










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.111 no.7 Pretoria Jul. 2021
http://dx.doi.org/10.7196/samj.2021.v111i7.15058
RESEARCH
Thoughts of self-harm in early and late pregnancy in urban South Africa: Investigating prevalence, predictors and screening options
S RedingerI, II; R M PearsonIII, IV; B HouleV, VI, VII; S A NorrisVIII, IX; T J RochatX, XI
IBOccTher; SAMRC/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics and Child Health, Faculty of Health Sciences., University of the Witwatersrand, Johannesburg, South Africa
IIBOccTher; DSI-NRF Centre of Excellence in Human Development, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIPhD; SAMRC/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics and Child Health, Faculty of Health Sciences., University of the Witwatersrand, Johannesburg, South Africa
IVPhD; Centre for Academic Mental Health, Population Health Sciences, University of Bristol, Bristol, United Kingdom
VPhD; School of Demography, College of Arts and Social Sciences, The Australian National University, Canberra, Australia
VIPhD; MRC/Wits Rural Public Health and Health Transitions Research Unit (Agincourt), School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIIPhD; CU Population Center, Institute of Behavioral Science, University of Colorado Boulder, Boulder, Colorado, USA
VIIIPhD; SAMRC/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics and Child Health, Faculty of Health Sciences., University of the Witwatersrand, Johannesburg, South Africa
IXPhD; Global Health Research Institute, School of Health and Human Development, Faculty of Medicine, University of Southampton, Southampton, UK
XPhD; SAMRC/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics and Child Health, Faculty of Health Sciences., University of the Witwatersrand, Johannesburg, South Africa
XIPhD; DSI-NRF Centre of Excellence in Human Development, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Thoughts of self-harm (TSH) are an important marker of mental health risk, and risk for attempted and completed suicide. While there is increasing attention being paid to mental health problems in pregnancy in South Africa (SA), TSH have received less attention despite some cross-sectional studies suggesting that prevalence maybe high (12 - 39%). There is a dearth of longitudinal research to inform prevention and treatment
OBJECTIVES: To examine the rates of TSH across pregnancy in a longitudinal SA cohort and to investigate factors associated with the onset and persistence of TSH, as well as the relationship between TSH, depression and/or anxiety
METHODS: Women were enrolled in a prospective pregnancy cohort (S1000) in Soweto, SA between 2014 and 2016, and assessed using validated screening measures (Edinburgh Postnatal Depression Scale (EPDS) and State Trait Anxiety Index short form) in early and later pregnancy. Data were available for 649 women. TSH were determined using EPDS item 10. Logistic regression and bifactor models were used to determine factors associated with TSH across pregnancy
RESULTS: Of the 649 women, 18% reported TSH at some stage during their pregnancy. Prevalence of TSH was slightly higher in early pregnancy (12.5%) than later in pregnancy (11.6%). TSH were associated with a history of mental illness (adjusted odds ratio (aOR) 4.17; 95% confidence interval (CI) 1.3 - 13.7; p=0.020), concurrent depression (aOR 4.8; 95%CI 2.7 - 8.6; p<0.001); marital stress (aOR 1.74; 95% CI 1.0 - 3.0; p=0.040); and practical support (aOR 0.43; 95% CI 0.2 - 1.0; p=0.040) using a multivariate logistic regression. Bifactor analysis examining depression and anxiety scales showed that TSH contributed the highest variance to a shared depression and anxiety factor in early pregnancy. Logistic regressions showed that early depression was a strong predictor of later reports of TSH
CONCLUSIONS: The present study shows that the risk of TSH during pregnancy is relatively common, and starts early during pregnancy. Screening approaches could be simplified to encourage healthcare practitioners working in busy and over-burdened public healthcare settings to engage in identifying at-risk women. Efforts in improving early identification of mental health risk in pregnancy should be matched with strengthening of current treatment and referral options. Since practical support and a good marital relationship reduce the risk of TSH, these may be important avenues of focus for designing interventions
Young women and adolescent girls are particularly vulnerable to self-harm.[1] While many of these women might be mothers, or at least of child-bearing age, there is very little research on thoughts of self-harm (TSH) during the perinatal period.[2] Most research has been cross-sectional and limited to the postnatal period.[2] The few studies in South Africa (SA) that have investigated TSH and suicidal ideation during pregnancy have found prevalence of between 12% and 39%, which is double the rates found in developed countries.[3] SA also has high rates of antenatal mood disorders,[4,5] which have been shown to be a common risk factor for TSH.[3,6]
Despite evidence of risk during pregnancy, there are few routine screening programmes to identify TSH or suicidal ideation for pregnant women in developing countries. Both TSH and suicidal ideation are known antecedents of suicide attempts,[7] suggesting that early detection and prevention of TSH would have significant public health benefit. While the justification for early detection may be compelling, resistance to the introduction of time-intensive screening procedures in an already over-burdened public healthcare system is likely to be high. Developing our understanding of how to efficiently detect and evaluate risk for TSH is central to reducing barriers to early detection, and to focus limited prevention efforts where and when they are most needed.
