










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.5 Pretoria Mai. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i5.15971
RESEARCH
Mandrax use, sexual risk, and opportunities for pre-exposure prophylaxis among out-of-school adolescent girls and young women in Cape Town, South Africa
C P BonnerI, II; F A BrowneIII, IV; T CarneyV; Ν ShangaseVI; J W NdiranguVII; B MyersVIII; W M WechsbergIX, X, XI, XII, XIII
IMS, PhD; Substance Use, Gender, and Applied Research Program, RTI International, Research Triangle Park, NC, USA
IIMS, PhD; Maternal and Child Health, Gillings School of Global Public Health, University of North Carolina at Chapel Hill, NC, USA
IIIMPH, ScD; Substance Use, Gender, and Applied Research Program, RTI International, Research Triangle Park, NC, USA
IVMPH, ScD; Maternal and Child Health, Gillings School of Global Public Health, University of North Carolina at Chapel Hill, NC, USA
VMSocSci, PhD; Alcohol, Tobacco and Other Drugs Research Unit, South African Medical Research Council, Cape Town, South Africa
VIMSPH; Maternal and Child Health, Gillings School of Global Public Health, University of North Carolina at Chapel Hill, NC, USA
VIIMSc Global Health; Use, Gender, and Applied Research Program, RTI International, Research Triangle Park, NC, USA
VIIIMSc, PhD; Alcohol, Tobacco and Other Drugs Research Unit, South African Medical Research Council, Cape Town, South Africa
IXSubstance Use, Gender, and Applied Research Program, RTI International, Research Triangle Park, NC, USA
XMS, PhD; Maternal and Child Health, Gillings School of Global Public Health, University of North Carolina at Chapel Hill, NC, USA
XIMS, PhD; Alcohol, Tobacco and Other Drugs Research Unit, South African Medical Research Council, Cape Town, South Africa
XIIMS, PhD; Department of Psychology, North Carolina State, Raleigh, NC, USA
XIIIMS, PhD; Psychiatry and Behavioral Sciences, Duke University School of Medicine, Durham, NC, USA
ABSTRACT
BACKGROUND. In South Africa (SA), adolescent girls and young women (AGYW) aged 15 - 24 years account for nearly 25% of all new HIV infections in the country. The intersection of substance use and sexual risk continues to drive the HIV epidemic among AGYW. For example, methaqualone, also known as Mandrax, has sedative effects that may affect women's ability to negotiate condom use during sex, refuse sex without a condom, or consent to sex, thereby increasing their risk for HIV. Consequently, it is critical to understand how Mandrax use affects HIV risk among AGYW and to assess awareness of and willingness to use biomedical HIV prevention methods, such as pre-exposure prophylaxis (PrEP), among AGYW who use Mandrax.
OBJECTIVES. To examine the role of Mandrax use in sexual behaviours and investigate the extent to which AGYW who use Mandrax are aware of and willing to initiate PrEP.
METHODS. Data for this report were derived from baseline and 6-month follow-up data provided by 500 AGYW participating in a cluster-randomised trial assessing the efficacy of a young woman-focused intervention to reduce substance use and HIV risk. AGYW who self-identified as black African or coloured, reported using substances, reported condomless sex in the past 3 months, and had discontinued school early were recruited from 24 community clusters across Cape Town, SA. Following consent/assent, participants provided biological specimens to test for recent drug use (including Mandrax) and completed the self-report questionnaire.
RESULTS. Logistic regression analysis revealed that the AGYW who had a positive test result for Mandrax use were less likely to use a condom with their main partner (p=0.01), and almost three times more likely to use alcohol and/or other drugs before or during their last act of sexual intercourse (p<0.001), compared with the AGYW who had a negative Mandrax test result. Mandrax use was not significantly related to PrEP awareness (p>0.10) or willingness to use PrEP (p>0.10), but 70% of AGYW who used Mandrax were willing to initiate PrEP.
CONCLUSION. The study findings highlight how Mandrax use may contribute to HIV risk among SA AGYW. Key decision-makers should consider incorporating substance use prevention efforts into existing HIV reduction programmes and equip youth-friendly clinics with the resources to identify AGYW who use Mandrax and offer them PrEP.
