










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.111 n.8 Pretoria Aug. 2021
http://dx.doi.org/10.7196/samj.2021.v111i8.15604
RESEARCH
Antiretroviral therapy non-adherence among HIV-positive patients presenting to an emergency department in Johannesburg, South Africa: Associations and reasons
A E LaherI; G A RichardsII; F ParukIII; W D F VenterIV
IMB BCh, MMed (Emerg Med), FCEM, Cert Critical Care (SA), EDIC, Dip PEC (SA), DCH, Dip Allerg (SA), Dip HIV Man (SA); Department of Emergency Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMB BCh, PhD, FCP, FRCP, FCCP; Department of Critical Care, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIMB ChB, PhD, FCOG, Cert Critical Care (SA); Department of Critical Care, School of Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
IVMB BCh, MMed (Int Med), PhD, FCP, Cert ID (SA), DTM&H, Dip HIV Man (SA); Ezintsha, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Suboptimal antiretroviral therapy (ART) adherence is associated with viral resistance, opportunistic infections and increased mortality
OBJECTIVES: To determine the rates of ART non-adherence and its associations, and also the reasons for ART non-adherence, among HIVpositive patients presenting to a major central hospital emergency department (ED
METHODS: Consecutive HIV-positive patients presenting to the Charlotte Maxeke Johannesburg Academic Hospital adult ED between 7 July 2017 and 18 October 2018 were prospectively enrolled. Self-reported adherence was assessed using the AIDS Clinical Trials Group Adherence Questionnaire (ACTG-AQ
RESULTS: Of the 1 224 consecutive HIV-positive participants enrolled, 761 (75.2%) were on ART at the time of ED presentation. Of these, 245 (32.2%) were non-adherent as per the ACTG-AQ. Participants not yet on ART prior to ED presentation had significantly higher in-hospital mortality than participants on ART (odds ratio 1.69; 95% confidence interval 1.21 - 2.34; p=0.002). Younger age, male sex, CD4 count <100 cells/(μL, lack of viral suppression, a high National Early Warning Score 2 (>7 points) and length of hospital stay >7 days were significantly associated with ART non-adherence (p<0.05). Forgetfulness (13.9%) and lack of social support, depression/stress/mental illness, and lack of money for transport to collect medications (9.9% each) were the most common reasons given for ART non-adherence
CONCLUSIONS: Of HIV-positive patients presenting to the ED, a high proportion were either not yet initiated on ART or ART non-adherent. HIV programmes should focus on HIV-positive ED attendees with the aim of identifying high-risk patients and providing adequate ART adherence support
Sub-Saharan Africa has the highest prevalence of HIV in the world, with more than two-thirds of the global cases.[1] In 2019, South Africa (SA) had an estimated 7.5 million people living with HIV (PLWH), more than any other country in the world. The most current Joint United Nations Program on HIV/AIDS (UNAIDS) data report estimates that 92% of PLWH in SA are aware of their status, 70% are on antiretroviral therapy (ART), and 64% are virally suppressed.[2]
The use of ART in PLWH has been associated with improvement in health-related quality of life and an overall reduction in the transmission of HIV,[3,4] whereas suboptimal adherence has been associated with a reduction in rates of viral suppression and an increase in rates of viral resistance, opportunistic infections, progression to AIDS and mortality.[5-9] In 2014, UNAIDS set a target for 90% of persons diagnosed with HIV to be on sustained ART by the year 2020.[10] Studies have shown that in order to achieve optimal viral suppression, ART adherence must be maintained above 90 - 95%.[7,11,12]
ART has been made available at SA public sector healthcare facilities since 2004, with significant strides over recent years in making ART more accessible to PLWH.[13] Currently there are ~5 million South Africans on ART, which is freely available at>3 500 healthcare facilities across the country.[2,14] Over the past decade, criteria for the initiation of ART in SA have gradually been relaxed in line with the World Health Organization recommendations, and as of September 2016, all HIV-positive patients, irrespective of their CD4 cell count or stage of disease, are considered eligible for ART initiation.[15]
ART adherence rates have been measured by various methods including patient self-reporting, pill counts, pharmacy records, electronic medication monitoring devices, and laboratory evidence of virological or immunological failure.[11] In comparison with alternative measures of adherence, there is a tendency for patient self-reporting to overestimate ART adherence.[5] However, owing to its ease of use, this method remains widely used.[16]
There is a lack of data pertaining to the rates of ART adherence and reasons for poor adherence among HIV-positive patients presenting to the emergency department (ED) with an acute illness. Because acutely ill HIV-positive patients frequently present with opportunistic infections and related pathology, we hypothesised that the rate of suboptimal adherence would be high in this group. Findings pertaining to other aspects of this study have been published separately.[17,18]
Objectives
To explore ART non-adherence and its associations, and also determine the reasons for non-adherence among HIV-positive patients presenting to the ED.
