










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.111 no.3 Pretoria Mar. 2021
http://dx.doi.org/10.7196/samj.2021.v111i3.15119
RESEARCH
Rapid review of the effects of cloth and medical masks for preventing transmission of SARS-C6V-2 in community and household settings
T ChettyI, II; V RamokoloIII, IV; K ReesV; T KredoVI, VII; Y BalakrishnaVIII; C MathewsIX; N SiegfriedX
IMB ChB, FCPHM (SA), MMed, PhD; Health Systems Research Unit, South African Medical Research Council, Cape Town, South Africa
IIMB ChB, FCPHM (SA), MMed, PhD; HIV Prevention Research Unit, South African Medical Research Council, Cape Town, South Africa
IIIBSc (Hons), MPH, PhD; Health Systems Research Unit, South African Medical Research Council, Cape Town, South Africa
IVBSc (Hons), MPH, PhD; HIV Prevention Research Unit, South African Medical Research Council, Cape Town, South Africa
VMB BCh, FCPHM (SA); Department of Community Health, School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg., South Africa
VIMB ChB, MMed (Clin Pharm), PhD; Cochrane South Africa, South African Medical Research Council, Cape Town, South Africa
VIIMB ChB, MMed (Clin Pharm), PhD; Division of Clinical Pharmacology, Department of Medicine, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town South Africa
VIIIMSc; Biostatistics Unit, South African Medical Research Council, Durban, South Africa
IXBA, MSc, PhD; Health Systems Research Unit, South African Medical Research Council, Cape Town, South Africa
XMB ChB, MPH (Hons), FCPHM (SA), PhD; Health Systems Research Unit, South African Medical Research Council, Cape Town, South Africa
ABSTRACT
BACKGROUND: Evidence on mask use in the general population is needed to inform SARS-CoV-2 responses
OBJECTIVES: To assess the effectiveness of cloth and medical masks for preventing SARS-CoV-2 transmission in community settings
METHODS: Two rapid reviews were conducted searching three electronic databases (PubMed, Embase, Cochrane Library) and two clinical trials registries on 30 and 31 March 2020
RESULTS: We screened 821 records and assessed nine full-text articles for eligibility. One and seven RCTs were included for cloth and medical mask reviews, respectively. No SARS-CoV-2-specific RCTs and no cloth mask RCTs in community settings were identified. A single hospital-based RCT provided indirect evidence that, compared with medical masks, cloth masks probably increase clinical respiratory illnesses (relative risk (RR) 1.56; 95% confidence interval (CI) 0.98 - 2.49) and laboratory-confirmed respiratory virus infections (RR 1.54; 95% CI 0.88 - 2.70). Evidence for influenza-like illnesses (ILI) was uncertain (RR 13.00; 95% CI 1.69 - 100.03). Two RCTs provide low-certainty evidence that medical masks may make little to no difference to ILI infection risk versus no masks (RR 0.98; 95% CI 0.81 - 1.19) in the community setting. Five RCTs provide low-certainty evidence that medical masks may slightly reduce infection risk v. no masks (RR 0.81; 95% CI 0.55 - 1.20) in the household setting
CONCLUSIONS: Direct evidence for cloth and medical mask efficacy and effectiveness in the community is limited. Decision-making for mask use may consider other factors such as feasibility and SARS-CoV-2 transmission dynamics; however, well-designed comparative effectiveness studies are required
Severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) is spread from person to person, predominantly through respiratory droplets and contact with contaminated surfaces,[1] and possibly through airborne transmission.[2] Consequently, close contact with infected people should be avoided. Transmission risk may be mitigated by wearing personal protective equipment (PPE) such as face masks.