In South Africa (SA), an estimated 7.5 million people are living with HIV.[1] Adolescent girls and young women (AGYW) aged 15 -24 years account for nearly 25% of all new HIV infections in the country, double the figure for their male peers.[2,3] The intersection of substance use and sexual risk continues to drive the HIV epidemic among AGYW.[4-6] For example, methaqualone, also known as Mandrax, is a synthetic sedative-hypnotic that has a long history of illicit recreational use in SA and may affect HIV risk among AGYW.[7-9] Typically in SA, Mandrax tablets are crushed and mixed with cannabis and tobacco before being smoked in a pipe, called 'white pipe'. The effects of smoking Mandrax include a euphoric high followed by drowsiness, temporary unconsciousness or passing out, with potential sedation lasting up to 5 hours.[10] Given its sedative effects, Mandrax may affect women's ability to negotiate condom use during sex, refuse sex without a condom, or consent to sex, thereby increasing their risk for HIV.[6,11] Consequently, it is critical to understand how Mandrax use affects HIV risk among AGYW and to assess awareness of and willingness to use biomedical HIV prevention methods, such as pre-exposure prophylaxis (PrEP), among AGYW who use Mandrax.
Although Mandrax use is reported in all of SA's provinces, it is particularly well established in Western Cape Province, where it is consistently the third most frequently reported substance of abuse among persons entering specialist substance abuse treatment facilities.[12] Additionally, treatment utilisation data and data from community settings suggest that Mandrax use is becoming more prevalent among women.[12] Data from substance use treatment centres show that 9% of women report the use of Mandrax as a drug of concern, and 24% of non-treatment-seeking women who use substances report Mandrax use.[13,14]
Previous research has highlighted how substances such as alcohol and methamphetamine may contribute to HIV risk.[5,13] However, less is known about the effects of Mandrax on HIV risk behaviours, such as condomless sex. Understanding the link between Mandrax use and HIV risk may become increasingly important given the recent decriminalisation of cannabis in SA. In 2018, the SA government legalised the consumption of cannabis by adults in their private dwelling.[15] As Mandrax is typically smoked with cannabis, it is plausible that this cannabis policy change may increase the use of Mandrax, although to date this has not been empirically demonstrated.[7,15]
Since AGYW are at increased risk for HIV, they also are a priority population for the provision of PrEP to curtail the HIV epidemic.[16] Recently, the Joint United Nations Programme on HIV/ AIDS (UNAIDS) established the goals of ensuring that 95% of people at risk for HIV use a combination of prevention strategies and that 95% of women have access to sexual and reproductive healthcare, including PrEP.[17] Recent estimates show that between 20% and 50% of AGYW in SA are aware of PrEP and ~50% would be willing to take PrEP; however, very few have taken PrEP.[18,19] The lack of PrEP uptake may be attributed to the slow roll-out of PrEP in SA. Although SA approved the use of PrEP in 2015, it has only recently been available in public clinics. If the UNAIDS goal is achieved among AGYW, PrEP has the potential to have a significant impact on community-level HIV risk.[20] Given the increased awareness of PrEP among AGYW and the increase in availability of PrEP in SA, it is important to understand the demand for PrEP among AGYW who are at increased risk for HIV acquisition, such as those who use Mandrax.
Objectives
This study aimed to examine the role of Mandrax use in sexual behaviours and investigate the extent to which AGYW who use Mandrax are aware of and willing to initiate PrEP.
Methods
Design
Data for this report were derived from baseline and 6-month follow-up data provided by participants in a cluster-randomised trial assessing the efficacy of a young-woman-focused intervention to reduce substance use and HIV risk, the Young Women's Health CoOp. The published protocol describes the study design and procedures in detail.[21]
Setting
Participants were recruited from 24 community clusters across Cape Town, SA. Twelve communities comprised predominantly individuals who self-identify as black African and 12 communities comprised predominantly individuals who self-identify as coloured (mixed race) - racial categories created during the apartheid era in SA. All communities were in areas that have been historically disadvantaged, in part as a result of apartheid-era policies.
