










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.111 n.8 Pretoria Aug. 2021
http://dx.doi.org/10.7196/samj.2021.v111i8.15477
RESEARCH
Expanding the epidemiological understanding of hepatitis C in South Africa: Perspectives from a patient cohort in a rural town
M W SonderupI; J HorakII; H SmutsIII, IV; J SaaymanV; L BorettiVI; J BlackVII, VIII
IBPharm, MB ChB, FCP (SA), MMed (Med), FRCP (Lond); Division of Hepatology, Department of Medicine, Faculty of Health Sciences, University of Cape Town and Groote Schuur Hospital, Cape Town, South Africa
IIMB ChB, Dip HIV Man (SA); Department of Medicine, Livingstone Hospital, Port Elizabeth, South Africa
IIIPhD; Medical Virology, National Health Laboratory Service, Groote Schuur Hospital, Cape Town, South Africa
IVPhD; Division of Medical Virology, Department of Pathology, Faculty of Health Sciences, University of Cape Town, South Africa
VMB ChB; Department of Medicine, Livingstone Hospital, Port Elizabeth, South Africa
VIBHSc, MB BCh, Dip HIV Man (SA); Department of Medicine, Livingstone Hospital, Port Elizabeth, South Africa
VIIMB ChB, FCP (SA), Cert ID (SA)Department of Medicine, Livingstone Hospital, Port Elizabeth, South Africa
VIIIMB ChB, FCP (SA), Cert ID (SA); Department of Medicine, Faculty of Health Sciences, Walter Sisulu University, South Africa
ABSTRACT
BACKGROUND: The epidemiology of hepatitis C virus (HCV) in the general population of South Africa (SA) is incompletely understood. A high HCV prevalence in key populations is known, but data are limited in terms of a broader understanding of transmission risks in our general population
OBJECTIVES: To investigate a patient cohort with HCV infection clustering in a rural SA town, in order to identify possible HCV transmission risks, virological characteristics, phylogenetic data and treatment outcomes
METHODS: A cluster of patients with positive HCV serology, previously identified from laboratory records, were contacted by a local district hospital and offered confirmatory testing for HCV viraemia where needed. Those with confirmed HCV RNA were invited to a local hospital visit, where relevant demographic information was recorded, clinical assessment performed and a confidential questionnaire administered. HCV population-based sequencing was performed on HCV NS3/4A, NS5A and NS5B using polymerase chain reaction-specific or M13 universal primers, and sequences were aligned using BioEdit 7.2.5. Phylogenetic trees were constructed. Clinical assessments included liver fibrosis determination with FibroScan (cut-off >12.5 kPa = F4). Patients were offered treatment, and sustained virological response (SVR) was confirmed by undetectable HCV RNA at least 12 weeks after the end of treatment
RESULTS: Twenty-one patients, all from the same town, median (interquartile range (IQR)) age 64 (59 - 70) years, 57% female, were evaluated. Of these, 24% (n=5) were HIV co-infected, stable on antiretrovirals. The median (IQR) alanine aminotransferase level was 51 (31 - 89) U/L, with fibrosis distribution including 29% F1, 29% F2, 9% F3 and 33% F4 METAVIR fibrosis. Virologically, two genotypes were observed: 62% (n=13) genotype (GT) 1b and 38% (n=8) GT5a. No patient had ever used injecting drugs, 14% (n=3) had received blood products before 1992, and 9.5% (n=2) had undergone traditional healer-administered scarification. All (n=21) reported attendance at a single primary care clinic in the past, with most (n=20) recalling having received parenteral therapies at the clinic. Phylogenetic analysis of the HCV NS5A and NS5B regions confirmed GT1b and GT5a genotypes and formed two separate clusters within their respective genotypes, suggesting a common source for each genotype infection. Most patients received treatment with sofosbuvir/daclatasvir, 1 was treated with sofosbuvir/velpatasvir, and 1 was re-treated with sofosbuvir/velpatasvir/voxilaprevir. Per protocol SVR was 95%, with the non-SVR patient successfully re-treated
CONCLUSIONS: Data from a rural town cluster of patients suggest parenteral medical exposure as the probable common source of hepatitis C transmission risk. The cohort was of older age with a significant number having advanced fibrosis or cirrhosis, suggesting HCV acquisition in the distant past. Using a simplified care approach, treatment outcomes were very good
