










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.111 no.9 Pretoria Set. 2021
http://dx.doi.org/10.7196/SAMJ.2021.v111i9.15664
RESEARCH
The incidence of fragility hip fractures in a subpopulation of South Africa
M L GrundillI; M C BurgerII
IMB ChB, MMed (Orth), FC Orth (SA); Department of Orthopaedic Surgery, Livingstone Tertiary Hospital, Port Elizabeth, South Africa
IIBSc, BMedSc Hons, MMedSc, PhD; Division of Orthopaedic Surgery, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
ABSTRACT
BACKGROUND. Fragility hip fractures (FHFs) are associated with significant morbidity, mortality and burden on the healthcare system. European and North American literature suggests that the worldwide incidence of FHFs is increasing, but very little is known about the incidence of FHFs in Africa and South Africa (SA). Historically FHFs were believed to be uncommon in black African populations, but recent studies have shown a marked increase in the incidence compared with the early literature.
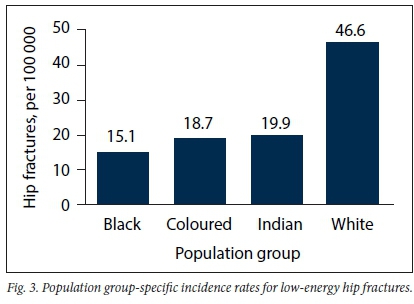
OBJECTIVES. To investigate the age-, gender- and population group-specific incidences of FHFs in a subpopulation in Eastern Cape Province, SA. Methods. A retrospective review of all patients presenting with FHFs was performed at a tertiary hospital in the Eastern Cape over a 1-year period. Age-, gender- and population group-specific incidence rates were calculated for 5-year age intervals using the age distribution data of the western region of the Eastern Cape (WREC) as a denominator for each age group. Overall crude incidence rates were calculated by using the sum total of FHFs, divided by the study population. All incidences were calculated as number of fractures per 100 000 people annually. Results. A total of 253 patients with FHFs were included. The crude incidence rate of low-energy hip fractures in the WREC was 19.3 per 100 000 (males 14.6, females 23.4) over the study period. Population group-specific incidences were 15.1, 18.7, 19.9 and 46.6 per 100 000 for black, coloured, Indian and white population groups, respectively. The highest number of low-energy hip fractures in females occurred in the >85-year (19.6%) and 70 - 74-year (16.5%) age groups, with the highest number of male cases observed in the 60 - 64-year group (20.2%). The highest frequency distribution of FHFs was observed in black males aged 60 - 64 years (5.5%; n=14) and black females aged 70 - 74 years (6.3%; n=16).
CONCLUSIONS. The local incidence of FHFs is higher than initially reported, but when compared with other countries remains on the lower end of spectrum. A large proportion of FHFs are occurring in young patients (<65 years). These findings warrant further investigation that may prompt the development of preventive strategies and optimal treatment programmes.
Fragility hip fracture (FHF) is a common medical problem associated with significant morbidity and mortality and a considerable economic burden. The 1-year mortality rate for FHF has been reported to be as high as 30%,[1] with the global cost per patient averaging USD43 669 for the first year.[2] The literature suggests that the worldwide incidence of FHF is increasing and has the potential to exceed 6.3 million cases by 2050.[3-5] The main driver of this increase appears to be a growing elderly population and improved healthcare.[6! However, most literature on the subject stems from populations in Europe and North America, with few studies investigating African countries where traditional risk factors are compounded by extreme poverty, malnutrition and a differing disease burden.
Historically FHFs were believed to be uncommon in black African populations, with some evidence attributing this to differences in bone mineral density and hip geometry.[7-11] Until recently, the only literature available on hip fractures in South Africa (SA) was published by Solomon[9! in 1968, focusing on a small subpopulation of black South Africans in Johannesburg, which reported low incidence rates of 4.2 and 4.6 per 100 000 for males and females, respectively. This reported incidence is surprisingly low when compared with Scandinavian countries such as Denmark, with 290 and 574 per
100 000 for males and females, respectively.[4] Work has subsequently been published focusing on another black African subpopulation in the eThekwini region of KwaZulu-Natal.[12] This study showed a 10-fold increase in incidence compared with previous data. Most recently, a multicentre study involving three of the nine provinces of SA has supported a marked increase in incidence, with rates of 46.2 and 87.7 per 100 000 for males and females, respectively.[3] It appears that the incidence of FHFs in the SA population has been underestimated, but there is not currently a data set encompassing all geographical regions of the country, including the rural areas. Understanding differences in incidence rates of hip fractures will contribute to a more complete view of the SA hip fracture burden and has implications for the way we screen, prevent and treat FHFs in our population. Furthering our understanding of FHFs in SA will guide the allocation of resources, as well as highlight opportunities for preventive measures.