The pandemic has led to global shortages of PPE, including masks and respirators. Masks are critical to protecting healthcare workers from becoming infected and from infecting patients.[1] Masks have also been widely promoted for preventing transmission in community settings. This is particularly relevant for SARS-CoV-2, since pre-symptomatic transmission may be important.[3]
Guidance from global oversight bodies varies. At the start of the pandemic, the World Health Organization (WHO) noted in April 2020 that there was insufficient evidence to support mask use, with uncertainties about risks for healthy people in the community setting.[1] The WHO offered advice to decision-makers to consider the following before using masks in communities: (i) the rationale and reason for mask use must be clear; (ii) SARS-CoV-2 exposure risk in the community; (iii) population vulnerability to develop severe disease or mortality risk; (iv) population setting and ability to implement social distancing; (v) feasibility in terms of mask use costs, availability and tolerability; and (vi) mask type. The potential risks should also be considered, particularly diversion of medical mask supplies from essential service personnel such as healthcare providers. Regarding non-medical cloth masks, the WHO advised in June 2020 that decision-makers apply a risk-based approach and recommended the use of these masks in some situations such as in communities with widespread transmission and when there's limited space for physical distancing. Cloth masks should be used together with handwashing, cough and sneezing etiquette, and physical distancing as key to reducing transmission.[1]
The US Centers for Disease Control and Prevention (CDC) changed its guidance on 6 April 2020 regarding mask use for the general public by issuing a directive to cover your mouth and nose with a cloth face cover when around others'.[4] For healthcare workers, they recommended the use of homemade masks as a last resort, with a warning that their protective capacity is unknown and homemade masks should not be classified as PPE.[5] The CDC further recommended that medical masks or respirators be prioritised for healthcare providers and not be used by the general public.[6]
Evidence of the effectiveness of the cloth mask arises mainly from in vitro filtration studies, which showed that cloth masks may offer some protection from respiratory pathogens, despite substantially lower filtration ability compared with surgical masks.[7] Factors that may affect filtration include cloth type, stretching and the manner of mask washing.[8] In a simulation study assessing prevention of airborne particle expulsion, cloth masks offered marginal protection, with substantially better protection offered by medical masks.[9] However data from another simulation study reported that wearing any face mask reduces the distance travelled by a persons breath by more than 90%.[10] Further, all face masks without an outlet valve substantially minimised the ejection of air through a front flow jet. However, both medical and homemade cloth masks generate backward and sideways jets that may be hazardous to those behind or beside wearers.[10]
Widespread wearing of any type of mask has been proposed to reduce discrimination by limiting the identification of persons with SARS-CoV-2 infection. It has been further postulated that wearing a mask will limit face touching and create more general awareness.[11] Researchers have argued that health agencies consider asking the public to wear masks, even without strong evidence, due to the urgency of the pandemic and the need to distinguish between absence of evidence and evidence of absence.[12]
At the time of writing this review in early April 2020, guidance on the use of cloth and medical masks in the South African general population and households (community settings) was urgently needed to enable decision-makers to ensure evidence-based policies about preventing community transmission without depleting essential PPE stocks for healthcare workers. Since that time, face-coverings have been mandated for use in public; however, the need for strong evidence-based measures to prevent community transmission remains.
We conducted two rapid reviews of the evidence to quantify the effectiveness of cloth and medical masks in reducing the risk of SARS-CoV-2 transmission in community settings in April 2020. These informed evidence-based recommendations produced by the College of Public Health Medicine of South Africa (http://medat.samrc.ac.za/index.php/catalog/42).
Methods
We used a prespecified protocol following the Cochrane guidelines for rapid reviews.[13]
Eligibility criteria were developed a priori and applied throughout the screening process. The intervention was masks (cloth or medical) compared with no mask or other types of masks in community settings (general populations or households) with the primary outcomes of clinical or laboratory-confirmed respiratory illness. RCTs were included and non-controlled observational studies, editorials, guidelines and public press articles were excluded.
We searched three electronic databases (PubMed, Embase and the Cochrane Library) and two trials registries (www.clinicaltrials.gov/ and https://www.who.int/ictrp/en/) without language or date restrictions and not limited by terms for SARS-CoV-2, as this was early in the pandemic. The strategy is available on request. The search strategy was developed and conducted by an experienced information specialist on 30 and 31 March 2020. All records were uploaded into EndNote.