Globally, ~71 million people are viraemic for hepatitis C virus (HCV) infection, with 10.2 million (14%) residing in sub-Saharan Africa.[1]The prevalence of HCV in South Africa (SA) is <1%, with modelled data suggesting ~600 000 infected.[2] Despite typical HCV transmission risks being present in SA, such as people who inject drugs (PWID), pre-1992 blood or blood products (before universal HCV screening was introduced into blood services), parenteral injuries in healthcare workers and traditional practices such as scarification, HCV epidemiology is incompletely characterised. Historically, blood transfusion service HCV incidence, as a marker of the general population in SA, is low at 0.03 - 0.1%.[3,4] Unsurprisingly, recent data from key populations in SA demonstrate a high prevalence of HCV and HIV-HCV co-infection.[5] HCV prevalence studies in men who have sex with men (MSM) have demonstrated rates of 6%, with genotype (GT) 1a and 3a the predominant genotypes identified.[6] Interestingly, to date no GT5a, an HCV genotype unique to SA, has been identified in any of the key population studies in SA. Local key population data align with global epidemiology as the current major drivers of ongoing HCV infection.[7] Key population patients tend to be younger, the median age being 29 years in SA, whereas the other HCV prevalence peak comprised people invariably >50 years of age.[5,6,8] In recent data from Cape Town looking at a general HCV patient cohort accessing treatment, 26% of patients had no identifiable risk factor, possibly pointing towards other parenteral exposure, e.g. through traditional or unsafe medical practices, as a likely means of transmission.'91 Rwandan data also identified that, in addition to scarification or traditional healer operations, healthcare interventions were associated with an increased likelihood of HIV or HCV infection.[10] Healthcare-acquired HCV infection accounts for a significant portion of the infections in highly HCV-prevalent countries such as Egypt and Pakistan.[11] However, data to suggest this as a mode of HCV transmission in SA are lacking.
Objectives
A clinical observation of an unusual number of patients, all emanating from a single SA rural town and testing positive for hepatitis C, warranted further investigation. Additionally, since 2015, given the evolution of hepatitis C therapy to the highly effective, well-tolerated and all-oral direct-acting antiviral (DAA) therapy, the prospect of managing these patients efficiently existed.[12] The patients also provided an opportunity for proper evaluation and treatment, to better understand their transmission risk and hence guide further intervention measures and policy development. For patients previously identified, previous pegylated interferon and ribavirin-based therapy was unavailable. The newer DAA therapy was not yet widely available and required South African Health Products Regulatory Authority (SAHPRA) named patient approval via a section 21 certificate.
Methods
A Port Elizabeth-based tertiary hospital specialist clinic observed a pattern of referral of patients with HCV infection. The patients clustered from a defined geographical area and town and were not characteristically from recognised key populations with a high HCV prevalence. To better understand this observation, apart from already known patients, National Health Laboratory Service records were accessed to identify patients who screened positive for HCV between January 2015 and January 2018 from the region in question. Contact tracing was undertaken to find those in whom hepatitis C viraemia had not been undertaken after screening HCV-seropositive. Hepatitis C screening had been performed with a laboratory-based anti-HCV antibody test (ARCHITECT I or II; Abbott Diagnostics, USA).
Confirmation of HCV viraemia was performed using either Cobas Amplicor (Roche, Switzerland) or HCV Xpert (Cepheid, USA), as per standard diagnostic protocol. Where HCV viraemia had not yet been performed, patient contact tracing was done via a local hospital and patients were invited back.
The specialist clinic looked for mechanisms to better understand the observed clustering of HCV patients and sought access to care. In collaboration, the pan-genotypic DAA therapy, sofosbuvir and daclatasvir, donated by Médecins Sans Frontières, South Africa, to the University of Cape Town and Groote Schuur Hospital (UCT/GSH) Liver Clinic, was provided to enhance access to care for the HCV-infected patients.
