










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.4 Pretoria abr. 2022
http://dx.doi.org/10.7196/samj.2022.v112i4.15967
RESEARCH
High prevalence of multimorbidity and non-communicable disease risk factors in South African adolescents and youth living with HIV: Implications for integrated prevention
M KamkuemahI; B GausiII; T OniIII, IV
IMPH, PhD; Research Initiative for Cities Health and Equity (RICHE), Division of Public Health Medicine, School of Public Health and Family Medicine., University of Cape Town, South Africa
IIMD, MPH; Research Initiative for Cities Health and Equity (RICHE), Division of Public Health Medicine, School of Public Health and Family Medicine., University of Cape Town, South Africa
IIIMD, PhD; Research Initiative for Cities Health and Equity (RICHE), Division of Public Health Medicine, School of Public Health and Family Medicine., University of Cape Town, South Africa
IVMD, PhD; Medical Research Council Epidemiology Unit, University of Cambridge, UK
ABSTRACT
BACKGROUND: Adolescents and youth living with HIV (AYLHIV) face an elevated non-communicable disease (NCD) risk resulting from HIV, psychosocial challenges, and the complications of antiretroviral therapy
OBJECTIVES: To investigate the prevalence of common NCDs and their risk factors among AYLHIV in urban Cape Town, South Africa, in order to inform an integrated approach to NCD screening and prevention in AYLHIV
METHODS: We conducted a cross-sectional study in six primary care facilities in Cape Town between March 2019 and January 2020. We collected sociodemographic information, and assessed dietary intake, physical activity and nutritional knowledge. We also screened for pre-existing and previously unidentified NCDs and modifiable risk factors in 92 adolescents and youth receiving treatment for HIV in primary care settings using self-report and objective measures. Differences between sexes and age groups were compared using parametric and non-parametric statistical tests
RESULTS: Three out of four participants were female, and the median (interquartile range) age was 20.5 (18.9 - 22.9) years. More than a quarter were not in education, employment or training, and 44% were multidimensionally poor. Five percent of participants had measured hypertension, and 37% had central obesity. AYLHIV self-reported high levels of household food insecurity (70%), low daily fruit and vegetable consumption (28% and 52%, respectively), high refined sugar and sugar-sweetened beverage intake (31% and 29% daily intake, respectively), regularly skipping breakfast (42%), low nutritional knowledge (37% average score) and insufficient weekly physical activity levels (31%). A third (30%) were current smokers, and 24% engaged in binge drinking
CONCLUSIONS: Our findings of a high prevalence of NCDs and risk factors in AYLHIV highlight the importance of NCD risk screening as part of HIV care for AYLHIV. Such integrated approaches are needed to achieve the dual purpose of improving outcomes through early diagnosis of pre-existing NCDs as well as the prevention of NCD multimorbidity in AYLHIV. This study further demonstrates the need for early intervention on the social, environmental and economic determinants of NCDs targeting adolescents and youth
Globally, non-communicable diseases (NCDs) are the leading cause of disability and premature mortality, accounting for 71% of deaths worldwide and 80.6% of years lived with disability in 2016.[1] NCDs affect low- and middle-income countries (LMICs) disproportionately, with more than three-quarters of NCD deaths occurring in LMICs.[2] In 2017, the burden of NCDs in sub-Saharan Africa (SSA) was higher than the global average, almost equivalent to the total burden associated with communicable, maternal, neonatal and nutritional diseases.[3] Of note, unhealthy diets and physical inactivity, which are significantly associated with cardiometabolic conditions and cancers, are rising globally,[1,4] especially among the poor residing in urban LMIC settings.[5] South Africa (SA) also has the largest HIV epidemic and the largest antiretroviral treatment (ART) programme globally, with 7.5 million people living with HIV in 2019 and 5.2 million on ART.[6] Of note, SA also has the highest burden of adolescent HIV globally[7]
Against this background, the prevalence of NCDs and NCD risk factors has increased over the past two decades. The prevalence of overweight and obesity among adult women increased from 56% to 68% between 1998 and 2016.[8] One in three SA adults has hypertension, 12.8% have diabetes,[8] 16.2% smoke daily,[9] and 18.3% engage in binge drinking.[10] SA also has the highest prevalence of childhood and adolescent overweight and obesity in SSA (19% of boys and 26% of girls aged <20 years).[11] Furthermore, >40% of young South Africans have insufficient levels of physical activity,[12] and 20% consume sugar-sweetened beverages (SSBs) daily.[9] Moreover, HIV and ART are associated with several NCDs. Evidence of rising prevalences of both NCD comorbidities[13] and NCD risk factors such as physical inactivity[14] and smoking[15] has been documented in adults living with HIV, with an excess burden of NCD risk factors compared with the general population. Similarly, adolescents and youth living with HIV (AYLHIV) face elevated health risks with similar comorbidity patterns to adults due to HIV and long-term ART.[16,17]
Even though many risk behaviours for NCDs are initiated or reinforced in adolescence,[18] little is known about NCD risk and comorbidity patterns in AYLHIV. Given that AYLHIV routinely access care and are potentially additionally vulnerable to NCDs compared with their age peers, there is an opportunity for early intervention to identify risk factors and prevent other comorbidities. However, there has been little focus on NCD prevention in AYLHIV. A previous folder review of AYLHIV conducted by the authors in the same urban setting identified limited integration of NCD screening and health promotion in adolescent HIV healthcare services,[19] raising questions about the true prevalence of NCD multimorbidity and NCD risk factors in AYLHIV.