We used longitudinal data from an urban cohort of pregnant women in Soweto, SA to investigate TSH in both early and late pregnancy. We report on prevalence, onset and duration of TSH, exploring both individual and contextual factors that are associated with TSH. We also investigated the relationship between TSR depression and anxiety, and make recommendations for approaches to, and timing of, screening efforts in low-resource settings.
Methods
Setting
The study was nested within a large pregnancy cohort study -the Soweto First 1000 Days Study (S1000) that is based at the Developmental Pathways for Health Research Unit (DPHRU) in Johannesburg, SA. The overall aim of the S1000 cohort was to investigate the associations between multiple maternal factors during pregnancy (including health and nutrition) and fetal and infant outcomes.
Participants
Pregnant women were enrolled into the study from the Fetal Medicine Unit at Chris Hani Baragwanath Academic Hospital (CHBAH) between 2014 and 2016. Inclusion criteria for S1000 were as follows: resident of Soweto, <20 weeks gestational age at recruitment, non-epileptic, non-diabetic, 18 years or older and pregnant with a singleton and naturally conceived pregnancy. Women were followed through pregnancy and up until their child's second birthday with data being collected at 14 timepoints during this period. This present study reports on data collected at two timepoints during the pregnancy period only (T1 - first trimester and T2 - late second trimester). These timepoints were study-specific and not necessarily linked to routine antenatal appointments.
Any participant reporting TSH during an assessment was referred to a senior professional nurse (with mental health training) at DPHRU for counselling. This nurse also facilitated a referral to mental health support services at CHBAH, and made follow-up calls to ensure that the participant was receiving these services.
All women provided written informed consent prior to their inclusion in the pregnancy component of the study (Soweto Fetal Growth Study; SFGS). Ethical approval was obtained from the University of the Witwatersrand's Research Ethics Committee (Medical) for data collection (ref. no. M120524) and data analysis (ref. no. M160670 and M180949).
Measures
Probable depression, anxiety and TSH were collected at both timepoints during pregnancy using validated psychometric scales.
Depression
The Edinburgh Postnatal Depression Scale (EPDS)[8] is a well validated 10-item screening tool for perinatal depression, which has shown good internal consistency and scale reliability in this cohort (Cronbach 0.80)[9] and in other studies in SA.[10,1l] Items are scored on a severity scale of 0 to 3 and summed for a total score of 30.
Anxiety
The State Anxiety Inventory short form (STAI-6) is a 6-item version of the 20-item Spielberger State-Trait Anxiety Inventory Index, which has shown good internal consistency, reliability and validity when correlated with the original scale.[12,13] Items are scored on a severity scale of 1 to 4 and summed for a total score of 24.
Thoughts of self-harm
Using an approach common in the literature,[14] reports of TSH were identified using item 10 of the EPDS, which states that 'The thought of harming myself has occurred to me'. Respondents self-reported TSH in the preceding 7 days on a Likert scale scoring 0 (never), 1 (hardly ever), 2 (sometimes) or 3 (quite often).
Data analysis
Analysis was performed in STATA, version 15 (StataCorp., USA) and MPlus version 8.3 (Statmodel, USA).
Consistent with previous analyses of this cohort,[4,9] the baseline covariates included in this analysis were selected a priori based on theoretical evidence.[15,17] Baseline individual and contextual covariates included maternal age, relationship status, pregnancy intention, education, asset ownership, health status, social support (practical and emotional) and social stressors (partner, family, economic and societal). Differences between baseline characteristics of women with and without TSH were determined using non-parametric tests (χ2, Wilcoxon rank-sum).
Probable depression was identified using a cut-off of > 3/30 on the EPDS.[18] Using the same approach as authors of the original full length STAI (>40/80),[12] probable anxiety was determined using the midpoint (>12/24) of the short form scale as a cut-off.