Records were screened independently in duplicate to identify eligible studies and the full-text articles were then obtained. Eligibility assessment, data extraction and assessment was conducted with the Cochrane risk of bias 2.0 tool (https://sites.google.com/site/riskofbiastool/welcome/rob-2-0-tool?authuser=0) were conducted in duplicate and independently.[14] Any disagreements were resolved through discussion or in consultation with a third reviewer (NS).
Where data permitted pooled synthesis, we conducted a meta-analysis using the generic inverse variance option in REVMAN (https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman) to combine adjusted estimates of effects using the random-effects model. Where reports of cluster trials did not include an intra-cluster correlation coefficient, we adjusted the variance accordingly and conducted a sensitivity analysis of both the reported and adjusted results to ascertain the robustness of the meta-analysis.
We conducted a grading of recommendations, assessment development and evaluation (GRADE) assessment to establish the certainty of the evidence across each outcome, taking into account risk of bias, directness, consistency, precision, and other considerations such as publication bias to determine whether the confidence in the overall results was high, moderate, low or very low.[15]
Results
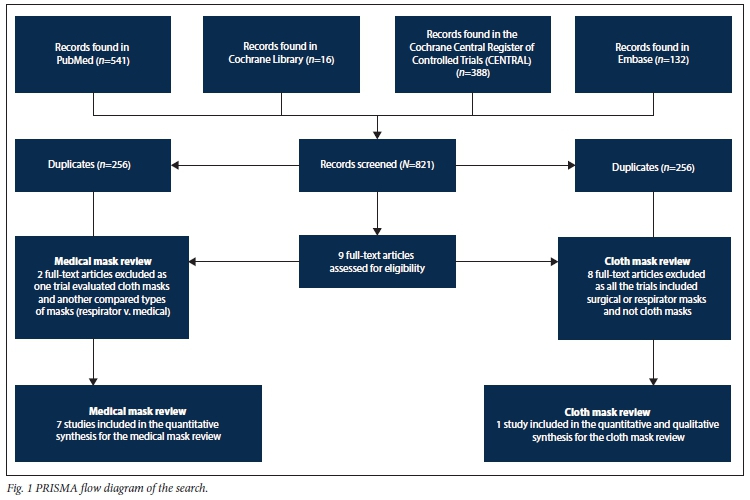
There were 821 unique articles retrieved and screened from three databases. Nine studies were assessed for eligibility, from which one RCT was identified for cloth masks and seven RCTs for medical masks. No SARS-CoV-2-specific studies were identified and as a result, we included studies which included other viral respiratory illnesses (Fig. 1). More detailed study data are available elsewhere (http://medat.samrc.ac.za/index.php/catalog/42).
No additional studies were identified from www.clinicaltrials.gov or the dedicated COVID-19 WHO international clinical trials registry platform (ICTRP) (https://www.who.int/ictrp/en/). Reference screening from systematic reviews did not yield additional studies.
Cloth mask review
Characteristics of the included RCT
No eligible studies were identified for cloth mask use in the community setting or SARS-CoV-2 infection. A cluster RCT conducted in healthcare workers was included to provide indirect evidence. Seventy-four wards across 15 hospitals in Hanoi, Vietnam[16] were randomised to adopt cloth masks, medical masks, or usual practice (a mixture of medical, cloth and no masks) for their healthcare workers. The study compared continuous mask use in a medical mask group (two new masks per day) with a cloth mask group (five masks for the entire 4-week period). We do not report on the control group, which used masks in compliance with existing hospital protocols as a high proportion of participants donned both medical and cloth masks (53%; n=245/458). Participants in the medical mask (n=580) and cloth mask (n=569) arms were required to wear masks all day.