Methods
This was a cross-sectional study conducted at the adult medical ED at Charlotte Maxeke Johannesburg Academic Hospital (CMJAH). CMJAH is a 1 088-bed tertiary-level academic hospital affiliated to the University of the Witwatersrand. The adult medical ED manages all non-trauma patients >16 years of age. On arrival in the ED triage area, patients are briefly assessed and categorised as 'emergency' (red), 'very urgent' (orange), 'urgent' (yellow) or 'routine' (green), based on specific criteria as defined by the South African Triage Scale.[19] Because CMJAH is a tertiary-level facility, patients who are categorised as red, orange or yellow are generally managed at the facility, while stable patients who are categorised as green are referred to an alternative facility. Additionally, clinically stable patients not residing within the drainage area of the facility are referred to an alternative facility closer to the patient's home.
As per the facility protocol, apart from patients already known to be HIV-positive (either self-reported or confirmed on laboratory records of patients who had previously attended the facility), all other patients attending the ED are offered HIV rapid diagnostic testing to determine their HIV status. Whole-blood samples of patients consenting to HIV testing are tested with the Abon HIV 1/2/0 Tri-Line rapid test (Abon Biopharm, China), with reactive samples being subjected to a second confirmatory rapid test (First Response HIV 1-2.0 card, PMC Medical India Pvt Ltd, India). If the first test is positive but the confirmatory test is negative, a sample of whole blood is collected and sent to the laboratory for enzyme-linked immunosorbent assay HIV testing.
Data collection commenced once ethics clearance (University of the Witwatersrand Human Research Ethics Committee, ref. no. M160512) and relevant permissions had been obtained. Adult patients aged >18 years who had previously tested positive for HIV, as well as those newly diagnosed with HIV after undergoing testing in the ED, were prospectively enrolled into the study between 7 July 2017 and 18 October 2018. They included HIV-positive patients who required admission as well as patients who were directly discharged from the ED, but excluded patients who were referred to another facility from the triage section. In addition, HIV-negative patients, patients with unknown HIV status who did not consent to HIV testing, and patients who did not consent to study participation were excluded.
Prior to the commencement of data collection, informal training pertaining to the methodology and principles of data collection from medical charts was undertaken by the primary investigator. After all doctors employed in the ED had been briefed regarding the study objectives and design, they were requested to inform the primary investigator of all HIV-positive patients being managed in the ED. Written informed consent for study participation was obtained from potential participants by either the primary investigator or the doctor on shift. In the event that participants were unable to grant consent (e.g. decreased level of consciousness), consent was obtained from the next of kin/legal guardian and later from the participant if their mental capacity improved. ED registers were also reviewed daily in an effort to identify potential participants who may have been missed by the ED doctors.
The four-question AIDS Clinical Trials Group Adherence Questionnaire (ACTG-AQ) was utilised to determine non-adherence to ART: (i) have you missed your antiretroviral therapy pills yesterday; (ii) have you missed your antiretroviral therapy pills the day before yesterday; (iii) have you missed your antiretroviral therapy pills during the past weekend; and (iv) have you missed your antiretroviral therapy pills in the past 2 weeks.[20] Patients who responded 'yes' to any of the questions were considered to be ART non-adherent and were further engaged to explore reasons for non-adherence. The questionnaire was administered to all participants who had been prescribed ART at any time in the past.
For the purposes of the study, virological failure was defined as an HIV viral load (VL) >1 000 copies/mL measured at ED presentation, and viral suppression was defined as an HIV VL <50 copies/mL measured at ED presentation.
Data were extracted from the patient's hospital file by the primary investigator and electronically entered into an anonymised and standardised data collection form that was created in the REDCap system.[21] Additional information relevant to the study but not found in the patient's hospital records was directly obtained from the participant, the participant's laboratory records, or the participant's next of kin/legal guardian where applicable. Only where the next of kin/legal guardian indicated that they were aware of the participant's HIV status were they questioned regarding relevant HIV history such as treatment adherence. Data from hospital records were collected daily over the entire duration of hospital stay or until data collection was completed. Inter-rater reliability was assessed by an independent researcher experienced in the methods of data collection and blinded to the study objectives. Data extracted from a random sample of 43 medical charts were compared with data extracted by the primary investigator.