Objectives
To investigate age-, gender- and population group-specific incidences of FHFs in a subpopulation in Eastern Cape Province, SA, a population that has not previously been investigated.
Methods
A retrospective review of hospital medical records of all patients presenting with FHFs was performed at Livingstone Tertiary Hospital in the Eastern Cape over a 1-year period (1 April 2014 - 30 March 2015). The study was conducted according to the ethical guidelines and principles of the International Declaration of Helsinki and the South African Guidelines for Good Clinical Practice. Ethical approval was obtained from the Faculty of Health Sciences Research Ethics and Bio-Safety Committee at the affiliated university, Walter Sisulu University (ref. no. 079/2017).
Livingstone Hospital serves the western region of the Eastern Cape (WREC), with a population of 1 602 699 people in 2011 (the year of the last formal census in SA). According to Statistics South Africa, the population group distribution of the Eastern Cape in 2011 was 86.3% black African, 8.3% coloured, 0.4% Indian/Asian, 4.7% white and 0.3% other.[14] For the purpose of this study it was important to distinguish between the various population groups in SA, as literature from other regions has shown potential differences in FHF incidence between population groups. The HIV prevalence in the Eastern Cape is 19.9%.[15]
It can be assumed that a proportion of the population in the WREC will make use of a private health facility should they sustain an FHF. In the Eastern Cape, 18.2% make use of the private healthcare sector.[14] It is therefore estimated that the population that makes use of Livingstone Hospital is ~1 311 008 people (total population of the WREC less the 18.2% of patients who make use of private healthcare).
All patients presenting with FHFs were included. An FHF is defined as a fracture that occurs as a result of low-energy trauma, e.g. a fall from a standing height or while walking.[16] A hip fracture refers to a fracture of the proximal femur to ~5 cm below the lower border of the lesser trochanter, and includes neck of femur fractures, intertrochanteric fractures and subtrochanteric fractures.[17]
Patient records were utilised to collect information on patient demographics, including age, gender and ethnic group. Information about diagnosis and mechanisms of injury was also collected, and medical records were cross-referenced with operating theatre records to ensure accuracy. All diagnoses of hip fractures were confirmed with the X-ray database (Picture Archiving and Communications System).
The total number of FHFs seen at Livingstone Hospital during the study period was calculated, while the size of the study population was calculated as previously described. Age-, gender- and population group-specific incidence rates were calculated for 5-year age intervals using the age distribution data of the WREC as a denominator for each age group. Overall crude incidence rates were calculated by using the sum total of FHFs divided by the study population (1 311 008). Five-year age intervals were chosen because this is the standard representation reported in the literature.
In order to negate the confounding influence of age and gender on overall crude incidence rates, age and gender adjustment is necessary so that comparison can be made with other populations. The overall age- and gender-adjusted incidence rate was calculated by the sum total of each of these age- and gender-specific weighted adjustments. Population group-specific crude incidences were calculated. All incidences were calculated as number of fractures per 100 000 people annually. Participants with missing data (n=12) were excluded from the study. Finally, data were expressed as frequencies and percentages for categorical variables, while central tendency and dispersion were reported for continuous variables.
