










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.6 Pretoria jun. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i6.16253
RESEARCH
Safety and efficacy of inclisiran in South African patients at high cardiovascular risk: A subanalysis of the ORION phase III clinical trials
F RaalI; M AbelsonII; S BlignautIII; L BurgessIV; S CoetzerV; I EbrahimVI; A GibbonVII; D Jansen van RensburgVIII; M JarosIX; L LombardX; E van NieuwenhuizenXI; M PretoriusXII; A van TonderXIII; D UrbachXIV
IMB BCh, PhD ; Carbohydrate and Lipid Metabolism Research Unit, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMB BCh; Vergelegen Mediclinic, Somerset West, Western Cape, South Africa
IIIMB ChB, Hons (Pharma); Paarl Research Centre, Paarl, South Africa
IVMB ChB, PhD; Tread Research, Cardiology Unit, Department of Medicine, Tygerberg Hospital and Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
VMB ChB: Accelerated Enrollment Solutions, Helderberg Clinical Research Centre, Somerset West, Western Cape, South Africa
VIMB BCh, MMed (Int Med); Netcare Unitas Hospital, Centurion, Gauteng, South Africa
VIIMed Hons, PhD; Medical Affairs, Novartis, Waterfall City, Gauteng, South Africa
VIIIMB ChB, Μ Prax Med (Fam Med); Park Medical Centre, Emalahleni, Mpumalanga, South Africa
IXPhD (Biostatistics); Summit Analytical, Denver, Colo., USA
XMB ChB, MMed (Int Med); Kuilsriver Netcare Hospital, Cape Town, South Africa
XIMB ChB; Accelerated Enrollment Solutions, Watermeyer Clinical Research Centre, Pretoria, South Africa
XIIMB ChB; Tiervlei Trial Centre, Cape Town, South Africa
XIIIPhD, MBA; Medical Affairs, Novartis, Waterfall City, Gauteng, South Africa
XIVMB ChB; Accelerated Enrollment Solutions, Helderberg Clinical Research Centre, Somerset West, Western Cape, South Africa
ABSTRACT
BACKGROUND. Inclisiran significantly reduced low-density lipoprotein cholesterol (LDL-C) in individuals with heterozygous familial hypercholesterolemia, established atherosclerotic cardiovascular disease (ASCVD) or ASCVD risk equivalents (type 2 diabetes, familial hypercholesterolaemia or a 10-year risk of a cardiovascular event >20%) in the ORION phase III clinical trials. Infrequent dosing at days 1, 90, 270 and 450 resulted in a mean LDL-C reduction of -50%. A total of 298 participants from South Africa (SA) were enrolled. Local data are needed to support the use of inclisiran in the SA population, potentially addressing an unmet need for additional LDL-C-lowering therapies.
OBJECTIVES. To analyse the ORION phase III trial data to assess the efficacy and safety of inclisiran in SA participants.
METHODS. ORION-9, 10 and 11 were randomised, double-blind, phase III trials. Participants were receiving maximally tolerated statins with or without other lipid-lowering therapies (excluding protein convertase subtilisin/kexin type 9 (PCSK9) inhibitors). Participants were randomised 1:1 to inclisiran sodium 300 mg/284 mg (free acid) or placebo administered at days 1, 90, 270 and 450. The co-primary endpoints were the LDL-C percentage change from baseline to day 510 and the time-averaged percentage change in LDL-C from baseline after day 90 up to day 540. Key secondary endpoints included the absolute change in LDL-C from baseline to day 510, the time-averaged absolute change from baseline after day 90 up to day 540, and changes in other lipids and lipoproteins.
