










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.111 n.9 Pretoria Sep. 2021
http://dx.doi.org/10.7196/SAMJ.2021.v111i9.15813
IN PRACTICE
ISSUES IN PUBLIC HEALTH
Unnatural deaths, alcohol bans and curfews: Evidence from a quasi-natural experiment during COVID-19
T A MoultrieI; R E DorringtonII; R LaubscherIII; P GroenewaldIV; C D H ParryV, VI; R MatzopoulosVII, VIII; D BradshawIX, X
IBBusSc, MSc, PhD; Centre for Actuarial Research, Faculty of Commerce, University of Cape Town, South Africa
IIBCom, BSc Hons, BA, MPhil, FASSA; Centre for Actuarial Research, Faculty of Commerce, University of Cape Town, South Africa
IIIBCom; Biostatistics Research Unit, South African Medical Research Council, Cape Town, South Africa
IVMB ChB, MPH; Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa
VMSc, MA, PhD; Alcohol, Tobacco and Other Drug Research Unit, South African Medical Research Council, Cape Town, South Africa
VIMSc, MA, PhD; Department of Psychiatry, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
VIIBBusSc, MPhil, PhD; Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa
VIIIBBusSc, MPhil, PhD;School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
IXMSc, DPhil; Burden of Disease Research Unit, South African Medical Research Council, Cape Town, South Africa
XMSc, DPhil; School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND. Coronavirus disease-19 (COVID-19) restrictions, particularly relating to the sale of alcohol and hours of curfew, have had a marked effect on the temporal pattern of unnatural deaths in South Africa.
METHODS. Death data were collected over 68 weeks from January 2020 to April 2021, together with information on the nature of restrictions (if any) on the sale of alcohol, and hours of curfew. Data were analysed using a simple ordinary least square (OLS) regression model to estimate the relative contribution of restrictions on the sale of alcohol and hours of curfew to the pattern of excess unnatural deaths.
RESULTS. The complete restriction on the sale of alcohol resulted in a statistically significant reduction in unnatural deaths regardless of the length of curfew. To the contrary, periods where no or limited restrictions on alcohol were in force had no significant effect, or resulted in significantly increased unnatural deaths.
CONCLUSION. The present study highlights an association between alcohol availability and the number of unnatural deaths and demonstrates the extent to which those deaths might be averted by disrupting the alcohol supply. While this is not a long-term solution to addressing alcohol-related harm, it further raises the importance of implementing evidence-based alcohol control measures.
The South African (SA) government has invoked a suite of policy responses to curb the coronavirus disease-19 (COVID-19) pandemic. These have included a mix of interventions aiming to attenuate the spread of the severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2), including restricting mobility through curfews and measures aimed at reducing the burden on the healthcare system through restrictions on the sale or consumption of alcohol. The question as to whether these two particular responses (curfews and restrictions on sale of alcohol) had an effect on reducing unnatural deaths and trauma unit admissions in SA is important in its own right, and has generated substantial debate and commentary due to its economic impacts.[1-8]
Recently, media attention[9, 10] has been given to a study funded by an alcohol-industry group that asserts that the ban on alcohol sales and consumption had no effect in reducing trauma unit admissions, of which unnatural deaths are the extreme end of the continuum of trauma injuries. This contradicts another analysis that ascribes a significant decrease in unnatural deaths to the implementation of a sudden unexpected prohibition on alcohol sales in mid-July 2020 and a negligible impact of curfew duration.
In this present study, we performed statistical analysis on the effects of the policy implementation on the number of excess unnatural deaths in SA, making use of the extensive time-series of data on unnatural deaths compiled by a team of researchers at the South African Medical Research Council and the University of Cape Town (the 'SAMRC-UCT Collaboration').
Methods
The SAMRC-UCT Collaboration has published a weekly report of deaths in SA since March 2020[12] using information on deaths reported to the National Department of Home Affairs (DHA) and recorded on the National Population Register. The data are collected and collated in near-real-time, do not contain detailed information on the cause of death, simply whether the death was due to natural or unnatural causes. The data are provided weekly, and deaths are classified according to date of death (as opposed to date of reporting). The DHA data are adjusted for the small proportion of deaths that have been notified but not included on the National Population Register either because the deceased did not have a SA ID or died before the birth could be registered, and for deaths that were not registered at all.