Objectives
Given the emerging NCD epidemic in SSA and increased comorbidity risk in people living with HIV (PLHIV), this study aimed to measure the prevalence of commonly occurring cardiometabolic NCDs and risk factors in AYLHIV accessing primary healthcare in Cape Town, SA, in order to inform a comprehensive, integrated approach to NCD screening and prevention in AYLHIV.
Methods
Study setting and population
We conducted a cross-sectional study of AYLHIV aged 15-24 years attending primary care health facilities in Cape Town. Cape Town is the second-biggest city in SA, with an estimated population of 4 million people, of whom 16.3% are aged 15 - 24 years.[20] NCDs, including diabetes mellitus, ischaemic heart disease, cerebrovascular disease and HIV, are ranked among the top five causes of premature death in Cape Town.[21] Recruitment and data collection took place at six public sector HIV clinics located in four legislated health substructures in the city. These facilities serve patients living in periurban, high-density, low-income townships.
Study design and sampling
The sample size was determined using prevalence estimates for youth aged 15-24 years, for whom data are readily available.[9] The confidence level was set at 95%, with a 5% degree of precision and an obesity prevalence of 5.6%, yielding a minimum required sample size of 82. We previously described the method used to estimate the number of AYLHIV accessing care at each facility.[19] Study procedures were conducted at each clinic using a convenience sampling approach from March 2019 until January 2020.
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki. Ethical clearance was obtained from the Human Research Ethics Committee in the Faculty of Health Sciences at the University of Cape Town (ref. no. HREC 520/2017) and the health research ethics committees of the City of Cape Town and the Western Cape provincial government. Parents or legal guardians provided written consent for their children to participate in the study, and participants provided written informed assent (or consent if aged >18 years).
The data that support the findings of this study are not publicly available owing to the sensitive nature of the information that could compromise minor research participants' privacy/consent, but are available from the corresponding author MK on reasonable request.
Study procedures
Sociodemographic characteristics
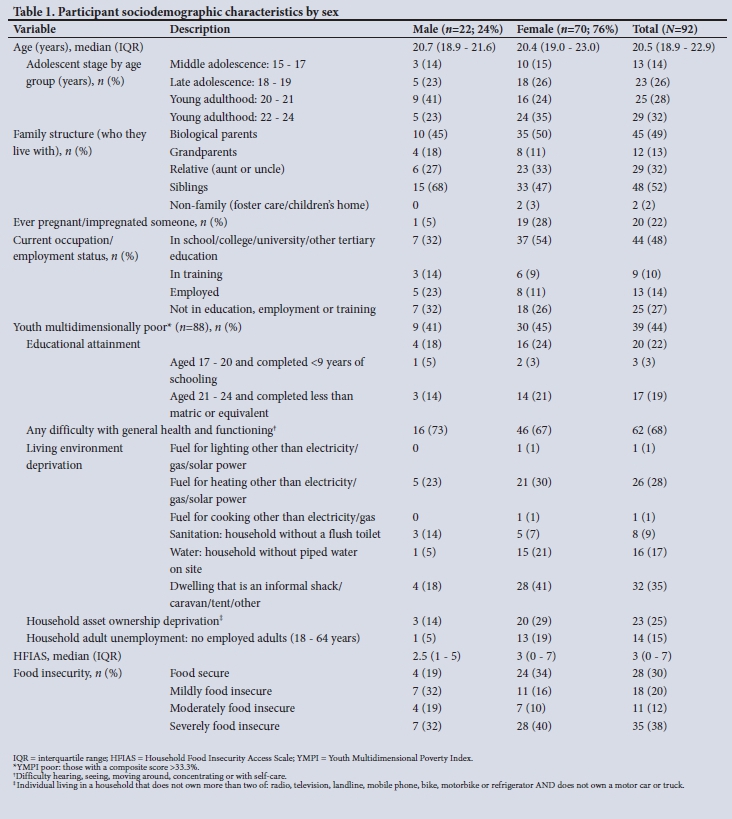
Adolescence can be categorised into three primary developmental stages: early adolescence (10 - 14 years), middle adolescence (15 - 17 years), and late adolescence/young adulthood (18 - 24 years).[22] We categorised participants into four age groups in line with these stages, further subdividing the oldest age group as follows: 15 - 17, 18 - 19, 20 - 21 and 22 - 24 years.
Deprivation was assessed using the Youth Multidimensional Poverty Index (YMPI), comprising 11 weighted indicators in five dimensions: educational attainment, general health and functioning, living environment, household assets and employment.[23] An individual was defined as being YMPI poor if deprived in a third or more of the weighted indicators, with a composite score >33.3%.[23]
Food insecurity was measured using the Household Food Insecurity Access Scale (HFIAS).[24] Participants were categorised as living in food-secure or mildly, moderately or severely food-insecure households.[24]
Behaviour and knowledge
Physical activity was assessed using the International Physical Activity Questionnaire (IPAQ), validated in youth and adults in SA.[25] We used the Ainsworth et al.[26]scoring algorithms to derive an average metabolic equivalent of task (MET) score. Insufficient physical activity was defined as a score <600 MET minutes/week.[27] Sedentary behaviour was defined as spending >3 hours per day watching television or other sitting activities.[28]
Dietary intake was assessed using a food frequency questionnaire (FFQ) adapted from the Health Behaviour in School-aged Children Survey, validated for adolescents.[29] Skipping breakfast was defined as eating breakfast on 0 - 2 days/week, semi-skipping as 3 - 4 days/week, and not skipping as 5 - 7 days/week.