RESULTS. The mean age of the participants was 58.6 years (56% male). The mean LDL-C level at baseline was 3.6 mmol/L. At day 510, inclisiran reduced LDL-C levels by 54.2% compared with placebo (95% confidence interval (CI) -61.3 -47.2; p<0.0001). The corresponding time-averaged reduction in LDL-C was 52.8% (95% CI -57.9 - -47.8; p<0.0001). Treatment-emergent adverse events at the injection site were more common with inclisiran compared with placebo (10.1% v. 0.7%); however, all were mild or moderate in nature and none were persistent.
CONCLUSION. Inclisiran, given in addition to maximally tolerated standard lipid-lowering therapy, is effective and safe and results in robust reductions in LDL-C in SA patients at high cardiovascular risk.
Cardiovascular disease (CVD) is the leading cause of mortality and morbidity worldwide, accounting for -18.6 million deaths in 2019.[1] In accordance, CVD is now the leading cause of non-communicable death in South Africa (SA).[2] The marked shift in the disease landscape in SA mirrors increased urbanisation and associated lifestyle behaviours. ·[4]
Well-characterised factors contributing to increased CVD risk include hypertension, obesity, tobacco use, diabetes mellitus and dyslipidaemia, among others. With a focus on hypercholesterolaemia it is important to note that the management of this condition in SA is suboptimal.[5 7] Low-density lipoprotein cholesterol (LDL-C) is a major risk factor for atherosclerotic CVD (ASCVD) and is the primary target of cholesterol-lowering therapies.[8, 10] Poor disease awareness, restricted access to high-intensity lipid-lowering therapies and clinical inertia may explain why a significant proportion of patients do not reach guideline-recommended target concentrations of LDL-C.'[5-7] The problem of hypercholesterolaemia in SA is further compounded by a founder effect in individuals of Afrikaner Jewish and South Asian Indian descent, predisposing -1 in 80 to familial hypercholesterolaemia (FH) and consequently premature ASCVD.[11] To appropriately reduce CVD risk in such patients, intense lipid-lowering therapies are generally required. However, restricted reimbursement by SA funders has limited the prescription of high-intensity statins and additional lipid-lowering therapies, such as ezetimibe. Besides financial constraints relating to cost or reimbursement, clinical inertia and the lack of ongoing educational initiatives to reaffirm guideline-recommend LDL-C targets and the use of combination therapy in uncontrolled hypercholesterolaemia may also contribute to suboptimal management strategies. Even with the optimisation of combination lipid-lowering therapies, it is not expected that all high-risk patients will attain guideline-recommended LDL-C targets, and access to additional therapies is therefore warranted.
Despite poor lipid control in SA, this therapeutic area has recently seen the development and introduction of several novel agents with the potential to address a critical unmet need. The fully humanised monoclonal antibodies (mAbs) to protein convertase subtilisin/kexin type 9 (PCSK9), alirocumab and evolocumab, are highly effective in lowering LDL-C by 50 - 60% in patients with heterozygous familial hypercholesterolaemia (HeFH) and/or established ASCVD.[12, 15] More recently, inclisiran, a small-interfering RNA (siRNA) that inhibits the production of PCSK9 in the liver, was shown to significantly reduce LDL-C compared with placebo in individuals with HeFH over 18 months of follow-up (time-averaged change -44.3%; p<0.001).[16 In addition, this agent significantly reduced LDL-C compared with placebo in those with established ASCVD (time-averaged change -53.8%; p<0.001) and/or ASCVD risk equivalents (time-averaged change -49.2%; p<0.001), as demonstrated in a series of trials of the ORION clinical phase III programme.[17] The phase III ORION trials were multinational studies, including several investigator sites in SA.
Objectives
The aim of the current study was to localise the results of the ORION phase III clinical trials by evaluating the subpopulation of SA participants independently to the global study population. In this manner, the data should support the efficacy and safety of inclisiran in this patient population.
