










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.112 no.3 Pretoria Mar. 2022
http://dx.doi.org/10.7196/SAMJ.2022.v112i3.16184
IN PRACTICE
HEALTHCARE DELIVERY
Perspectives on gestational diabetes mellitus in South Africa
V NicolaouI; N LevittII; K HuddleIII; L SoepnelIV; S A NorrisV, VI
IMB BCh, PhD; SAMRC/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMB ChB, MD; Chronic Disease Initiative for Africa, Department of Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
IIIMB BCh; Department of Internal Medicine, Chris Hani Baragwanath Academic Hospital and Faculty of Health Sciences, University of the Witwatersrand., Johannesburg, South Africa
IVMD, PhD; SAMRC/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VMSc, PhD; SAMRC/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIMSc, PhD; Global Health Research Institute, School of Human Development and Health, University of Southampton, UK
ABSTRACT
The field of gestational diabetes mellitus has attracted increasing attention and research in South Africa (SA) over the past decade, creating a better understanding of the disease burden, risk factors, availability of specialised healthcare services, and importantly the far-reaching maternal and childhood consequences beyond the pregnancy. This article brings together all the local published literature in the field and outlines the implications of this condition, together with recommendations regarding particular areas that require attention in order to prevent and alleviate the disease burden in SA.
Gestational diabetes mellitus (GDM) has increasingly become a global burden alongside the obesity epidemic. According to the latest International Diabetes Federation data (2019),[1] 16% of live births globally had some form of hyperglycaemia in pregnancy, of which 84% was due to GDM. Concerningly, the vast majority of cases arise from low- to middle-income countries (LMICs).[2]
Worldwide, the landscape of GDM has remained a dynamic entity with the prevalence, terminology, screening protocols and diagnostic criteria continuously changing from as early as the 1980s. The varying terminology employed to define GDM was modified by the World Health Organization (WHO) in 2013[3] following the findings of the Hyperglycemia and Adverse Pregnancy Outcome Study (HAPO),[4] which reported that blood glucose thresholds below recognised or accepted GDM diagnostic criteria at the time were linked to adverse maternal and neonatal outcomes. The term 'hyperglycaemia first detected in pregnancy' (HFDP), coined by the WHO in 2013, encompasses the varying degrees of glucose intolerance detected in pregnancy, with GDM being the milder degree of HFDP and diabetes in pregnancy (DIP) the more severe form, and will be utilised for the purposes of this article.
Globally there is a lack of uniformity in the approach to HFDP among both international and local organisations, translating into variations in practice within and between countries. Additionally LMICs often have to adopt different strategies given their limited resource infrastructure and lack of availability of diabetes care, particularly in pregnancy. This is the case in South Africa (SA), where limited access to specialised maternal health services remains an issue, together with variations in clinical practice across provinces. In those provinces where specialised maternal services are available, health system governance differs. For example, Western Cape Province adopts a decentralised service in comparison with the centralised services in Gauteng. This difference translates into differences in healthcare delivery in terms of equity, efficiency and resilience. The growing body of research in the field of HFDP over the past decade has highlighted numerous shortfalls in healthcare delivery in SA, in addition to the health burden and consequences of HFDP.[5-14]
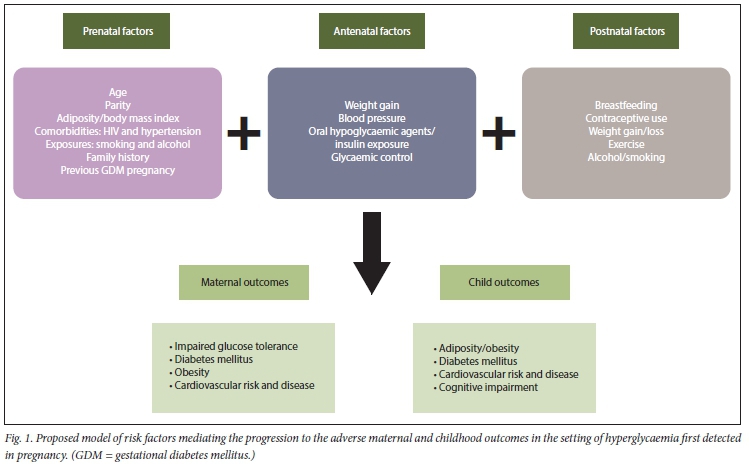