Data relevant to this study included demographic details, HIV status, prior ART history including non-adherence, reasons for ART non-adherence, CD4 cell count and VL measured during the current presentation, hospital length of stay and in-hospital mortality. In addition, data pertaining to respiratory rate, oxygen saturation, temperature, systolic blood pressure, heart rate and Glasgow Coma Scale score were collected and used to calculate the quick Sequential Organ Failure Assessment (qSOFA) score and the National Early Warning Score 2 (NEWS-2). Both the qSOFA score and the NEWS-2 are standardised scoring tools that characterise acute illness severity, with higher scores indicating greater severity of illness and a higher risk of worse outcomes.[22,23]
Data were exported to Microsoft Excel (Office 365, 16.0.13029. 20232; Microsoft, USA) and thereafter to Stata version 16 (StataCorp, USA) for statistical analysis. Frequencies and percentages were determined for categorical variables. Depending on the frequency of participants in each group, either Pearson's x2 test or Fisher's exact test was used to determine whether there were significant differences between the two groups. Since data for continuous variables were not normally distributed, medians and interquartile ranges (IQRs) were calculated, while the Mann-Whitney rank-sum test was used to determine whether there were significant differences between the two groups. The two groups were further analysed by univariate logistic regression, and odds ratios (ORs) for ART non-adherence were determined for each of the variables. A two-sided p-value <0.05 was considered significant throughout. Study reporting conformed with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.[24]
Results
During the data collection period, 29 416 patients presented to the adult medical ED triage area, of whom 11 383 were triaged into the ED for further management. The remaining patients were referred to an appropriate facility in accordance with the CMJAH ED triage protocol. A total of 1 308 patients were HIV-positive, of whom 84 were excluded from the study because informed consent could not be obtained.
A total of 1 224 HIV-positive participants were included in the final study sample. Approximately one-sixth of the participants were newly diagnosed with HIV (n=212; 17.3%). Participants who were newly diagnosed had a significantly lower median (IQR) CD4 cell count (81 (22.5 - 171.5) cells/μL v. 125 (35.5 - 332) cells/μL; p<0.001) and a significantly higher median (IQR) HIV VL (253 500 (36 150 -913 193.5) copies/mL v. 1 400 (10 - 215 502.5) copies/mL; p<0.001) than participants who had been diagnosed prior to ED presentation.
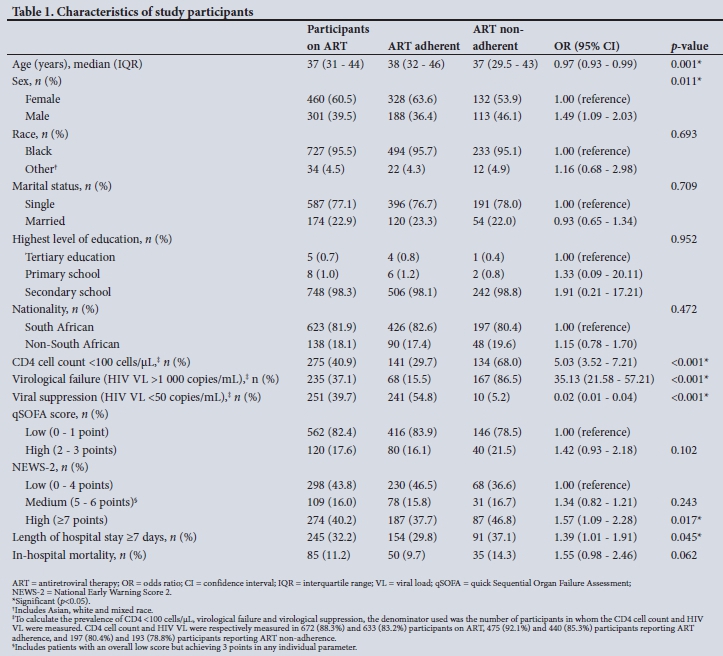
Of the 1 012 participants (82.7%) who had been diagnosed with HIV prior to ED presentation, 761 (75.2%) were on ART, of whom 516 (67.8%) were adherent and 245 (32.2%) non-adherent as per the ACTG-AQ self-report questionnaire utilised in the study. The median age of participants on ART was 37 (interquartile range 31 - 44) years, with the majority being female (n=460; 60.4%), unmarried (n=587; 77.1%) and having completed secondary school as the highest level of education (n=748; 98.3%).