Participants and recruitment
Trained study outreach staff recruited AGYW into the study individually, ensuring privacy and confidentiality, with the assistance of AGYW peers. Study staff were multilingual in English, Afrikaans and/or isiXhosa, three prevalent languages spoken in Western Cape. Eligibility criteria included AGYW who: (i) were between 16 and 19 years old; (ii) self-identified as a woman; (iii) reported consuming 2 - 3 alcoholic drinks at least once in the past 30 days or using illicit drugs at least once a week in the past 30 days; (iv) currently dropped out of school; (v) had been out of school for at least 6 months; (vi) had not completed grade 12 (high school) or did not have an N3 (National Technical Certificate); (vii) reported condomless sex with a male partner in the past 90 days; (viii) reported living in one of the target communities; (ix) had lived in the target community for at least 6 months; (x) planned to reside in the target community for the next year and could provide verifiable locator information; and ( xi) provided verbal and written consent/assent. Additionally, a short cognitive test was given at the end of the eligibility screening and individuals were excluded if they had a score indicative of cognitive impairment. The study enrolled a total of 500 AGYW
Procedures
Individuals who were eligible and interested in participating in the study were scheduled for an intake appointment. During intake, young women were rescreened to ensure eligibility before continuing with the informed consent/assent process. Participants aged >18 years provided consent, whereas participants aged 16 or 17 provided assent and were required to obtain written permission to participate via an in loco parentis consent procedure. The in loco parentis consent procedure required the AGYW to receive permission from an older (>25 years) trusted woman who they identified, or a woman in the community selected by community stakeholders and the research team in place of their parent.[22]
Following consent/assent, participants underwent a breathalyser test for recent alcohol use and provided locator information to be used to contact them for follow-up. They then completed the baseline questionnaire via computer-assisted personal-interviewing technology and via audio computer-assisted self-interviewing for sensitive topics, such as experiences of abuse. Participants could complete the questionnaire in their choice of English, Afrikaans or isiXhosa. Next, participants provided urine samples for pregnancy testing and screening for recent drug use, including cannabis, Mandrax, opiates and MDMA (Ecstasy). Participants completed rapid HIV testing and counselling, following procedures and protocols approved by the SA Department of Health.[23] This enrolment visit lasted ~2 hours and all participants were scheduled to return at 6 and 12 months post intake for follow-up assessments. Participants were remunerated ZAR150 (~USD10) for their time and were provided with referrals to other services when needed. Participants who were in communities randomised to the intervention were scheduled to attend two intervention workshops, spaced ~1 week apart. Intervention workshops included content on reducing alcohol and other drug use, condom negotiation and use, and preventing violence. The intervention did not include content about PrEP. All procedures were approved by ethics review boards at RTI International (ref. no. 13790) and the South African Medical Research Council (ref. no. EC006-3/2016). This article reports data from the baseline and 6-month follow-up appointments.
Measures Baseline measures
Participants' condom use with a main partner and other sexual partner were assessed separately. AGYW were asked whether they used a condom during their last sex act with their boyfriend, and during their last sex act with any partner. Responses were dichotomous. Participants' use of alcohol or other drugs before or during their last sex act was also assessed. Additionally, based on the results of the urine drug screen, participants were coded as 1 = positive or 0 = negative for Mandrax use.
Six-month follow-up measures
At the time of baseline data collection, the guidelines for the provision of PrEP were not finalised in SA. Measures of PrEP awareness and willingness to initiate PrEP were therefore collected at the 6-month follow-up appointment for all participants. Participants' awareness of PrEP was assessed by asking if they had ever heard of PrEP. After participants responded to the item assessing PrEP awareness, they were given a brief description of PrEP including information about effectiveness, adherence requirements and side-effects. Participants were then asked if they would be willing to take PrEP if it were readily available for free (1 = yes, 0 = no).
Covariates
Based on bivariate analyses, education (i.e. completion of standard 6 (grade 8) or less v. standard 7 (grade 9) or higher) was included in the model as a covariate.
Analysis
We used Stata version 15 (StataCorp, USA) for all the analyses. Descriptive analyses were performed, and we then explored the associations among the variables of interest (condom use, use of alcohol or drugs before or during last sex act, and Mandrax use) and the conceptually meaningful covariates. Next, separate logistic regression models were conducted to explore the association between biomarker-confirmed Mandrax use and condom use at last sex with a boyfriend, condom use at last sex with a non-main partner, and use of alcohol or other drugs before or during the participant's last sex act, with odds ratios indicating effect sizes. All analyses controlled for clustering at the community level using a robust cluster estimator. p-values <0.05 and 95% confidence intervals (CIs) that did not include 1 indicated statistical significance.