The significance of HFDP lies in the well-established short- and more recently explored long-term ramifications for both mother and child, ultimately augmenting the intergenerational risk of cardiometabolic diseases. Of profound concern is that HFDP is fuelling the type 2 diabetes mellitus (T2DM) epidemic, with over half the mothers developing diabetes within the first decade following delivery, making HFDP one of the strongest predictors of T2DM.[15,16] Cardiovascular disease (CVD) and the metabolic syndrome (MetS) are two times[17] and four times[18] higher among women with a previous history of HFDP compared with women without HFDP. Furthermore, studies have shown that the offspring of women with HFDP are at increased risk of T2DM, obesity and CVD.[19-21] The HAPO follow-up study[22] demonstrated that exposure to higher levels of glucose in utero is independently associated with childhood adiposity and that offspring exposed to untreated GDM in utero are insulin resistant, with limited beta-cell compensation compared with offspring of mothers without GDM. The impact of exposure to HFDP in the offspring may extend beyond the cardiometabolic consequences, and it has been suggested that it may adversely affect childhood cognitive and motor development, as explored in two recent systematic reviews of data largely from high-income countries.[23,24]
Although the underlying pathophysiological mechanisms for the increased cardiometabolic risk in mothers and children following HFDP remain to be fully elucidated, the risk is augmented by various maternal, environmental and societal factors present along the life course. In the context of HFDP exposure, the model in Fig. 1 highlights the complex interplay of modifiable and non-modifiable maternal factors present from the prenatal period and extending well into the postpartum period that potentially interact and mediate the outcomes.
Fortunately, there is now a growing body of research in SA highlighting the burden and risk factors for HFDP, as well as maternal, neonatal and early childhood outcomes following HFDP, [5,6,8,10,11,14,25-31]
The burden of HFDP in SA
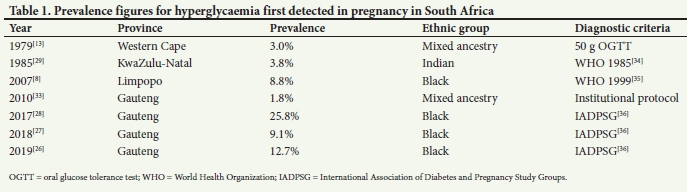
Urbanisation and recent socioeconomic changes in SA have fuelled a rapid nutritional transition that has been accompanied by a dramatic shift in the burden of disease from communicable diseases, such as HIV, to non-communicable diseases (NCDs) such as diabetes mellitus and HFDP.[32] Prevalence studies of HFDP for SA are limited to seven studies in the past four decades, [8,13,26,29,33] in which the prevalence ranged from 1.8% to 25.8% owing to varying screening strategies and diagnostic tests being employed. However, three of the studies performed in Gauteng, all of which utilised the same diagnostic criteria (International Association of Diabetes and Pregnancy Study Groups (IADPSG)), demonstrated markedly varying prevalence figures of 9.1%, 12.7% and 25.8%. These differences may have been attributable to laboratory inaccuracies, including higher quality control biases at lower glucose concentrations, resulting in a higher prevalence of HFDP. Table 1 demonstrates the varying prevalences by ethnic groups, diagnostic criteria, and provinces in SA.
A concern is the potential underestimation of this disease burden, which may be attributable to three major factors: (i) the current risk factor-based screening approach, as opposed to universal screening for HFDP; (ii) the lack of public and healthcare professional awareness of the condition; and (ii) the primary healthcare services mostly providing a selective, vertically based care for diseases, as opposed to comprehensive care that incorporates health promotion and disease prevention. The primary healthcare services, which are generally the first port of call for pregnant women, are often fraught with difficulties, from problems with access to lack of continuity of care and understaffing, bringing into question the true appreciation of the disease burden. While risk factor-based screening remains the cornerstone of screening strategies in LMICs owing to its cost and ease, numerous studies[37,38] have demonstrated the poor predictive value of this approach to screening, with a local study[28] showing that 10.6% of HFDP cases would have been missed.