Results
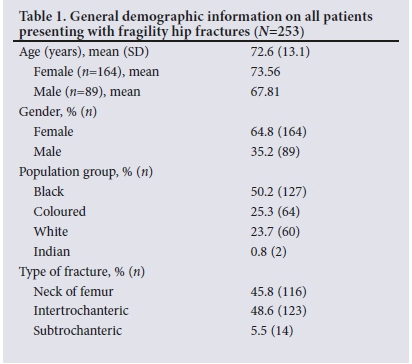
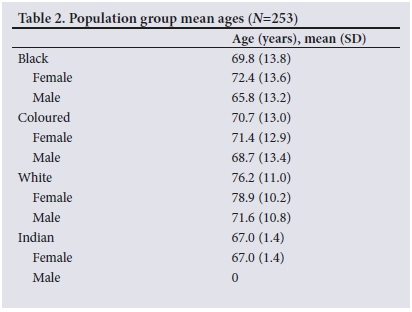
During the 1-year study period, a total of 305 patients with new hip fractures were admitted to Livingstone Hospital for further management. Information on mechanism of injury was not recorded in 12 cases (3.9%), and these cases were therefore excluded from analysis. Of the remaining 293 fractures, 253 (86.3%) were low-energy hip fractures and 40 (13.7%) were high-energy fractures. A total of 253 patients were therefore included in the study. The mean (standard deviation) age of patients with an FHF was 72.6 (13.1) years (95% confidence interval 69.9 - 73.2). The majority of participants were female (64.8%; n=164) (Table 1), with most participants having suffered intertrochanteric fracture (48.6%; n=123). The mean ages for the different population groups are presented in Table 2.
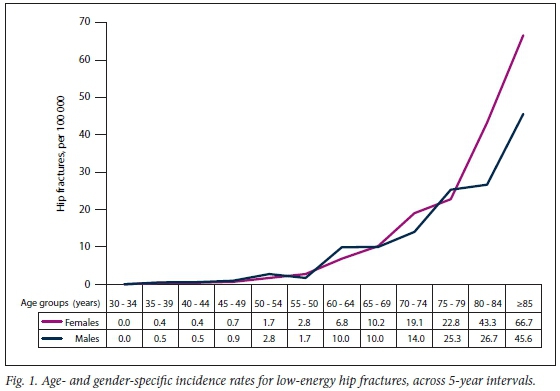
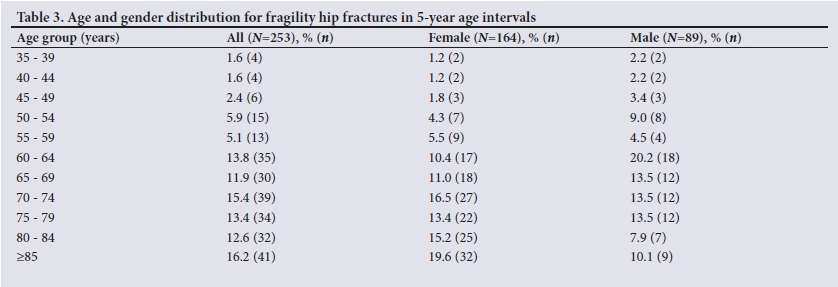
The highest number of low-energy hip fractures in females occurred in the >85- (19.6%) and 70 - 74-year (16.5%) age groups, while the highest number of male cases was observed in the 60 - 64-year group (20.2%) (Table 3).
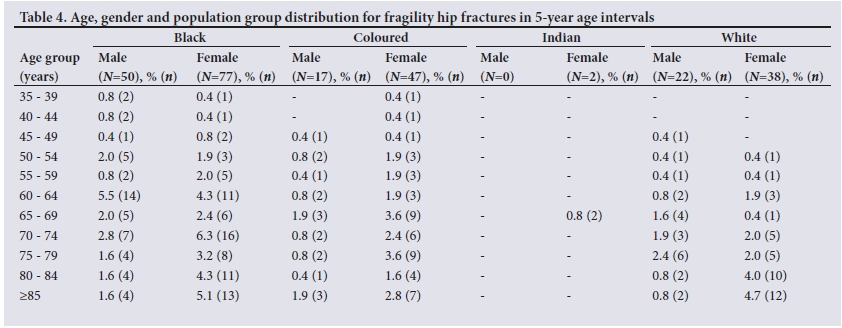
The highest frequency distribution of FHFs was observed in black males aged 60 - 64 years (5.5%; n=14) and black females aged 70 - 74 years (6.3%; n=16) (Table 4).
Incidence rates
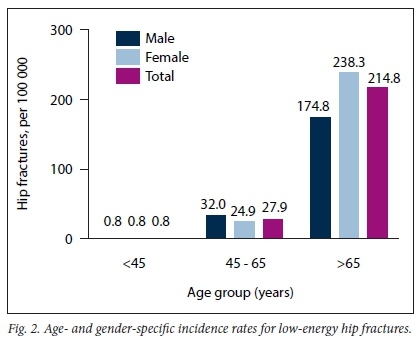
The crude incidence rate of low-energy hip fractures in the WREC was 19.3 per 100 000. The crude incidence of hip fractures in males and females was 14.6 and 23.4 per 100 000, respectively. Age-, gender-and population group-specific incidence rates for low-energy hip fractures are depicted in Figs 1 - 3.
