who were at the forefront of SA's response, as well as information extracted from the documentation used to guide the response. An overview of the data sources used is summarised in Table 1.
From these data sources, information specific to coordination and management were gathered. In the following sections, a description of the coordination and governance structures utilised during the response are described. The strengths and weaknesses of the mechanisms are thereafter discussed.
Findings: Coordination and management structures used during the COVID-19 response
Existing structures
Respondents from the Intra-Action Review reports (IAR) lauded SA's strong coordination mechanisms for prevention and response to outbreaks. Pre-existing structures that were established to prevent, detect and respond to outbreaks has enabled strong coordination and these include the Multi-sectoral National Outbreak Response Team (MNORT), which was set up in the late 1990s and managed outbreaks such as the Lujo Virus outbreak in 2008, the Cholera outbreak in 2008/2009, the Rift Valley Fever outbreak in 2010/2011, the influenza (H1N1) pandemic in 2009/2010 and the Measles outbreak in 2011. This structure also played a coordination role in event-based surveillance for the 2010 World Cup. The National Emergency Operations Centre (EOC) was rapidly established at the National Institute for Communicable Disease in 2014 at the time of the West African Ebola outbreak and coordinated the response to the world's largest listeria outbreak. Provinces and districts in the country are meant to have similar structures but these differ from province to province dependant on the availability of resources.
New structures: Coordination structures to respond to COVID-19
With COVID-19 cases and deaths rapidly increasing in affected countries, in early January 2020, the SA MNORT and provincial outbreak response teams were activated. The Minister of Health met with other governmental departments through the preparedness and response structures that were in place. Shortly thereafter, a national Incidence Management Team (IMT) was established, in line with the WHO's framework for emergency response,[11] replacing the MNORT. The EOC was activated on 31 January 2020 by the Minister of Health as the coordinating structure to respond to the pandemic.
A month after these structures were established and activated, the first case of COVID-19 was confirmed in SA on 5 March 2020.[11] On 15 March 2020, the President of SA declared the COVID-19 outbreak a 'national disaster' in terms of Section 23 of the Disaster Management Act 57 of 2002,[7] announcing extraordinary interventions including travel restrictions, social distancing, and scaling up testing and contact tracing. The prescripts of the Act[7] allowed for the activation of, additional coordination structures such as the National Joint Intelligence structures (NATJoints) and the Provincial Joint Operation Centre (ProvJOC) system.
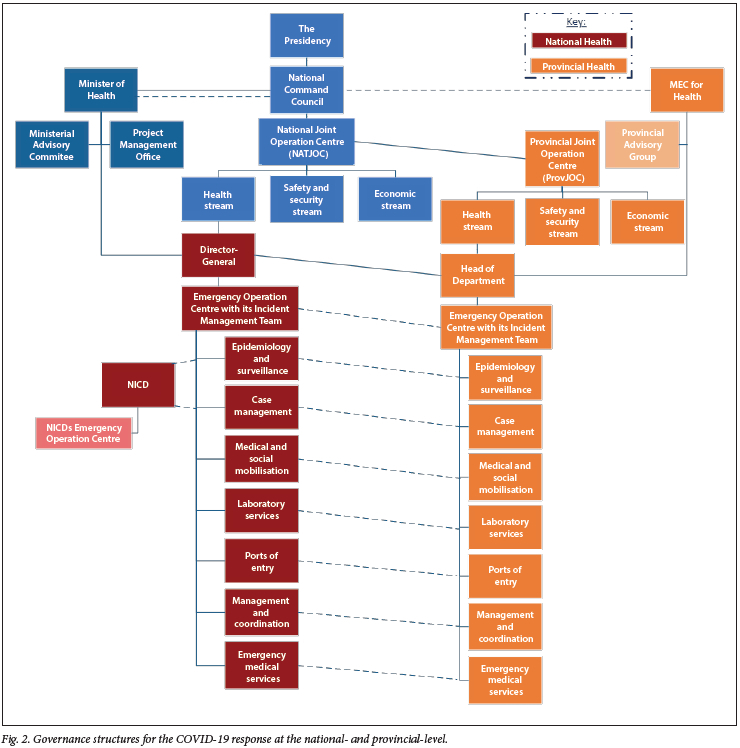
The detailed governance structures for the COVID-19 response at the national and provincial levels are shown in Fig 2. The outbreak is led politically by the National Coronavirus Command Council (NCCC) as established by the President of the country. The inter-government technical work is managed and coordinated within the NATJoints and its various workstreams.
The overall health response is led by the Minister of Health, and the Provincial Members of Executive Committees (MECs) responsible for health and is guided by the Ministerial Advisory Committees (MAC),[] National IMT, Project Management Office (PMO), NHC Tec and strategic partners and agencies such as WHO and NICD.