Availability of specialised antenatal maternal services
There is limited availability of maternal services dedicated to the care of women with HFDP, and these are exclusively offered at three tertiary hospital sites (public health sector) located in Gauteng and Western Cape, home to 23 million of SAs 60 million population.[39] These centres have afforded excellent care and management over the years, which has become evident in the improved outcomes for both mother and child.[6,12,25] However, there is limited access to quality care for the majority of women in rural and urban areas outside of Gauteng and Cape Town.
Varying screening and diagnostic strategies and novel testing
While oral glucose tolerance tests (OGTTs) remain the gold standard for diagnosing HFDP, difficulties arise because varying diagnostic criteria are employed worldwide, with four commonly used criteria being utilised in SA. These are the National Institute for Health and Care Excellence (NICE),[40] the IADPSG,[41] the American College of Obstetricians and Gynecologists (ACOG)[42] and the WHO 2013.[3] In 2017, the Society for Endocrinology, Metabolism and Diabetes of South Africa published guidelines that endorsed universal screening and the IADPSG criteria.[43] The application of these criteria is currently still debatable and not endorsed by the South African Society of Obstetricians and Gynaecologists, as it remains unfeasible in a resource-strapped country such as SA, where more diagnosed cases, because of the lower glycaemic thresholds, will add to the
cost burden and may overwhelm the existing healthcare system. The OGTT remains cumbersome. It is often associated with nausea and occasionally with vomiting, necessitates multiple blood samples and importantly is expensive, which has led to the evaluation of simpler novel tests such as fasting plasma glucose (FPG), glycated haemoglobin (HbAlc) and other biomarkers. FPG has shown promise as both a screening[11,44]and diagnostic test,[27,28] with a recent local study showing that an FPG level >4.5 mmol/L has a sensitivity and specificity of 98% and 80%, respectively, for identifying HFDP v. risk factor-based screening, where the sensitivity and specificity were 56% and 67%, respectively[11] Use of FPG as a diagnostic test is limited by the fact that women need to be in the fasting state and to return for their result if the test is not performed by a point-of-care device, which itself is also limited by quality control issues. Although random blood glucose and HbAlc measurements are convenient fast, simple and relatively inexpensive, they have shown inconsistent sensitivity and specificity results, which is a major limiting factor. A further novel strategy, investigated in a small cross-over study at Tygerberg Hospital in 51 participants, was a 'breakfast test' - a non-standardised glucose load of 75 g v. the standard OGTT. This study reported a good correlation between blood glucose values, suggesting a useful alternative to the non-palatable OGTT.[9] However, a major limitation of the study was small numbers, and the findings would require validation in an adequately powered study
Postpartum screening
Postpartum care for women with HFDP appears to be poorly structured and misaligned with existing policy. Follow-up is often lacking and, if available, poorly attended. The determinants and barriers are generally consistent across studies (mostly derived from high- to middle-income countries); however, many are contextual and culture specific.[45] In the SA setting, a qualitative study identified health and patient-related barriers as major obstacles in the context of three public sector hospitals in Western Cape and Gauteng, resulting in poor compliance with follow-up.[46] Among others, financial constraints, time constraints and misalignment of neonatal and maternal follow-up at primary care level, and lack of education and awareness surrounding the importance of follow-up, were reported.