Methods
Trial design and oversight
ORION-9 (HeFH), 10 (ASCVD) and 11 (ASCVD or ASCVD risk equivalents) were randomised, double-blind, placebo-controlled, parallel-group phase III trials (Clinicaltrials.gov numbers: NCT03397121, NCT03399370 and NCT03400800, respectively). [16·17] The detailed trial protocols were approved by the institutional review boards or independent ethics committees at each participating site and are available with the trial publications on NEJM.org. The ORION-10 study only included study sites in the USA. The aim of the current study was to analyse the trial data to assess the efficacy, safety and adverse event profile of inclisiran in a cohort of SA participants with HeFH and those with established ASCVD or ASCVD risk equivalents with elevated LDL-C levels despite maximally tolerated statin therapy (with or without additional lipid-lowering therapy). All participants provided written informed consent.
Participants
Collectively, 298 eligible participants from SA were enrolled in the ORION phase III trials. Participants presented with either established ASCVD and an LDL-C level >1.8 mmol/L or with ASCVD risk equivalents (high-risk primary prevention), including type 2 diabetes, FH or a 10-year Framingham Risk Score for CVD >20% and an LDL-C level >2.6 mmol/L. Furthermore, all participants had to be stable on a background of lipid-lowering therapies (such as statins with or without ezetimibe) for at least 30 days prior to screening. Individuals who had previously received treatment with mAbs directed against PCSK9 within 90 days prior to screening were excluded. The diagnosis of HeFH was based on genetic screening or phenotyping according to the Simon Broome criteria in ORION-9 and standard clinical criteria according to the region of the participating centres in ORION-10 and 11. Detailed inclusion and exclusion criteria are provided in Appendix 1 (https://www.samedical.org/file/1830).
Trial procedure
Participants were randomised in a 1:1 ratio to receive, in total, four doses of inclisiran sodium 300 mg (equivalent to 284 mg of inclisiran free acid) or matching placebo, administered by subcutaneous injection on days 1, 90, 270 and 450. Additional clinic visits, which involved limited laboratory assessments, were conducted on days 30, 150, 330 and 510. The last trial visit occurred 90 days after the last dose of the study drug (Fig. 1).
Endpoints
The prespecified co-primary endpoints were the LDL-C percentage change from baseline to day 510 and the time-averaged percentage change in LDL-C from baseline after day 90 up to day 540. Key secondary endpoints were the absolute change in LDL-C from baseline to day 510 and the time-averaged absolute change in LDL-C from baseline after day 90 up to day 540. In addition, the percentage changes in plasma PCSK9, apolipoprotein Β (ApoB), total cholesterol and non-high-density lipoprotein cholesterol (non-HDL-C) from baseline to day 510 were investigated. A prespecified exploratory endpoint was the proportion of participants who met the LDL-C targets for their level of cardiovascular risk at day 510.
Safety
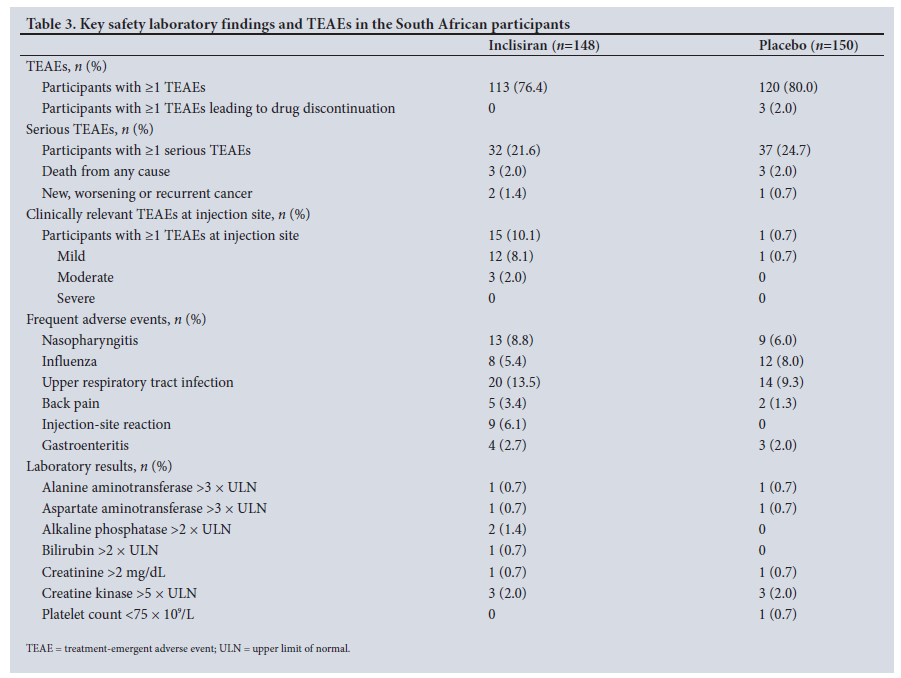