Table 1 describes and compares demographic characteristics, including the number of participants with a CD4 cell count <100 cells/μL, the number presenting with virological failure, the number presenting with viral suppression, the median qSOFA score, the median NEWS-2, the median length of hospital stay and in-hospital mortality, between participants who were ART adherent and those who were non-adherent.
There were significant differences between participants who were ART adherent and those who were non-adherent with regard to age, sex, CD4 cell count <100 cells/μL, virological failure, viral suppression, NEWS-2 and length of hospital stay. Every year's increase in age was associated with a 3% (p=0.001) lower likelihood of ART non-adherence, while males had a 49% (p=0.011) higher likelihood of ART non-adherence. Overall, those who had not been initiated on ART prior to ED presentation (n=81; 17.5%) had higher in-hospital mortality than those who had been initiated on ART (n=85; 11.2%), with the former having a 69% higher likelihood of death (OR 1.69; 95% confidence interval 1.21 - 2.34; p=0.002).
Participants with a CD4 cell count <100 cells/μL and those with virological failure had a 5.03 times (p<0.001) and 35.13 times (p<0.001) higher likelihood of ART non-adherence, respectively, whereas participants who were virally suppressed had a 98% (p<0.001) lower likelihood of ART non-adherence.
Compared with participants with a low qSOFA score (0 - 1 point) at presentation, there were no statistically significant differences with regard to ART non-adherence among those with a high qSOFA score (2 - 3 points) (p=0.102). Compared with participants with a low NEWS-2 (0 - 4 points) at presentation, those with a medium NEWS-2 (5 - 6 points overall, or an overall low score but achieving 3 points for any individual parameter) did not have a statistically significant difference with regard to ART non-adherence, but those with a high NEWS-2 (>7 points) had a 57% (p=0.017) higher likelihood of ART non-adherence.
Participants who required hospital admission for >7 days had a 39% (p=0.045) higher likelihood of ART non-adherence. Although in-hospital mortality was associated with a 55% (p=0.062) higher likelihood of ART non-adherence, it did not reach (though marginally) statistical significance.
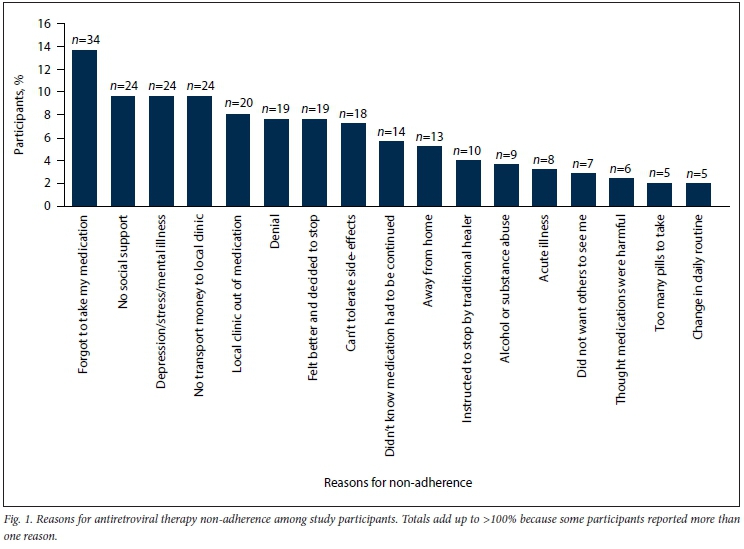
Fig. 1 describes the reasons for ART non-adherence. Two hundred and twenty-nine participants (93.5%) reported a single reason for non-adherence, while the remaining 16 (6.5%) reported two reasons each. Of note, 'Forgot to take my medication' was reported as the most common reason (n=34; 13.9%), followed by 'No social support', 'Depression/stress/mental illness' and 'No transport money to local clinic' at 9.9% (n=24) each.
Discussion
To our knowledge, no previous studies have reported on ART adherence among acutely ill HIV-positive patients presenting to an ED in southern Africa. Most published studies relating to ART adherence were conducted in non-acutely ill patients attending outpatient ART clinics.[25] Overall, our findings indicate that the ED setting is an ideal opportunity to identify high-risk HIV-positive patients.
Despite rigorous nationwide HIV awareness campaigns,[26] approximately one-sixth of the study participants (17.2%) were only diagnosed at ED presentation. However, this figure is better than the findings by Hansoti et al[27]at the Frere Hospital ED in East London, SA, where 115 out of 400 HIV-positive participants (28.75%) were newly diagnosed with HIV at ED presentation. Of concern, newly diagnosed HIV-positive participants had very low CD4 cell counts and high VLs. This finding calls for an urgent public health response, and ascertaining the reasons for this group presenting with late-stage disease should be considered a research priority. Additionally, this finding indicates the need to further improve local HIV awareness programmes with particular emphasis on the importance of early testing.