Clinical respiratory illness (CRI) (two or more respiratory symptoms or one respiratory symptom and a systemic symptom), influenza-like illness (ILI) (fever >38°C plus one respiratory symptom) and laboratory infections were assessed. Viral respiratory infection was confirmed in the laboratory by detecting nucleic acids using multiplex reverse transcriptase PCR (RT-PCR) for 17 respiratory viruses: respiratory syncytial virus (RSV) A and B, human metapneumovirus (hMPV), influenza A (H3N2), (H1N1) pdm09, influenza B, parainfluenza viruses 1-4, influenza C, rhinoviruses, SARS-CoV, coronaviruses 229E, NL63, OC43 and HKU1, adenoviruses and human bocavirus (hBoV).
Healthcare workers kept diary records and monitored their temperature daily for 5 weeks. Symptomatic participants were swabbed for infection on the reporting day. Medical masks consisted of non-woven material, three-layered and locally sourced. Cloth masks were cotton and two-layered.
We judged the trial to be at low risk of bias. The lack of participant and researcher intervention blinding was a possible source of both measurement and detection bias, but this was mitigated by thermometer measurement and laboratory confirmation for positive symptoms.
Evidence of effects
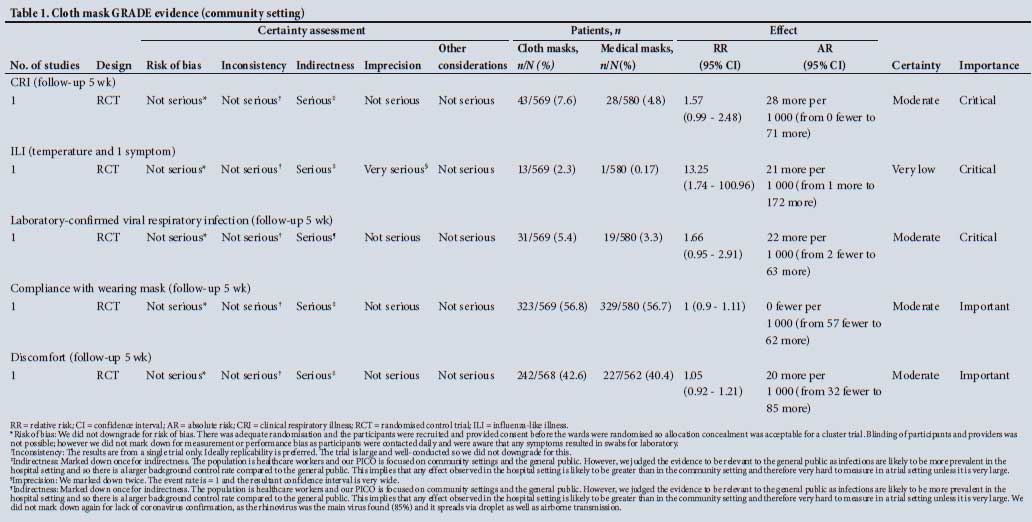
Using the GRADE approach, the overall evidence certainty for all outcomes was marked down for indirectness as the trial randomised masks in healthcare workers and not the general public. The rhinovirus, which is airborne and can also be spread in droplets, was identified as the main virus. We did not deem the lack of coronavirus-specific infections to warrant for further mark down tor indirectness (Table 1).
Clinical respiratory illness
In the crude analysis, there is moderate certainty that participants wearing cloth masks were probably more likely to exhibit CRI than those wearing medical masks (relative risk (RR) 1.57; 95% confidence interval (CI) 0.99 - 2.48). The effect remained similar even after adjusting for clustering (RR 1.57; 95% CI 0.87 - 2.84) and clustering and confounders (RR 1.56; 95% CI 0.98 - 2.49).
Influenza-like illness
There is very low certainty that participants wearing cloth masks may be more likely to exhibit ILI than those wearing medical masks (RR 13.25; 95% CI 1.74 - 100.96). The very low certainty was caused by the imprecision in the data due to the very low event rate and resultant wide confidence interval. The effect remained similar even after adjusting for clustering (RR 13.25; 95% CI 0.98 - 179.90) and clustering and confounders (RR 13.00; 95% CI 1.69 - 100.03).
