










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 n.4 Pretoria Apr. 2022
http://dx.doi.org/10.7196/samj.2022.v112i4.16327
IN PRACTICE
ISSUES IN PUBLIC HEALTH
Teenage births and pregnancies in South Africa, 2017 - 2021 - a reflection of a troubled country: Analysis of public sector data
P BarronI; H SubedarII; M LetsokoIII; M MakuaIV; Y PillayV
IBCom, MB ChB; School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMCur, MPA; Clinton Health Access Initiative, Pretoria, South Africa
IIIBCom; Clinton Health Access Initiative, Pretoria, South Africa
IVBSc Hons (Epidemiology and Biostatistics), DLitt et Phil (Nursing); National Department of Health, Pretoria, South Africa
VMSc, PhD; Division of Health Systems and Public Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
Articles on teenage pregnancies have been proliferating in both the popular press and the medical media. We analysed data available in the public sector database, the District Health Information System, from 2017 to 2021. During this time, the number of births to young teenagers aged 10-14 years increased by 48.7% (from a baseline of 2 726, which is very high by developed-country standards) and the birth rate per 1 000 girls in this age category increased from 1.1 to 1.5. These increases occurred year on year in most provinces. In adolescent girls aged 15-19, the number of births increased by 17.9% (from a baseline of 114 329) and the birth rate perl 000 girls in this age category increased from 49.6 to 55.6. These increases also occurred year on year in a continuous upward trend as well as in all provinces, but at different rates. Generally, rates were higher in the more rural provinces such as Limpopo, Mpumalanga and Eastern Cape than in more urban provinces such as Gauteng and Western Cape. The increases during the past 2 years were particularly large and may be due to disruption of health and school services with decreased access to these as a result of COVID-19. These metrics pose serious questions to society in general and especially to the health, education and social sectors, as they reflect socioeconomic circumstances (e.g. sexual and gender-based violence, economic security of families, school attendance) as well as inadequate health education, life skills and access to health services.
During 2021, there were a number of media reports that teenage pregnancies had dramatically increased. For example, Save the Children noted that 'The number of children born to teen mothers in South Africas most populous province, Gauteng, has jumped 60% since the start of the COVID-19 pandemic.[1] A Daily Maverick column had the headline 'Schoolgirl births "unacceptably high" in South Africa.'[2] This article tests the validity of these concerns. It quantifies and analyses teenage births and pregnancies in the public sector from 2017 to 2021, showing trends geographically, as well as disaggregating data into very young teenagers 10 - 14 years old and those aged 15 - 19. The media use of the word pregnancy is loosely used, as this includes miscarriages and pregnancy terminations, which are often extremely difficult to measure, and childbearing would be the more correct and appropriate term.
Early childbearing can have negative effects on the education, livelihoods and health of adolescents. Many girls who are pregnant drop out of school, which can impact on their educational and employment opportunities. Early pregnancy and childbearing can also have social consequences for girls, including reduced status in the home and community, stigmatisation, rejection and violence by family members, peers and partners, and early marriage. Early pregnancy can also affect the health of adolescent girls, and globally maternal conditions are among the top causes of death and disability among adolescents aged 15 - 19 years. The younger the girl the greater the health risk, especially among girls aged 10 - 14.[3] Studies have found that early childbearing, particularly by teenagers and young women who have not completed school, has a significant impact on the education outcomes of both the mother and child, and is also associated with poorer child health and nutritional outcomes.[4]
During the period 2015 - 2020, the global adolescent birth rate was 41 births per 1 000 adolescents aged 15-19 years. There were large differences around the world, with sub-Saharan Africa having an adolescent birth rate of 99, Western Europe 8, and South Africa (SA) being in line with the global average of 41.[5,6]
The South Africa Demographic and Household Survey (SADHS) of 2016 found that the proportion of 15 - 19-year-olds who had begun childbearing was 16%, unchanged from the SADHS of 1998. The SADHS also found large inequities, with teenagers who lived in rural areas and those who were from the lowest socioeconomic quintiles more likely to have had children than those from urban areas and in the higher socioeconomic quintiles.[7] The Department of Basic Educations analysis of the General Household Survey of 2019 on schooling found that the average pregnancy rate of girls aged > 14 ranged between 3% and 4% during the period 2010 - 2019. It also found that pregnancy rates increased significantly in grades 10-12 compared with grades 8 and 9. Furthermore, pregnancy rates tended to be higher in rural provinces such as Limpopo and Mpumalanga compared with more urban provinces such as Gauteng, Western Cape and Free State.[8]
In SA, up to 2017 in the public sector, the delivery rate to girls aged < 18 years was used as a marker for teenage pregnancy: between 2013 and 2017 the proportion of total pregnancies in this age group fell nationally from 7.7% to 6.8%.[9] This article estimates the teenage pregnancy rate from 2017 to 2021.