Discussion
The objective of this study was to determine age-, gender- and population group-specific incidence rates of FHFs in a subpopulation of the Eastern Cape, South Africa, a population that has not been investigated previously. The main finding was that the crude incidence rate of FHFs in our population was 19.3 per 100 000, while males and females had incidence rates of 14.6 and 23.4 per 100 000, respectively.
FHF incidence in SA has traditionally been reported as being low compared with other countries, owing to the initial crude incidence rates as reported by Solomon.[9] The incidence rates for males and females, as reported in 1968 for a subpopulation in Johannesburg, were 6.9 and 4.3 per
100 000, respectively, with an overall crude incidence of 5.6.[9] Although the 1968 study had several limitations, including lack of distinction between high- and low-energy fractures, male-biased representation of the study population and a lack of specific age group assessments, it is still interesting to note the large difference between the reported incidence rates and those in the current study. Although the studies report on different geographical areas, this alone is unlikely to account for the large differences observed between them.
The second finding of this study illustrated a similar trend of increased incidence rates compared with recent studies in other regions of SA. Data from work done by Paruk et al.[12] and Dela et al.[13] indicate much higher incidence rates than previously reported by Solomon.[9] Paruk et al.[12] reported an incidence rate of 68.5 and 133.0 per 100 000 for males and females, respectively, with an overall crude incidence of 97.4 per 100 000, in black patients from the eThekwini region aged >60 years. In a comparison between the Paruk study population and the present study population from the WREC, adjusted for age groups >60 years, it is interesting to note that even higher crude incidences are reported in the present study (Fig. 4A). The marked difference can be attributed to the multiple population groups included in the Eastern Cape study, while the eThekweni study only included the black population group. Higher incidence rates in the white population therefore influence the overall incidence rates in the WREC.
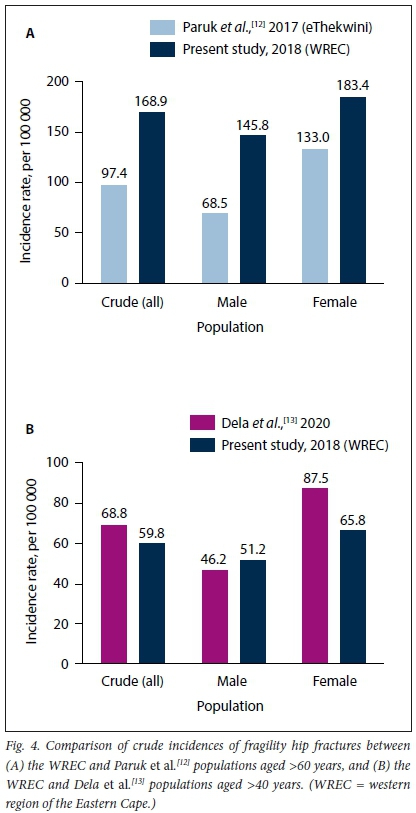
Interestingly, the investigation by Dela et al.,[13]which reported on the rate of hip fractures in males and females aged >40 years and included all population groups, showed similar numbers to those reported in the present study (Fig. 4B). The incidence rate of hip fractures reported by Dela et al.[13]for males and females aged >40 years (including all population groups) was 46.2 and 87.5, respectively (overall crude incidence 68.6 per 100 000). It is, however, important to note that this study investigated both state and private health institutions. It is therefore inappropriate to directly compare this study's data with studies representing state-only institutions, considering the broad differences in populations attending state and private healthcare facilities that might potentially influence the findings.!141 Despite this, it is interesting to note that there are similarities in crude incidence between the WREC and data produced by Dela et al.Mas shown in Fig. 4B.
Comparing South African populations with other countries and/ or subpopulations highlights that the incidence rate of FHFs in SA is at the lower end of the spectrum (Figs 5 and 6).[18, 23] Of interest was how SA populations would compare with other developing countries.