Despite ART being freely available to all PLWH in SA,[15] only 83.3% of study participants diagnosed with HIV >1 month prior to ED presentation had been initiated on ART. This is, however, higher than current national figures indicating that ~70% of PLWH in SA have been initiated on ART. It may also be a reflection of the ART programme being well established in central Johannesburg.[2] Furthermore, study participants who were on ART prior to ED presentation had significantly lower in-hospital mortality than those who were not on ART (p=0.002). Reduction in the rates of clinical deterioration as well as several other benefits associated with the early initiation of ART have been well described in previous studies.[28,29]
As per the ACTG-AQ questionnaire used in this study, approximately a third (32.2%) of study participants on ART were non-adherent, whereas if we had relied on the presence of virological failure as a marker of non-adherence, a slightly higher percentage of participants (37.2%) would have been regarded as non-adherent. In contrast, a study conducted in 2019 in Durban, SA, among non-acutely ill patients reported ART adherence in >95% of the 270 participants who were enrolled. However, the authors used pharmacy pill counts as a measure to determine non-adherence.[30] Results of a meta-analysis that included 33 199 pooled patients from 84 studies reported an overall global rate of ART adherence of 62%. Adherence was assessed using one method only in 63 studies (75%), two methods in 20 studies (23.8%) and three methods in one study (1.2%). Self-reporting was the most frequently used technique, employed in 77 of the included studies. None of these included studies were conducted in the ED or in patients presenting with acute illness.[31]
In the present study, age and sex were significantly associated with ART adherence, with the odds of ART non-adherence being significantly higher among younger participants and males. Similarly, in a systematic review that included 146 studies conducted in sub-Saharan Africa, age was reported in 20 of the included articles as a determinant of adherence, with poor adherence being more prominent in younger individuals overall. Among studies that reported on sex differences, 11 reported better adherence among females, while 6 reported better adherence among males.[32]
It is not surprising that virological failure was significantly more prevalent among ART non-adherent study participants (84.5% v. 15.5%) and that viral suppression was significantly more prevalent among ART-adherent participants (54.8% v. 5.2%). Comparatively, in a study by Arnsten et al.,[5]62% of participants were virally suppressed. However, these authors defined viral suppression as a VL <500 copies/mL, whereas in our study we used a much lower threshold of <50 copies/mL (as per the 2019 National Department of Health guidelines[33]). If we had also used a higher threshold of <500 copies/mL, 77.7% of participants with reported ART adherence would have achieved viral suppression.
The facts that virological failure was still present in ~15% of ART-adherent study participants and that viral suppression was not achieved in almost half of ART-adherent participants are of concern. While pharmacokinetic drug-drug interactions and ART drug resistance may be responsible for the lack of viral suppression in some cases, ART non-adherence is more likely to be the underlying reason in most cases.[34] It is therefore possible that ART non-adherence was under-reported by study participants, and the ACTG-AQ questionnaire used in this study may not have been sufficiently sensitive to identify all cases of non-adherence. A transient increase in the VL (viral 'blip'), which is common in the setting of intercurrent illness, may also have contributed to the relatively low rates of viral suppression among ART-adherent study participants.[35]
Similarly, a CD4 count <100 cells/μL was identified in almost one-third of ART-adherent study participants (29.7%). Taking into consideration that a low CD4 cell count may be a prominent feature in any patient with acute illness (independent of the underlying HIV status),[36] this finding may well account for the relatively high number of participants with a low CD4 cell count. In the setting of acute intercurrent illness, the presence of a low CD4 cell count and a high HIV VL may therefore not necessarily be reliable indicators of ART treatment failure.
Furthermore, the significantly higher proportion of ART non-adherent participants presenting with a high NEWS-2 and also requiring a longer hospital length of stay (>7 days), and the trend towards higher in-hospital mortality in ART non-adherent participants, indicate that this group presented with more severe illness.