The lack of awareness and perceived seriousness of the long-term impact of HFDP among policymakers, healthcare providers, affected women and their families may be the biggest hurdle. However, there are data from recent SA studies[14,30,31] highlighting the significant maternal cardiometabolic risks following pregnancy and therefore the need to prioritise postpartum surveillance. These were prospective cohort studies. One, performed in Cape Town in a predominantly mixed ethnic group of women, found that at 6 weeks postpartum the prevalence of T2DM was 27%,[14] although this was a small study. Another larger study in the same region at 5 - 6 years postpartum demonstrated that 47% of women with HFDP progressed to T2DM (81% in the DIP group and 31% in the GDM group), of whom the majority were unaware of their disease and 60.9% met criteria for MetS.[30] In both studies, the majority of the women who progressed to T2DM probably had pre-existing diabetes, since they were found to have overt diabetes by IADPSG criteria. The latest prospective cohort study, currently under review for publication (V Nicolaou et al, unpublished data), evaluated mother-child pairs exposed and unexposed to HFDP at 3-6 years postpartum. In this study, 45% of women exposed to HFDP progressed to T2DM compared with 5% of women who did not have HFDP. Similarly, 41% of the women exposed to HFDP v. 6% of women who did not have HFDP, had MetS. Cardiovascular risk as assessed by the Framingham risk score and carotid intima media thickness was also significantly higher among women exposed to HFDP.
In the last of the three studies, it is of significant concern that the offspring of mothers with HFDP were found to have cognitive impairment, with lower cognitive scores and fine motor skills. In this study, offspring obesity and height were not independently associated with HFDP when adjusting for maternal BMI.[47] Longer prospective follow-up may unmask this consequence in later childhood. For example, a recent study under review for publication (T Chivese et al, unpublished data) of children 5-6 years of age who had been born to mothers with HFDP showed a significant combined prevalence of overweight and obesity at preschool age of 26.5%, although no comparison was made with an unexposed group of children.
The HIV epidemic has brought about the development of healthcare platforms that could be expanded for use for women with HFDP and their offspring. The country's prevention of mother-to-child (PMTC) infection programme has been one of the flagship programmes in the government's efforts to curb the spread of HIV, particularly among the vulnerable of society - women and children. Applying similar principles to women and children exposed to HFDP wouldbe beneficial. Attention should be focused on integrating healthcare services to address the multiple morbidities in the postpartum period. This can be achieved through better continuity of care, which includes the transfer of patients from obstetrics and paediatrics to primary care to provide ongoing screening for NCDs such as T2DM, hypertension, dyslipidaemia and obesity, as well as counselling regarding lifestyle modifications, and initiating therapeutic interventions where necessary[48-51]
Implications
Until recently, the emphasis from an obstetrics point of view in SA has been on acute obstetric complications that affect early maternal and infant mortality, so HFDP has been largely neglected. Based on our local data, urgent action is called for in SA. These findings have highlighted that HFDP is not just a transient obstetric condition, but identifies a significant risk for future cardiometabolic health in mothers. As the prevalence of HFDP and its risk factors increases, this can increasingly contribute to the NCD burden that already drives mortality and morbidity in SA and that exacerbates the dire consequences of health emergencies such as the ongoing COVID-19 pandemic.[52] Moreover, the emerging evidence for an intergenerational impact of HFDP on the next generation's health and development indicates the need to break this cycle to optimise the health of SA children, to improve their ability to reach their developmental potential, and to curb the longer-term CVD and NCD burden in SA by reducing early-life risks. Addressing modifiable maternal risk factors is key in preventing these consequences of HFDP.
Recommendations
The health of women and children is central to building a healthy and stable society. Our current healthcare system fails to meet the needs of women and children exposed to HFDP and may remain as such given our current economic climate. Attention should be focused on improving and expanding health services through laws, policies and programmes that will aid in improving the health of our women and children. The proposed National Health Insurance would provide the ideal opportunity for an integrated package of care for affected women and children. Preconception care programmes that optimise the health of women before pregnancy, as described in recommendations from the International Federation of Gynaecology and Obstetrics (FIGO), could help prevent the onset of HFDP, and the implementation and evaluation of such interventions should be further explored in our setting. While screening for HFDP in pregnancy should ideally be universal, this may be difficult to achieve in the current economic climate, which necessitates the exploration of novel, inexpensive and convenient testing for all pregnant women that is as effective as the gold standard. Furthermore, consideration should be given to an integrated seamless service, as showcased in the PMTC programme, where both mother and child can receive routine care in the postpartum period involving screening for chronic NCDs such as T2DM with a focus on the reduction of risk through preventive strategies including weight loss among others. Exploring and confirming the usefulness of FPG as a screening test for T2DM would simplify screening and hence have a major impact on health services.