The TSH outcome variable for use in the logistic regressions and MPlus models was constructed from EPDS item 10. Responses of never' and 'hardly ever' were coded as 0, indicating 'no thoughts of self-harm', and responses of 'sometimes' and 'yes, quite often' as 1, denoting 'thoughts of self-harm present'. This dichotomous variable was used to calculate the presence or absence (prevalence) at each timepoint. Additionally, a variable describing the presence or absence of TSH across the pregnancy was created: 0 = no TSH at any point during pregnancy ('thoughts of self-harm never'); 1 = TSH at either Tl or T2, or both Tl and T2 ('thoughts of self-harm ever').
Logistic regression was used to determine the strength of associations between TSH ever' and baseline covariates (including Tl depression and anxiety) - with women who 'never' reported TSH as the reference group.
To explore the relationship between TSH and symptoms of depression and anxiety, we used confirmatory factor analysis (CFA) in MPlus to develop latent factors and logistic regression in STATA to explore associations. Firstly, the individual items of the EPDS and the STAI scales were organised into specific depression and anxiety factors. Then, given the strong evidence of depression and anxiety being highly comorbid and sharing characteristics,[9] we also created a shared depression/anxiety factor. In creating the shared factor each item of both the EPDS and STAI contributed variance to the unique depression and anxiety factors previously created, as well as contributing to the shared depression/anxiety factor. We then used the three factors to test model fit for the individual depression, anxiety factors and the shared depression/anxiety factor. For the CFA models, model fit was evaluated using root mean square error of approximation (RMSEA), comparative fit index (CFI) and Tucker-Lewis index (TLI). RMSEA is an absolute measure of fit adjusted for model complexity (values closer to zero indicate good fit), using an upper limit of <0.06 to indicate good fit. As CFI and TLI are measures of fit compared to the null with no correlations, when interpreting these indices we used the values >0.90 to indicate good fit.[19]
We explored the relationship between these factors and later TSH in a bifactor model using the depression, anxiety and shared factors as independent variables and TSH ever' as a dependent variable. Because CFA latent variables use individual items to contribute to variance, and given that the TSH variable was created using EPDS 10, for this particular analysis the depression factor was created without EPDS item 10. We could not explore the association between early TSH (as an independent variable) on later depression or anxiety as dependent variables in MPlus because TSH was created as a dichotomous variable and therefore could not be used as an independent variable in MPlus. Instead, to explore the association between reporting early TSH (Tl) and later TSH and mental health problems (TSH, depression or anxiety at T2), we used logistic regression analysis in STATA.
Results
Description of sample
Of the 1 055 women enrolled in the S1000 study, 649 had psychological data at both timepoints and were included in this analysis (Fig. 1). Women who did not have complete psychological data at both timepoints were excluded from the analysis. When comparing prevalence of TSH between women with data only at Tl or T2 with those who had data at both timepoints, we found no significant difference in rates using a χ2- test. At Tl, the rate of TSH was 12.5% among the included women and 11.4% (p=0.646) in excluded women. At T2, there was no significant difference (p=0.297) in the rates of TSH between those who were excluded (7.0%) and those who were included (11.6%). Previous sensitivity analysis[9] also demonstrated little to no difference in sociodemographic variables (a difference of 0.3 on an 11-point asset score) between those with complete data and those with incomplete data (i.e., data at only one timepoint). Sample characteristics are shown in Table 1. Women with TSH in pregnancy tended to be younger, single, pregnant with their first child, had a lower asset score and fewer years of education.

Prevalence of thoughts of self-harm
Prevalence of TSH was slightly higher in early pregnancy compared with later pregnancy. Less than a quarter of women (18.2%; )1=118) had TSH at some stage during pregnancy (either Tl or T2, or both Tl and T2), while 5.9% (n=39) of women reported TSH at both timepoints. Of the women who had TSH ever, 84.7% (n=100) had TSH alongside either depression or anxiety or both, while 15.3% (n=18) of women had TSH without either depression or anxiety being present.