Methods
In 2017, SA adopted the World Health Organization indicator[10] of births to adolescent girls aged 15 - 19 years as a proxy for teenage pregnancy. This metric was introduced in April 2017 at the start of the financial year and data are reported in financial years, viz. from 1 April through to 31 March. In addition, SA measures the numbers of births in young teenagers aged 10 - 14 as well as terminations of pregnancies in all teenagers aged 10 - 19. Provincial-level data for these metrics were extracted from the public sector's District Health Information System (DHIS) for the period April 2017 through to September 2021. This article analyses these data by comparing rates over the 4 years of available data, as well as comparing rates geographically by province and in the two age groups.
These data reflect the numbers of deliveries and terminations of pregnancy in the public sector of SA, accounting for -85% of all deliveries in SA, and exclude births and terminations taking place in the private health sector. Miscarriages and terminations outside the public sector (either illegally or in the private and not-for-profit sector) and deliveries in the private health sector or at home are not captured in the DHIS. These factors all serve to underestimate the numerator for the calculation of the pregnancy rates, while the denominator reflects all girls in the relevant age bands in SA, in both the public and private sectors.
These data were disaggregated into age bands 10-14 years and 15 - 19 years, as well as by province. Disaggregating further down the system into districts or facilities would bias the indicators, as the location of national, tertiary and secondary hospitals with large numbers of deliveries would skew the data in the districts where these facilities are located. To calculate the rates, the mid-year populations of females aged 10-14 and 15-19 were extracted from Statistics South Africa (Stats SA) mid-year population data.[11-15] Using the numerators from the DHIS and the denominators from Stats SA, we calculated indicators and rates for a number of variables and compared provinces over time. The most recently available data from April 2021 to September 2021 comprise 6 months, and this reflects in smaller numbers in the tables, which were adjusted to estimate annual rates. The total number of teenage pregnancies was estimated by adding the number of deliveries to the number of terminations in adolescent girls aged 10 - 19. This estimate excludes spontaneous miscarriages and pregnancy terminations outside the formal public sector health system in SA, both legitimate and illegitimate.
Results
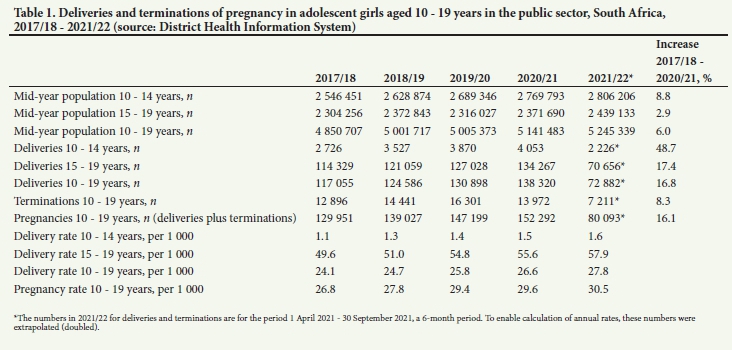
Table 1 shows the national picture, with the numbers of deliveries in the public sector to adolescent girls aged 10-14 years and 15 -19 years for the 4.5 financial years from 1 April 2017 through to 30 September 2021. It also shows the number of terminations of pregnancy in adolescents aged 10-19. These numbers are converted into rates per 1 000 adolescent girls in these age categories. A feature of this table is that teenage pregnancies increased (both in numbers and rates) year on year for the past 5 years. The only exception to this was a decrease in terminations during 2020/21 following the large increase during 2019/20.