Adverse events and laboratory values were recorded for all participants at each study visit through to day 540. Treatment-emergent adverse events (TEAEs) were classified by the investigators according to organ class using the Medical Dictionary for Regulatory Activities criteria (www.meddra.org). Injection-site reactions were evaluated according to prespecified terms (mild, moderate or severe) (see Table 3).
Statistical analysis
The detailed statistical plans for the ORION phase III trials are available with the protocols at NEJM.org. The intention-to-treat population included all participants randomised in the trial and was the primary population for the efficacy analysis. The first primary endpoint was analysed using an analysis of covariance model, while the second primary efficacy endpoint was analysed using a mixed model for repeated measures.[16, 17] The primary and secondary endpoints used multiple imputation to account for missing data. Missing data were imputed for the assessment of efficacy but not safety. Results were consistent across all imputation methods/models used. Only participants who received at least one dose of either placebo or inclisiran were included in the safety population.[18]
Results
Trial population
In total, 148 SA participants were randomised to receive inclisiran while 150 were randomised to receive placebo. During the follow-up period, 14 participants (4.7%) (8 in the inclisiran group, 6 in the placebo group) discontinued the study. Baseline characteristics for the cohort are presented in Table 1. Baseline lipid-lowering therapy differed between the inclisiran and placebo groups. Specifically, a significantly greater proportion of participants in the inclisiran group were treated with high-intensity statins compared with those in the placebo group (83.8% v. 73.3%; p=0.034). Conversely, more participants in the placebo group were on treatment with ezetimibe at study entry compared with the inclisiran group (30.7% v. 20.9%; p=0.064).
For LDL-C and total cholesterol levels, the baseline value was defined as the mean of the values at screening and before receipt of the first dose of inclisiran or placebo (day 1). Race was self-reported by the participants.
Co-primary endpoints
The co-primary efficacy endpoints indicated a percentage change in LDL-C from baseline to day 510 of -46.5% (95% confidence interval (CI) -51.7 -41.3) for the inclisiran group, while an increase of 7.7% (95% CI 2.9 - 12.6) was reported for the placebo group. This translates to a between-group difference of -54.2% (95% CI -61.3 - -47.2; p<0.0001) (Fig. 2). The time-averaged percentage change in LDL-C from baseline after day 90 up to day 540 was -45.2% (95% CI -48.8 - -41.6) for the inclisiran group and 7.6% (95% CI 4.0 - 11.2) for the placebo group, resulting in a between-group difference of -52.8% (95% CI -57.9 - -47.8; p<0.0001) (Fig. 2).
Key secondary and prespecified exploratory endpoints
The absolute change in LDL-C from baseline to day 510 was -1.8 (95% CI -2.0 -1.6) mmol/L for inclisiran-treated participants, while an increase of 0.2 (95% CI 0.0 - 0.3) mmol/L was recorded for the placebo group, with a between-group difference of -2.0 (95% CI -2.2 - -1.7) mmol/L (p<0.0001) (Fig. 3). The time-averaged absolute change in LDL-C from baseline after day 90 up to day 540 was -1.6 (95% CI -1.8 - -1.5) mmol/L for the inclisiran group and 0.2 (95% CI 0.0 - 0.3) mmol/L for the placebo group, with a between-group difference of -1.8 (95% CI -2.0 -1.6) mmol/L (p<0.0001) (Fig. 3).