Clinicians from the specialist clinic in Port Elizabeth, in collaboration with a hepatologist from the UCT/GSH Liver Clinic in Cape Town, initiated a treatment intervention and patient evaluation. A total of 67 patients who screened HCV-positive were identified from searching laboratory records. Of these, 18 could be traced; 13 patients were alive, and 5 were confirmed deceased with cause of death unknown. Of the 13, most (12/13) were confirmed to be HCV viraemic. The remaining 49 patients were untraceable. During the process, an additional 9 patients, all from the same region (and not part of the initial 67), were identified. Patients were seen and evaluated either in their regional hospital (through two outreach visits) or in the specialist clinic.
Apart from the standard consent provided for a SAHPRA section 21 certificate, patients were also requested to give consent (in their language of choice) prior to clinical evaluation, as an extensive standardised history of possible hepatitis C transmission risks was taken and documented. All patients' relevant demographic, serological and virological data were captured. Patients were screened for HIV (if not known to be HIV-positive) and hepatitis B surface antigen (HBsAg; Roche Diagnostics, Switzerland). To be eligible for DAA therapy, HIV-infected patients were required to be stable on antiretroviral therapy with a suppressed HIV viral load. As a routine, all patients had baseline renal and liver function tests and hepatitis C viral sequencing performed using standard population-based Sanger sequencing to determine genotype and to construct phylogenetic trees. The NS3/4A, NS5A and NS5B polymerase chain reaction (PCR) products were directly sequenced using PCR-specific or M13 universal primers with the BigDye terminator cycle sequencing kit (Applied Biosystems, USA). Sequences were aligned using BioEdit 7.2.5[13] and phylogenetic trees were constructed in MEGA 6 (USA).[14]
Point-of-care liver fibrosis assessment was performed using vibration-controlled transient elastography (FibroScan; Echosens, France), and patients were classified as having F0, F1, F2, F3 or F4 fibrosis according to the METAVIR system.[15] A FibroScan liver stiffness measurement of >12.5 kPa was used to define F4 fibrosis. Cirrhosis was classified according to the Child-Turcotte-Pugh system.[16]
Patients were treated with a combination of sofosbuvir and daclatasvir for 12 weeks. In those with cirrhosis, ribavirin 400 mg twice daily was added, or for those likely to be intolerant of ribavirin, treatment was extended to 24 weeks. In patients with predicted drug-drug interactions with daclatasvir, dose adjustment was made for the duration of therapy.
A sustained virological response (SVR) was defined as a patient being PCR-negative for hepatitis C RNA using a sensitive HCV viral load analysis at least 12 weeks after the end of treatment. As per standard of care, patients failing to achieve SVR would be evaluated for re-treatment based on hepatitis C sequencing and determination of their HCV resistance-associated substitution analysis.
Ethics approval
The study was approved by the University of Cape Town Human Research Ethics Committee (ref. no. 624/2020).
Statistical analysis
All values are expressed as medians and interquartile ranges (IQRs) for continuous variables. Baseline and on-treatment data are summarised using standard descriptive characteristics. Where appropriate, differences between qualitative parameters were explored using the Wilcoxon rank-sum test. Statistical analysis was performed using MedCalc v19.5.3 (MedCalc Software, Belgium).