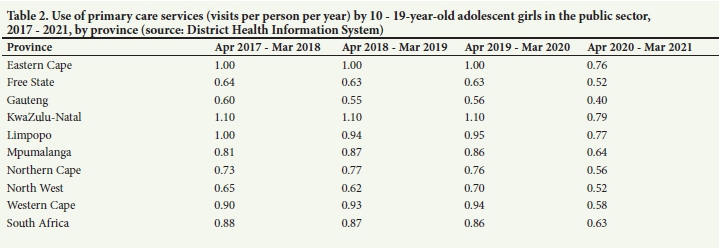
This decrease in terminations is probably due to a decrease in access to public sector services as a result of COVID-19, and the disruption it causes to service delivery. Table 2 clearly shows the large drop in utilisation by 10 - 19-year-olds generally during the period 2017/18 - 2020/21. For the 3 years 2017, 2018 and 2019, the rate of visits per teenager aged 10-19 was stable at -0.86 visits per person per year, and in the financial year April 2020 - March 2021 the rate dropped to 0.63 visits, which equates to a decline of 26.7%.
In teenagers aged 10 - 14, the number of deliveries increased from 2 726 in 2017/18 to 4 053 in 2020/21, an increase of 48.7%. Where the number of deliveries is expressed per 1 000 adolescents aged 10-14 (i.e. the rate), the value increased from 1.1 per 1 000 in 2017/18 to 1.5 per 1 000 in 2020/21. In the older teenagers aged 15 - 19, the number of deliveries increased from 114 329 in 2017/18 to 134 267 in 2020/21, an increase of 17.4%. During this same time period, the delivery rate in older teenagers increased from 49.6 per 1 000 to 55.6 per 1 000. Overall, estimated teenage pregnancies (deliveries plus terminations) during this period increased by 16.1% from 129 951 in 2017/18 to 152 292 in 2020/21.
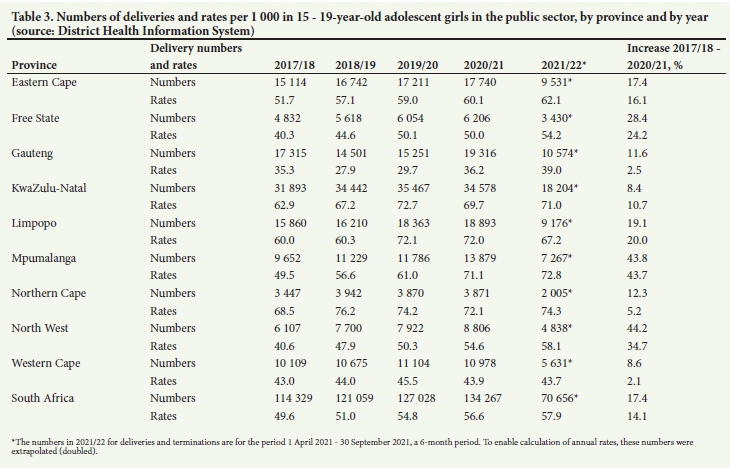
Table 3 and Fig. 1 show details of the numbers and rates of deliveries in older teenagers aged 15 - 19, analysed by province. Overall, the numbers of deliveries in the public sector increased by 17.4% from 2017/18 to 2020/21. During this time, the total population of adolescent girls in this age group increased by 2.9%. Every province, with the exception of Western Cape, which was fairly stable at -43 deliveries per 1 000 teenagers, had increases in delivery numbers and rates. There is a wide difference between provinces, with the more urbanised Gauteng and Western Cape having rates between 35 and 45 deliveries per 1 000 teenagers, while the more rural KwaZulu-Natal and Limpopo had rates closer to 60 - 70 per 1 000 teenagers. Some provinces had very large increases, with, for example, Mpumalanga increasing from a rate of 49.5 per 1 000 to 71.1 per 1 000 (an increase in numbers of deliveries of 43.8%) and North West increasing from 40.6 to 54.6 per 1 000 (an increase in numbers of deliveries of 44.2%). The very large jump in the numbers of deliveries and rates in Gauteng (from 29.7 to 36.2 per 1 000) between 2019/20 and 2020/21 had a marked impact on the national rate.