In the present study, 'forgetfulness' (13.9%), followed by 'lack of social support', 'depression/stress/mental illness' and 'no transport money to collect medication' (n=24, 9.9% each) were reported as the most frequent reasons for ART non-adherence. In a study that also used the ACTG-AQ to determine non-adherence among 200 patients attending an ART clinic in New Delhi, India, ART non-adherence was reported in 10% of participants, with 'travel' (10.5%) and 'forgetfulness' (9.5%) reported as the most frequent reasons.[25] A separate study that used a modified ACTG questionnaire to assess non-adherence among 151 patients in Mississippi, USA, reported that 47.7% of patients were non-adherent.[37] In contrast to our study, the authors reported the most frequent reasons as 'not having the medication with them' (39%), 'sleeping through the dose time' (25%), 'running out of the medication' (22%), and 'being busy with other things' (21%).[37]
In a recent study conducted in Uganda, 20% of participants reported ART side-effects or fear of side-effects as the reason for non-adherence, while 26.7% indicated that alternative medicines were preferred over ART.[38] Comparatively, in the present study, 7.3% of respondents reported intolerable side-effects as the reason, while 4.1% reported that they were instructed to stop their ART by a traditional healer.
A systematic review and meta-analysis that included 125 studies across 38 countries with ~19 016 pooled participants cited the most frequently reported reasons for ART non-adherence among adult patients as forgetfulness (41.4%), being away from home (30.4%), a change in daily routine (28.0%), depression (15.5%), alcohol/substance misuse (12.9%), secrecy/stigma (13.6%), feeling sick (15.9%) and pharmacy stock-outs (16.1%).[39] In comparison, in the present study, frequency rates for the above reasons were as follows: forgetting (13.9%), being away from home (5.7%), a change in daily routine (2.0%), depression (9.8%), alcohol/substance misuse (3.7%), secrecy/stigma (2.9%), feeling sick (3.3%) and pharmacy stock-outs (8.2%).
Study limitations
There are some limitations to this study. Firstly, measurement of adherence was reliant on the ACTG-AQ questionnaire, which only determined ART adherence over the 2 weeks before ED presentation. This may have resulted in under-reporting of overall adherence, as some participants may have been non-adherent prior to the 2 weeks before ED presentation, but were more adherent in the past 2 weeks owing to the onset of symptoms of acute illness. Fear of being reprimanded, the acuity of the presenting illness and reliance on information from the next of kin or relatives may be other reasons for inaccurate reporting of ART adherence. Although reasons for a low CD4 cell count and virological failure were not explored, it is likely that the relatively high proportion of ART-adherent participants with a high VL and low CD4 cell count may also indicate that ART non-adherence rates were possibly higher than reported.
Conclusions
HIV-positive participants not initiated on ART and presenting with acute illness to the ED had significantly higher mortality than HIVpositive participants who had been initiated on ART. Younger age, male sex, CD4 count <100 cells/μL, virological failure, lack of viral suppression, a higher NEWS-2, and length of hospital stay >5 days were significantly associated with ART non-adherence among acutely ill HIV-positive patients presenting to the ED. There is a need for improved local HIV awareness and educational programmes, and for these programmes to further emphasise the importance of early testing, early initiation of ART and ART adherence.
Declaration. The research for this study was done in partial fulfilment of the requirements for AEL's PhD degree at the University of the Witwatersrand.
Acknowledgements. The authors thank the staff at the CMJAH for their assistance with identifying potential study participants.
Author contributions. AEL was the primary author and was responsible for the study design, data collection, data analysis, manuscript write-up, revision of the manuscript and approval of the final manuscript. GAR, FP and WDFV assisted with the study design, interpretation of results, revision of the manuscript and approval of the final manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Shisana O, Rehle T, Simbayi L, et al South African National HIV Prevalence, Incidence and Behaviour Survey, 2012. Cape Town: HSRC Press, 2014. https://www.hst.org.za/publications/NonHST%20Publications/SA%20National%20HIV%20Prevalence%20Incidence%20and%20Behaviour%20Survey%202012.pdf (accessed 20 August 2020). [ Links ]