Smoking and alcohol use. Tobacco and alcohol use were assessed using questions from the 2011 South African Youth Risk Behaviour Survey.[12] Current smoking and drinking were defined as smoking cigarettes or other tobacco products and consuming alcohol at least once during the preceding month, respectively.[12] Binge drinking was defined as drinking five or more drinks in succession at least once during the preceding month.[12]
Nutritional knowledge was assessed using a revised General Nutrition Knowledge Questionnaire (GNKQ-R), validated for young people.[30] A nutritional knowledge score was generated across four domains with a maximum possible score of 88: 18 for questions on dietary recommendations, 36 for questions on food groups, 13 for healthy food choices, and 21 for associations between diet and disease.
Comorbidities
Blood pressure (BP). Sitting BP was measured in mmHg using an automatic BP monitor (Rossmax (Shanghai) Incorporation Ltd, China) according to the SA hypertension practice guideline.[31]
Overweight and obesity. Height, weight and waist circumference (WC) were measured according to the World Health Organization (WHO) STEPS protocol.[32] The abdominal obesity criteria for WC were >102 cm in males and >88 cm in females and a waist-hip ratio >0.85 for females and >0.90 for males.[32] A waist-to-height ratio (WHtR) >0.5 was used as a measure of central obesity.[33]
Statistical analysis
Data were analysed using Stata version 14.0 (StataCorp, USA). All variables were checked for normality using graphical data exploration and the Shapiro-Wilk test and analysed stratified by sex and age. If the normal distribution assumption was violated, non-parametric statistical methods were used. Data were described using summary statistics (frequencies, percentages, medians and interquartile ranges (IQRs)) or means and 95% confidence intervals. Comparisons were made between sexes and age groups using Pearson's x2and Fisher's exact tests. The Mann-Whitney (7-test was used to compare medians between sexes, and the Kruskal-Wallis test to compare medians across age groups. All tests of significance were two-tailed and performed at the 5% significance level.
Results
Sociodemographic characteristics
A total of 176 adolescents and youth were recruited, of whom 92 were successfully interviewed. The majority (76%) were female, and the median (IQR) age was 20.5 (18.9 - 22.9) years. Overall, 44% of participants were YMPI poor, 70% were living in food-insecure households, and 38% were severely food insecure. Further details of the socioeconomic characteristics of participants are shown in Table 1.
Behaviour and knowledge
Physical activity
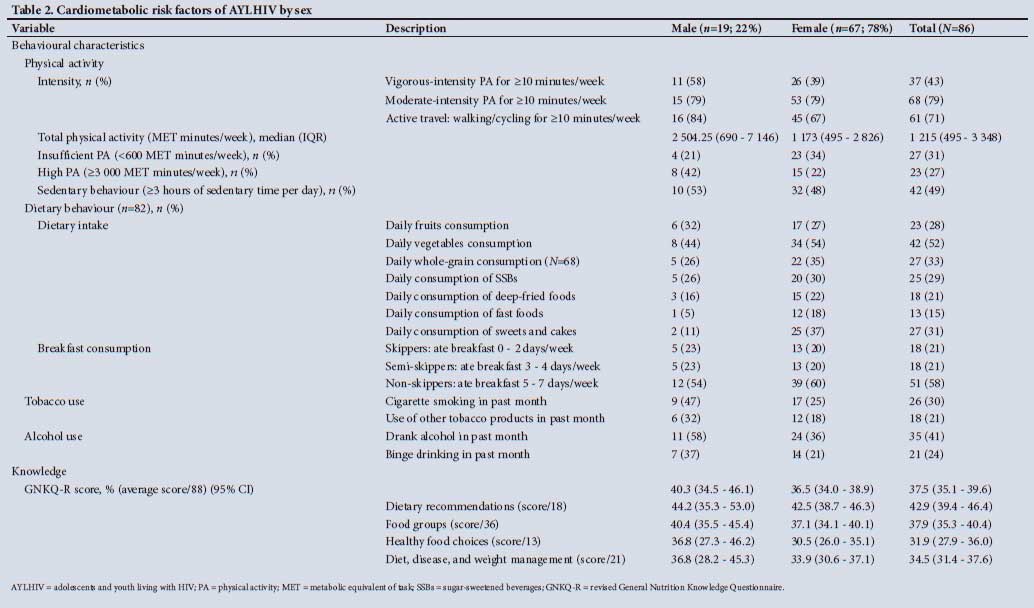
Overall, a third of respondents had insufficient levels of weekly physical activity. The median MET minutes per week was higher for males than for females, but this was not statistically significant (Table 2). Over two-thirds of participants reported using active transport in a typical week, while almost half were sedentary for >3 hours per day.
Dietary intake
Fifty-two percent of participants ate vegetables daily, while a lower proportion ate fruits (28%) and whole grains (33%) daily (Table 2).