Results
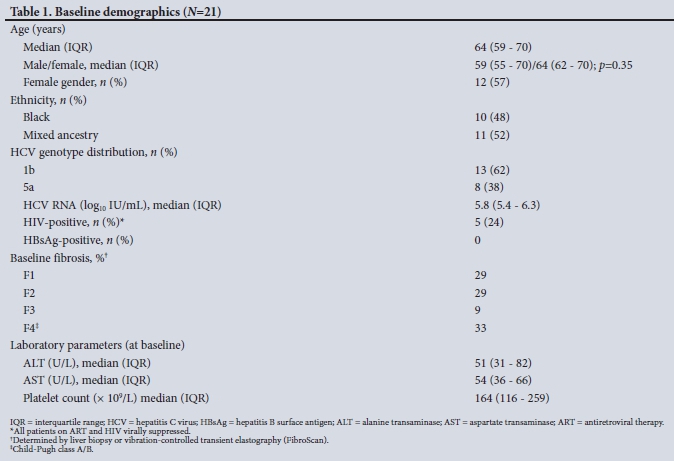
A total of 21 patients were evaluated and treated, of whom 12 (57%) were female. Table 1 shows the baseline demographic data. The median (IQR) age was 64 (59 - 70) years, with no significant difference between women and men (64 (62 - 70) v. 59 (55 - 70) years, respectively; p=0.35). HIV co-infection was present in 5 patients (24%), all on antiretroviral therapy and virally suppressed. Although the number of patients is small, HIV-positive patients were younger than HIV-negative patients (median 65 v. 61 years; p=0.05). Overall, only two HCV genotypes were observed, 1b and 5a, with most (n=13; 62%) GT1b-infected. Baseline liver fibrosis assessment yielded 42% with advanced fibrosis or established cirrhosis; all but 1 of those with cirrhosis had Child-Turcotte-Pugh class A compensated cirrhosis. Median alanine and aspartate transaminase levels, at51 U/L and 54 U/L, respectively (normal range 5 - 40 U/L), were elevated at baseline.
Table 2 depicts associated comorbidities as well as epidemiological factors likely to be associated with HCV acquisition risk from individual patient interviews. Hypertension and diabetes were frequently observed. No patients reported current or previous use of injecting drugs. Three patients reported receiving blood transfusions prior to 1992, all women and associated with peripartum haemorrhage. Notably, 13 patients (62%) reported a range of surgical interventions (as tabulated) or dental work. Of significance, almost all patients (n=20/21) reported having attended the town's local primary care clinic during the preceding decades, with all recalling having received parenteral therapies at the clinic.
Fig. 1 depicts the neighbour-joining phylogenetic tree of a concatenated sequence of the NS5A and NS5B regions of the HCV genome (1 015 base pairs), which was constructed using sequences from the study participants, other local sequences and reference sequences from the GenBank database. Patients were infected with either HCV GT1b or GT5a, and each formed a separate cluster within the respective genotypes. The clustering suggests a common source or mode of infection. In 2 cases (patients 11 and 15), samples from two different collection dates were available and each patient pair grouped together on the phylogenetic tree, indicating a close genetic relationship between sequences, although there was greater diversity in patient 11's samples from 2018 and 2019.

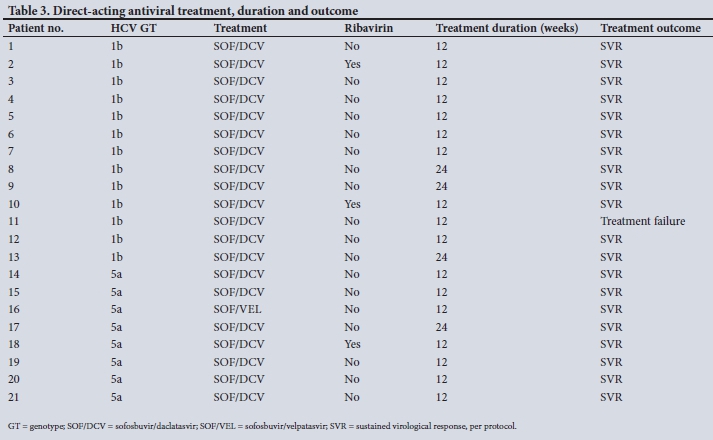
Table 3 reports the patient DAA therapy regimens and treatment outcomes. Most received sofosbuvir/daclatasvir, with 1 patient switched to sofosbuvir/velpatasvir after reporting gastrointestinal intolerance to daclatasvir after 1 week. No other significant adverse events were reported. Per protocol, 95% (20/21) achieved an SVR. The patient in whom treatment failed was successfully retreated with 12 weeks of sofosbuvir/ velpatasvir/voxilaprevir.
Discussion
We report our experience from a modest patient cohort, all emanating from a defined town in a rural area of SA and infected with HCV. These are the first such data to be reported in SA, and have advanced our understanding of HCV epidemiology in our country. We have also incidentally demonstrated that a treatment intervention for HCV-infected patients in this community is feasible and possible at point of service.