COVID-19 Incident Management Team
The National IMT, established in January 2020, is the technical arm of the health response and is responsible for strategic leadership, governance, and resource mobilisation for the health response. Initially the IMT held daily face-to-face meetings. As the number of cases increased however, and considering the need for physical distancing, the limitation on movement during the Level 5 lockdown, and the ban on gatherings, the meetings transitioned to a virtual meeting that continued to provide oversight of response activities.
The IMT structure was replicated in all provinces. The IMT structure aligned to the pillars of the WHO Strategic Preparedness and Readiness guidance[11] but adapted to the architecture of the SA Health System. The IMT was composed of public health and emergency management experts from the National Department of Health, NICD, National Health Laboratory Services (NHLS), and other partners according to the principles of an Incident Management System.[11]
The National IMT comprised nine workstreams namely Clinical Management; Community Screening and Testing; Environmental and Port Health; Epidemiology Surveillance and Response; Health Facility Readiness; Infection Prevention and Control; Laboratory and Diagnostics; Occupational Health and Safety; Risk Communication and Community Engagement; and Quarantine and Isolation, Human resource.
The National IMT developed a National Plan for COVID-19 Health Response which outlined the strategic objectives, strategies, and accountabilities for systematically responding to the pandemic. The plan had nine strategic priorities which corresponded to the nine workstreams of the IMT with an overarching goal of strengthening national and provincial mechanisms for timely detection, management, and containment of the spread of COVID-19.
The plan was later reviewed and supplemented with the COVID-19 Resurgence Mitigation plans at national, provincial, and district levels.
Discussion: Strengths and Weaknesses of the Coordination and Management Mechanisms
We reflect on the strengths and weaknesses of the existing and additional COVID-19 structures below.
Role of existing structures and networks
Pre-existing established relationships within the National Department of Health, Provincial Departments of Health, other government departments (e.g., South African National Defence Force), academics, the private sector, non-governmental organisations (NGO), and several partners such as the Centres of Disease Control and Prevention and the WHO were all leveraged to develop guidelines, plans and response strategies.
High-level political support through the NCC ensured a whole-of-government response to the pandemic and later incorporated a whole-of-society approach. Coordination in communicating the urgency of actions and advocating for additional resources for the response activities came from the office of the ministry of health.
Existing networks and relationships provided the prerequisites for efficient coordination particularly in laboratory testing, where the NICD was part of a global network of diagnostic testing laboratories and already a reference laboratory for SARS-CoV-2 testing for neighbouring countries. The National IMT leveraged networks with established networks with the private and NGO sector for joint training activities, resource sharing, and technical exchange.
Leveraging existing networks and structures was a strength of SA's response to COVID-19. There are however, areas that need improvement and strengthening, including the lack of standardisation of systems and processes and bi-directional linkages between national, province, and district. Intersectoral collaborations were challenging at times with sectors having competing priorities or not cooperating with the response.
SA COVID-19 IMT
Leadership and governance played an important role in preparing the facilities for the COVID-19 response. At the national IMT, plans, guidelines, and processes were developed at an early stage. The alignment between the National and Provincial IMT is key and provides the opportunity for reinforcment through regular catch-up sessions. While plans were developed timely, the implementation of the plans were not always successful. Follow ups, monitoring and evaluation of the developed plans need to be strengthened.
Several good practices can be highlighted from the functioning of the National IMT. Certain IMT workstreams had regular in-depth sessions through established network structures with provinces, specifically when challenges were experienced. Oxygen reticulation and facility readiness were well-coordinated through these structures.
A key strength of the IMT was illustrated by workstreams operating collaboratively to solve issues raised by provinces and districts. The benefits of a collaborative, non-siloed response should be prioritised during emergency responses. A detailed interrogation and rapid decision making were required to collectively respond with clearly defined roles and responsibilities that enabled the coordination, where this was absent, often resulted in duplication of efforts and left grass-root staff without direction.
Constant changes in information flow channels or requirements were a challenge that adversely impacted decision-making. The National IMT also experienced several challenges which affected its functioning. The initial IMT workstream leads were not able to work on the required tasks in a full-time capacity as they had to continue in their regular roles. This resulted in some of the workstreams being sub-optimally functional. In addition, changing leadership and lack of significant authority to act also hindered the functioning of the IMT
The National IMT liaised with the provincial colleagues through designated provincial senior managers, which improved coordination of the COVID-19 response between the national and provincial Departments of Health. However, even with these structures in place, provinces and districts worked independently, only relying on national structures for a daily line list of cases and guidelines to be made available. Response activities were made at the district and provincial level and information flowed top-down, without it necessarily filtering up to the national level. This resulted in a disconnect between the problem identified, the response, and the evaluation of the impact of the response.
