










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.111 n.6 Pretoria Jun. 2021
http://dx.doi.org/10.7196/SAMJ.2021.v111i6.15272
RESEARCH
Survival of South African children with cerebral palsy
J C BrooksI; R D D CampbellII; G A WhittakerIII
IPhD, MPH; Life Expectancy Project, California, USA
IIMB ChB; Nurture Health, South Africa
IIIBEconSc, FSA, FASSA; Algorithm Consultants & Actuaries, Sandton, South Africa
ABSTRACT
BACKGROUND. The South African (SA) public healthcare sector has experienced a surge in birth injury claims in recent years, particularly in respect of cerebral palsy (CP). The lump sum settlements in these matters are a function of the expected survival curve of the individual concerned. It is known from international studies that the life expectancy of children with CP is shorter than that of the general population, and depends on the pattern and severity of their disabilities. However, empirical estimates of survival for children with CP in SA are not available. Objectives. To construct survival curves according to the pattern of gross motor skills for CP children in SA and compare these with international studies.
METHODS. We collected data on mortality and functional status for 339 CP children on whose behalf claims for medical negligence had been instituted. Motor disabilities were classified according to the five-level Gross Motor Function Classification System (GMFCS). Children who were unable to walk unaided were further classified according to more basic motor skills, including the ability to lift their heads or chests in the prone position, rolling and sitting. Mortality rates were calculated and survival curves were estimated using the Kaplan-Meier method. Results. No deaths were observed among 119 children in GMFCS levels I - IV. Among the 220 children in GMFCS V, there were 20 observed deaths. The proportions surviving to ages 10 and 15 years were 85% (standard error (SE) 5%) and 55% (SE 11%), respectively. The former is comparable to what has been reported for children in California and Sweden, but the survival to age 15 is lower. Among 82 children who could not lift their heads in the prone position, there were 11 observed deaths for a mortality rate of 48.5 (95% confidence interval (CI) 24.2 - 86.9) deaths per 1 000 person-years. Among 72 children who could lift their heads but not their chests, there were 6 observed deaths for a mortality rate of 33.5 (95% CI 12.3 - 73.0) deaths per 1 000 person-years. These mortality rates are 22% and 15% higher than the corresponding figures documented for children with comparable abilities and disabilities in California.
CONCLUSIONS. Life expectancy of children with CP in SA is lower than that of children with comparably severe disabilities in high-income countries.
The contingent liability for claims for medical negligence against provincial health departments increased from ZAR28.61 billion for the year ending 31 March 2015 to an estimated ZAR104.49 billion for the year ending 31 March 2019.[1] Over the 5 years from 1 April 2014 to 31 March 2019, total claims payments made by provincial health departments amounted to an estimated ZAR6.29 billion.[1]
Estimates of the contribution of cerebral palsy (CP) claims to the abovementioned totals in South Africa (SA) are unknown, but on the basis of a substantial body of Superior Court rulings[2-6] they are likely to be the main contributing factor. In the UK, it has been estimated that about half of the cost of litigation in the National Health Service relates to claims for CP.[7]
The expected lifetime cost of care for persons with severe CP is substantial, and the likely duration of survival is an essential determinant of litigation awards.[8]
Note. It is not the intention of this article to comment on the merits of the once-and-for-all rule or lump sum settlements. There have, however, been numerous developments in this regard and various alternative methods of compensation are covered by the South African Law Reform Commission issue paper on medicolegal claims,[9] the matter of MEC for Health and Social Development, Gauteng v DZ obo WZ,[5] the State Liability Amendment Bill,[10] and the matter of MSM obo KBM v MEC for Health, Gauteng.[6]
There is a large body of published research on survival of children with CP in high-income countries including Australia,[11] Canada,[12] Japan,[13] Sweden,[14] the UK[7] and the USA (California)[15,16] Survival of children with CP in these countries proves to be remarkably similar. There are no recent published data on survival of children with CP in SA. The normal general population life expectancy in SA is lower than that in high-income countries, and it is usually assumed that life expectancy of children with CP in SA is lower than that documented in high-income countries.
In SA litigation, it has become common to compute lifetime cost-of-care awards for children with CP on the assumption that proportionate reductions from normal life expectancy indicated by published studies in high-income countries can be applied to the normal SA general population figure. While this approach has intuitive appeal, its validity has not yet been confirmed with empirical data.