Significantly more males than females ate fruit frequently, and younger adolescents had the lowest prevalence of daily consumption of fruits, vegetables and whole grains compared with older age groups. A third of respondents reported daily intake of added sugar, either drinking SSBs or eating sweets and cakes daily. SSB consumption was similar across sexes and age groups. Adolescents aged 18-19 years reported the highest daily consumption of deep-fried and fast foods compared with other age groups (Table 3). More than two-fifths of participants skipped breakfast regularly (on >3 days), although skipping breakfast did not differ significantly by sex or age.
Tobacco and alcohol use
Overall, a third of participants reported current smoking, 21% reported using other tobacco products, and 41% reported current drinking. Current drinking and binge drinking did not differ by sex. The prevalences of current smoking and binge drinking were highest for the youngest age group (Table 3). More than half (15/26) of current smokers also drank alcohol during the preceding month.
Nutrition knowledge
Overall, the mean GNKQ-R score was 33/88 points (37.5%). Knowledge of dietary recommendations was the highest-scoring domain with an average of 42.9%, while knowledge of healthy food choices was the lowest-scoring domain at 31.9%. There were no significant differences in nutrition knowledge by sex or age.
Comorbidities Overweight and obesity
A quarter of participants were overweight and 11% were obese, with significant differences by sex (Fig. 1). A greater proportion of participants aged 18-19 years were overweight or obese compared with the other age groups (Fig. 1). More females had central obesity compared with males (44% and 14%, respectively). A quarter of participants with a normal BMI had an abnormal WHtR consistent with central obesity.
Blood pressure
Overall, 20% had elevated BP, and 5% had hypertension. The prevalences of elevated BP and hypertension were higher in males compared with females (Fig. 2). The median (IQR) age of participants with elevated BP or hypertension was 21.2 (18.8 - 22.7) years, similar to those with normal BP (20.2 (19.0 - 22.8) years) (data not shown). Of those with elevated BP or hypertension, 11 (35%) were overweight or obese, and 2 (6%) reported a previous diagnosis of hypertension (data not shown).

Discussion
This study describes the prevalence of cardiometabolic NCDs and risk factors among SA AYLHIV in an urban setting. We found that a quarter had elevated BP or hypertension, more than a third were overweight or obese, a third had insufficient levels of weekly physical activity, the majority did not meet dietary guidelines for fruit and vegetable intake, a third were current smokers, and almost a quarter were binge drinkers. There was low nutritional knowledge, particularly on healthy food choices and diet-disease relationships. A detailed interpretation and comparisons with other studies and settings are discussed further below, beginning with risk factors.
Almost three-quarters of AYLHIV did not meet recommended dietary guidelines for daily fruit and vegetable intake necessary to reduce the risk of NCDs. More respondents, particularly females, consumed deep-fried foods and fast foods daily compared with previous estimates for youth in the same province.[12] Skipping breakfast in adolescence tends to persist until adulthood and has been associated with cardiometabolic risk factors, including higher prevalences of excess body weight and central obesity[34] and increased risk for NCDs.[35] Notably, a greater proportion
of AYLHIV reported skipping breakfast regularly compared with national estimates of 13 - 36%[36] and other LMICs (40%).[37] The high prevalence of food insecurity (50% moderate or severe food insecurity) experienced undoubtedly poses a challenge in terms of addressing these unhealthy dietary practices, with implications for NCD risk and viral suppression.[38] The finding that 44% of participants in this study were multidimensionally poor (higher than provincial estimates for youth of 22.8%[39]) is particularly striking. Addressing this challenge requires a multisectoral approach.
The SA government has implemented mandatory legislation for salt reduction in processed foods[40] and a tax on SSBs[41] to promote healthier food environments. Our findings suggest that greater efforts are needed, including appropriate social protection systems, to translate these legislations into action at a community and household level, especially among young girls, who have a higher prevalence of obesity than boys.
Furthermore, participants also scored low on general nutrition knowledge questions and specifically had poor knowledge of healthy food choices and associations between diet and diseases. Inadequate knowledge of nutrition-related NCDs among AYLHIV in our study is concerning in a country undergoing nutritional transition.[42] Although adolescents may lack autonomy in navigating their food environment, this life stage is characterised by increasing independence, highlighting the importance of good dietary knowledge to support healthier food choices, including daily breakfast consumption.
On the other hand, more than two-thirds of our respondents used active transport, walking to and from either school or work. This behaviour is encouraging, and it would be important for future interventions aimed at promoting physical activity to consider strategies to retain this healthy behaviour. The levels of physical inactivity in our study are similar to levels reported in urban SA students,[43] although we found a higher prevalence of sedentary behaviour.[12] Our results are consistent with those of studies from Botswana and Brazil, which found that AYLHIV had significantly lower daily physical activity levels than HIV-negative controls.[44,45] Additional research is needed to explore the relationship between physical activity and HIV in adolescents and promote physical activity in the context of a dynamic urban built environment.