Since there are strong temporal patterns in mortality from road traffic injuries, homicides, and some other unnatural causes of death (particularly on weekends and at month-end),[1314] a weekly time-series with weeks following the US Centers for Disease Control and Prevention (CDC) definition of an epi-week, running from a Sunday to a Saturday of the expected numbers of unnatural deaths is derived using a regression model based on the DHA data from 2014 - 2019. The methodology applied to derive this time-series is described in a report prepared by the SAMRC-UCT Collaboration[15]
In each weekly report, a figure is presented showing the reported number of unnatural deaths by week since week 1 of 2020 (beginning 29 December 2019), the expected number of unnatural deaths, and the prediction interval surrounding that expected number. Data from a recent report covering the week through 17 April 2021[16] are reproduced as Fig. 1. The data underpinning the figure are also published weekly on the SAMRC website as a supplement to the report.[12]
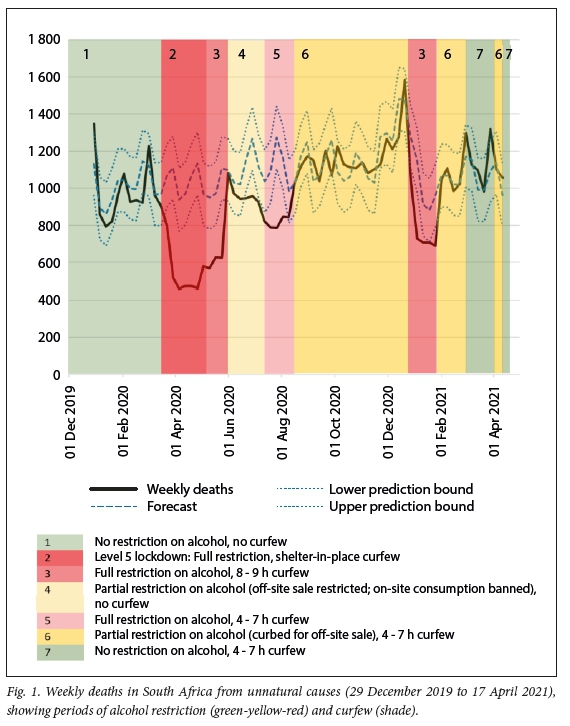
Fig. 1 also records the weeks in which significant changes were made to national regulations relating to curfew and the sale or consumption of alcohol. The online record of regulations imposed in terms of the Disaster Management Act[17] was consulted to establish for each week whether there was a ban on the sale or consumption of alcohol, and the number of nightly hours of curfew then in force. Where the regulations were changed during an epi-week, those regulations were for simplicity assumed to apply for that whole week. Alcohol restrictions were classified according to a three-way classification: no restriction on the sale and consumption of alcohol; partial restriction on sale of alcohol - this reflects periods when restrictions were imposed on sale for off-site consumption (usually from Mondays to Thursdays) and/or sale for on-site consumption (e.g. in restaurants or taverns); and a complete restriction on sale for off-site or on-site consumption.
Analysis
A simple ordinary least square (OLS) regression model was fitted to the excess of weekly deaths (that is the difference between observed and predicted unnatural deaths) covering 68 weeks from week 1 of 2020 (starting on 29 December 2019)
to week 15 of 2021 (starting on 11 April 2021), together with the weekly flags for the alcohol restrictions and hours of curfew with independent variables for alcohol restrictions and the curfew. Because regulations affecting the independent variables tended often to be adjusted simultaneously (and to preclude fitting the model to combinations of the two independent variables that do not exist in the data), we allowed for an interaction effect between the two independent variables. The model specification is thus:

where the y. are the numbers of observed weekly deaths from unnatural deaths in week i (i = 1, 2...68). The alphas represent the effect in week . of the level of alcohol restriction, j (0 = no restriction; 1 = partial restriction; 2 = full restriction), and the daily curfew duration in that week, k (k = 0 hours, 4 - 7 hours, 8 - 9 hours, and the level 5 lockdown restrictions). The constant (c) represents the weekly excess deaths in the absence of either alcohol restriction or curfew; the error term (e) represents the effect of omitted variables.
Sensitivity analysis was used to explore whether alternative formulations of the model might lead to either a better fit and/or materially different results. This assessed the effect of implementing curfews of different duration and the incorporation (and substitution) of data on mobility using data curated by Google.[18] The appendix (https://www.samrc.ac.za/bod/UnnaturalDeathsSupplementaryMaterial.pdf) contains details of a number of alternative models investigated to assess the sensitivity of the results to different model formulations. The conclusion drawn is that alternative measures of mobility or curfew do not produce materially different results.
Data were prepared in Excel and modelled using Stata software, version15 (StataCorp., US), treating the independent variables as categorical.