Objectives
To construct survival curves according to the pattern of gross motor skills for CP children in SA and compare these with international studies.
The present study appears to be the first to report on and examine empirical data on patterns of gross motor abilities and disabilities and survival among SA children with CP. The practical goals of this research are twofold. The first is to provide a framework for the development of a more comprehensive national CP registry, modelled on those in high-income countries, that systematically links functional assessments in childhood with long-term health outcomes. The second is to serve the immediate need for empirical data to guide the determination of fair cost-of-care awards in SA litigation settings.
Methods
There is no standardised system for monitoring the prevalence of CP in SA. For the present study, data were collected on individuals with CP in cases where it was known that litigation proceedings had been instituted.
Data collected included date of birth, gender, mode of feeding, Gross Motor Function Classification System (GMFCS) level (I - V), and more basic gross motor abilities and disabilities corresponding to the stratification reported in Table II of Brooks et al [15] in accordance with criteria for the relevant items in the Client Development Evaluation Repor[17] The latter comparison groups included children who were: (i) unable to lift head or chest when lying in the prone position; (ii) able to lift head but not chest in the prone position; (iii) able to lift head and chest or roll side to side or front to back; (iv) able to roll fully, but not to walk unaided; and (v) able to walk unaided.
Gross motor abilities and disabilities in all cases were assessed by a medical practitioner with a special interest in rehabilitation medicine (author RDDC) during the years 2009 - 2020. In 112 cases, children were also assessed independently by at least one other medical practitioner.
Vital status was tracked using SA identity numbers issued by the Department of Home Affairs identity verification system through the LexisNexis WinDeed system[18] It can take 3 - 5 weeks from the date of issuance of a death certificate for the Department of Home Affairs database to be updated. Follow-up times were computed from the date of assessment until death or, for those still alive, until the censoring date of 1 July 2020. The date 1 July 2020 was chosen because the identity verification system was accessed on 25 August 2020. The censor date therefore makes provision for the time lag between the date of death and the date of registration of the death, and for the time lag between the date of issuance of the death certificate and the capturing of the death on the Department of Home Affairs database.
Mortality rates were calculated by dividing the total number of deaths by the follow-up time (in person-years) observed during the study period. The mortality rate for children with severe CP was assumed to be constant throughout childhood, as indicated by the empirical results of Brooks et al[15,16] and others. Exact 95% confidence intervals (CIs) were computed assuming that the mortality rates followed a Poisson distribution. Age-specific survival probabilities (i.e. survival curves) were estimated and plotted using the Kaplan-Meier method, adjusted for both right-censoring and left-truncation of the survival times. Standard errors and CIs were computed using Greenwood's formula together with the complementary log-log transformation. Statistical analyses were conducted using Stata 16 (StataCorp, USA). Mortality rates and age-specific survival probabilities were compared with those reported in previously published studies of children with comparable patterns of gross motor disabilities.
Results
The sample comprised 339 children with CP (66% male), who collectively were observed for 948 person-years; 93.5% of the children were referred for functional assessment by plaintiff attorneys, and the remaining 6.5% by the State Attorney, the Medical Protection Society or private sector attorneys representing the Department of Health. The median (interquartile range) age at functional assessment was 6.3 (4.4 - 8.6) years. Among the 112 children who were examined by multiple medical practitioners, there was complete concordance with respect to the assessment of gross motor skills in 93% of cases. In 6% of cases, disagreement was minimal (limited to a single-level disparity between the allocated level of mobility). The gross motor skill classifications used in the present study were taken to be the majority view.
Characteristics of the study population are summarised in Table 1. Relatively few (17%) had mild CP (GMFCS I/II) and were able to walk unaided. The latter percentage is markedly lower than that recorded in the service-based register studied by Brooks et al.[1516] (34%) and in the population-based register studied by Reid et (56%). The majority of children in the present study (65%) had very severe CP (GMFCS V). Some 24% of children in the present study were unable to lift their heads, while only 7% of the Brooks cohort fell into this category.
There were 20 deaths, all of which were observed in the GMFCS V group. The overall mortality rate was 33.6 (95% Cl 20.5 - 51.9) per 1 000 person-years. The GMFCS survival curve is shown in Fig. 1, and age-specific survival probabilities are compared with those reported in various international studies in Table 2.