The results of additional secondary efficacy endpoints are shown in Table 2. Treatment with inclisiran was associated with a 59.9% (95% CI -64.7 - -55.1) reduction in plasma PCSK9 from baseline to day 510, in comparison with a 25% (95% CI 20.0 - 29.9) increase in plasma PCSK9 in the placebo group. In addition, the percentage change in total cholesterol from baseline to day 510 was -29.5% (95% CI -32.7 - -26.3) for the inclisiran group in comparison with 6.0% (95% CI 2.8 - 9.2) for the placebo group. From baseline to day 510, a reduction in ApoB of -39.8% (95% CI -43.2 - -36.5) was reported for inclisiran-treated participants, while an increase of 0.4% (95% CI -2.9 - 3.7) was recorded for the placebo group. Non-HDL-C levels were reduced by -41.5% (95% CI -45.6 - -37.5) in the inclisiran group and increased by 5.4% (95% CI 1.4 - 9.3) in the placebo group from baseline to day 510.
At day 510, the LDL-C target of <1.8 mmol/L was attained by 54.6% of participants in the inclisiran group compared with 1.5% of participants in the placebo group. Of the participants treated with inclisiran, 41.5% demonstrated LDL-C levels <1.4 mmol/L. Among the participants with established ASCVD in the inclisiran group, 53.2% had an LDL-C level <1.4 mmol/L at day 510. Similarly an LDL-C level <1.8 mmol/L was reported in 41.7% of inclisiran-treated participants with confirmed HeFH (Appendix 4, https://www.samedical.org/file/1830).
Safety and adverse events
TEAEs reported for the SA cohort are shown in Table 3. A total of 113 participants (76.4%) in the inclisiran group and 120 (80%) in the placebo group reported TEAEs during the study. TEAEs leading to drug discontinuation were reported in 3 participants (2.0%) receiving placebo. Clinically relevant injection-site adverse events were more frequent in the inclisiran group compared with the placebo group (10.1% v. 0.7%), but these were all mild or moderate in nature and none were persistent. Laboratory-defined adverse events were similar between the groups.
The safety population included all patients who received at least one dose of inclisiran or placebo. Adverse events were recorded over the trial period of 540 days.
Discussion
The ORION phase III clinical programme consisted of three trials, all of which evaluated an infrequent dosing regimen of inclisiran with regard to the percentage change in LDL-C from baseline to day 510 as well as the time-averaged percentage change in LDL-C from baseline after day 90 up to day 540.[16, 18] In addition, these trials assessed the safety profile of this novel siRNA agent over 18 months of follow-up compared with placebo. Of the total participants (N=3 660), 298 were recruited from sites across SA. The size of the SA cohort justifies publication of the results of this cohort separately from the global cohort to gain perspective on the safety and efficacy of inclisiran treatment in the SA population.
Data from the SA cohort indicate that inclisiran effectively reduced LDL-C over the trial period when administered at days 1, 90, 270 and 450. The LDL-C reduction observed in the SA cohort (between-group difference of -54.2% in LDL-C from baseline to day 510) was comparable to that observed in the pooled analysis of the phase III global studies (placebo-adjusted LDL-C reduction of -50.7% from baseline to day 510).[18]
Inclisiran treatment was well tolerated overall by the SA participants. However, an increased incidence of clinically relevant TEAEs at the injection site was reported in the inclisiran group compared with the placebo group (10.1% v. 0.7%). Importantly, the majority of these reactions were mild in nature and none were persistent. The pooled data from the global ORION cohort reported an incidence of 5.0% for injection-site TEAEs in the inclisiran group v. 0.7% in the placebo group.[18] The small sample size of the SA cohort may potentially explain the difference in injection-site reactions reported in the current analysis compared with that reported for the global cohort. The SA participants who received treatment with inclisiran contributed towards a total of 2 653 patient-years of exposure across the phase III trial programme.[18] No additional safety signals for inclisiran were detected in the SA cohort.