Results
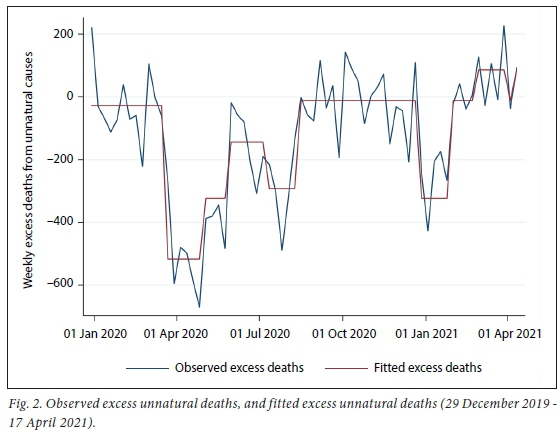
The model provides a good fit to the observed excess unnatural deaths (Fig. 2), explaining almost three-quarters of the variation in the dependent variable (adjusted R2 = 0.7308). The remaining sources of variation emanate from random fluctuations in both observed and expected numbers of deaths, as well as a slew of other factors (e.g. restrictions on interprovincial movements and prohibitions on being on beaches) that as a consequence of the regulations might have affected unnatural deaths.
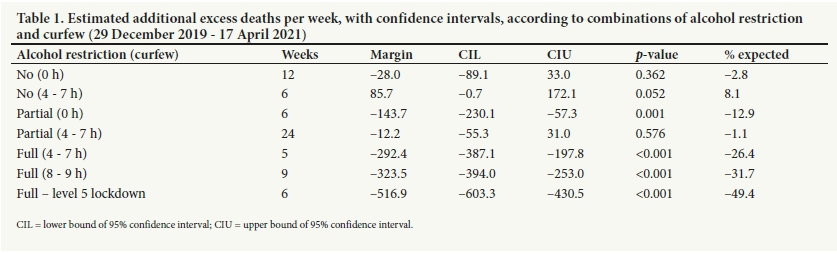
The marginal effect of each combination of the independent variables was then extracted, together with their 95% confidence intervals (Table 1 and Fig. 3). The final column of Table 1 shows the average weekly effect on excess deaths expressed as a percentage of the average weekly expected unnatural deaths in that combination of alcohol restrictions and curfew.
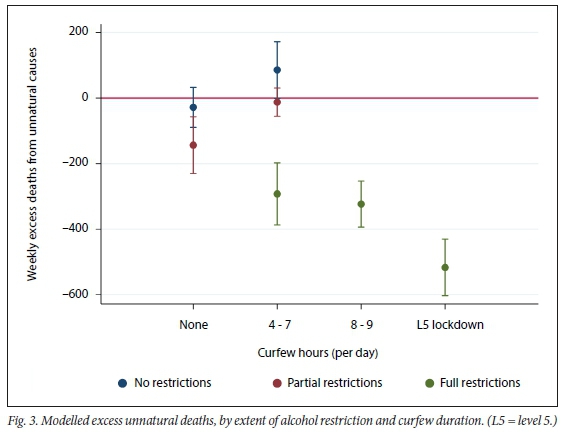
There is a significant association between the weekly unnatural deaths and full restriction on the sale of alcohol (Table 1). This effect increases with increasing duration of curfew, but even with fairly modest curfew hours (4-7 hours), full restriction on alcohol had the effect of reducing unnatural deaths by around 42 deaths per day, or 26%.
In all periods where there were full restrictions on the sale of alcohol for off-site consumption, the excess number of unnatural deaths was significantly lower than zero, indicating a protective effect of the restrictions. Barring one situation (partial restrictions under no curfew), periods where there was no full restriction on the sale of alcohol (regardless of the duration of curfew) did not significantly impact excess deaths (the confidence interval containing zero).
Discussion
Our results provide compelling evidence that the restriction on the sale of alcohol rather than curfew is associated with the reduction in unnatural deaths observed during the COVID-19 outbreak in SA. These results are further corroborated by data from a Worcester hospital (SA) study[19] showing that full restrictions on the sale of alcohol were substantially more effective than partial restrictions in reducing trauma admissions.
Although the changing policy interventions have created a quasi-natural experiment, this remains an ecological study assessing correlations over time. The common fallacy of incorrectly attempting to interpret findings from an ecological study at the level of individuals does not apply, as we are seeking to evaluate the impact of policy interventions at a population level.