Multivariate logistic regression model
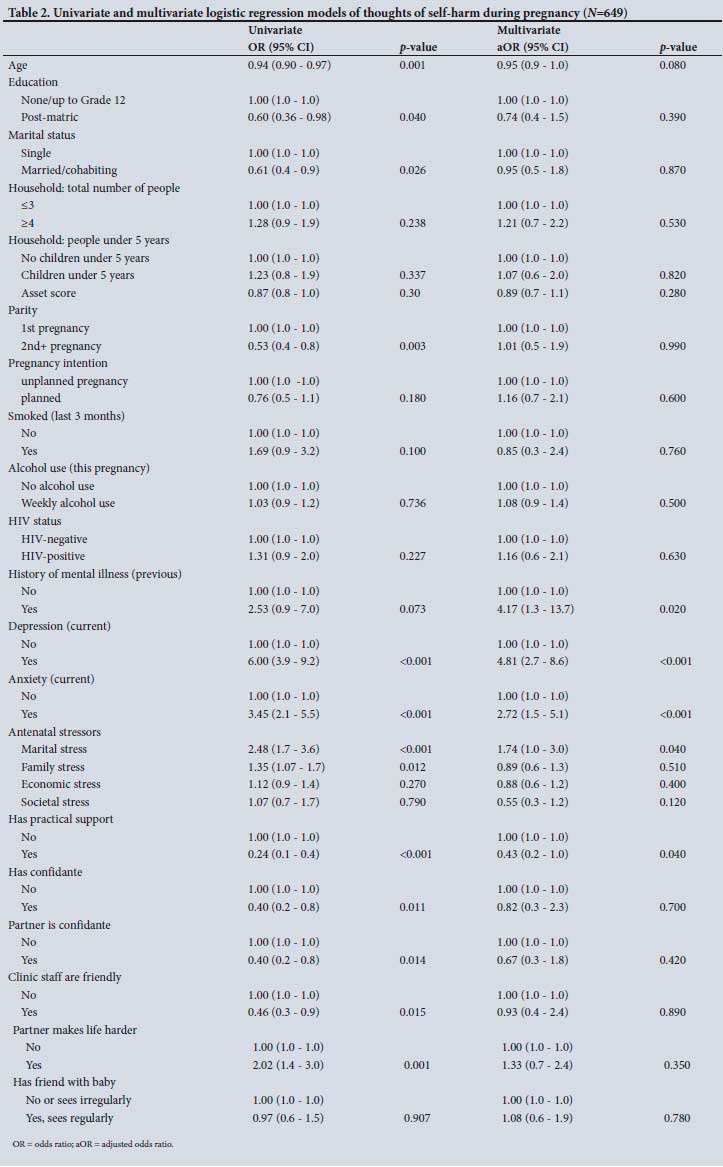
In the multivariate logistic regression model (Table 2), depression (adjusted odds ratio (aOR) 4.81; 95% confidence interval (CI) 2.7 - 8.6; p<0.001), anxiety (aOR 2.72; 95% CI 1.5 - 5.1; p<0.001) and a history of mental illness (aOR 4.17; 95% CI 1.3 - 13.7; p=0.020) prior to pregnancy were significantly associated with higher odds of TSH at some point in the pregnancy. Those reporting marital stress had higher odds of reporting TSH (aOR 1.74; 95% CI 1.0 - 3.0; p=0.040), while having practical support was associated with reduced odds of TSH (aOR 0.43; 95%CI 0.2 - 1.0; p=0.040).
Confirmatory factor analysis
Using the observed depression and anxiety scale items, both a unifactor and a bifactor model were fitted in MPlus to examine the existence of a general latent factor for depression and anxiety (Fig. 2). The unifactor models at both timepoints had poor fit - Tl: RMSEA (0.071; 90% CI 0.065 -0.078); CFI (0.838) and TFI (0.812); and T2: RMSEA (0.081; 90% CI 0.075 - 0.088); CFI (0.81) and TFI (0.78). At both timepoints, the bifactor model with the general shared factor had the best model fit at Tl (RMSEA (0.056; 90% CI 0.048 - 0.063); CFI (0.92) and TFI (0.89)) and T2 (RMSEA (0.066 90% CI 0.058 - 0.073); CFI (0.90) and TFI (0.86)).

When examining the association of early (Tl) depression, anxiety and the shared factor on later TSH, the largest association was with the shared factor (standardised estimate 0.468; standard error (SE) 0.065; p<0.001). There was no association between the unique anxiety factor and later TSH (standardised estimate 0.100; SE 0.066; p=0.129); however, depression alone was associated with TSH (standardised estimate 0.393; SE 0.071; p<0.001).