Several factors emerge from this patient cohort. Firstly, the median age of 64 years is much older than recently reported heterogeneous SA HCV patient cohorts, of 52 and 47 years, respectively.[9,17] Also, knowing the natural history of chronic HCV infection with a progression time to cirrhosis of ~20 - 40 years, infection in this cohort is likely to have occurred many years before, given that 42% had advanced fibrosis or cirrhosis.[18] It must, however, be noted that co-factors such as alcohol use and HIV co-infection influence the natural history of HCV. A substantial proportion (24%) of our cohort were HIV co-infected. Nonetheless, co-infection is usually seen in patients with shared transmission risks for HIV and HCV, such as people who inject drugs or MSM.[12] These shared transmission risk factors were not observed in our patient cohort, suggesting HIV infection possibly following previous HCV infection, through dissimilar transmission routes. Although HIV co-infected patients in this cohort were slightly younger, although not significantly, their median age of 61 years is considerably older than the median age of HIV-positive South Africans in the general population, where the prevalence peaks at 35 -39 years of age.[19] This finding further supports our contention that HCV acquisition in our cohort is likely to have occurred before their HIV infection and not through shared transmission routes.
Another pertinent finding is that the phylogenetic concatenated tree supports the probability that the two HCV genotypes observed each arise from a common source. SA is pan-genotypic for HCV, with numerous data supporting this and confirming the relative endemic nature of GT5a, with GT1 being equally prevalent.[20] Of the many sub-genotypes of GT1, GT1a and GT1b are most frequently observed in SA, with GT1b representing 38 - 70% of GT1 sub-genotypes, suggesting that the GT1b sub-genotype in our cohort is in keeping with local patterns.[9,20] GT5a has also not been detected in any key population studies to date - here GT1 and GT3a are prevalent[5]
Reviewing the patients' self-reported histories suggests a shared mode of HCV transmission. Most patients reported attending the local primary care clinic and receiving parenteral therapies at time points in their lives. Healthcare-associated HCV infection is well described, and our study suggests this as the possible shared route of transmission. To date, this has not been clearly documented in SA. As noted, the more frequent means of transmission such as PWID were absent in this cohort. Equally, blood services in SA have adopted universal HCV screening since 1992.[3] This had the effect of reducing this route of HCV transmission to almost zero in the general population.[21] Other risk factors, e.g. traditional practices such as scarification, were identified in some of our patients, but were not frequently reported. Even so, it would not explain the phylogenetic findings. Unsafe medical or injection practices and iatrogenic transmission, through inadequate infection control, are a key risk factor for HCV transmission in high-prevalence countries such as Egypt, India, Pakistan and other parts of Asia.[22-24] Our study suggests this transmission route to be the likely common risk transmission factor. Equally, it perhaps represents a historic route of HCV infection in SA, given the significant changes in infection control practice emerging in the 1990s consequent to HIV and other emerging pathogens. This too could further explain the older age of this patient cohort.
We would suggest that more extensive HCV testing is now justified in this community and should form part of an expanded viral hepatitis screening, prevention and treatment service. SA has a national strategic plan on viral hepatitis with guidance on the management of viral hepatitis, adopted in 2019. COVID-19, while having created many challenges for the health sector and attenuated many health policies, has demonstrated what can be achieved if resolve is present.[25]
An important aspect of our study was the delivery of care to HCV-infected patients in a rural town, at point of service, with consequent good outcomes. Such simplified care models are achievable, with decentralised care being delivered by local practitioners with support being provided by leveraging on technology such as the viral hepatitis ECHO programme started at the University of Cape Town and Groote Schuur Hospital in 2019.[26]
Conclusions
We report a patient cohort with HCV infection, observed to cluster from a rural SA town. The pattern was investigated through directly assessing patients and linking them to care at their point of service in their community. Epidemiological supported by virological data suggest probable previous unsafe administration of parenteral therapies as the mode of HCV transmission. Treatment outcomes were good; however, our findings warrant a specific intervention in this broader community to screen, diagnose and treat identified HCV infection.