2. Joint United Nations Program on HIV/AIDS (UNAIDS). UNAIDS Data 2020. https://www.unaids.org/sites/default/files/media_asset/2020_aids-data-book_en.pc (accessed 21 August 2020). [ Links ]
3. Gakhar H, Kamali A, Holodniy M. Health-related quality of life assessment after antiretroviral therapy: A review of the literature. Drugs 2013;73(7):651-672. https://doi.org/10.1007/s40265-013-0040-4 [ Links ]
4. Albert J, Berglund T, Gisslén M, et al. Risk of HIV transmission from patients on antiretroviral therapy: A position statement from the Public Health Agency of Sweden and the Swedish Reference Group for Antiviral Therapy. Scand J Infect Dis 2014;46(10):673-677. https://doi.org/10.3109/00365548.2014.926565 [ Links ]
5. Arnsten JH, Demas PA, Farzadegan H, et al. Antiretroviral therapy adherence and viral suppression in HIV-infected drug users: Comparison of self-report and electronic monitoring. Clin Infect Dis 2001;33(8):1417-1423. https://doi.org/10.1086/323201 [ Links ]
6. Low A, Gavriilidis G, Larke N, et al. Incidence of opportunistic infections and the impact of antiretroviral therapy among HIV-infected adults in low- and middle-income countries: A systematic review and meta-analysis. Clin Infect Dis 2016;62(12):1595-1603. https://doi.org/10.1093/cid/ciw125 [ Links ]
7. Bangsberg DR, Perry S, Charlebois ED, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS 2001;15(9):1181-1183. https://doi.org/10.1097/00002030-200106150-00015 [ Links ]
8. Mannheimer S, Friedland G, Matts J, Child C, Chesney M. The consistency of adherence to antiretroviral therapy predicts biologic outcomes for human immunodeficiency virus-infected persons in clinical trials. Clin Infect Dis 2002;34(8):1115-1121. https://doi.org/10.1086/339074 [ Links ]
9. Maphula RW, Laher AE, Richards GA. Patterns of presentation and survival of HIV-infected patients admitted to a tertiary-level intensive care unit. HIV Med 2020;21(5):334-341. https://doi.org/10.1111/hiv.12834 [ Links ]
10. Joint United Nations Program on HIV/AIDS (UNAIDS). 90-90-90: An ambitious treatment target to help end the AIDS epidemic. 2014. http://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf (accessed 22 May 2017). [ Links ]
11. Turner BJ. Adherence to antiretroviral therapy by human immunodeficiency virus-infected patients. J Infect Dis 2002;185(s2):S143-S151. https://doi.org/10.1086/340197 [ Links ]
12. Paterson DL, Swindells S, Mohr J, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med 2000;133(1):21-30. https://doi.org/10.7326/0003-4819-133-1-200007040-00004 [ Links ]
13. Abdool Karim SS, Churchyard GJ, Karim QA, Lawn SD. HIV infection and tuberculosis in South Africa: An urgent need to escalate the public health response. Lancet 2009;374(9693):921-933. https://doi.org/10.1016/S0140-6736(09)60916-8 [ Links ]
14. Bekker L-G, Venter F, Cohen K, et al. Provision of antiretroviral therapy in South Africa: The nuts and bolts. Antivir Ther 2014;19(Suppl 3):105-116. https://doi.org/10.3851/IMP2905 [ Links ]
15. Cullinan K. ARVs now for anyone with HIV - Motsoaledi. Health24, 10 May 2016. http://www.health24.com/medical/hiv-aids/management-of-hiv-aids/arvs-now-for-anyone-with-hiv-says-minister-20160510 (accessed 8 August 2020). [ Links ]
16. Berg KM, Arnsten JH. Practical and conceptual challenges in measuring antiretroviral adherence. J Acquir Immune Defic Syndr 2006;43(Suppl 1):S79-S87. https://doi.org/10.1097/01.qai.0000248337.97814.66 [ Links ]
17. Laher AE, Venter WDF, Richards GA, Paruk F. Profile of presentation of HIV-positive patients to an emergency department in Johannesburg, South Africa. South Afr J HIV Med 2021;22(1):a1177. https://doi.org/10.4102/sajhivmed.v22i1.1177 [ Links ]
18. Laher AE, Paruk F, Venter W, Ayeni O, Richards G. Predictors of in-hospital mortality among HIVpositive patients presenting with an acute illness to the emergency department. HIV Med 2021 (epub 31 March 2021). https://doi.org/doi:10.1111/hiv.13097 [ Links ]
19. Bruijns SR, Wallis LA, Burch VC. A prospective evaluation of the Cape triage score in the emergency department of an urban public hospital in South Africa. Emerg Med J 2008;25(7):398-402. https://doi.org/10.1136/emj.2007.051177 [ Links ]