Results
Description of sample
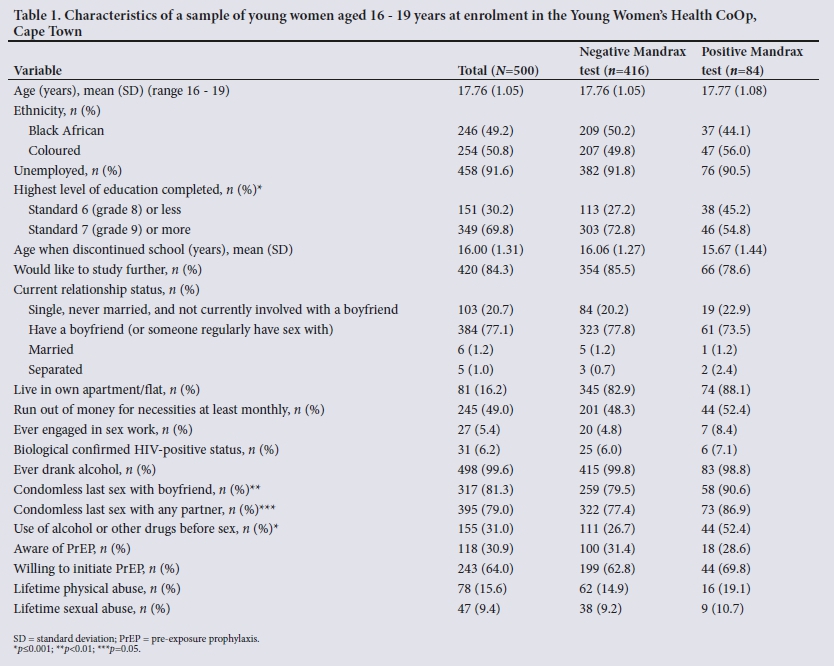
The baseline sample comprised 500 SA AGYW who reported engaging in substance use and who had left school (Table 1). The 6-month follow-up rate was 95% (n=477). At baseline, ~51% of the AGYW in the study self-identified as coloured and the mean (standard deviation (SD)) age was 17.8 (1.1) years. The majority (92%) of the AGYW were unemployed and 49% reported running out of money for necessities at least monthly. Among the AGYW, 17% tested positive for Mandrax use. Approximately 31% of the AGYW had heard of PrEP and 64% reported that they would be willing to take PrEP. Most of the AGYW were hopeful for their future, as indicated by a mean (SD) score of 31.69 (5.7) on an adapted future orientation scale.[24]
Main findings
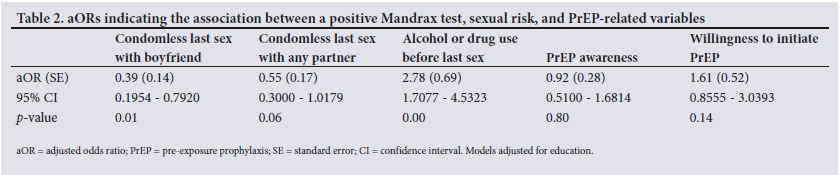
Logistic regression analysis revealed that the AGYW who had a positive test result for Mandrax use were less likely to use a condom during last sex with any partner (adjusted odds ratio (aOR) 0.55; 95% CI 0.30 - 1.02; p=0.06) and with their main partner (aOR 0.39; 95% CI 0.20 - 0.79; p=0.01) compared with the AGYW who had a negative Mandrax test result (Table 2). The AGYW who tested positive for Mandrax use were also almost three times more likely to use alcohol and/or other drugs before or during their last act of sexual intercourse (OR 2.78; 95% CI 1.71 - 4.53; p<0.001). Mandrax use was not significantly related to PrEP awareness (p>0.10) or willingness to use PrEP (p>0.10). However, among the AGYW who had a positive test result for Mandrax use, 29% had heard of PrEP and 70% reported that they would take PrEP if it was freely available.
Discussion
SA has a considerable disease burden attributable to substance use and HIV, and a substantial number of individuals affected are AGYW.[1,12,25-28] Previous research has illustrated the association between substance use and sexual risk among AGYW; however, few studies have examined the link between Mandrax use and sexual risk, especially in this population.[4,5,13,29] Furthermore, no research to date has examined PrEP awareness and willingness to initiate PrEP among AGYW who use Mandrax. Mandrax use as an illicit drug is prevalent in SA,[30] and understanding the effects of Mandrax on sexual risk is particularly timely given the recent legalisation of cannabis in SA.[15] Given that Mandrax is often combined with tobacco, marijuana or other drugs and smoked through a pipe,[30] the use of Mandrax may increase. The effects of Mandrax, such as intense drowsiness, may increase the risk of sexual assault or condomless sex, which may increase HIV risk among vulnerable populations such as AGYW.[6,11] The present study contributes to the literature by examining the association between Mandrax use and sexual risk, and awareness of and willingness to initiate PrEP among SA AGYW.
Statement of principal findings
The study findings suggest that Mandrax use may be negatively related to condom use with a main partner and positively related to using alcohol and other drugs before sex. Additionally, we did not find a statistically significant association between Mandrax use and PrEP awareness or willingness to initiate PrEP. However, among the AGYW who used Mandrax, only 29% were aware of PrEP, but the majority were willing to initiate PrEP after they were educated about it.