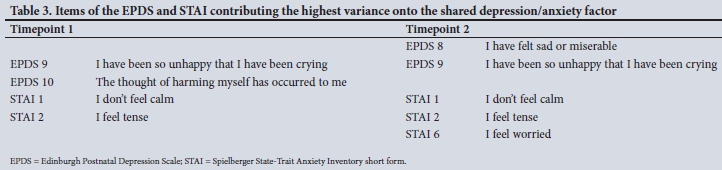
Table 3 shows the EPDS and STAI items contributing the highest variance to the shared factor at each timepoint. TSH was one of these items at Tl, but not at T2. Items common to both timepoints were EPDS item 9 (I have been so unhappy that I have been crying) and STAI items 1 (I feel calm, reversed scored) and 2 (I feel tense).
In terms of the impact of early TSH on later TSH, depression and anxiety, and TSH at Tl were strongly associated with TSH at T2 (OR 12.7; 95% CI 7.3 - 22.0; p<0.001); however, this effect was attenuated when controlling for depression at Tl (aOR 9.9; 95% CI 5.3 - 18.2; p<0.001). Early TSH was not associated with later depression (aOR 1.33; 95% CI 0.7 - 2.5; p=0.357) or anxiety (aOR 1.66; 95% CI 0.9 - 3.0; p=0.095) when controlling for later TSH.
Discussion
We determined the prevalence of TSH to be 18% in this present study, which is similar to other studies in SA,[16,17,20,21] and confirms that TSH are a significant public health concern. To the best of our knowledge, this is the first study in SA to demonstrate that TSH are present as early as the first trimester of pregnancy and that prevalence is slightly higher in early pregnancy as compared with later in pregnancy. Similar to other studies, we found that TSH are frequently reported in the context of concurrent depression, and that a history of mental illness is strongly associated with TSH during pregnancy,[16,20,21] TSH are more likely among women with marital stress, and less likely among those with good support. Lastly, we show that a combination of scale items on depressive and anxious symptoms best identifies women who endorse the TSH item in late pregnancy.
While suicidal risk among pregnant women is still largely under-researched in SA, there is growing evidence that risk for TSH is substantial, potentially double that reported in studies from developed countries.[16,22] Previously, cross-sectional studies in urban SA reported rates of 12, 18 and 19.8%,[16,20,21] while prevalence rates of up to 39% were reported in rural populations (with concurrent HIV).[17,24] Using repeated measures of TSH, depression and anxiety, we are able to demonstrate that TSH starts early, remain high in pregnancy, and that early TSH increases the odds of later TSH, especially in the context of depression. Previous cross-sectional studies reporting only on TSH in late pregnancy may have underestimated the extent of antenatal risk.
The public health justification for regular, routine mental health screening starting early in pregnancy in SA is therefore compelling, and ignoring the early warning signals could have far reaching consequences. Beyond the risk of TSH alone, is the risk of these progressing to suicide attempts, or in rare but tragic cases, completed suicide. A nationally representative study of adults in SA has shown that half of suicide attempts occur within a year of the onset of reporting suicide ideation.[24] Furthermore, suicide is a leading cause of death during the first postnatal year,[25] and has devastating effects not only for the expectant or new mother, her fetus or newborn, but also her partner, other children and family[26]
Regardless of this strong justification for supporting early screening, finding a balance between the need to screen and detect risk while limiting public healthcare burden, will likely be key to the acceptability and feasibility of increased screening in public healthcare clinical settings. Some research in SA has already advocated for ultra-short screening in primary healthcare settings,[27] and while we provide support for those calls, our findings suggests that focusing only on depressive screening items may have limitations. The results of the logistic regression models show that depression and anxiety are both strongly associated with later TSH. In the bifactor models, we show that the shared factor (symptoms of both depression and anxiety) had the strongest association with TSH later in pregnancy. This suggests that a combination of screening questions about both depressive and anxious symptoms might best identify or predict later reports of TSH.
Enquiring from the first antenatal contact whether a pregnant women has been feeling tense and unable to calm herself, feeling so unhappy that she has been crying or has had thoughts of harming herself, may provide healthcare practitioners a simple and approachable way to enquiring about mental health, which is not overly technical. These short, gentle enquiries about emotional coping, alongside queries about support (both marital and otherwise) may help to reduce the stigma associated with mental health problems. It may also encourage greater disclosure by patients in healthcare provider interactions, which in turn could facilitate timely, efficient and targeted referrals. The potential to mitigate risk for at-risk individuals may outweigh the additional time burden of introducing these mental health related screening questions during antenatal consultations.