Conclusions
A multidisciplinary approach to HFDP in SA, from prevention to screening, management and postpartum care, is critical to reduce the disease burden together with the short- and long-term impact on mothers and their offspring. An HFDP study group of researchers, interested obstetricians, physicians, endocrinologists, paediatricians, diabetes nurses, dieticians and public health and health authorities is called for to drive this agenda.
Declaration. None.
Acknowledgements. VN was supported by the South African Medical Research Council and SAN by the DSI-NRF Centre of Excellence in Human Development at the University of the Witwatersrand.
Author contributions. VN and SN conceptualised the article. VN wrote the initial version of the manuscript, and all the authors contributed to editing and revising the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. International Diabetes Federation. IDF Diabetes Atlas 9th ed., 2019. https://wwwdiabetesatlas.org/en/ (accessed 7 September 2020). [ Links ]
2. Ogurtsova K, da Rocha Fernandes JD, Huang Y, et al. IDF Diabetes Atlas. Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract 2017;12:40-50. https://doi.org/10.1016/j.diabres.2017.03.024 [ Links ]
3. Diagnostic criteria and Classification of hyperglycaemia first detected in pregnancy. A World Health Organization guideline. Diabetes Res 2013;103(3):341-363. https://doi.org/doi.org/10.1016/j.diabres.2013.10.012 [ Links ]
4. Catalano PM, Mclntyre HD, Cruickshank JK, et al. The Hyperglycemia and Adverse Pregnancy Outcome Study. Associations of GDM and obesity with pregnancy outcomes. Diabetes Care 2012;35(4):780-786. https://doi.org/10.2337/dcll-1790 [ Links ]
5. Huddle K, England M, Nagar A. Outcome of pregnancy in diabetic women in Soweto, South Africa 1983 - 1992. Diabet Med 1993;10(3):290-294. https://doi.org/10.1111/j.l464-5491.1993.tb00062.x [ Links ]
6. Huddle KR Audit of the outcome of pregnancy in diabetic women in Soweto, South Africa, 1992 -2002. S Afr Med J 2005;95(10):789. https://doi.org/10.7196/SAMJ.1862 [ Links ]
7. Soepnel LM, Nicolaou V, Huddle KRL, Klipstein-Grobusch K, Levitt NS, Norris SA. Maternal and neonatal outcomes following a diabetic pregnancy within the context of HIV. Int J Gynecol Obstet 2019;147(3):404-412. https://doi.org/10.1002/ijgo.12956 [ Links ]
8. Mamabolo RL, Alberts M, Levitt NS, Delemarre-van de Waal HA, Steyn NP Prevalence of gestational diabetes mellitus and the effect of weight on measures of insulin secretion and insulin resistance in third-trimester pregnant rural women residing in the Central Region of Limpopo Province, South Africa. Diabet Med 2007;24(3):233-239. https://doi.org/10.1111/j.l464-5491.2006.02073.x [ Links ]
9. Marais C, Hall DR van Wyk L, Conradie M. Randomized cross-over trial comparing the diagnosis of gestational diabetes by oral glucose tolerance test and a designed breakfast glucose profile. Int J Gynecol Obstet 2018;141(1):85-90. https://doi.org/10.1002/ijgo.12427 [ Links ]
10. Dias S, Pheiffer C, Rheeder P, Adam S. Screening and diagnosis of gestational diabetes mellitus in South Africa. What we know so far. S Afr Med J 2019;109(7):457-462. https://doi.org/10.7196/SAMJ.2019.v109i7.14064 [ Links ]
11. Dickson LM, Buchmann EJ, Janse van Rensburg C, Norris SA. Fasting plasma glucose and risk factor assessment. Comparing sensitivity and specificity in identifying gestational diabetes in urban black African women. S Afr Med J 2020;110(1):21-26. https://doi.org/10.7196/SAMJ.2019.v110il.14089 [ Links ]