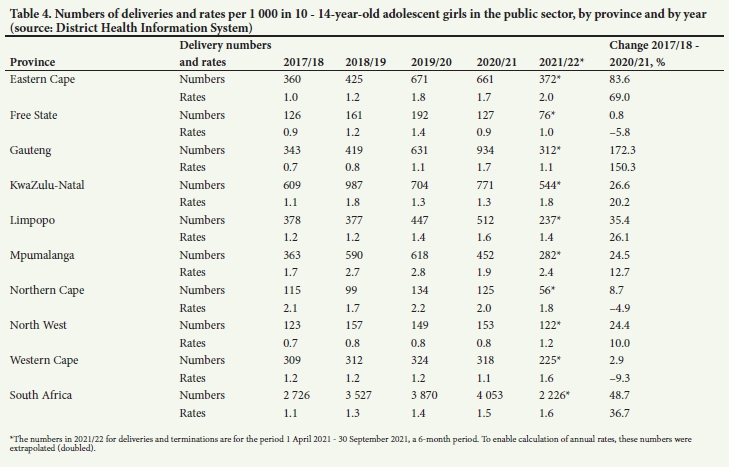
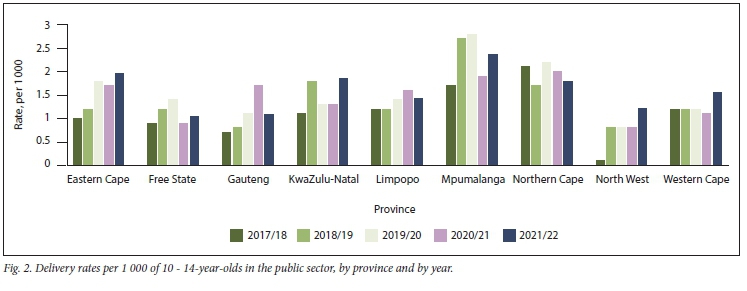
Table 4 and Fig. 2 show the numbers of deliveries in very young teenagers aged 10-14 years, as well as the rates per 1 000 girls in this age band, analysed by province and by year. Although the numbers of deliveries in this group are relatively small, each one represents a failure of society in general and often a personal tragedy for the girl and family involved. Over the period of this analysis, there has been a steady but large increase nationally from 1.1 per 1 000 adolescents (2 726 deliveries) in 2017/18 to 1.5 per 1 000 adolescents (4 053 deliveries) in 2020/21. Although there were fluctuations in both absolute numbers and rates, the general trend in the provinces is upwards. Northern Cape, starting at a very high base nearly three times higher than Gauteng in 2017/18, is the exception to this and has been fairly stable. Western Cape has also been stable except for the current year (2021/22), where there has been a sharp increase. The overall rates in Gauteng have generally been the lowest (~1 delivery per 1 000), except for a very large increase in 2020/21 to 1.7 per 1 000. The overall rates in Mpumalanga and Northern Cape have been the highest (~2 deliveries per 1 000).