The disadvantage of the largely top-down approach is that often situations that could have been responded to sooner or more efficiently came to the attention of the national level too late or not at all. Challenges existed around the national IMT's ability to hold provinces and districts accountable. This challenge is a result of a combination of conflicting legislation for emergency and outbreak response, and the three-tiered governance structure (national, province, district) that exists in SA.
These challenges were reflected in the variance in data elements, approaches to contact tracing, screening, and testing, and other key response elements.
Conclusion
In this paper, SA's coordination and management of the COVID-19 pandemic were considered. An overview of the structures used during the response was described and the strengths and weaknesses of these structures discussed.
The lessons learned should be integrated to make improvements to the SA structures as the pandemic continues and for future outbreaks or health crises. SA experienced varying degrees of success in terms of its COVID-19 coordination and management. By having intermittent review sessions, through the IAR, and resurgence planning sessions, a continuous improvement framework was established. During a health emergency, the ability for coordination and management structures to quickly adapt is key, as it is unlikely that the first approach taken will be the most effective. With the need to continuously adapt, it is important that transparency is maintained and that timely community communication strategies are developed.
Effective coordination is required to ensure joint planning and the evaluation of a response. Effective bi-directional communication and agility are required to navigate the complexity of the COVID-19 pandemic. While provinces need to have a level of autonomy when responding to a health emergency, there need to be strong relationships and open communication structures between the three governance tiers prior to the pandemic. Regular reviews and scenario planning would ensure that interventions are timely and best practices are disseminated.
The importance of coordination mechanisms in emergency response, cannot be overemphasised, early, decisive, and harmonised coordination are key principles needed to gain public trust and to respond to a public health emergency effectively and efficiently.
Declaration. None.
Acknowledgments. The authors acknowledge the efforts of the National Department of Health and all planners, stakeholders and decision-makers who provided the required support to respond to the COVID-19 epidemic in South Africa.
Author contributions. DM & EL conceptualised the manuscript; EL, DM, RN, YP, NG, PC, RM, WR, OPR, NM contributed to writing the manuscript; all authors edited and reviewed the manuscript.
Funding. Funding support was received from Clinton Health Access Initiative (South Africa) and the National Institute for Communicable Diseases. The funders had no role in study design, the collection, analysis and interpretation of data, the writing of the report, or the decision to submit the article for publication. All researchers were independent of funders and sponsors.
Conflicts of interest. None.
References
1. World Health Organization. 2019 Novel Coronavirus (2019-nCoV): Strategic preparedness and response plan. Geneva:WHO, 2020. [ Links ]
2. World Health Organization. COVID-19 strategic preparedness and response plan: operational planning guideline. Geneva: WHO, 2021. [ Links ]
3. Al Saidi AMO, Nur FA, Al-Mandhari AS, El Rabbat M, Hafeez A, Abubakar A. Decisive leadership is a necessity in the COVID-19 response. Lancet 2020;396(x)295-298. https://doi.org/10.1001/jama.2020.10802. [ Links ]
4. Moonasar D, Pillay A, Leonard E, et al. COVID-19: Lessons and experiences from South Africa's first surge. BMJ Glob Heal 2021;6(2):e004393. https://doi.org/10.1136/bmjgh-2020-004393 [ Links ]
5. Yin RK. Case study research, design and method. London: Sage Publications Ltd., 2009:4 [ Links ]
6. Guidance for conducting a country COVID-19 intra-action review (IAR). Geneva: World Health Organization; 2020 [ Links ]
7. National Department of Health, South Africa. Disaster Management Act, 2002. Government Gazette No. 24252: 98. 2003. [ Links ]
8. National Department of Health. Guidelines and Relief. SA Corona Virus. 2021. https://sacoronavirus.co.za/guidelines-and-relief/ (accessed 30 Dec 2021) [ Links ]
9. National Department of Health, South Africa. National Plan for COVID-19 Health Response: South Africa. 2020. [ Links ]
10. National Department of Health, South Africa. Plan of Action to Mitigate a COVID-19 Resurgence in South Africa. 2020. [ Links ]
11. World Health Organization. Emergency Response Framework (ERF). Geneva:WHO, 2017 [ Links ]
12. Cook J. Incident command in the time of COVID-19. Lab Med 2020;51(6):E78-E82. https://doi.org/10.1093/labmed/lmaa073 [ Links ]
 Correspondence:
Correspondence:
E Leonard
eleonard@clintonhealthaccess.org
Accepted 14 February 2022


{kind=link}
{kind=link}
{kind=link}