Identification of risk has no real benefit at a population level when treatment is not available, and therefore finding cost-efficient ways to not only identify, but also respond, is critical. In this cohort, all women reporting TSH at Tl received at least one study-supported counselling session, and were referred to routine mental healthcare services. Despite this, a significant proportion had a similar response at T2, with rates of TSH increasing later in pregnancy, suggesting that the intensity and content of existing interventions may need to be enhanced to respond to this high-risk population. When controlling for depression and anxiety, women reporting marital stress were almost twice as likely to have TSH as those without, and having practical support halved the odds of reporting TSH. Including partner and family-based support in mental health care services and interventions could enhance existing intervention approaches and highlights the important role a multidisciplinary team (including social workers and psychologists) can play in delivering pregnancy care.
Study strengths and limitations
The strengths of this study include its longitudinal design and that it measures both depression and anxiety alongside rich contextual data. Limitations include that while we report on TSH during pregnancy, we do not have any additional information on the extent of suicidal ideation, for example whether women have intent and plans, or any history of suicidal attempts. However, in another study in SA, item 10 on the EPDS 'the thought of harming myself has occurred to me was found to have good sensitivity of 77% (CI 57 - 89) and excellent specificity of 92% (CI 83 - 96) for detecting suicide ideation when compared with a clinical interview[28] Additionally, in the present study, the approach to defining TSH was more conservative than previous studies in SA, some of which included a response of 'hardly ever' as indicating TSH,[23,29] suggesting this research has provided a sound estimate of potential risk. Even though a third of women in the full S1000 cohort did not have mental health data at both timepoints, large numbers of women were retained in the study at timepoint 2. providing us with sufficient data to establish that it was unlikely that systematic bias was introduced by having missing data. There is growing evidence of the negative impact of internet and social media use on self-harm and suicidal behaviours;[30] however, most of this research is focused on children and adolescents, including in SA.[31] While we did not measure the impact of internet and social media use on TSH in this present study, we feel that it should be explored in future studies of mental health in SA
Conclusions
Given that TSH is a robust predictor for attempted suicide,[3] findings from the present study call for attention to the need for early detection to identify the subset of women requiring urgent evaluation and care, as early as possible in pregnancy. In low-resource public healthcare settings, the reporting of TSH by patients immediately places a responsibility on healthcare providers to ensure the safety and care of the patient. In this regard, the services of public healthcare psychiatric nurses, psychologists and social workers play a key role as do interventions delivered by lay counsellors or community healthcare workers, and a wide range of non-governmental services positioned to respond to mental health crises. Healthcare workers in perinatal settings could easily be trained in approachable, effective screening methods, but emergency response and referral protocols need to be developed within their institutions or communities to assist with case management. How this might be operationalised in tertiary v. decentralised primary healthcare institutions (where such human resources may be scarce) is less understood and warrants further investigation. Importantly, what this present study demonstrates is that not measuring or identifying risk of self-harm does not invalidate the likely presence of TSH. Taking a 'don't ask, don't tell' approach not only raises an ethical dilemma for healthcare practitioners, but may further stigmatise TSH among the 2 out of 10 pregnant women at high risk in their patient population.
Declaration. None.
Acknowledgements. The authors would like to thank the women who participated in this study. We would also like to acknowledge and thank the staff at the SAMRC/Wits Developmental Pathways for Health Research Unit for their involvement in the collection and curation of data.
Author contributions. SR, SAN and TJR conceptualised the study, analysed and interpreted the data and critically reviewed the manuscript. BH and RMP reviewed data analysis and interpreted the data and critically revised the manuscript.
Funding. S1000 was funded by the UK MRC/DfID African Research Leader Scheme, the Medical Research Council of South Africa and the Gates Foundation. SR is supported by the DSI-NRF Centre of Excellence in Human Development (University of Witwatersrand, South Africa) PhD Scholarship (D201900013). RMP is supported by a European Research Commission grant (grant ref: 758813 MHINT). SAN is supported by the DSI-NRF Centre of Excellence in Human Development. TJR is supported by a Wellcome Trust Intermediate Fellowship (211374/Z/18/Z). Opinions expressed and conclusions arrived at are those of the authors and are not necessarily to be attributed to the funders.
Conflicts of interest. None.