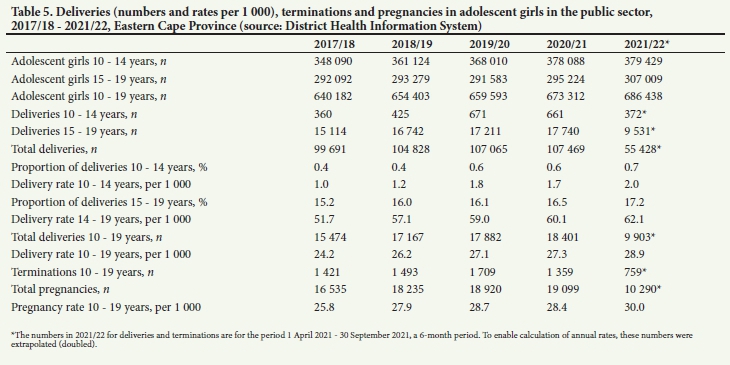
Table 5 is an example of one province, Eastern Cape, showing in different age bands (10 - 14, 15 - 19 and overall, 10-19 years) the numbers, proportions and rates of delivery in the province, as well as the terminations and the estimated pregnancy rate in teenagers over the period 2017/18 - 2021/22. During this time, the proportion of total deliveries in the province that were to teenagers increased from 15.6% to 17.9%. At a national level, the proportion has increased faster, with 10.0% of all deliveries in 2017/18 to teenagers rising to 14.0% in 2021/22. Overall, in Eastern Cape between 2017/18 and 2020/21, the rate of deliveries in the young teenagers (10 - 14) has increased from 1 per 1 000 to 1.7 per 1 000, while nationally the rate increased from 1.1 to 1.5 per 1 000.
Discussion
The numbers of estimated pregnancies and resultant rates in the results reported above are an underestimate of the true picture (see 'Methods' for more details). These metrics pose serious questions to society in general and to the health, education and social sectors in particular, as they reflect socioeconomic circumstances (e.g. sexual and gender-based violence, economic security of families, school attendance) as well as inadequate health education and life skills and access to health services. Clearly the country has much to do to reverse these negative trends. There have been problems with access to contraceptives in the public sector in the past 5 years. Injectable contraceptives, for example, were out of stock for several months during 2015 - 2019, and then during COVID-19, access to facilities and health workers has sometimes been difficult because of lockdowns and diversion of health workers to COVID-related activities. Birth rates have increased during the past 2 years, and one factor influencing this may have been the impact of COVID-19 on access to contraceptive and other sexual and reproductive health services for adolescent girls with disruption of primary-level clinic services and schooling. During 2020/21, the number of terminations dropped sharply and with the exception of Gauteng every province showed significant drops compared with 2019/20. It is highly likely that one of the negative side-effects of COVID-19 has been a lack of access to termination services. This was particularly marked in Mpumalanga, where the numbers of terminations dropped from 1 134 in 2019/20 to 394 in 2020/21.
This article puts actual numbers and rates to the data around teenage deliveries and pregnancies in SA. It clearly shows that, since 2017, there has been a significant increase in teenage deliveries in all provinces. This applies to young teenagers aged 10-14 years as well as to adolescents aged 15 - 19. The article also puts into perspective many of the headlines about teenage pregnancy that have recently been circulating in both the medical and lay media. 'Mounting concern over SAs child and teen pregnancy crisis' is a headline in Medical Brief,[16] where the President of the South African Society of Obstetricians and Gynaecologists warns that many of the pregnancies may follow gender-based violence and sexual abuse. In the lay media, The Sowetan had a headline quoting the Department of Basic Education: '... of the 120,000 schoolgirls who fall pregnant annually, only a third returned to school after giving birth.[17]
Teenage pregnancy rates are difficult to calculate directly, because it is hard to determine how many pregnancies end in miscarriage, stillbirth or abortion and are not necessarily accurately reported. In the absence of reliable data on pregnancy, researchers tend to rely on childbearing data when comparing countries (i.e. the percentage of women aged 15 - 19 who have given birth to a live child). The data in this article represent the best available data and include deliveries in young girls aged 10 - 14 as well as terminations in teenagers aged 10 - 19, in the public sector database (private sector data are not included in the national dataset), and are therefore a proxy for the real situation in SA.