12. Van Zyl H, Levitt NS. Pregnancy outcome in patients with pregestational and gestational diabetes attending Groote Schuur Hospital, Cape Town, South Africa. S Afr Med J 2018;108(9):772-776. https://doi.org/10.7196/SAMJ.2018.v108i9.12992 [ Links ]
13. Coetzee EJ, Jackson WP Diabetes newly diagnosed during pregnancy. A 4-year study at Groote Schuur Hospital. S Afr Med J 1979;56(12):467-475. [ Links ]
14. Coetzee A, Mason D, Hall DR, Conradie M. Prevalence and predictive factors of early postpartum diabetes among women with gestational diabetes in a single-center cohort. Int J Gynecol Obstet 2018;142(1):54-60. https://doi.org/10.1002/ijgo.12494 [ Links ]
15. Bellamy L, Casas JP, Hingorani AD, Wilhams D. Type 2 diabetes mellitus after gestational diabetes. A systematic review and meta-analysis. Lancet 2009;373(9677):1773-1779. https://doi.org/10.1016/S0140-6736(09)60731-5 [ Links ]
16. Song C, Lyu Y, Li C, et al. Long-term risk of diabetes in women at varying durations after gestational diabetes. A systematic review and meta-analysis with more than 2 million women. Obes Rev 2018;19(3):421-429. https://doi.org/10.1111/obr.l2645 [ Links ]
17. Kramer CK, Campbell S, Retnakaran R. Gestational diabetes and the risk of cardiovascular disease in women. A systematic review and meta-analysis. Diabetologia 2019;62(6):905-914. https://doi.org/10.1007/s00125-019-4840-2 [ Links ]
18. Xu Y, Shen S, Sun L, Yang H, Jin B, Cao X. Metabolic syndrome risk after gestational diabetes. A systematic review and meta-analysis. PLoS ONE 2014;9(1):e87863. https://doi.org/10.1371/journal.pone.0087863 [ Links ]
19. Clausen TD, Mathiesen ER, Hansen T, et al. High prevalence of type 2 diabetes and pre-diabetes in adult offspring of women with gestational diabetes mellitus or type 1 diabetes. The role of intrauterine hyperglycemia. Diabetes Care 2008;31(2):340-346. https://doi.org/10.2337/dc07-1596 [ Links ]
20. Catalano PM. The impact of gestational diabetes and maternal obesity on the moth er and her offspring J Dev Orig Health Dis 2010;1(4):208-215. https://doi.org/10.1017/S2040174410000115 [ Links ]
21. Pathirana MM, Lassi ZS, Roberts CT, Andraweera PH. Cardiovascular riskfactors in offspring expose to gestational diabetes mellitus in utero. Systematic review and meta-analysis.J Dev Orig Health Dis 2020;11(6):599-616. https://doi.org/10.1017/S2040174419000850 [ Links ]
22. Scholtens DM, Metzger BE. Hyperglycemia and Adverse Pregnancy Outcome Follow-up Study (HAPO FUS). Maternal glycemia and childhood glucose metabolism. Diabetes Care 2019;42(7):e128-e129. https://doi.org/10.2337/dci19-0024 [ Links ]
23. Adane AA, Mishra GD, Tooth LR Diabetes in pregnancy and childhood cognitive development. A systematic review. Pediatrics 2016;137(5):e20154234. https://doi.org/10.1542/peds.2015-4234 [ Links ]
24. Robles MC, Campoy C, Garcia Fernandez L, Lopez-Pedrosa JM, Rueda R, Martin MJ. Maternal diabetes and cognitive performance in the offspring. A systematic review and meta-analysis. PLoS ONE 2015;10(11):e0142583. https://doi.org/10.1371/journal.pone.0142583 [ Links ]
25. Soepnel LM, Nicolaou V, Huddle KRL, Klipstein-Grobusch K, Levitt NS, Norris SA. Maternal and neonatal outcomes following a diabetic pregnancy within the context of HIV. Int J Gynecol Obstet 2019;147(3):404-412. https://doi.org/10.1002/ijgo.12956 [ Links ]