We also found a higher prevalence of current smoking and drinking compared with national estimates for young people,[8,12] though aligned with smoking trends in Western Cape, the province with the highest prevalence of tobacco smoking in SA.[12] Concerningly, the prevalence of these risky behaviours was highest in the youngest age group, suggesting that targeted interventions to reduce uptake of smoking and drinking should start before adolescence. Smoking and alcohol use amplify the risk of developing cardiovascular diseases in PLHIV compared with HIV-negative people.[46] Studies from high-income settings and SSA report higher rates of smoking and alcohol use among AYLHIV compared with the general population.[47,48] Our findings corroborate this and add to the limited literature from LMIC settings. However, further research is needed in settings where heavy drinking is endemic to identify patterns of comorbidity and cardiovascular risk associated with increased alcohol consumption in AYLHIV.
With regard to other cardiometabolic risk factors, we found evidence of pre-existing hypertension and obesity in AYLHIV in our study. Our BP findings are consistent with those for youth in urban SA, with measured elevated BP and hypertension prevalences of 31% and 5%, respectively.[49] Hypertension is associated with ART in adults,[50] but there are conflicting data on the link between HIV infection and elevated BP in paediatric and adolescent populations.[51] Our findings support routine monitoring of BP in HIV care, even in younger populations, in settings such as SA with a high background prevalence of hypertension, to avert future disease.
Additionally, more than a third of our respondents were overweight or obese, with significant differences by sex. Obesity in PLHIV is well documented in high-income countries and is emerging as a significant challenge in Africa, with several studies showing increased rates of obesity in PLHIV[52,53] Notably, we found that 26% of our respondents with a normal BMI met the criteria for central obesity. This finding underscores the importance of anthropometric measurements beyond BMI, especially in females.
Moreover, in our study, obesity co-occurred with hypertension - 35% of those with elevated BP or hypertension were also overweight or obese (data not shown). This finding hints at the potential for obesity screening to help detect other related conditions that tend to cluster with obesity. Given that anthropometric measurements and calculations are non-invasive, low-cost and easy-to-use interventions, our findings support the value of integrating this screening into routine care to identify AYLHIV who are at increased cardiometabolic risk earlier and intervene as they transition into adulthood.
In the context of pre-existing multi-morbidity, our findings suggest that NCD care should be integrated with HIV care and should include screening for weight status and BP to identify comorbid NCDs and intervene early to improve NCD outcomes. Anthropometric assessment is especially pertinent given prolonged exposure to ART regimens linked to obesity, altered glucose metabolism and dyslipidaemia. Of note, the updated 2021 WHO HIV treatment guidelines call for integrated delivery of NCD health services within HIV care.[54]
In AYLHIV without a current NCD comorbidity, HIV care should include early identification of the most common NCD risk factors to facilitate early intervention and prevent NCD multimorbidity. To this end, our findings of low levels of nutritional knowledge, poor dietary practices and binge drinking (particularly in the youngest age group) suggest that these risk factors should be incorporated into HIV care to prevent multimorbidity.
Study limitations
While our study provides novel findings for the SSA context, adding to the limited evidence base on NCD prevalence and risk factors in AYLHIV, we note some limitations. Lack of random sampling may limit the generalisability of our findings. The necessity for parental consent may also have led to participant bias in the age distribution. However, sampling from six different facilities across all substructures in the City of Cape Town improved representativeness. We utilised subjective recall methods to assess behavioural risk factors, which maybe prone to information bias. However, self-report methods such as the IPAQ and FFQ have acceptable validity and have been widely used in similar contexts. We did not measure ART-associated and laboratory measures of other NCD risk factors such as blood lipids and renal function, as we were particularly interested in methods that can be implemented easily at the point of care in primary care settings. The use of point-of-care screening methods narrows the range of NCDs covered by the study. Despite these limitations, this study represents an essential contribution to the limited literature on HIV/NCD multimorbidity in adolescents and youth in SSA.
Conclusions
This study contributes to a critical gap in the literature on NCD comorbidity in AYLHIV in SSA. We identified existing cardiometabolic risk factors and conditions (obesity, abdominal obesity, hypertension, physical inactivity, unhealthy diet, inadequate nutritional knowledge, binge drinking) in this vulnerable population. Our findings suggest that these risk factors should be integrated into routine HIV care for the primary and secondary prevention of NCD multimorbidity in AYLHIV. Beyond healthcare, the findings of high levels of food insecurity and multidimensional poverty reinforce the need to address the social, economic and environmental exposures that coexist with and perpetuate NCD risk. Multisectoral interventions are required beyond the healthcare sector to reduce the impact of NCDs on health systems and broader societal development. Further studies are needed to assess risk factors at a broader socioecological level and explore multilevel determinants of HIV/ NCD comorbidity in adolescents and youth.
Declaration. The research for this study was done in partial fulfilment of the requirements for MK's PhD degree at the University of Cape Town.
Acknowledgements. We appreciate the assistance from the City of Cape Town and Western Cape departments of health, who made access to the facilities and participants possible. We acknowledge and thank the adolescents and youth who agreed to make themselves available to participate in this research and share their insights and experiences with us.
Author contributions. MK and TO conceptualised the study. MK and BG conducted data collection. MK conducted data analysis and interpretation and wrote the first draft of the manuscript. TO contributed to data interpretation and manuscript preparation. All authors read and approved the final manuscript.