Our findings also highlight that the association between Mandrax use and condom use with a main partner is novel. This finding aligns with the tradition of methaqualone as 'heroin for lovers' and indicates there is a belief that Mandrax may be a 'love drug' leading to less inhibition during sex.[31] The idea of less inhibited sex may involve condomless sex, which may increase HIV risk among AGYW, an already vulnerable population. This study illustrates the need for and potential benefit of further examining the link between sexual risk and Mandrax use among AGYW in SA. Additionally, our findings indicate a need for HIV prevention efforts to include and prioritise AGYW who use substances, such as Mandrax.
We also demonstrated the association between Mandrax use and alcohol or other drug use before sex. This finding is important for several reasons. If AGYW are using Mandrax before sex, they may be more likely to engage in condomless sex. Additionally, using Mandrax in a context where sex is possible but not imminent has the potential to contribute to non-consensual sex or impair the ability of AGYW to negotiate for condom use or actively consent to certain aspects of the sexual experience.[32] Although we did not assess participants' frequency of combining alcohol and Mandrax, this combination has proven fatal. Consequently, HIV prevention efforts should educate AGYW on the effects of Mandrax and how Mandrax and/or other drug use may affect their ability to have control over their sexual experience and increase their HIV risk.
Finally, we found that most AGYW in our sample had not heard of PrEP but were willing to initiate PrEP once it became widely and freely available. We did not demonstrate a link between Mandrax use and PrEP awareness or willingness to use PrEP. This finding indicates that there is no difference between the awareness or demand for PrEP between AGYW who use Mandrax and AGYW who do not. Consequently, PrEP demand-creation activities should include and prioritise AGYW who use substances, especially those who use substances that increase their HIV risk, such as Mandrax and methamphetamine.[5,13]
Study strengths and limitations
The present study is among a very few to explore the association between Mandrax use and sexual risk among vulnerable AGYW in Cape Town. Examining Mandrax use as a correlate of sexual risk is a particular strength of this study, given the prevalence of HIV among SA AGYW, the increasing prevalence of Mandrax use among women, and the recent legalisation of cannabis in SA.[1,12,15] Additionally, to our knowledge, this is the first study to examine PrEP awareness and willingness to initiate PrEP among AGYW who use alcohol or other drugs. Furthermore, our focus on out-of-school AGYW - a hard-to-reach population that has been understudied regarding their Mandrax use - is a strength. Understanding substance use and sexual risk in this population is important given their role in HIV risk and unintended pregnancy among AGYW in SA.[33] Also, our study sample was recruited from SA communities, which strengthens the external validity of the findings. Additionally, in terms of measurement, we used assessments that have been utilised and validated in similar samples in SA.[5] Finally, we assessed recent Mandrax use using a urine drug screen, which typically detects drug metabolites and is more accurate than self-report. Collectively, these strengths contribute to the validity of our findings.
The findings and implications of this study should be viewed in the light of several study limitations. First, the data for this study were drawn from baseline and 6-month follow-up data of a larger trial examining the efficacy of a young-woman-focused HIV prevention intervention; consequently, causality cannot be inferred. Therefore, longitudinal assessments of Mandrax use and sexual risk are necessary for future research to understand the causality of these associations. Second, the assessment of sexual risk focused on participants' last sex act. Although the last sex act may be easier to recall for participants and does indicate their risk level, assessing sexual risk over a longer recall period, such as 30 days, may provide a more accurate depiction of risk. Future research should examine these associations using methods such as the Timeline Follow-back method to evaluate drug use and sexual risk over a longer period.[34] Third, the biological assessment of recent substance use also has some limitations. While rapid urine drug screens are more reliable than self-report, there is the risk of false-positives caused by secondary exposure to cannabis.[35] We did not conduct a comprehensive assessment of the second-hand exposure to cannabis smoke and consequently could not address this risk. Fourth, we assessed PrEP awareness and willingness to use PrEP during participants' 6-month follow-up. Although it would have been ideal to assess PrEP-related variables and Mandrax use at the same timepoint, the SA PrEP guidelines were not finalised at the time of baseline data collection, indicating that the national roll-out had not commenced. However, by using Mandrax use at baseline to predict PrEP awareness and willingness to use PrEP at 6-month follow-up, we can infer temporality. Lastly, we did not assess how the composition of Mandrax that AGYW reported using was related to their sexual behaviour. Mandrax is often mixed with cannabis and/ or other substances and smoked.[26] It will therefore be important for future research to understand how the composition of Mandrax plus other substances may differentially affect AGYW's sexual risk. These limitations notwithstanding, this study adds to the existing literature and serves as a basis to explore the nuanced associations between Mandrax use and sexual risk among AGYW in Cape Town.