Several observational studies have indicated that despite awareness of current lipid guidelines on the part of healthcare professionals and limited disease awareness of hypercholesterolaemia among patients, management of the condition in SA is suboptimal.[5 7] Notable is the recently published CARDIO TRACK study, in which only 32.8% of very high-risk patients attained the LDL-C target recommended by the SA guidelines.' These local data align with international observations as presented in the recent DA VINCI study,[20] in which only 33% of patients across 18 European countries attained LDL targets as recommended by the most recently published European Society of Cardiology/European Atherosclerosis Society guidelines for the management of dyslipidaemias in 2019.[10] Although numerous factors have been identified as contributing to poor LDL-C target attainment, the most frequently cited include inappropriate use of low-intensity lipid-lowering therapy, compliance with medication, out-of-pocket costs and limited access to combination therapy.
The use of combination therapy was limited in the SA cohort, although the use of ezetimibe was greater in the SA cohort compared with the pooled global cohort (25.8% v. 14.2%).[18] Additionally, the SA cohort included more participants with confirmed HeFH (62.6%) than the global cohort (19.7%). A possible explanation is that a notable proportion of SA participants were recruited from dedicated lipid and cardiac clinics or clinical research sites associated with academic institutions. As a result, a bias may have existed towards the enrolment of HeFH patients and the aggressive treatment of lipid disorders.
The introduction of agents that effectively lower LDL-C levels while reducing treatment burden provides a means to address patient compliance in a resource-limited setting such as SA. The mAbs against PCSK9 require biweekly or monthly administration and are only registered for use in patients at high or very high risk for CVD despite maximally tolerated statins and ezetimibe.[21] With the anticipated registration of inclisiran in SA, eligible patients will have the potential to attain individualised LDL-C targets with twice-yearly administration, as demonstrated in the ORION programme. In the SA cohort, >40% of participants treated with inclisiran attained an LDL-C level <1.4 mmol/L at day 510. In contrast, this level of LDL-C reduction was not reported for any participants in the placebo group, and only 1.5% attained the LDL-C target of <1.8 mmol/L at day 510. In this regard, effective lipid-lowering therapies that require infrequent administration and are therefore more convenient may improve long-term compliance and provide the cardiovascular benefit of sustained reductions in LDL-C.'[22]
Study limitations
The limitations of the current publication must be considered. While this study provides initial insight into the response of SA patients to inclisiran treatment, the participant demographics were not truly representative of the general SA population, with limited inclusion of patients from ethnic groups other than white and a high proportion of HeFH patients. As the majority of HeFH patients enrolled in the ORION programme in SA were descended from European immigrants, one can postulate that this may have accounted for the similarity in responses between the SA participants and those in Europe and North America. Consequently, the inference of these results to the broader SA population is cautioned against. Furthermore, the SA cohort consisted of -300 participants, a sample size that may limit the ability to draw statistically meaningful conclusions. In addition, local treatment guidelines recommend the use of advanced lipid-lowering therapies such as PCSK9-directed therapies only in patients who do not reach LDL-C target after treatment with a combination of maximally tolerated high statins and cholesterol-absorption inhibitors,[21] while a limited proportion of SA participants included in the ORION programme were managed according to these recommendations. Certain data were unfortunately unavailable for the SA cohort, including information on the prespecified exploratory cardiovascular events as reported in the publications of the phase III studies.