26. Dickson LM, Buchmann EJ, Janse van Rensburg C, Norris SA. Accuracy of five plasma calibrated glucometers to screen for and diagnose gestational diabetes mellitus in a low resource clinic setting. J Clin Transl Endocrinol 2019;16:100174. https://doi.org/10.1016/J.JCTE.2018.12.003 [ Links ]
27. Macaulay S, Ngobeni M, Dunger DB, Norris SA. The prevalence of gestational diabetes mellitus amongst black South African women is a public health concern. Diabetes Res Clin Pract 2018;139:278-287. https://doi.org/10.1016/j.diabres.2018.03.012 [ Links ]
28. Adam S, Rheeder P. Screening for gestational diabetes mellitus in a South African population. Prevalence, comparison of diagnostic criteria and the role of riskfactors. S Afr Med J 2017;107(6).523-527. https://doi.org/10.7196/SAMJ.2017.v107i6.12043 [ Links ]
29. Ranchod HA, Vaughan JE, Jarvis P. Incidence of gestational diabetes at Northdale Hospital, Pietermaritzburg. S Afr Med J 1991:80(1):14-16. [ Links ]
30. Chivese T, Norris SA, Levitt NS. Progression to type 2 diabetes mellitus and associated risk factors after hyperglycemia first detected in pregnancy. A cross-sectional study in Cape Town, South Africa. PLoS Med 2019;16(9):e1002865. https://doi.org/10.1371/journal.pmed.1002865 [ Links ]
31. Chivese T, Norris SA, Levitt NS. High prevalence of cardiovascular riskfactors and insulin resistance 6 years after hyperglycemia first detected in pregnancy in Cape Town, South Africa. BMJ Open Diabetes Res Care 2019;7:e000740.https://doi.org/10.1136/bmjdrc-2019-000740 [ Links ]
32. Nnyepi MS, Gwisai N, Lekgoa M, Seru T. Evidence of nutrition transition in southern Africa. Proc Nutr Soc 2015;74(4):478-486. https://doi.org/10.1017/S0029665115000051 [ Links ]
33. Basu JK, Jeketera CM, Basu D. Obesity and its outcomes among pregnant South African women. Int J Gynaecol Obstet 2010;110(2):101-104. https://doi.org/10.1016/j.ijgo.2010.02.020 [ Links ]
34. World Health Organization. Diabetes mellitus. Report of a WHO Study Group. WHO, 1985. http://apps.who.int/iris/bitstream/handIe/10665/39592/WHO_TRS_727.pdf,jsessionid=D9BCBC8AlCClEB20C3CA5BF6D150020A?sequence=1 (accessed 24 January 2022). [ Links ]
35. World Health Organization. Definition, diagnosis and classification of diabetes mellitus and its complications. Report of a WHO consultation. Part 1. Diagnosis and classification of diabetes mellitus. WHO, 1999. https://apps.who.int/iris/handie/10665/66040 (accessed 14 September 2021). [ Links ]
36. International Association of Diabetes and Pregnancy Study Groups Consensus Panel International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010;33(3):676-682. https://doi.org/10.2337/dc09-1848 [ Links ]
37. Matta-Coelho C, Monteiro AM, Fernandes V, et al. Universal vs. risk-factor-based screening for gestational diabetes - an analysis from a 5-year Portuguese cohort. Endocrine 2019;63(3):507-512. https://doi.org/10.1007/s12020-018-1760-8 [ Links ]
38. Miaiihe G, Kayem G, Girard G, Legardeur H, Mandelbrot L. Selective rather than universal screening for gestational diabetes mellitus? Eur J Obstet Gynecol Reprod Biol 2015;191:95-100. https://doi.org/10.1016/j.ejogrb.2015.05.003 [ Links ]
39. Statistics South Africa. Mid-year population estimates 2021. Statistical release P0302, July 2021. http://www.statssa.gov.za/publications/P0302/P03022021.pdf (accessed 13 September 2021). [ Links ]