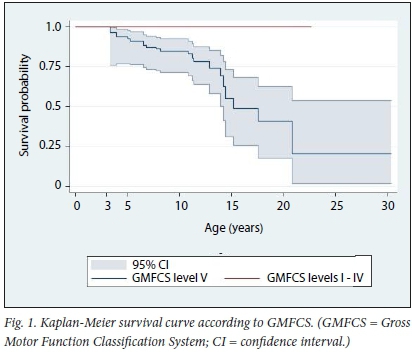
The median survival time for 3-year-olds was 12.2 additional years, to age 15.2 (90% CI 14.2 - 20.8); 85% (95% CI 77 - 98) survived to age 10, which was similar to that reported in the studies of Westbom et al.[14] and Brooks et al.[15,16] Survival to ages 15 and 20, 55% (95% CI 31 - 73) and 41% (95% CI 18 - 62), respectively, was lower than reported in these other studies.
As shown in Table 3, mortality rates for children who were unable to lift their heads in the prone position were 22% higher than those indicated by Brooks et al [15]For those who could lift their heads but not their chests, the mortality rates were 15% higher. As noted, these comparisons are based on 11 and 6 observed deaths in the SA comparison groups and are therefore imprecise. Because there were only 2 other observed deaths in other comparison groups, we do not present the calculated relative risks here.
Discussion
This is the first report on systematically collected data on gross motor function and survival of SA children with CP. As expected, more severe motor disabilities were associated with poorer survival. Among children in GMFCS V, finer stratification in terms of more basic gross motor skills including head control and rolling were predictive of survival.
Survival of children with severe CP in SA is poorer than that in high-income countries. The probability of survival to age 10 years estimated in the present study was similar to those reported in studies from high-income countries, but our estimates of the probabilities of survival to older ages were lower. Averaged across age, mortality rates for persons with the most severe forms of CP in SA were -20% higher than those reported for persons with comparably severe disabilities in the USA.
It may be noted that the children studied here represent a select group who were involved in litigation. As noted, the proportion of children with very severe motor disabilities was much higher in the present study than has been documented in both population-based birth registers and service-based registers from high-income countries. It is possible that this reflects a general difference in the distribution of severity of disability in middle-income v. high-income countries, but it may also reflect differences between cases in SA that ultimately lead to litigation v. those that do not. There is no national registry or other standardised system for monitoring CP in SA, and the extent to which our results may apply more generally to SA children with CP (outside of litigation settings) is not yet clear.
By the nature of the data collection in the present study, our results are directly relevant to the estimation of life expectancy of SA children with CP who are involved in litigation. As noted, these indicate that mortality rates for children with very severe CP are -20% higher than those documented for children with comparably severe disabilities in the USA. This is broadly consistent with a 10 -15% reduction from the US-based life expectancy estimates. It is notable that the proportionate difference between the normal general population life expectancies in the two countries is also -10 - 15%, which adds empirical support for the proportionate approach to life expectancy estimation that has been used in SA litigation matters over the past decade.
Study limitations
The major limitation of the present study is the relatively small sample size. The data were collected from a medical practitioner who has examined hundreds of CP patients over a decade, but precision in the estimation of survival probabilities and mortality rates requires either follow-up of many more patients or much longer follow-up of the existing patients.
Recommendations for future research
Given the immediate needs associated with a growing number of CP litigation matters, there is a clear need for the Department of Health to create a centralised database for monitoring CP claimants against the public sector so as to accurately assess life expectancy. The methods described in this article can easily be extended to larger data sets and longer follow-up times. The growth of the database would require the co-operation of the Department of Health with the attorneys handling the litigation volumes. Information on gross motor skills should necessarily be included in the database, and ideally more extensive information on factors that are known to be associated with survival should also be collected. Following this, it may then be reasonable to investigate survival rates by province or level of service provision.
Conclusions
Mortality rates for SA children with very severe CP are ~20% higher than those for children with comparably severe disabilities in high-income countries. The development of a larger centralised database with information on children with CP in SA is needed to provide more precise empirical estimates of their survival.
Declaration. None.
Acknowledgements. The authors acknowledge the assistance of Dr Jennifer Winstead and Jennifer Hemsley in managing the database. Author contributions. JCB performed all statistical analyses. GAW checked all statistical analyses and wrote the article. RDDC assessed all subjects and maintained the database.