References
1. Quarshie EN, Waterman MG, House AO. Self-harm with suicidal and non-suicidai intent in young people in sub-Saharan Africa. A systematic review. BMC Psychiatry 2020;20:1-26. https://doi.org/10.1186/s12888-020-02587-z [ Links ]
2. Ayre K, Dutta R, Howard LM. Perinatal self-harm. An overlooked public health issue. Lancet Public Health 2019;4(3):e125. https://doi.org/10.1016/s2468-2667(19)30020-9 [ Links ]
3. Lindahl V, Pearson JL, Colpe L. Prevalence of suicidality during pregnancy and the postpartum. Arch Womens Ment Health 2005;8(2):77-87. https://doi.org/10.1007/s00737-005-0080-1 [ Links ]
4. Redinger S, Nords SA, Pearson RM, Richter L, Rochat T. First trimester antenatal depression and anxiety. Prevalence and associated factors in an urban population in Soweto, South Africa. J Dev Orig Health Dis 2018;9(1):30-40. https://doi.org/10.1017/s204017441700071x [ Links ]
5. Baron EC, Hanlon C, Mali S, et ai. Maternal mental health in primary care in five low- and middle-income countries. A situational analysis. BMC Health Serv Res 2016;16:53. https://doi.org/10.1186/s12913-016-1291-z [ Links ]
6. Gavin AR, Tabb KM, Melville JL, Guo Y, Katon W. Prevalence and correlates of suicidal ideation during pregnancy. Arch Womens Ment Health 2011;14(3):239-246. https://doi.org/10.1007/s00737-011-0207-5 [ Links ]
7. Ruiz P. Global epidemiology of suicide. In. Nemeroff CB, Ruiz P, Koslow SH, eds. A Concise Guide to Understanding Suicide. Epidemiology, Pathophysiology and Prevention. Cambridge: Cambridge University Press, 2014:13-16. https://doi.org/10.1017/cbo9781139519502.004 [ Links ]
8. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry 1987;150(6):782-786. https://doi.org/10.1192/bjp.150.6.782 [ Links ]
9. Redinger S, Pearson RM, Houle B, Norris SA, Rochat TJ. Antenatal depression and anxiety across pregnancy in urban South Africa. J Affect Disord 2020;277:296-305. https://doi.org/10.1016/j.jad.2020.08.010 [ Links ]
10. Tsai AC, Scott JA, Hung KJ, et al. Reliability and validity of instruments for assessing perinatal depression in African settings. Systematic review and meta-analysis. PLoS ONE 2013;8(12):e82521. https://doi.org/10.1371/journal.pone.0082521 [ Links ]
11. Rochat TJ, Tomlinson M, Barnighausen T, Newell M-L, Stein A. The prevalence and clinical presentation of antenatal depression in rural South Africa. J Affect Disord 2011;135(1):362-373. https://doi.org/10.1016/j.jad.2011.08.011 [ Links ]
12. Marteau TM, Bekker H. The development of a six-item short-form of the state scale of the Spielberger State - Trait Anxiety Inventory (STAI). Br J Clin Psychol 1992;31(3):301-306. https://doi.org/10.1111/j.2044-8260.1992.tb00997.x [ Links ]
13. Tluczek A, Henriques JB, Brown RL. Support for the reliability and validity of a six-item state anxiety scale derived from the State-Trait Anxiety Inventory J Nurs Meas 2009;17(1):19-28. https://doi.org/10.1891/1061-3749.17.1.19 [ Links ]
14. Howard LM, Flach C, Mehay A, Sharp D, Tylee A. The prevalence of suicidal ideation identified by the Edinburgh Postnatal Depression Scale in postpartum women in primary care. Findings from the RESPOND trial. BMC Preg Childbirth 2011;11(1):57. https://doi.org/10.1186/1471-2393-11-57 [ Links ]
15. Gelaye B, Kajeepeta S, Williams MA. Suicidal ideation in pregnancy. An epidemiologic review. Arch Womens Ment Health 2016;19(5):741-751. https://doi.org/10.1007/s00737-016-0646-0 [ Links ]
16. Onah MN, Field S, Bantjes J, Honikman S. Perinatal suicidal ideation and behaviour. Psychiatry and adversity. Arch Womens Ment Health 2017;20(2):321-331. https://doi.org/10.1007/s00737-016-0706-5 [ Links ]
17. Rochat TJ, Bland RM, Tomlinson M, Stein A. Suicide ideation, depression and HIV among pregnant women in rural South Africa. Health 2013;5(3A):650-661. https://doi.org/10.4236/health.2013.53a086 [ Links ]