Conclusion
Data from the SA participants enrolled in the ORION phase III clinical trials indicate that treatment with inclisiran was efficacious in reducing LDL-C and was well tolerated. These data correspond with those reported for the global ORION cohort. Future studies should prioritise the identification and enrolment of black participants to create further awareness of FH and improve our understanding of the disease and treatment responses in this ethnic group.
Declaration. None.
Acknowledgements. The authors thank Ben Stein (Summit Analytical. USA) for statistical support during the writing process.
Author contributions. All authors contributed to the conception of this publication. MJ facilitated the statistical analysis of the data. FR, AvT and AG drafted the manuscript. All authors contributed to the review of the manuscript and approved the final version to be published. Funding. Publication fees were covered by Novartis Pharma AG, South Africa.
Conflicts of interest. FR: has received fees for conducting clinical research on inclisiran from The Medicines Company, and has personally received fees from Amgen, Sanofi and Regeneran and for advisory board meetings and/or lecture contributions. MA: has received fees for conducting clinical research on inclisiran from The Medicines Company SB: has received fees for conducting clinical research on inclisiran from The Medicines Company. LB: has received fees for conducting clinical research on inclisiran from The Medicines Company, and has personally received fees from Amgen, Sanofi, Novartis and CSL Behring for advisory board meetings and lecture contributions. AG: is an employee of Novartis South Africa. MJ: has received fees for performing statistical analyses on inclisiran from The Medicines Company and Novartis. LL: has received fees for conducting clinical research on inclisiran from The Medicines Company, and has personally received fees from Novartis for advisory board meetings and/or lecture contributions. AvT: is an employee of Novartis South Africa. Other authors: no conflicts of interest to disclose.
References
1. Virani SS, Alonso A, Aparicio FH, et aL Heart disease and stroke statistics - 2021 update. Circulation 2021;143(8):e254-e743. https://doi.org/10.1161/CIR0000000000000950 [ Links ]
2. World Health Organization. Noncommunicable diseases country profiles 2018. https://www.who.int/ publications/i/item/9789241514620 (accessed 12 January 2022). [ Links ]
3. Mayosi BM, Flisher AJ, Lalloo UG, Sitas F, Tollman SM, Bradshaw D. The burden of non-communicable diseases in South Africa. Lancet 2009,374(9693):934-947. https://doi.org/10.1016/S0140-6736(09)61087-4 [ Links ]
4. Mkoko P, Naidoo S, Niazi M, et al. The spectrum prevalence and in-hospital outcomes of cardiovascular diseases in a South African district hospital. A retrospective study Cardiovasc J Afr 2021,32(5).237-242. https://doi.org/10.5830/CVJA-2021-016 [ Links ]
5. Raal F, Schamroth C, Blom D, et al. CEPHEUS SA. A South African survey on the undertreatment of hypercholesterolaemia. Cardiovascular topics. Cardiovasc J Afr 2011,22(5).234-240. https://doi.org/10.5830/CVJA-2011-044 [ Links ]
6. Raal FJ, Blom DJ, Naidoo S, Bramlage P, Brudi P. Prevalence of dyslipidaemia in statin-treated patients in South Africa! Results ofthe DYSlipidaemia International Study (DYSIS). Cardiovasc J Afr 2013,24(8).330-338. https://doi.org/10.5830/CVJA-2013-071 [ Links ]
7. Blom DJ, Raal F, Amod A, Naidoo P, Lai YY. Management of low-density lipoprotein cholesterol levels in South Africa. The International ChoLesterol management Practice Study (ICLPS). Cardiovasc J Afr 2019,30(1).15-23. https://doi.org/10.5830/CVJA-2018-054 [ Links ]