Funding. This work was supported by a Bristol-Myers Squibb Foundation grant awarded to TO (grant no. 430960). MK was supported by the South African National Research Foundation under joint funding with the German Academic Exchange Service for her PhD. TO is also funded by the National Institute for Health Research (NIHR) (16/137/34) using UK aid from the UK government to support global health research. The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the UK Department of Health and Social Care. The funding bodies had no role in the design of the study, data collection, analysis, interpretation of data or writing the manuscript.
Conflicts of interest. None.
References
1. Vos T, Abajobir AA, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990 - 2016. A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017;390(10100):1211-1259. https://doi.org/10.1016/S0140-6736(17)32154-2 [ Links ]
2. World Health Organization. Noncommunicable diseases. 1 June 2018. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed 21 April 2020). [ Links ]
3. Gouda HN, Charlson F, Sorsdahl K, et al. Burden of non-communicable diseases in sub-Saharan Africa, 1990 - 2017. Results from the Global Burden of Disease Study 2017. Lancet Glob Health 2019;7(10):el375-el387. https://doi.org/10.1016/S2214-109X(19)30374-2 [ Links ]
4. Lee IM, Shiroma EJ, Lobelo F, et al. Effect of physical inactivity on major non-communicable diseases worldwide. An analysis of burden of disease and life expectancy. Lancet 2012;380(9838):219-229. https://doi.org/10.1016/S0140-6736(12)61031-9 [ Links ]
5. Remais JV, Zeng G, Li G, et al. Convergence of non-communicable and infectious diseases in low-and middle-income countries. Int J Epidemiol 2013;42(1):221-227. https://doi.org/10.1093/ije/dysl35 [ Links ]
6. Joint United Nations Programme on HIV and AIDS (UNAIDS). Country factsheets. South Africa 2019. https://www.unaids.org/en/regionscountries/countries/southafrica (accessed 17 January 2021). [ Links ]
7. United Nations Childrens Fund (UNICEF). Key HIV epidemiology indicators for children and adolescents aged 0-19, 2000-2018. 2019. https://data.unicef.org/wp-content/uploads/2019/07/HIV_Epidemiology_Children_Adolescents_2019.xlsx (accessed 28 April 2020). [ Links ]
8. National Department of Health (NDoH), Statistics South Africa (Stats SA), South African Medical Research Council (SAMRC), and ICF South Africa Demographic and Health Survey 2016. January 2019. http://dhsprogram.com/pubs/pdf/FR337/FR337.pdf (accessed 17 January 2021). [ Links ]
9. Shisana O, Labadarios D, Rehle T, et al. The South African National Health and Nutrition Examination Survey, 2012. SANHANES-1. The health and nutritional status of the nation. Cape Town. HSRC Press, 2015. https://repository.hsrc.ac.za/handle/20.500.11910/2864 (accessed 17 January 2021). [ Links ]
10. World Health Organization, Global status report on alcohol and health 2018. 27 September 2018. https://www.who.int/publications/i/item/9789241565639 (accessed 17 January 2021). [ Links ]
11. Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980 - 2013. A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014,384(9945)766-781. https://doi.org/10.1016/S0140-6736(14)60460-8 [ Links ]
12. Reddy S, James S, Sewpaul R, et al. Umthente uhlaba usamila. The 3rd South African National Youth Risk Behaviour Survey 2011. Cape Town. South African Medical Research Council, 2015. https://repository.hsrcacza/handle/20.500.11910/2487 (accessed 28 April 2020). [ Links ]
13. Patel P, Rose CE, Collins PY, et al. Noncommunicable diseases among HIV-infected persons in low-income and middle-income countries. A systematic review and meta-analysis. AIDS 2018;32(Suppl 1):S5-S20. https://doi.org/10.1097/QAD.0000000000001888 [ Links ]
14. Vancampfort D, Mugisha J, Richards J, de Hert M, Probst M, Stubbs B. Physical activity correlates in people living with HIV/AIDS. A systematic review of 45 studies. Disabil Rehabil 2018;40(14): 16181629. https://doi.org/10.1080/09638288.2017.1306587 [ Links ]
15. Elf JL, Variava E, Chon S, et al. Prevalence and correlates of smoking among people living with HIV in South Africa. Nicotine Tob Res 2018;20(9):1124-1131. https://doi.org/10.1093/ntr/ntxl45 [ Links ]
16. Agwu AL, Fairlie L. Antiretroviral treatment, management challenges and outcomes in perinatally HIV-infected adolescents. J Int AIDS Soc 2013;16(1):18579. https://doi.org/10.7448/IAS.16.1.18579 [ Links ]
17. Barlow-Mosha L, Ross Eckard A, McComsey GA, Musoke PM. Metabolic complications and treatment of perinatally HIV-infected children and adolescents. J Int AIDS Soc 2013;16(1):18600. https://doi.org/10.7448/IAS.16.1.18600 [ Links ]
18. Sawyer SM, Afifi RA, Bearinger LH, et al Adolescence. A foundation for future health. Lancet 2012;379(9826):1630-1640. https://doi.org/10.1016/S0140-6736(12)60072-5 [ Links ]