The anomalous result for the period of partial restriction and no curfew is probably explained by the fact that the data underpinning that estimate comprise a contiguous period of 6 weeks running from the week beginning 31 May 2020 to the week ending 11 July 2020. This was the period in which SA exited a hard lockdown. Economic activity was still heavily restricted, and while there were restrictions on the sale of alcohol for off-site consumption, there was a complete prohibition on the sale of alcohol for on-site consumption.
While bans on alcohol are particularly blunt instruments, the argument that it is curfews rather than bans on the sale of alcohol that avert unnatural deaths is refuted by this analysis. All instances of full restriction on the sale of alcohol are associated with a significant decrease in unnatural deaths (ranging from 42 deaths per day with a curfew of 4 - 7 hours' duration to 74 deaths per day under full lockdown). However, this latter estimate is most certainly at the extreme of the likely impact of a ban on the sale of alcohol: that reduction arose from a very sudden imposition of the ban, and in the context of particularly severe restrictions on mobility and economic activity. Nevertheless, these results are consistent with work that estimated a minimum of 21 unnatural deaths averted per day in SA coincided with the implementation of the mid-July 2020 ban on alcohol sales.[11]
Study limitations
The lack of data on potential confounding factors such as restrictions on inter-provincial travel, beach attendance, or data on liquor trading hours is a study limitation, as is the absence of detailed information on the underlying causes of these unnatural deaths. Given the proportion of variance explained in the model presented, we are less concerned about the possibility that other variables on the causal pathway to unnatural death have substantial explanatory power. However, the inability to secure near-real-time information on cause of death represents a significant impediment to more careful analysis of the question.
Conclusion
The present study highlights an association between alcohol availability and unnatural deaths and quantifies how many of those deaths might have been averted by disrupting the alcohol supply. In the short term, this present study will help policymakers in SA assess the impact of implementing these bans as an emergency public healthcare response. It also strengthens the case for the implementation of bans on the sale of alcohol as part of the emergency response to ease the demand for emergency healthcare services during COVID-19 or future infectious disease outbreaks in SA and other countries with high alcohol-related injury burdens. Yet such a strategy also raises complex policy-related issues. While complete restrictions on sale of alcohol might avert unnatural deaths and contribute to preventing overload of the healthcare system during surges of COVID-19, long-term implementation of this policy would require significant trade-offs in terms of economic activity, as well as lives and livelihoods. Further research into this aspect is urgently required.
By demonstrating an association between alcohol and unnatural deaths, the present study adds to the corpus of evidence that enables SA policymakers to adopt evidence-based strategies known to reduce alcohol harm through actions such as stricter advertising and promotions restrictions, minimum unit pricing, increased excise taxes, raising the minimum drinking age, restrictions on container sizes, etc.
Furthermore, the possibility of capturing and making available near-real-time cause-of-death data would represent a significant step forward in monitoring and responding to future outbreaks of communicable diseases.
Declarations. None.
Acknowledgements. None.
Author contributions. TM conceptualised the study, wrote the draft manuscript and performed the statistical analysis. TM, RD, RL, PG, and DB contributed to the preparation and analysis of the underlying data. All authors approved the final manuscript for publication.
Funding. None.
Conflicts of interest. None.
References
1. Greyling T, Rossouw S, Adhikari T. The good, the bad and the ugly of lockdowns during Covid-19. PLoS ONE 2021;16(1):e0245546. https://doi.org/10.1371/journal.pone.0245546 [ Links ]
2. Matzopoulos R Walls H, Cook S, London L. South Africa's COVID-19 alcohol sales ban: The potential for better policy-making. Int J Health Policy Manag 2020;9( 11):486-487. https://doi.org/10.34172/ijhpm.2020.93 [ Links ]