Declaration. None.
Acknowledgements. We thank Médecins Sans Frontières, South Africa, for supporting us through their donation of DAA therapy, staff at the regional hospital for their generous time and support, and our patients, who placed their trust in us to achieve the benefit of curing their hepatitis C infection.
Author contributions. MWS was responsible for the design of the study and drafting the manuscript. JB designed the confidential questionnaire.
JH, JS, LB, JB and MWS all contributed to assessing and managing patients. HS performed all virological analysis. All authors contributed to the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. World Health Organization. Global hepatitis report 2017. Geneva: WHO, 2017. https://apps.who.int/iris/handle/10665/255016 (accessed 30 June 2021). [ Links ]
2. Polaris Observatory HCV Collaborators. Global prevalence and genotype distribution of hepatitis C virus infection in 2015: A modelling study. Lancet Gastroenterol Hepatol 2017;2(3):161-176. https://doi.org/10.1016/s2468-1253(16)30181-9 [ Links ]
3. Vermeiden M, Swanevelder R, Chowdhury D, et al. Use of blood donor screening to monitor prevalence of HIV and hepatitis B and C viruses, South Africa. Emerg Infect Dis 2017;23(9):1560-1563. https://doi.org/10.3201/eid2309.161594 [ Links ]
4. Prati D. Transmission of hepatitis C virus by blood transfusions and other medical procedures: A global review. J Hepatol 2006;45(4):607-616. https://doi.org/10.1016/j.jhep.2006.07.003 [ Links ]
5. Scheibe A, Young K, Versfeld A, et al. Hepatitis B, hepatitis C and HIV prevalence and related sexual and substance use risk practices among key populations who access HIV prevention, treatment and related services in South Africa: Findings from a seven-city cross-sectional survey (2017). BMC Infect Dis 2020;20(1):655. https://doi.org/10.1186/s12879-020-05359-y [ Links ]
6. Gogela NA, Sonderup MW, Rebe K, Chivese T, Spearman CW. Hepatitis C prevalence in HIV-infected heterosexual men and men who have sex with men. S Afr Med J 2018;108(7):568-572. https://doi.org/10.7196/SAMJ.2018.v108i7.13041 [ Links ]
7. Williams IT, Bell BP, Kuhnert W, Alter MJ. Incidence and transmission patterns of acute hepatitis C in the United States, 1982 - 2006. Arch Intern Med 2011;171(3):242-248. https://doi.org/10.1001/archinternmed.2010.511 [ Links ]
8. Ryerson AB, Schillie S, Barker LK, Kupronis BA, Wester C. Vital signs: Newly reported acute and chronic hepatitis C cases - United States, 2009 - 2018. MMWR Morb Mortal Wkly Rep 2020;69(14):399-404. https://doi.org/10.15585/mmwr.mm6914a2 [ Links ]
9. Sonderup MW, Gogela N, Nordien R, et al. Direct-acting antiviral therapy for hepatitis C: The initial experience of the University of Cape Town/Groote Schuur Hospital Liver Clinic, South Africa. S Afr Med J 2020;110(2):112-117. https://doi.org/10.7196/SAMJ.2020.v110i2.14195 [ Links ]
10. Makuza JD, Nisingizwe MP, Rwema JOT, et al. Role of unsafe medical practices and sexual behaviours in the hepatitis B and C syndemic and HIV co-infection in Rwanda: A cross-sectional study. BMJ Open 2020;10(7):e036711. https://doi.org/10.1136/bmjopen-2019-036711 [ Links ]
11. Pozzetto B, Memmi M, Garraud O, Roblin X, Berthelot P. Health care-associated hepatitis C virus infection. World J Gastroenterol 2014;20(46):17265-17278. https://doi.org/10.3748/wjg.v20.i46.17265 [ Links ]