19. Kamkuemah M, Gausi B, Oni T. Missed opportunities for NCD multimorbidity prevention in adolescents and youth living with HIV in urban South Africa. BMC Public Health 2020,20.821. https://doi.org/10.1186/sl2889-020-08921-0 [ Links ]
20. City of Cape Town. 2016 Community Survey Cape Town Trends 1996 to 2016. April 2017. https://resource.capetown.gov.za/documentcentre/Documents/Maps%20and%20statistics/2016%20Community%20Survey%20Cape%20Town%20Trends.pdf (accessed 19 March 2021). [ Links ]
21. Western Cape Government. Cape Metro District Health Plan 2018/19 - 2020/21. 2018. https://resource.Capetown.gov.za/documentcentre/Documents/City%20strategies,%20plans%20and%20frameworks/Metro%20District%20Health%20Plan_2019-20.pdf (accessed 19 March 2021). [ Links ]
22. Klein H. Adolescence, youth, and young adulthood. Rethinking current conceptualisations of life stage. Youth Soc 1990,21(4)446-471. https://doi.org/10.1177/0044118X9002100400223 [ Links ]
23. Alkire S, Santos ME. Acute multidimensional poverty: A new index for developing countries. Oxford Poverty & Human Development Initiative (OPHI) Working Paper No. 38, United Nations Development Programme Human Development Report Office Background Paper No. 2010/11. 1 July 2010. https://doi.org/10.2139/ssrn.l815243 [ Links ]
24. Ballard T, Coates J, Swindale A, Deitchler M. Household Hunger Scale. Indicator definition and measurement guide. Food and Nutrition Technical Assistance III Project, August 2011. 360. https://www.fantaproject.org/sites/default/tiles/resources/HHS-Indicator-Guide-Aug2011.pdf (accessed 19 March 2020). [ Links ]
25. Craig CL, Marshall AL, Sjostrom M, et al. International physical activity questionnaire. 12-country reliability and validity. Med Sci Sports Exerc 2003;35(8):1381-1395. https://doi.org/10.1249/01.mss.0000078924.61453.fb [ Links ]
26. Ainsworth BE, Haskell WL, Whitt MC, et al. Compendium of physical activities. An update of activity codes and MET intensities. Med Sci Sports Exerc 2000;32(9):S498-S516. https://doi.org/10.1097/00005768-200009001-00009 [ Links ]
27. World Health Organization, Global recommendations on physical activity for health. Geneva. WHO; 1 January 2010. https://www.who.int/pubhcations/i/item/9789241599979 (accessed 17 January 2021). [ Links ]
28. Guthold R, Cowan MJ, Autenrieth CS, Kann L, Riley LM. Physical activity and sedentary behavior among schoolchildren. A 34-country comparison. J Pediatr 2010;157(1):43-49.E1. https://doi.org/10.1016/j.jpeds.2010.01.019 [ Links ]
29. Saioheimo T, Gonzalez SA, Erkkola M, et al. The reliability and validity of a short food frequency questionnaire among 9 - 11-year olds. A multinational study on three middle-income and high-income countries. Int J Obes Suppl 2015;5(2):S22-S28. https://doi.org/10.1038/ijosup.2015.15 [ Links ]
30. Kliemann N, Wardle J, Johnson F, Croker H. Reliability and validity of a revised version of the General Nutrition Knowledge Questionnaire. Eur J Clin Nutr 2016;70(10):1174-1180. https://doi.org/10.1038/ejcn.2016.87 [ Links ]
31. Seedat Y, Rayner B, Veriava Y. South African hypertension practice guideline 2014. Cardiovasc J Afr 2014;25(6):288-294. https://doi.org/10.5830/CVJA-2014-062 [ Links ]
32. World Health Organization. Waist circumference and waist-hip ratio. Report of a WHO expert consultation, Geneva, 8-11 December 2008. Geneva. WHO, 2011. https://apps.who.int/iris/bitstream/handle/10665/44583/9789241501491_eng.pdf?sequence=l&isAllowed=y (accessed 17 January 2021). [ Links ]
33. Browning LM, Hsieh SD, Ashweli M. A systematic review of waist-to-height ratio as a screening tool for the prediction of cardiovascular disease and diabetes. 0.5 could be a suitable global boundary value. Nutr Res Rev 2010;23(2):247-269. https://doi.org/10.1017/S0954422410000144 [ Links ]
34. De Souza MR, Neves MEA, Souza AM, et al. Skipping breakfast is associated with the presence of cardiometabolic risk factors in adolescents. Study of Cardiovascular Risks in Adolescents - ERICA. Br J Nutr 126;(2):276-284. https://doi.org/10.1017/s0007114520003992 [ Links ]
35. St-Onge M-P, Ard J, Baskin ML, et al. Meal timing and frequency. Implications for cardiovascular disease prevention. A scientific statement from the American Heart Association. Circulation 2017;135(9):e96-el21.https://doi.org/10.1161/CIR.0000000000000476 [ Links ]
36. Tee L, Botha C, Laubscher R, Jerling J. The intake and quality of breakfast consumption in adolescents attending public secondary schools in the North West province, South Africa. S Afr J Clin Nuti 2015;28(2):81-88. https://doi.org/10.1080/16070658.2015.11734536 [ Links ]