Because of the limitations of length, it was not possible to publish all the provincial results. The Eastern Cape results were chosen to illustrate the rapid increase in births, especially in young teenagers aged 10-14. Other important features from the provincial-level data were that on the whole teenage birth rates in rural provinces such as Limpopo, Mpumalanga and Eastern Cape were much higher than in more urbanised provinces such as Western Cape and Gauteng. Very disturbingly, birth rates in adolescent girls in the rural provinces increased at a much faster rate than in the urbanised provinces, where the rates were relatively stable, thus accentuating the differences. Northern Cape generally had the highest birth rates for adolescent girls aged 15-19 and one of the highest for young teenagers aged 10-14. However, because of the relatively smaller overall population of young girls, the actual numbers are lower than the other provinces. It had a different pattern to the other provinces, with a high baseline and fluctuations in the rates.
Teenage pregnancy implies that the pregnancy is usually unplanned. A 2019 survey of a large number of public sector pregnancies in SA showed that more than three-quarters (76%) of pregnancies in girls aged 15-19 were unplanned.[18] Teenage pregnancy also indicates risky, coerced and unprotected sex for many girls, with consequences of contracting sexually transmitted infections in general and HIV in particular.[19] Adolescent girls and young women have the highest rate of acquisition of HIV, and the current (2021) HIV incidence rate for females aged 15 - 24 is 1.25% (Thembisa model 4.4., in Johnson et al.[20]). Many of the interventions aimed at reducing HIV acquisition in adolescent girls are similar to those aimed at reducing teenage pregnancies, and it is of great concern that the HIV/AIDS Life Skills conditional grant was slashed in the June 2020 Supplementary Budget. The grant was cut by ZAR60 million, and a further ZAR40 million was reprioritised for COVID-19 information at schools, which meant less money for training teachers to deliver comprehensive sexuality education (CSE). Research from around the world, including SA has found that effective CSE programmes delivered by well-trained teachers result in improved knowledge about HIV and pregnancy prevention; decreased sexual risk-taking; the prevention of learners from having multiple concurrent sexual partners; improved attitudes towards sexual refusal and condom use; and delayed sexual debut.[2] Ironically, shortly after this in September 2021, the Department of Basic Education presented its policy on learner pregnancy to the Parliamentary Portfolio Committee. This policy has been endorsed by Cabinet and will be implemented in 2022.[22]
Pregnancy in very young adolescent girls aged 10 - 14 is a savage indictment of SA society. Each of these pregnancies is de facto evidence of statutory rape. In a country where gender-based violence is given such a high political profile, the fact that each of these pregnancies should result in prosecution, but is for the most part ignored, highlights how much effort is going to be required to remedy the problem.
A systematic review of the predictors of pregnancy among young people in sub-Saharan Africa[23] found that the most common factors predicting teenage pregnancy included sexual coercion or pressure from male partners; low or incorrect use of contraceptives; lack of parental communication and support, or poor parenting; low socioeconomic status; economic constraints, low income or lack of employment opportunities; and low educational expectations and school dropout. As these issues cut through multiple areas of society, policymakers should focus on addressing them in a holistic manner. In SA, access to a wide range of contraceptive methods and empathetic skilled caregivers is a basic and essential service. It needs to be absolutely prioritised and made available everywhere, but especially in rural and under-served areas.
Study limitations
The results presented in this article reflect teen pregnancy rates of the majority of the population, who use public health services. It excludes teenagers in the highest economic quintile who use the private sector through medical aids. It therefore under-represents the true rates and numbers of teenage births and pregnancies. As the data are based on the DHIS, any quality issues in the data would impact on the results.