Study contributions
This study helps bridge the gap in the literature examining Mandrax use and sexual risk among vulnerable AGYW in SA.[13] Overall, the findings demonstrate the link between Mandrax and condomless sex and also showed willingness to initiate PrEP among SA AGYW. Recently, this population has received much attention related to the need for HIV prevention because of a high HIV incidence in this group. Also, access to reproductive health services to reduce unintended pregnancy among AGYW is of great concern in SA. Our findings suggest that AGYW who use alcohol and other drugs should be prioritised in policy that guides these efforts and that HIV prevention education should include content related to the effects of alcohol and other drugs on sexual risk.
Clinical and policy implications and recommendations
The study findings have practical and policy implications. Recently, SA has begun to make PrEP widely available in public health clinics through youth-friendly clinics, and has ~165 000 PrEP users.[36,37] Our findings highlight the need to address substance use and sexual risk among AGYW and to integrate services as an efficient way to address these public health issues. Public health clinics that provide more youth-friendly services may be ideal settings for integrated care to educate youth about the effects of Mandrax use and treat substance use disorders among youth who are already using drugs such as Mandrax. The results of the current study suggest that government stakeholders should consider providing additional resources to youth-friendly clinics and extending clinics' efforts to increase the provision of youth-friendly services to include substance use education and treatment. Additionally, screening for substance use may enable providers to identify individuals who may benefit from PrEP. For example, if a nurse can identify an AGYW who is using Mandrax, she could offer her PrEP.
Conclusion
Our findings highlight how Mandrax use may contribute to HIV risk among SA AGYW. Efforts seeking to reduce HIV among AGYW may consider addressing substance use, especially drugs such as Mandrax. Key decision-makers may want to consider incorporating substance use prevention efforts into existing programmes that seek to reduce HIV, and to equip youth-friendly clinics with the resources to identify AGYW who use Mandrax and offer them PrEP. Addressing substance use among AGYW is an essential component of reducing HIV among this population.
Declaration. None.
Acknowledgements. We acknowledge the contributions of the project staff and the young women who participated in the study. We would also like to acknowledge Jeff Novey for his contributions as copy editor.
Author contributions. All authors participated in the research and article preparation. WMW conceived the study, oversaw drafts, and finalised the manuscript; CPB conducted the analyses and led the development of the manuscript; TC, FAB, JWN, NS and BM contributed to writing and reviewing the manuscript.
Funding. This work was supported by the National Institutes of Health, National Institute on Drug Abuse under grant no. R01DA041227-03S1. The funding source had no role in the analysis of the data, in writing the report, or in the decision to submit the article for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. A portion of this paper was presented during a poster presentation at the Society for Behavioral Medicine Virtual Conference on 12 - 16 April 2021.
Conflicts of interest. None.
References
1. Joint United Nations Programme on HIV and AIDS (UNAIDS). Country factsheet: South Africa. Geneva: UNAIDS; 2020. https://www.unaids.org/en/regionscountries/countries/southafrica (accessed 15 August 2021). [ Links ]
2. Simbayi LC, Zuma K, Zungu N, et al. South African National HIV Prevalence, Incidence, Behaviour and Communication Survey, 2017. Cape Town: HSRC Press, 2019. http://www.hsrc.ac.za/uploads/pageContent/10779/SABSSM%20V.pdf (accessed 15 August 2021). [ Links ]
3. Joint United Nations Programme on HIV and AIDS (UNAIDS). Global epidemic update: Communities at the centre. Geneva: UNAIDS, 2019. https://www.unaids.org/sites/default/files/media_asset/2019-global-AIDS-update_en.pdf (accessed 3 July 2021). [ Links ]