20. Chesney MA, Ickovics JR, Chambers DB, et al. Self-reported adherence to antiretroviral medications among participants in HIV clinical trials: The AACTG Adherence Instruments. AIDS Care 2000;12(3):255-266. https://doi.org/10.1080/09540120050042891 [ Links ]
21. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42(2):377-381. https://doi.org/10.1016/j.jbi.2008.08.010 [ Links ]
22. qSOFA: quick Sepsis Related Organ Failure Assessment. 2016. http://qsofa.org/ (accessed 13 September 2020). [ Links ]
23. Royal College of Physicians. National Early Warning Score (NEWS) 2. 19 December 2017. https://www.rcplondon.ac.uk/projects/outputs/national-early-warning-score-news-2 (accessed 12 September 2020). [ Links ]
24. Von Elm E, Altman DG, Egger M, Pocock SJ, G0tzsche PC, Vandenbroucke JP. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007;335(7624):806-808. https://doi.org/10.1136/bmj.39335.541782.AD [ Links ]
25. Lal V, Kant S, Dewan R, Rai S. Reasons for non-adherence to antiretroviral therapy among adult patients receiving free treatment at a tertiary care hospital in Delhi. Indian J Community Med 2010;35(1):172-173. https://doi.org/10.4103/0970-0218.62590 [ Links ]
26. Medwiser. HIV/AIDS in South Africa. https://www.medwiser.org/hiv-aids/around-the-world/hivaids-in-south-africa/ (accessed 3 September 2020). [ Links ]
27. Hansoti B, Stead D, Parrish A, et al. HIV testing in a South African emergency department: A missed opportunity. PLoS ONE 2018;13(3):e0193858. https://doi.org/10.1371/journal.pone.0193858 [ Links ]
28. Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med 2011;365(6):493-505. https://doi.org/10.1056/NEJMoa1105243 [ Links ]
29. Lee SA, Deeks SG. The benefits of early antiretroviral therapy for HIV infection: How early is early enough? EBioMedicine 2016;11:7-8. https://doi.org/10.1016/j.ebiom.2016.08.009 [ Links ]
30. Moosa A, Gengiah TN, Lewis L, Naidoo K. Long-term adherence to antiretroviral therapy in a South African adult patient cohort: A retrospective study. BMC Infect Dis 2019;19(1):775. https://doi.org/10.1186/s12879-019-4410-8 [ Links ]
31. Ortego C, Huedo-Medina TB, Llorca J, et al. Adherence to highly active antiretroviral therapy (HAART): A meta-analysis. AIDS Behav 2011;15(7):1381-1396. https://doi.org/10.1007/s10461-011-9942-x [ Links ]
32. Heestermans T, Browne JL, Aitken SC, Vervoort SC, Klipstein-Grobusch K. Determinants of adherence to antiretroviral therapy among HIV-positive adults in sub-Saharan Africa: A systematic review. BMJ Glob Health 2016;1(4):e000125. https://doi.org/10.1136/bmjgh-2016-000125 [ Links ]
33. National Department of Health, South Africa. 2019 ART Clinical Guidelines for the Management of HIV in Adults, Pregnancy, Adolescents, Children, Infants and Neonates. October 2019 (updated March 2020). https://sahivsoc.org/Files/2019%20ART%20Guideline%2028042020%20pdf.pdf (accessed 11 September 2020). [ Links ]
34. Moneti V, Luís N, Rijo J, et al Causes of virological failure in a population of 1895 HIV-infected patients: The experience of an infectious diseases service in Lisbon, Portugal. J Int AIDS Soc 2012;15(6, Suppl 4). https://doi.org/10.7448/IAS.15.6.18065 [ Links ]
35. Jones L, Perelson A. Opportunistic infection as a cause of transient viremia in chronically infected HIV patients under treatment with HAART. Bull Math Biol 2005;67(6):1227-1251. https://doi.org/10.1016/j.bulm.2005.01.006 [ Links ]
36. Feeney C, Bryzman S, Kong L, Brazil H, Deutsch R, Fritz LC. T-lymphocyte subsets in acute illness. Crit Care Med 1995;23(10):1680-1685. https://doi.org/10.1097/00003246-199510000-00012 [ Links ]
37. Amico KR, Konkle-Parker DJ, Cornman DH, et al. Reasons for ART non-adherence in the Deep South: Adherence needs of a sample of HIV-positive patients in Mississippi. AIDS Care 2007;19(10):1210-1218. https://doi.org/10.1080/09540120701426516 [ Links ]
38. Bukenya D, Mayanja BN, Nakamanya S, Muhumuza R, Seeley J. What causes non-adherence among some individuals on long term antiretroviral therapy? Experiences of individuals with poor viral suppression in Uganda. AIDS Res Ther 2019;16(1):1-9. https://doi.org/10.1186/s12981-018-0214-y [ Links ]
39. Shubber Z, Mills EJ, Nachega JB, et al. Patient-reported barriers to adherence to antiretroviral therapy: A systematic review and meta-analysis. PLoS Med 2016;13(11):e1002183. https://doi.org/10.1371/journal.pmed.1002183 [ Links ]
 Correspondence:
Correspondence:
A E Laher
abdullahlaher@msn.com
Accepted 22 February 2021


{kind=link}
{kind=link}