Conclusions
Teenage pregnancy in SA is an important and real issue and over the past 5 years has been increasing in all provinces and in each year. There is much that could and should be done to improve this situation, including the provision of age-appropriate and good-quality health education and life skills in schools; tackling sexual and gender-based violence; improving poverty alleviation for the most vulnerable; improving availability of, easy access to and understanding of modern contraception; and ensuring mechanisms to support the high number of young mothers and their infants. All sectors should make better use of digital platforms and community-based channels to improve access to information, support and services to reach teenagers. These factors are all particularly important in the more rural areas and under-served populations of the country.
It is possible to reduce teenage pregnancy rates. In the USA, for example, the adolescent pregnancy rate in 15 - 19-year-olds has been falling continuously since 1991 and in 2019 was 16.7 per 1 000. Although reasons for the declines are not totally clear, evidence suggests that they are due to more teens abstaining from sexual activity and more teens who are sexually active using contraceptives.[24]
Declaration. None.
Acknowledgements. Heather Jacklin and Sara Black read the initial draft of this article and made useful comments. We thank them for their generosity and insights.
Author contributions. The article was conceptualised by PB, HS and YP. Data were extracted by HS and ML. The first draft was written by PB. All authors reviewed the initial draft and contributed to the final article.
Funding. None.
Conflicts of interest. None.
References
1. Save the Children. Teen pregnancies in South Africa jump 60% during COVID-19 pandemic. Press release, 23 August 2021. https://wwwsavethechildren.net/news/teen-pregnancies-south-africa-jump-60-during-covid-19-pandemic (accessed 12 November 2021). [ Links ]
2. O'Regan V. Schoolgirl births 'unacceptably high' in South Africa. Daily Maverick, 7 September 2021. https://www.dailymaverick.co.za/article/2021-09-07-schoolgirl-births-unacceptably-high-in-south-africa/ (accessed 12 November 2021). [ Links ]
3. United Nations Childrens Fund (UNICEF). Early childbearing. May 2021. https://data.unicef.org/topic/child-health/adolescent-health/ (accessed 15 November 2021). [ Links ]
4. Branson N, Ardington C, Leibbrandt M. Health outcomes of children born to teen mothers in Cape Town, South Africa. Econ Dev Cult Change 2015;63(3):589-616. https://doi.org/10.1086/679737 [ Links ]
5. United Nations Childrens Fund (UNICEF). The State of the Worlds Children 2021. On My Mind -Promoting, protecting and caring for children's mental health. New York. UNICEF, October 2021. https://www.unicef.org/reports/state-worlds-children-2021 (accessed 15 November 2021). [ Links ]
6. May J, Witten C, Lake L, eds. South African Child Gauge 2020. Cape Town. Childrens Institute, University of Cape Town, 2020. http://wwwci.uct.ac.za/sites/default/nles/image_tool/images/367/Child_Gauge/South_African_Child_Gauge_2020/ChildGauge_2020_screen_final.pdf (accessed 12 November 2021). [ Links ]
7. National Department of Health (NDoH), Statistics South Africa (Stats SA), South African Medical Research Council (SAMRC), and ICF South Africa Demographic and Health Survey 2016. Pretoria, South Africa, and Rockville, Md, USA. NDoH, Stats SA, SAMRC, and ICF, 2019. https://dhsprogram.com/publications/publication-fr337-dhs-final-reports.cfm (accessed 12 November 2021). [ Links ]
8. Department of Basic Education, South Africa. General Household Survey (GHS). Focus on schooling 2019. Department of Basic Education, March 2021. https://www.education.gov.za/Portals/0/Documents/Reports/General%20Household%20Survey%20(GHS)%20Focus%20on%20Schooling%202019.pdf?ver=2021-06-24-081609-793 (accessed 3 December 2021). [ Links ]