4. Bello B, Moultrie H, Somji A, Chersich MF, Watts C, Delany-Moretlwe S. Alcohol use and sexual risk behaviour among men and women in inner-city Johannesburg, South Africa. BMC Public Health 2017;17(Suppl 3):548. https://doi.org/10.1186/s12889-017-4350-4 [ Links ]
5. Wechsberg WM, Jones HE, Zule WA, et al. Methamphetamine ('tik') use and its association with condom use among out-of-school females in Cape Town, South Africa. Am J Drug Alcohol Abuse 2010;36(4):208-213. https://doi.org/10.3109/00952990.2010.493592 [ Links ]
6. Peltzer K, Simbayi L, Kalichman S, Jooste S, Cloete A, Mbelle N. Drug use and HIV risk behaviour in three urban South African communities. J Soc Sci 2009;18(2):143-149. https://doi.org/10.1080/09718923.2009.11892675 [ Links ]
7. Bhana A, Parry CDH, Myers B, Plüddemann A, Morojele NK, Flisher AJ. The South African Community Epidemiology Network on Drug Use (SACENDU) project, phases 1 - 8 - cannabis and Mandrax. S Afr Med J 2002;92(7):542-547. [ Links ]
8. Gerald MC, Schwirian PM. Nonmedical use of methaqualone. Arch Gen Psychiatry 1973;28(5):627-631. https://doi.org/10.1001/archpsyc.1973.01750350011002 [ Links ]
9. Harker N, Lucas WC, Laubscher R, Dada S, Myers B, Parry CD. Is South Africa being spared the global opioid crisis? A review of trends in drug treatment demand for heroin, nyaope and codeine-related medicines in South Africa (2012 - 2017). Int J Drug Policy 2020;83:102839. https://doi.org/10.1016/j.drugpo.2020.102839 [ Links ]
10. McCarthy G, Myers B, Siegfried N. Treatment for methaqualone dependence in adults. Cochrane Database Syst Rev 2005, Issue 2. Art. No.: CD004146. https://doi.org/10.1002/14651858.CD004146.pub2 [ Links ]
11. Norris W, Nisbet H. Oral premedication: A study of the sedative effects of Mandrax. Br J Anaesth 1966;38(11):886-890. https://doi.org/10.1093/bja/38.11.886 [ Links ]
12. Dada S, Harker Burnhams N, Erasmus J, et al. Research Brief: Monitoring Alcohol, Tobacco, and other Drug Abuse Treatment in South Africa: July - December 2019 | Phase 47, 2019. South African Community Epidemiology Network on Drug Use, November 2020. https://www.samrc.ac.za/sites/default/files/attachments/2020-11-18/SACENDUFullReportPhase47.pdf (accessed 19 July 2021). [ Links ]
13. Wechsberg WM, Myers B, Kline TL, Carney T, Browne FA, Novak SP. The relationship of alcohol and other drug use typologies to sex risk behaviors among vulnerable women in Cape Town, South Africa. J AIDS Clin Res 2012;S1:015. https://doi.org/10.4172/2155-6113.S1-015 [ Links ]
14. Dada S, Burnhams NH, Laubscher R, Parry C, Myers B. Alcohol and other drug use among women seeking substance abuse treatment in the Western Cape, South Africa. S Afr J Sci 2018;114(9-10):1-7. https://doi.org/10.17159/sajs.2018/4451 [ Links ]
15. Parry C, Myers B, Caulkins J. Decriminalisation of recreational cannabis in South Africa. Lancet 2019;393(10183):1804-1805. https://doi.org/10.016/S0140-6736(19)30011-X [ Links ]
16. US President's Emergency Plan for AIDS Relief (PEPFAR). DREAMS: Partnership to reduce HIV/ AIDS in adolescent girls and young women. USAID, 2021. www.usaid.gov/global-health/health-areas/hiv-and-aids/technical-areas/dreams (accessed 19 July 2021). [ Links ]
17. Joint United Nations Programme on HIV/AIDS (UNAIDS). 2025 AIDS targets: Putting people living with HIV and communities at risk at the centre. 2021. https://aidstargets2025.unaids.org/ (accessed 12 August 2021). [ Links ]
18. Ajayi AI, Mudefi E, Yusuf MS, Adeniyi OV, Rala N, Goon DT. Low awareness and use of pre-exposure prophylaxis among adolescents and young adults in high HIV and sexual violence prevalence settings. Medicine 2019;98(43):e17716. https://doi.org/10.1097/MD.0000000000017716 [ Links ]
19. Shamu S, Shamu P, Khupakonke S, et al. Pre-exposure prophylaxis (PrEP) awareness, attitudes and uptake willingness among young people: Gender differences and associated factors in two South African districts. Glob Health Action 2021;14(1):1886455. https://doi.org/10.1080/16549716.2021.1886455 [ Links ]
20. Mudimu E, Peebles K, Mukandavire Z, et al. Individual and community-level benefits of PrEP in western Kenya and South Africa: Implications for population prioritization of PrEP provision. PLoS ONE 2020;15(12):e0244761. https://doi.org/10.1371/journal.pone.0244761 [ Links ]