3. Morris D, Rogers M, Kissmer N, Du Preez A, Dufourq N. Impact of lockdown measures implemented during the Covid-19 pandemic on the burden of trauma presentations to a regional emergency department in Kwa-Zulu Natal, South Africa. Afr J Emerg Med 2020; 10(4): 193-196. https://doi.org/10.1016/j.afjem.2020.06.005 [ Links ]
4. Moustakis J, Piperidis AA, Ogunrombi AB. The effect of COVID-19 on essential surgical admissions in South Africa: A retrospective observational analysis of admissions before and during lockdown at a tertiary healthcare complex. S Afr Med J 2020;110(9):910-915. https://doi.org/10.7196/SAMJ.2020.v110i9.15025 [ Links ]
5. Navsaria PH, Nicol AJ, Parry CDH, Matzopoulos R, Maqungo S, Gaudin R. The effect of lockdown on intentional and nonintentional injury during the COVID-19 pandemic in Cape Town, South Africa: A preliminary report. S Afr Med J 2020;111(2):110-113. https://doi.org/10.7196/SAMJ.2021v111i2.15318 [ Links ]
6. Reuter H, Jenkins LS, De Jong M, Reid S, Vonk M. Prohibiting alcohol sales during the coronavirus disease 2019 pandemic has positive effects on health services in South Africa. Afr J Prim Health Care Fam Med 2020;12(1):e1-e4. https://doi.org/10.4102/phcfm.v12i1.2528 [ Links ]
7. Venter A, Lewis CM, Saffy P, Chadinha LP. Locked down: Impact of COVID-19 restrictions on trauma presentations to the emergency department. S Afr Med J 2020;111(1):52-56. https://doi.org/10.7196/SAMJ.2021.v111i1.15289 [ Links ]
8. Zsilavecz A, Wain H, Bruce JL, et al. Trauma patterns during the COVID-19 lockdown in South Africa expose vulnerability of women. S Afr Med J 2020;110(11):1110-1112. https://doi.org/10.7196/SAMJ.2020.v110i11.15124 [ Links ]
9. Jobson J, Mtwa O. Alcohol lobby's data is wobbly. Mail & Guardian, 16 April 2021. https://mg.co.za/opinion/2021-04-16-alcohol-lobbys-data-is-wobbly/ (accessed 24 April 2021). [ Links ]
10. Mashego P. Ahead of possible third COVID-19 wave, industry says alcohol ban doesn't work. Fin24, 8 April 2021. https://www.news24.com/fin24/companies/travelandleisure/ahead-of-possible-third-covid-wave-industry-says-alcohol-ban-doesnt-work-20210408 (accessed 24 April 2021). [ Links ]
11. Barron K, Bradshaw D, Parry C, et al. Alcohol and short-run mortality: Evidence from a modern-day prohibition. SSRN 2020 (posted 8 Dec 2020). https://doi.org/10.2139/ssrn.3744031 (accessed 3 May 2021). [ Links ]
12. Bradshaw D, Laubscher R, Dorrington RE, Groenewald P, Moultrie TA. Report on weekly deaths in South Africa. Cape Town: South African Medical Research Council, 2021. https://www.samrc.ac.za/reports/report-weekly-deaths-south-africa?bc=254 (accessed 6 May 2021). [ Links ]
13. Rogot E, Fabsitz R Feinleib M. Daily variation in USA morality. Am J Epid 1976;103(2):198-211. https://doi.org/10.1093/oxfordjournals.aje.a112218 [ Links ]
14. Trudeau R. Monthly and daily patterns of death. Health Reports. 1997;9:43-50. [ Links ]
15. Dorrington RE, Bradshaw D, Laubscher R, Groenewald P, Moultrie TA. Methodological note: Predicted numbers of deaths by epi-week for South Africa in 2020 and 2021. Cape Town: South African Medical Research Council, 2021. https://www.samrc.ac.za/sites/default/files/files/2021-01-24/Methodological%20Note%20on%20Predicted%20Weekly%20Deaths%2020_ Jan_2021.pdf. (accessed 29 April 2021). [ Links ]
16. Bradshaw D, Laubscher R, Dorrington RE, Groenewald P, Moultrie TA. Report on weekly deaths in South Africa: 25 April - 1 May 2021 (Week 17). Cape Town: South African Medical Research Council, 2021. https://www.samrc.ac.za/sites/default/files/files/2021-05-05/weekly1May2021.pdf (accessed 6 May 2021). [ Links ]
17. South Africa. Disaster Management Act of 2002. Regulations to address, prevent and combat the spread of coronavirus COVID-19: Adjusted alert level 1. Government Gazette No. 44201, 2021. (Published under Government Notice R152). https://www.gov.za/covid-19/resources/regulations-and-guidelines-coronavirus-covid-19 (accessed 30 April 2021). [ Links ]
18. Google LLC. COVID-19 Community Mobility Reports 2021. https://www.google.com/covid19/mobility/ (accessed 30 April 2021). [ Links ]
19. Chu KM, Marco J-L, Owolabi EO, et al. Trauma trends during COVID-19 alcohol prohibition at a South African regional hospital. Drug and Alcohol Review 2021 (epub 17 May 2021). https://doi.org/10.1111/dar.13310 [ Links ]
 Correspondence:
Correspondence:
TA Moultrie
tom.moultrie@uct.ac.za
Accepted 14 June 2021


{kind=link}