9. Pattinson R. Delivery In. Massyn N, Padarath A, Peer N, Day C, eds. District Health Barometer 2016/17. Durban. Health Systems Trust, 2017.52-71. https://www.hst.org.za/publications/District%20Health%20Barometers/4%20(Section%20A)%20%20%20Deliverypdf (accessed 15 November 2021) [ Links ]
10. World Health Organization. Global Health Observatory data repository Adolescent birth rate. https://apps.who.int/gho/data/node.main.REPAD039 (accessed 1 December 2021). [ Links ]
11. Statistics South Africa. Mid-year population estimates 2017. Statistical release P0302. Pretoria. Government Printer, July 2017. https://wwwstatssa.gov.za/publications/P0302/P03022017.pdf (accessed 1 December 2021). [ Links ]
12. Statistics South Africa. Mid-year population estimates 2018. Statistical release P0302. Pretoria. Government Printer, July 2018. https://wwwstatssa.gov.za/publications/P0302/P03022018.pdf (accessed 1 December 2021). [ Links ]
13. Statistics South Africa. Mid-year population estimates 2019. Statistical release P0302. Pretoria. Government Printer, July 2019. https://wwwstatssa.gov.za/publications/P0302/P03022019.pdf (accessed 1 December 2021). [ Links ]
14. Statistics South Africa. Mid-year population estimates 2020. Statistical release P0302. Pretoria. Government Printer, July 2020. http://wwwstatssa.gov.za/publications/P0302/P03022020.pdf (accessed 1 December 2021). [ Links ]
15. Statistics South Africa. Mid-year population estimates 2021. Statistical release P0302. Pretoria. Government Printer, July 2021. http://wwwstatssa.gov.za/publications/P0302/P03022021.pdf (accessed 1 December 2021). [ Links ]
16. Medical Brief. Focus Public Health. Mounting concern over SAs child and teen pregnancy crisis 1 December 2021. https://www.medicalbriefco.za/mounting-concern-over-sas-child-and-teen-pregnancy-crisis/ (accessed 2 December 2021). [ Links ]
17. Govender P. Big boost to help keep children in school. Sowetan, 16 November 2021. https://www.sowetanlive.co.za/news/south-africa/2021-ll-16-big-boost-to-help-keep-pupils-in-school/ (accessed 18 November 2021). [ Links ]
18. Woldesenbet S, Kufa T, Lombard C, et al. The prevalence of unintended pregnancy and its association with HIV status among pregnant women in South Africa, a national antenatal survey, 2019. Sci Rep 2021,11.23740. https://doi.org/10.1038/s41598-021-03096-z [ Links ]
19. Piliay Y. Towards an AIDS-free generation by 2030. How are South African children, adolescents caregivers and health care workers coping with HIV? S Afr J Psychol 2021;51(3):1-7. https://doi.org/10.1177/0081246321992175 [ Links ]
20. Johnson LF, May MT, Dorrington RE, et al. Estimating the impact of antiretroviral treatment on adult mortality trends in South Africa. A mathematical modelling study. PLoS Med 2017;14(12):e1002468. https://doi.org/10.1371/journal.pmed.l002468 [ Links ]
21. Badusa M, Chaskalson J. Opinion. Funding must be allocated to treat drivers of HIV. Spotlight, 30 November 2021. https://www.spotlightnsp.co.za/2021/ll/30/opinion-funding-must-be-allocated-to-treat-drivers-of-hiv/ (accessed 3 December 2021). [ Links ]
22. Department of Basic Education, South Africa. Teenage pregnancy & comprehensive sexuality e 7 September 2021. https://pmg.org.za/committee-meeting/33580/ (accessed 7 December 2021). [ Links ]
23. Gunawardena N, Fantaye AW, Yaya S. Predictors of pregnancy among young people in sub-Saharan Africa. A systematic review and narrative synthesis. BMJ Glob Health 2019,4.eOO 1499. https://doi.org/10.1136/bmjgh-2019-001499 [ Links ]
24. Centers for Disease Control and Prevention, USA. About teen pregnancy. Last reviewed 15 November 2021. https://www.cdc.gov/teenpregnancy/about/index.htm (accessed 5 December 2021). [ Links ]
 Correspondence:
Correspondence:
P Barron
pbarron@iafrica.com
Accepted 10 January 2022


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}