21. Wechsberg WM, Browne FA, Carney T, et al. The Young Women's Health CoOp in Cape Town, South Africa: Study protocol for a cluster-randomised trial for adolescent women at risk for HIV. BMC Public Health 2018;18:859. https://doi.org/10.1186/s12889-018-5665-5 [ Links ]
22. Bonner CP, Carney T, Browne FA, et al. 'Because all mothers is not the same': The development and implementation of an in loco parentis informed consent procedure to enroll adolescent girls and young women in participate in HIV research. J Adolesc 2021;93(1):234-244. https://doi.org/10.1016/j.adolescence.2021.11.001 [ Links ]
23. National Department of Health, South Africa. National HIV testing services: Policy. Pretoria: NDoH, 2016. https://sahivsoc.org/Files/HTS%20Policy%2028%20July%20final%20copy.pdf (accessed 19 July 2021). [ Links ]
24. Lippman L, Guzman L, Moore KA. Measuring flourishing among youth: Findings from the flourishing children positive indicators project. Child Trends, 19 July 2012. http://www.childtrends.org/wp-content/uploads/2013/05/FlourishingChildren.pdf (accessed 19 July 2021). [ Links ]
25. Abdool Karim Q, Ayesha K. Epidemiology of HIV/AIDS. In: Hall JC, Hall BJ, Cockerell CJ, eds. HIV/ AIDS in the Post-HAART Era: Manifestations, Treatment, and Epidemiology. 1st ed. Beijing, China: People's Medical Publishing House, 2011: chapter 5. [ Links ]
26. Peltzer K, Phaswana-Mafuya N. Drug use among youth and adults in a population-based survey in South Africa. S Afr J Psychiatry 2018;24:a1139. https://doi.org/10.4102/sajpsychiatry.v24i0.1139 [ Links ]
27. Degenhardt L, Stockings E, Patton G, Hall WD, Lynskey M. The increasing global health priority of substance use in young people. Lancet Psychiatry 2016;3(3):251-264. https://doi.org/10.1016/S2215-0366(15)00508-8 [ Links ]
28. Degenhardt L, Charlson F, Ferrari A, et al. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990 - 2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry 2018;5(12):987-1012. https://doi.org/10.6/S2215-0366(18)30337-7 [ Links ]
29. Stephens TT, Gardner D, Jones K, Sifunda S, Braithwaite R, Smith SE. Correlates of Mandrax use and condom beliefs in preventing sexually transmitted infections among a cohort of South African prison inmates. Int Health 2016;8(2):142-147. https://doi.org/10.1093/inthealth/ihv048 [ Links ]
30. Peltzer K, Ramlagan S, Johnson BD, Phaswana-Mafuya N. Illicit drug use and treatment in South Africa: A review. Subst Use Misuse 2010;45(13):2221-2243. https://doi.org/10.3109/10826084.2010.481594 [ Links ]
31. Inaba DS, Gay GR, Newmeyer JA, Whitehead C. Methaqualone abuse: 'Luding out'. JAMA 1973;224(11):1505-1509. https://doi.org/10.1001/jama.1973.03220250027010 [ Links ]
32. Cooper ML, Orcutt HK. Drinking and sexual experience on first dates among adolescents. J Abnorm Psychol 1997;106(2):191-202. https://doi.org/10.1037//0021-843x.106.2.191 [ Links ]
33. Myers B, Carney T, Wechsberg WM. 'Not on the agenda': A qualitative study of influences on health services use among poor young women who use drugs in Cape Town, South Africa. Int J Drug Policy 2016;30:52-58. https://doi.org/10.1016/j.drugpo.2015.12.019 [ Links ]
34. Midanik LT, Hines AM, Barrett DC, Paul JP, Crosby GM, Stall RD. Self-reports of alcohol use, drug use and sexual behavior: Expanding the Timeline Follow-back technique. J Stud Alcohol 1998;59(6):681-689. https://doi.org/10.15288/jsa.1998.59.681 [ Links ]
35. Hadland SE, Levy S. Objective testing: Urine and other drug tests. Child Adolesc Psychiatr Clin N Am 2016;25(3):549-565. https://doi.org/10.1016/j.chc.2016.02.005 [ Links ]
36. National Department of Health, South Africa. National Adolescent & Youth Health Policy 2017. 2017. https://www.datocms-assets.com/7245/1574921711-national-adolescent-and-youth-health-policy-2017.pdf (accessed 19 July 2021). [ Links ]
37. PrEPWatch. South Africa: A snapshot of PrEP scale-up, registration, and resources for South Africa. 2021. https://www.prepwatch.org/country/south-africa/ (accessed 5 July 2021). [ Links ]
 Correspondence:
Correspondence:
C P Bonner
cpbonner@rti.org
Accepted 1 February 2022


{kind=link}
{kind=link}