40. National Institute for Health and Care Excellence (NICE). Diabetes in pregnancy. Management from preconception to the postnatal period. NICE guideline (NG3). 25 February 2015. https://www.nice.org.uk/guidance/ng3 (accessed 16 January 2021). [ Links ]
41. Duran A, Sáenz S, Torrejón MJ, et aL Introduction of IADPSG criteria for the screening and diagnosis of gestational diabetes mellitus results in improved pregnancy outcomes at a lower cost in a large cohort of pregnant women. The St Carlos Gestational Diabetes Study. Diabetes Care 2014;37(9):2442-2450. https://doi.org/10.2337/dc14-0179 [ Links ]
42. ObG Project. Updated ACOG guidance on gestational diabetes. 2017. https://www.obgproject.com/2017/06/25/acog-releases-updated-guidance-gestational-diabetes/ (accessed 5 May 2021). [ Links ]
43. Nicolaou V, Huddle KR. SEMDSA 2017 Guidelines for the Management of Type 2 Diabetes Mellitus. J Endocrinol Metab Diabetes S Afr 2017;22(1 Suppl 1):51-S196. [ Links ]
44. Agarwal MM, Dhatt GS, Shah SM. Gestational diabetes mellitus. Simplifying the International Association of Diabetes and Pregnancy diagnostic algorithm using fasting plasma glucose. Diabetes Care 2010;33(9):2018-2020. https://doi.org/10.2337/dc10-0572 [ Links ]
45. Nielsen KK, Kapur A, Damm P, de Courten M, Bygbjerg IC. From screening to postpartum follow-up - the determinants and barriers for gestational diabetes mellitus (GDM) services, a systematic review. BMC Pregnancy Childbirth 2014;14:41. https://doi.org/10.1186/1471-2393-14-41 [ Links ]
46. Muhwava LS, Murphy K, Zarowsky C, Levitt N. Policies and clinical practices relating to the management of gestational diabetes mellitus in the public health sector, South Africa - a qualitative study. BMC Health Serv Res 2018;18:349. https://doi.org/10.1186/sl2913-018-3175-x [ Links ]
47. Soepnel LM, Nicolaou V, Slater C, et al. Obesity and adiposity of 3- to 6-year-old children born to mothers with hyperglycaemia first detected in pregnancy in an urban South African setting. Ann Hum Biol 2021;48(2):81-92. https://doi.org/10.1080/03014460.2021.1918245 [ Links ]
48. Cabizuca CA, Rocha PS, Marques JV, et al. Postpartum follow up of gestational diabetes in a tertiary care center. Diabetol Metab Syndr 2018;10:2. https://doi.org/10.1186/sl3098-017-0303-4 [ Links ]
49. Ratner RE. Prevention of type 2 diabetes in women with previous gestational diabetes. Diabetes Care 2007;30(Suppl 2):S242-S245. https://doi.org/10.2337/dc07-s223 [ Links ]
50. Xiang AH, Peters RK, Kjos SL, et al. Effect of pioglitazone on pancreatic ß-celi function and diabetes risk in Hispanic women with prior gestational diabetes. Diabetes 2006;55(2):517-522. https://doi.org/10.2337/diabetes.55.02.06.db05-1066 [ Links ]
51. Hedeager Momsen AM, Hotoft D, Ortenblad L, et al. Diabetes prevention interventions for women after gestational diabetes mellitus. An overview of reviews. Endocrinol Diabetes Metab 2021;4(3):e00230. https://doi.org/10.1002/EDM2.230 [ Links ]
52. Nyasulu J, Pandya H. The effects of Coronavirus disease 2019 pandemic on the South African health system. A call to maintain essential health services. Afr J Prim Health Care Fam Med 2020;12(1):e1-e5. https://doi.org/10.4102/phcfm.v12il.2480 [ Links ]
 Correspondence:
Correspondence:
V Nicolaou
docvic9@gmail.com
Accepted 15 November 2021


{kind=link}
{kind=link}