Heterogeneity of incidence rates between different populations can be attributed to environmental, population group, life expectancy and healthcare differences.[4] Comparing the results of the present study with others should be done with caution, however, as all published studies do not necessarily distinguish between high- and low-energy hip fractures, or include all age groups, which could influence the results substantially. It is, however, worthwhile noting that our population appears to be following a similar trend to other developing countries, such as the Rohtak district of India.[19] Another noteworthy finding of our study is that in the young male group (45 64 " years), our population showed a surprisingly high age-specific incidence rate. The increased incidence of FHFs in males aged 60 64 " years was specifically evident in the black group, which showed the highest age-specific incidence of any of the populations compared (Fig. 6).
The few studies investigating young patients with hip fractures have contrasting findings. Traditionally it was believed that hip fractures in young patients occur almost exclusively as a result of high-energy trauma.[24] However, more recent work indicates that there are two distinct patient groups, namely young, healthy males aged 20 - 40 years who sustain high-energy trauma, and a larger group of patients between the ages of 40 and 50 years who sustain low-energy-related fractures. The majority of patients in the latter group are reported to have associated medical conditions, and there is a high prevalence of alcohol use.[25] Lifestyle factors (smoking, alcohol and drug consumption) as well as other medical conditions further appear to be contributing to an increased incidence of low-energy hip fractures in young patients.[26]
Compared with women, men are thought to sustain fragility fractures at a later stage in life, possibly owing to higher bone mineral density and a lower propensity to falls[27,28] However, the opposite appears to be the case in the present study. The exact reasons for this finding are not clear, but it can potentially be attributed to various factors, including higher incidences of comorbidities and substance abuse, life expectancy differences, and possibly lower preventive measures in males.[29-31]
Owing to the significant prevalence of HIV in South Africa (13.1%),[32] the influence of HIV on FHFs also needs to be considered. The effect of HIV on the musculoskeletal system is well documented and HIV infection has been associated with a three-fold increased risk for any fracture, with almost a nine-fold higher risk of sustaining a hip fracture.[33] Although the potential influence of HIV was not within the scope of this investigation, it is an important variable that should be considered in future studies, as it could shed more light on the high incidence rate of hip fractures observed in our younger male patient population.
Study limitations
Limitations of this study include that only state patients were investigated, and patients attending private hospital facilities are therefore not represented. As this was a record review of patients presenting for surgery after sustaining an FHF, it is possible that some patients may have died prior to admission or preoperatively and therefore been excluded from the study. However, it is reasonable to assume that these cases would represent a very small number and would be unlikely to affect the overall incidence significantly. Some information, such as the presence of comorbidities or lifestyle habits, that could have influenced the outcomes of interest, was not reported in this investigation owing to its retrospective nature. Future prospective studies should aim to include all known risk factors for FHF. Finally, a single investigator performed data capturing and confirmation cross-referencing, which may be susceptible to bias.
Conclusions
For SA healthcare workers to fully understand the growing impact of FHFs in our country, it is imperative that we investigate the country as whole. This study of a subpopulation in SA, along with other recent publications from different regions, serves to contribute to the growing body of national knowledge on hip fractures. This work highlights that we have a higher incidence of FHFs than would be expected on the basis of previous reports, which mirrors findings from other local studies. Approximately 30% of our patients were aged <65 years, with young black males showing a markedly high incidence rate compared with other populations. In general, and in contrast to most other regions, it appears that our male population is sustaining FHFs earlier than females. These findings warrant further investigation that may prompt the development of preventive strategies and optimal treatment programmes.
Declaration. The research for this study was done in fulfilment of the requirements for MLG's postgraduate MMed (Orthopaedics) degree at Walter Sisulu University.
Acknowledgements. None.
Author contributions. MLG was responsible for the conception and design of the work, literature review, analysis, drafting of the work, and final approval of the version to be published. MCB was responsible for the analysis, drafting and final approval of the version to be published.
Funding. None.
Conflicts of interest. None.