12. Spearman CW, Dusheiko GM, Hellard M, Sonderup M. Hepatitis C. Lancet 2019;394(10207):1451-1466. https://doi.org/10.1016/S0140-6736(19)32320-7 [ Links ]
13. Hall TA, ed. BioEdit: A user-friendly biological sequence alignment editor and analysis program for Windows 95/98/NT. Nucleic Acids Symposium series, 1999. London: Information Retrieval Ltd, c1979-c2000. https://doi.org/10.14601/Phytopathol_Mediterr-14998u1.29 (accessed 30 June 2021). [ Links ]
14. Tamura K, Stecher G, Peterson D, Filipski A, Kumar S. MEGA6: Molecular evolutionary genetics analysis version 6.0. Mol Biol Evol 2013;30(12):2725-2729. https://doi.org/10.1093/molbev/mst197 [ Links ]
15. Bedossa P, Poynard T. An algorithm for the grading of activity in chronic hepatitis C. The METAVIR Cooperative Study Group. Hepatology 1996;24(2):289-293. https://doi.org/10.1002/hep.510240201 [ Links ]
16. Garcia-Tsao G. The Child-Turcotte classification: From gestalt to sophisticated statistics and back. Dig Dis Sci 2016;61(11):3102-3104. https://doi.org/10.1007/s10620-016-4319-7 [ Links ]
17. Nordien R, Sonderup MW, Spearman CW. A decade of hepatitis C at the University of Cape Town/ Groote Schuur Hospital Liver Clinic, South Africa, in the pre-direct-acting antivirals era. S Afr Med J 2020;110(2):106-111. https://doi.org/10.7196/SAMJ.2020.v110i2.14208 [ Links ]
18. Lingala S, Ghany MG. Natural history of hepatitis C. Gastroenterol Clin North Am 2015;44(4):717-734. https://doi.org/10.1016/j.gtc.2015.07.003 [ Links ]
19. South African National Aids Council. 2016 Global AIDS Response Progress Report. https://sanac.org.za//wp-content/uploads/2017/06/MandE-SANAC-Global-AIDS-Response-Progress-Report_2016.pdf (accessed 30 June 2021). [ Links ]
20. Prabdial-Sing N, Chirwa T, Thaver J, et al. Hepatitis C genotype distribution in patient and blood donor samples in South Africa for the period 2008 - 2012. J Viral Hepat 2016;23(11):881-888. https://doi.org/10.1111/jvh.12571 [ Links ]
21. Apata IW, Averhoff F, Pitman J, et al. Progress toward prevention of transfusion-transmitted hepatitis B and hepatitis C infection - sub-Saharan Africa, 2000 - 2011. MMWR Morb Mortal Wkly Rep 2014;63(29):613-619. [ Links ]
22. Kouyoumjian SP, Chemaitelly H, Abu-Raddad LJ. Characterizing hepatitis C virus epidemiology in Egypt: Systematic reviews, meta-analyses, and meta-regressions. Sci Rep 2018;8(1):1661. https://doi.org/10.1038/s41598-017-17936-4 [ Links ]
23. Mahajan R, Midha V, Goyal O, et al Clinical profile of hepatitis C virus infection in a developing country: India. J Gastroenterol Hepatol 2018;33(4):926-933. https://doi.org/10.1111/jgh.13995 [ Links ]
24. Pépin J, Abou Chakra CN, Pépin E, Nault V, Valiquette L. Evolution of the global burden of viral infections from unsafe medical injections, 2000 - 2010. PLoS One 2014;9(6):e99677. https://doi.org/10.1371/journal.pone.0099677 [ Links ]
25. Gupta N, Desalegn H, Ocama P, et al. Converging pandemics: Implications of COVID-19 for the viral hepatitis response in sub-Saharan Africa. Lancet Gastroenterol Hepatol 2020;5(7):634-636. https://doi.org/10.1016/S2468-1253(20)30155-2 [ Links ]
26. Spearman CWN, Sonderup MW. Launch of the Viral Hepatitis in sub-Saharan Africa Project ECHO program. S Afr Gastroenterol Rev 2019;17(2):43. https://www.cpdcentre.co.za/publications_/2019/SAGES_Volume17_Issue2_ADS/13/ (accessed 30 June 2021). [ Links ]
 Correspondence:
Correspondence:
M W Sonderup
msonderup@samedical.co.za
Accepted 9 March 2021


{kind=link}
{kind=link}
{kind=link}