18. ShresthaSD, Pradhan R, Tran TD, Gualano RC, Fisher JRW Reliability and validity of the Edinburgh Postnatal Depression Scale (EPDS) for detecting perinatal common mental disorders (PCMDs) among women in low-and lower-middle-income countries. A systematic review. BMC Pregnancy Childbirth 2016;16(1):1-19. https://doi.org/10.1186/sl2884-016-0859-2 [ Links ]
19. Hooper D, Coughlan J, Mullen MR. Evaluating model fit. A synthesis of the structural equation modelling literature. In. Brown A, editor. 7th European Conference on Research Methodology for Business and Management Studies. London. Academic Publishing Limited, 2008:195-200. [ Links ]
20. Garman EC, Cois A, Schneider M, Lund C. Association between perinatal depressive symptoms and suicidal risk among low-income South African women. A longitudinal study. Soc Psychiatry Psychiatr Epidemiol 2019;54(10):1219-1230. https://doi.org/10.1007/s00127-019-01730-w [ Links ]
21. Van Heyningen T, Myer L, Onah M, Tomlinson M, Field S, Honikman S. Antenatal depression and adversity in urban South Africa. J Affect Disord 2016;203:121-129. https://doi.org/10.1016/j.jad.2016.05.052 [ Links ]
22. Gordon H, Nath S, Treviliion K, et al. Self-harm, self-harm ideation, and mother-infant interactions. A prospective cohort study. J Clin Psychiatry 2019;80(5). https://doi.org/10.4088/JCP.18m12708. [ Links ]
23. Rodriguez VJ, Mandell LN, Babayigit S, Manohar RR, Weiss SM, Jones DL. Correlates of suicidal ideation during pregnancy and postpartum among women living with HIV in rural South Africa. AIDS Behav 2018;22(10):3188-3197. https://doi.org/10.1007/s10461-018-2153-y [ Links ]
24. Joe S, Stein DJ, Seedat S, Herman A, Williams DR. Non-fatal suicidal behavior among South Africans. Soc Psychiatry Psychiatr Epidemiol 2008;43(6):454-461. https://doi.org/10.1007/s00127-008-0348-7 [ Links ]
25. Oates M. Perinatal psychiatric disorders. A leading cause of maternal morbidity and mortality. Br Med Bull 2003;67(1):219-229. https://doi.org/10.1093/bmb/ldg011 [ Links ]
26. Ayre K, Gordon HG, Dutta R, Hodsoll J, Howard LM. The prevalence and correlates of self-harm in the perinatal period. A systematic review. J Clin Psychiatry 2019;81(1). https://doi.org/10.4088/jcp.19r12773 [ Links ]
27. Bhana A, Mntambo N, Gigaba S, et al. Validation of a brief mental health screening tool for common mental disorders in primary healthcare. S Afr Med J 2019;109(4):278-283. https://doi.org/10.7196/samj.2019.v109i4.13664 [ Links ]
28. Rochat TJ, Tomlinson M, Newell M-L, Stein A. Detection of antenatal depression in rural HIV-affected populations with short and ultrashort versions of the Edinburgh Postnatal Depression Scale (EPDS). Arch Womens Ment Health 2013;16(5):401-410. https://doi.org/10.1007/s00737-013-0353-z [ Links ]
29. Rodriguez VJ, Matseke G, Cook R, et al. Infant development and pre-and post-partum depression in rural South African HIV-infected women. AIDS Behav 2018;22(6):1766-1774. https://doi.org/10.1007/s10461-017-1925-0 [ Links ]
30. Mars B, Heron J, Biddle L, et al. Exposure to, and searching for, information about suicide and self-harm on the internet. Prevalence and predictors in a population based cohort of young adults. J Affect Disord 2015;185:239-245. https://doi.org/10.1016/j.jad.2015.06.001 [ Links ]
31. Marchant A, Hawton K, Stewart A, et al. A systematic review of the relationship between internet use, self-harm and suicidal behaviour in young people. The good, the bad and the unknown. PLoS ONE 2017;12(8):e0181722. https://doi.org/10.1371/journal.pone.0181722 [ Links ]
 Correspondence:
Correspondence:
S Redinger
stephanie.redinger@wits.ac.za
Accepted 18 January 2021


{kind=link}
{kind=link}
{kind=link}