References
1. Neuburger J, Currie C, Wakeman R et al. The impact of a national clinician-led audit initiative on care and mortality after hip fracture in England. Med Care 2015;53(8):686-691. https://doi.org/10.1097/mlr.0000000000000383 [ Links ]
2. Williamson S, Landeiro F, McConnell T, et al. Costs of fragility hip fractures globally: A systematic review and meta-regression analysis. Osteoporos Int 2017;28(10):2791-2800. https://doi.org/10.1007/s00198-017-4153-6 [ Links ]
3. Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporos Int 1997;7(5):407-413. https://doi.org/10.1007/pl00004148 [ Links ]
4. Kanis JA, Odén A, McCloskey EV, Johansson H, Wahl DA, Cooper C. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 2012;23(9):2239-2256. https://doi.org/10.1007/s00198-012-1964-3 [ Links ]
5. Cummings SR, Melton LJ. Osteoporosis I: Epidemiology and outcomes of osteoporotic fractures. Lancet 2002;359(9319):1761-1767. https://doi.org/10.1016/s0140-6736(02)08657-9 [ Links ]
6. Cooper C, Campion G, Melton LJ. Hip fractures in the elderly: A world-wide projection. Osteoporos Int 1992;2(6):285-289. https://doi.org/10.1007/bf01623184 [ Links ]
7. Zebaze RMD, Seeman E. Epidemiology of hip and wrist fractures in Cameroon, Africa. Osteoporos Int 2003;14(4):301-305. https://doi.org/10.1007/s00198-002-1356-1 [ Links ]
8. El Maghraoui A, Koumba BA, Jroundi I, Achemlal L, Bezza A, Tazi MA. Epidemiology of hip fractures in 2002 in Rabat, Morocco. Osteoporos Int 2005;16(6):597-602. https://doi.org/10.1007/s00198-004-1729-8 [ Links ]
9. Solomon L. Osteoporosis and fracture of the femoral neck in the South African Bantu. J Bone Joint Surg 1968;50-B(1):2-13. https://doi.org/10.1302/0301-620x.50bL2 [ Links ]
10. Barrett-Connor E, Siris ES, Wehren LE, et al. Osteoporosis and fracture risk in women of different ethnic groups. J Bone Miner Res 2005;20(2):185-194. https://doi.org/10.1359/jbmr.041007 [ Links ]
11. Looker AC, Melton LJ, Harris TB, Borrud LG, Shepherd JA. Prevalence and trends in low femur bone density among older US adults: NHANES 2005 - 2006 compared with NHANES III. J Bone Miner Res 2010;25(1):64-71. https://doi.org/10.1359/jbmr.090706 [ Links ]
12. Paruk F, Matthews G, Cassim B. Osteoporotic hip fractures in black South Africans: A regional study. Arch Osteoporos 2017;12(1):5-10. https://doi.org/10.1007/s11657-017-0409-1 [ Links ]
13. Dela SS, Paruk F, Brown SL, et al. Ethnic and gender-specific incidence rates for hip fractures in South Africa: A multi-centre study. Bone 2020;133:115253. https://doi.org/10.1016/j.bone.2020.115253 [ Links ]
14. Statistics South Africa. Census 2011. Provincial profile: Eastern Cape. Report no. 03-01-71. Pretoria: Stats SA, 2014. http://www.statssa.gov.za/publications/Report-03-01-71/Report-03-01-712011.pdf (accessed 20 September 2016). [ Links ]
15.Eastern Cape Provincal AIDS Council. Annual Progress Report 2014/15. March 2016:37. https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwi u0NnNt_3vAhXIVsAKHdTqD-sQFjAOegQILBAD&url=http%3A%2F%2Fsanac.org.za%2Fdownload%2F563% 2Fresources%2F3390%2Feastern-cape-annual-progress-report_final.pdf&usg=AOvVaw25sp2g1f4Zq8nl5AG23cDF (accessed 18 June 2016). [ Links ]
16. Bouxsein ML, Kaufman J, Tosi L, Cummings S, Lane J, Johnell O. Recommendations for optimal care of the fragility fracture patient to reduce the risk of future fracture. J Am Acad Orthop Surg 2004;12(6):385-395. https://doi.org/10.5435/00124635-200411000-00003 [ Links ]
17. Parker MJ. Hip fractures in the elderly. Surgery 2010;28(10):483-488. https://doi.org/10.1016/j.mpsur.2010.07.009 [ Links ]