Funding. None.
Conflicts of interest. None.
References
1. Rispel LC, Shisana O, Dhai A, et al. Achieving high-quality and accountable universal health coverage in South Africa: A synopsis of the Lancet National Commission Report. In: Moeti T, Padarath A, eds. South African Health Review 2019. Durban: Health Systems Tïust, 2019. https://www.hst.org.za/publications/South%20African%20Health%20Reviews/06%20SAHR_2019_ Achieving%20a%20high%20quality%20health%20system.pdf (accessed 26 August 2020). [ Links ]
2. Singh v Ebrahim 2010 JDR 1431 (SCA)
3. AD and Another v MEC for Health and Social Development, Western Cape 2017 (5) SA 134 (WCC)
4. NK v MEC for Health, Gauteng 2018 (4) SA 454 (SCA)
5. MEC for Health and Social Development, Gauteng v DZ obo WZ 2018 (1) SA 335 (CC)
6. MSM obo KBM v MEC for Health, Gauteng 2020 (2) SA 567 (GJ)
7. Hutton JL, Pharoah PO. Life expectancy in severe cerebral palsy. Arch Dis Child 2006;91(3):254-258. https://doi.org/10.1136/adc.2005.075002 [ Links ]
8. Blair E, Langdon K, McIntyre S, Lawrence D, Watson L. Survival and mortality in cerebral palsy: Observations to the sixth decade from a data linkage study of a total population register and National Death Index. BMC Neurol 2019;19(1):111. https://doi.org/10.1186/s12883-019-1343-1 [ Links ]
9. South Africa. South African Law Reform Commission Issue Paper 33: Medico-Legal Claims. 2017. https://www.justice.gov.za/salrc/ipapers/ip33_prj141_Medico-legal.pdf (accessed 26 August 2020). [ Links ]
10. South Africa. State Liability Amendment Bill, No. B16-2018, 2018. https://www.parliament.gov.za/storage/app/media/Bills/2018/B16_2018_State_Liability_Amendment _Bill/B16_2018_State_ Liability_Amendment_Bill.pdf (accessed 26 August 2020). [ Links ]
11. Reid SM, Carlin JB, Reddihough DS. Survival of individuals with cerebral palsy born in Victoria, Australia, between 1970 and 2004. Dev Med Child Neurol 2012;54(4):353-360. https://doi.org/10.1111/j.1469-8749.2012.04218.x [ Links ]
12. Crichton JU, Mackinnon M, White CP. The life-expectancy of persons with cerebral palsy. Dev Med Child Neurol 1995;37(7):567-576. https://doi.org/10.1111/j.1469-8749.1995.tb12045.x [ Links ]
13. Touyama M, Touyama J, Ochiai Y, Toyokawa S, Kobayashi Y. Long-term survival of children with cerebral palsy in Okinawa, Japan. Dev Med Child Neurol 2013;55(5):459-463. https://doi.org/10.1111/j.1469-8749.2012.04429.x [ Links ]
14. Westbom L, Bergstrand L, Wagner P, Nordmark E. Survival at 19 years of age in a total population of children and young people with cerebral palsy. Dev Med Child Neurol 2011;53(9):808-814. https://doi.org/10.1111/j.1469-8749.2011.04027.x [ Links ]
15. Brooks JC, Strauss DJ, Shavelle RM, Tran LM, Rosenbloom L, Wu YW. Recent trends in cerebral palsy survival. Part II: individual survival prognosis. Dev Med Child Neurol 2014;56(11):1065-1071. https://doi.org/10.1111/dmcn.12519 [ Links ]
16. Brooks JC, Strauss DJ, Shavelle RM. Survival in children with severe cerebral palsy: A further international comparison. Dev Med Child Neurol 2012;54(4):383-384. https://doi.org/10.1111/j.1469-8749.2012.04236.x [ Links ]
17. California Department of Developmental Services. Client Development Evaluation Report. Sacramento, Calif.: DDS, 1986. [ Links ]
18. LexisNexis. WinD eed. https://search.windeed.co.za/HomeAffairsIDV (accessed 25 August 2020). [ Links ]
 Correspondence:
Correspondence:
G A Whittaker
gregory@algorithm-ca.com
Accepted 29 October 2020


{kind=link}
{kind=link}
{kind=link}