8. Klug E, Raal FJ, Marais AD, et al. South African dyslipidaemia guideline consensus statement 2018 update: A joint statement from the South African Heart Association (SA Heart) and the Lipid and Atherosclerosis Society of Southern Africa (LASSA). S Afr Med J 2018;108(11b):973-1000. https://doi.org/10.7196/SAMJ.2018.v108i11.13383 [ Links ]
9. Arnett DK, Blumenthal RS, Albert MA et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease. Executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2019,74(10).1376-1414. https://doi.Org/10.1016/j.jacc.2019.03.009 [ Links ]
10. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias. Lipid modification to reduce cardiovascular risk The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J 2020)41(1).111-188. https://doi.org/10.1093/eurheartj/ehz455 [ Links ]
11. Raal FJ, BahassiEM, Stevens B, Turner TA, Stein EA. Cascade screening for familial hypercholesterolemia in South Africa. The Wits FIND-FH Program. Arterioscler Thromb Vase Biol 2020,40(11).2747-2755. https://doi.org/10.1161/atvbaha.120.315040. [ Links ]
12. Kastelein JJP, Ginsberg HN, Langslet G, et al. ODYSSEY FH I and FH II. 78 week results with alirocumab treatment in 735 patients with heterozygous familial hypercholesterolaemia. Eur Heart J 2015,36(43).2996-3003. https://doi.org/10.1093/eurheartj/ehv370 [ Links ]
13. Raal FJ, Stein Ε A Dufour R et al. PCSK9 inhibition with evolocumab(AMG 145) in heterozygous familial hypercholesterolemia (RUTHERFORD-2). A randomised, double-blind placebo-controlled trial Lancet 2015:385(9965).331-340. https://doi.org/10.1016/S0140-6736(14)61399-4 [ Links ]
14. Sabatine MS, Giugliano RP, Keech AG et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. Ν Engl J Med 2017,376(18).1713-1722. https://doi.org/10.1056/NEJMoa1615664 [ Links ]
15. Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med 2018;379(22):2097-2107. https://doi.org/10.1056/NEJMoa1801174 [ Links ]
16. Raal FJ, Kallend D, Ray KK, et al. Inclisiran for the treatment of heterozygous familial hypercholesterolemia. Ν Engl J Med 2020,382(16).1520-1530. https://doi.org/10.1056/NEJMoa1913805 [ Links ]
17. Ray KK, Wright RS Kallend D, et al. Two phase 3 trials of inclisiran in patients with elevated LDL cholesterol. Ν Engl J Med 2020,382(16).1507-1519. https://doi.org/10.1056/NEJMoal912387 [ Links ]
18. Wright RS Ray KK Raal FJ, et al. Pooled patient-level analysis of inclisiran trials in patients with familial hypercholesterolemia or atherosclerosis. J Am Coll Cardiol 2021,77(9).1182-1193. https://doi.org/10.1016/j.jacc.2020.12.058 [ Links ]
19. Blom DJ, Ranjith N, Joshi P, et al. The therapeutic management of South African dyslipidaemic patients at very high cardiovascular risk (CARDIO TRACK). A cross-sectional study. Cardiovasc J Afr 2020:31(5):245-251. https://doi.org/10.5830/CVJA-2020-010 [ Links ]
20. Ray KK, Molemans B, Schoonen WM, et al. EU-wide cross-sectional observational study of lipidmodifying therapy use in secondary and primary care: The DA VINCI study. Eur J Prev Cardiol 2021;28(11):1279-1289. https://doi.org/10.1093/eurjpc/zwaa047 [ Links ]
21. Klug EQ, Raal FJ. New cholesterol targets for patients at high or very high cardiovascular risk and the indications for PCSK9 inhibitors. S Afr Med J 2020,110(11):1059. https://doi.org/10.7196/SAMJ.2020.v110i11.15191 [ Links ]
22. Brandts J, Ray KK. Low density lipoprotein cholesterol-lowering strategies and population health. Time to move to a cumulative exposure model. Circulation 2020,141(11).873-876. https://doi.org/10.1161/CIRCULATIONAHA.119.043406 [ Links ]
 Correspondence:
Correspondence:
F Raal
frederick.raal@wits.ac.za
Accepted 2 February 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}