18. Dixon T, Crisp A. The problem of osteoporotic hip fracture in Australia. Bulletin no. 76. Canberra: Australian Institute of Health and Welfare, 2010. https://www.aihw.gov.au/getmedia/ea96bc4d-0b97-4c5a-b792-08b343752adc/10695.pdf.aspx?inline=true (accessed 2 May 2016). [ Links ]
19. Dhanwal DK, Siwach R, Dixit V, Mithal A, Jameson K, Cooper C. Incidence of hip fracture in Rohtak district, North India. Arch Osteoporos 2013;8(1-2):1-9. https://doi.org/10.1007/s11657-013-0135-2 [ Links ]
20. Kanis JA, Johnell O, Oden A, et al. Long-term risk of osteoporotic fracture in Malriio. Osteoporos Int 2000;11:669-674. https://doi.org/10.1007/s001980070064 [ Links ]
21. Ettinger B, Black DM, Dawson-Hughes B, Pressman AR Melton LJ III. Updated fracture incidence rates for the US version of FRAX®. Osteoporos Int 2010;21:25-33. https://doi.org/10.1007/s00198-009-1032-9 [ Links ]
22. Singer BR, McLauchlan GJ, Robinson CM, Christie J. Epidemiology of fractures in 15,000 adults: The influence of age and gender. J Bone Joint Surg 1998;80B(2):243-248. https://doi.org/10.1302/0301-620x80b2.7762 [ Links ]
23. Tsang SWY, Kung AWC, Kanis JA, Johansson H, Odenle A. Ten-year fracture probability in Hong Kong Southern Chinese according to age and BMD femoral neck T-scores. Osteoporos Int 2009;20:1939-1945. https://doi.org/10.1007/s00198-009-0906-1 [ Links ]
24. Cheng K, Montgomery S, Housley S, Wheelwright E. Clinical risk factors for hip fracture in young adults under 50 years old. Eur J "Trauma Emerg Surg 2009;35(1):40-42. https://doi.org/10.1007/s00068-008-7177-y [ Links ]
25. Pauyo T, Drager J, Albers A, Harvey EJ. Management of femoral neck fractures in the young patient: A critical analysis review. World J Orthop 2014;5(3):204-217. https://doi.org/10.5312/wjo.v5.i3.204 [ Links ]
26. Al-Ani AN, Neander G, Samuelsson B, Blomfeldt R, Ekstrom W, Hedstróhi M. Risk factors for osteoporosis are common in young and middle-aged patients with femoral neck fractures regardless of trauma mechanism. Acta Orthop 2013;84(1):54-59. https://doi.org/10.3109/17453674.2013.765639 [ Links ]
27. Hannan MT, Felson DT, Dawson-Hughes B, et al. Risk factors for longitudinal bone loss in elderly men and women: The Framingham Osteoporosis Study. J Bone Miner Res 2000;15(4):710-720. https://doi.org/10.1359/jbmr.2000.15.4.710 [ Links ]
28. Cooper C, Melton LJ. Epidemiology of osteoporosis. Trends Endocrinol Metab 1992;3(6):224-229. https://doi.org/10.1016/1043-2760(92)90032-V [ Links ]
29. Hawkes WG, Wehren L, Orwig D, Hebel JR, Magaziner J. Gender differences in functioning after hip fracture. J Gerontol A Biol Sci Med Sci 2006;61(5):495-499. https://doi.org/10.1093/gerona/6L5.495 [ Links ]
30. Becker C, Crow S, Toman J, et al. Characteristics of elderly patients admitted to an urban tertiary care hospital with osteoporotic fractures: Correlations with risk factors, fracture type, gender and ethnicity. Osteoporos Int 2006;17(3):410-416. https://doi.org/10.1007/s00198-005-0001-1 [ Links ]
31. Lofman O, Berglund K, Larsson L, Toss G. Changes in hip fracture epidemiology: Redistribution between ages, genders and fracture types. Osteoporos Int 2002;13(1):18-25. https://doi.org/10.1007/s198-002-8333-x [ Links ]
32. Statistics South Africa. Mid-year population estimates 2018. Statistical release P0302. Pretoria: Stats SA, 2018. https://www.statssa.gov.za/publications/P0302/P03022018.pdf (accessed 30 March 2021). [ Links ]
33. Prieto-Alhambra D, Guerri-Fernandez R, de Vries F, et al. HIV infection and its association with an excess risk of clinical fractures: A nationwide case-control study. J Acquir Immune Defic Syndr 2014;66(1):90-95. https://doi.org/10.1097/qai.0000000000000112 [ Links ]
 Correspondence:
Correspondence:
ML Grundill
mlgrundill@gmail.com
Accepted 13 May 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}