37. Keats EC, Rappaport AI, Shah S, Oh C, Jain R,BhuttaZA. The dietary intake and practices of adolescent girls in low- and middle-income countries. A systematic review. Nutrients 2018;10(12):1978. https://doi.org/10.3390/nul0121978 [ Links ]
38. Innes S, PatelK. Non-communicable diseases in adolescents with perinataliy-acquired HIV-1 infection in high-income and low-income settings. Curr Opin HIV AIDS 2018;13(3):187-195. https://doi.org/10.1097/COH.0000000000000458 [ Links ]
39. Frame E, De Lannoy A, Koka P, Leibbrandt M. Multidimensional youth poverty. Estimating the youth MPI in South Africa at ward level. Southern Africa Labour and Development Research Unit Working Paper Number 189. Cape Town. SALDRU, University of Cape Town, 2016. http://www.opensaidru.uct.ac.za/bitstream/handle/11090/823/2016_189_Saidruwp.zip?sequence=5 (accessed 17 January 2021). [ Links ]
40. Department of Health, South Africa. Foodstuffs, Cosmetics and Disinfectants Act 54 of 1972. Regulations relating to the reduction of sodium in certain foodstuffs and related matters. Government Gazette No. 36274 20 March 2013. Published under Government Notice R214. https://www.gov.za/sites/defauit/nles/gcis_document/201409/36274rg9934gon214.pdf (accessed 17 January 2021). [ Links ]
41. Arthur R. South Africa introduces sugar tax. Beverage Daily, 3 April 2018. https://www.beveragedaily.com/Article/2018/04/03/South-Africa-introduces-sugar-tax (accessed 30 January 2019). [ Links ]
42. Bourne LT, Lambert EV, Steyn K. Where does the black population of South Africa stand on the nutrition transition? Public Health Nutr 2002;5(1A):157-162. https://doi.org/10.1079/PHN2001288 [ Links ]
43. VanBiijon A, McKune AJ, Dubose KD, Kolanisi U, Semple SA. Physical activity levels in urban-based South African learners. A cross-sectional study of 7 348 participants. S Afr Med J 2018",108(2).126-131. https://doi.org/10.7196/SAMJ.2018.vl0812.12766 [ Links ]
44. Malete L, Tladi DM, Etnier JL, Makhanda J, Anabwani GM. Examining psychosocial correlates of physical activity and sedentary behavior in youth with and without HIV. PLoS ONE 2019;14(12):e0225890. https://doi.org/10.1371/journal.pone.022589C [ Links ]
45. Martins P, Castela E, Rocha G, Sena C, Seica R [Premature Atherosclerosis in HIV-infected Pediatric Patients Literature Review and Clinical Approach]. Acta Med Port 2017;30(10):742-749. https://doi.org/10.20344/amp.8726 [ Links ]
46. Freiberg MS, Chang C-CH, Kuller LH, et al. HIV infection and the risk of acute myocardial infarction. JAMA Intern Med 2013;173(8):614-622. https://doi.org/10.1001/jamainternmed.2013.3728 [ Links ]
47. Alperen J, Brummel S, Tassiopoulos K, et al. Prevalence of and risk factors for substance use among perinataliy HIV-infected and perinataliy exposed but uninfected youth. J Adolesc Health 2014;54(3):341-349. https://doi.org/10.1016/j.jadohealth.2013.09.003 [ Links ]
48. Ssewanyana D, Mwangala PN, van Baar A, et al. Health risk behaviour among adolescents living with HIV in sub-Saharan Africa. A systematic review and meta-analysis. Biomed Res Int 2018,2018:7375831. https://doi.org/10.1155/2018/7375831 [ Links ]
49. Naidoo S, Kagura J, Fabian J, Norris SA. Early life factors and longitudinal blood pressure trajectories are associated with elevated blood pressure in early adulthood. Hypertension 2019,73(2):301-309. https://doi.org/10.1161/HYPERTENSIONAHA.118.11992 [ Links ]
50. Nduka C, Stranges S, Sarki A, Kimani PK, Uthman OA. Evidence of increased blood pressure and hypertension risk among people living with HIV on antiretroviral therapy. A systematic review with meta-analysis. J Human Hypertens 2016;30(6):355-362. https://doi.org/10.1038/jhh.2015.97 [ Links ]
51. Sainz T, Serrano-Villar S, Mellado MJ. Prevalence of elevated blood pressure in HIV-infected children, adolescents and young adults. Pediatr Infect Dis J 2016;35(7):824-825. https://doi.org/10.1097/INF0000000000001178 [ Links ]
52. Castro ADCO, Silveira EA, Falco MDO, Nery MW, Turchi MD. Overweight and abdominal obesity in adults living with HIV/AIDS. Rev Assoc Med Bras 2016,62(4)353-360. https://doi.org/10.1590/1806-9282.62.04.353 [ Links ]
53. Huis in't Veld D, Pengpid S, Colebunders R, Peltzer K. Body mass index and waist circumference in patients with HIV in South Africa and associated socio-demographic, health related and psychosocial factors. AIDS Behav 2018-^2(6). 1972-1986. https://doi.org/10.1007/sl0461-017-1737-2 [ Links ]
54. World Health Organization. Guidelines, updated recommendations on HIV prevention, infant diagnosis, antiretroviral initiation and monitoring. Geneva. WHO, March 2021. https://apps.who.int/iris/bitstream/handle/10665/340190/9789240022232-eng.pdf (accessed 20 April 2021). [ Links ]
 Correspondence:
Correspondence:
M Kamkuemah
monika.kamkuemah@gmail.com
Accepted 19 January 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}