Laboratory-confirmed viruses
Among the 68 laboratory-confirmed cases, 85% (n=58) were rhinoviruses. There is moderate certainty that participants wearing cloth masks were more likely to have laboratory-confirmed viral illness v. medical masks (RR 1.66; 95% CI 0.95 - 2.91). The effect remained the same even after adjusting for clustering (RR 1.66; 95% CI 0.81 - 3.40), and clustering and confounders (RR 1.54; 95% CI 0.88 - 2.70).
Compliance with wearing masks and adverse effects
There is moderate certainty that compliance in both groups was probably the same (RR 1.00; 95% CI 0.90 - 1.11). Both groups were 56% compliant. The proportion of participants who complained of discomfort was 42.6% in the group wearing cloth masks compared with 40.4% in those wearing surgical masks. There is moderate certainty that discomfort in both groups was the same (RR 1.05; 95% CI 0.92- 1.21).
Medical mask review
Seven RCTs met the inclusion criteria for the medical mask review.
Characteristics of the included RCTs
Community settings
Two cluster RCTs evaluated medical mask effectiveness for protection against ILI in a university student population. Healthy students living in residence received medical masks and instructions on their use, and the control group received no masks.[17,18] The ILI rate was evaluated across the student population.
Household settings
Four cluster RCTs evaluated medical mask effectiveness for protecting household members from acquiring IL1 infection from an infected member.[19-22] Only the ill household member was given a mask in two RCTs,[19,21] the ill participant and all other members of the household were provided with masks in the third trial,[20] and the ill participant and all household members who became ill during the study follow-up were advised to wear masks in the fourth trial.[22] The fifth RCT was conducted among pilgrims attending Hajj, and both the pilgrims with ILI symptoms and those sleeping near them were given masks.[23]
Evidence of effects
Community settings
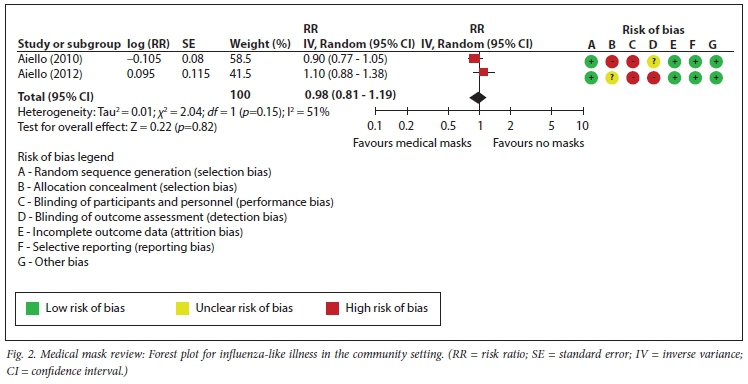
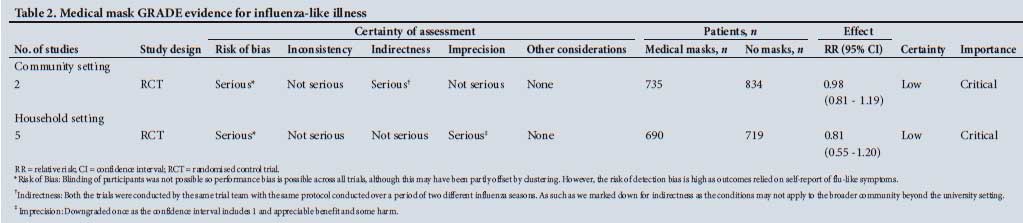
There is low-certainty evidence that there may be little or no difference in transmission between participants (mask group n=735; no mask group n=834) wearing medical masks and those not wearing medical masks (RR 0.98; 95% CI 0.81 - 1.19) in two trials (Fig. 2).[17,18] The low certainty is due to the probable risk of performance bias, as participants were not blinded and the assessment of the outcome relied on participant self-reported flu-like symptoms (possible detection bias). Furthermore, the trials were conducted by the same investigators over two seasons using a single protocol and may therefore have limited generalisability to community settings other than universities. We downgraded these trials for indirectness (Table 2).
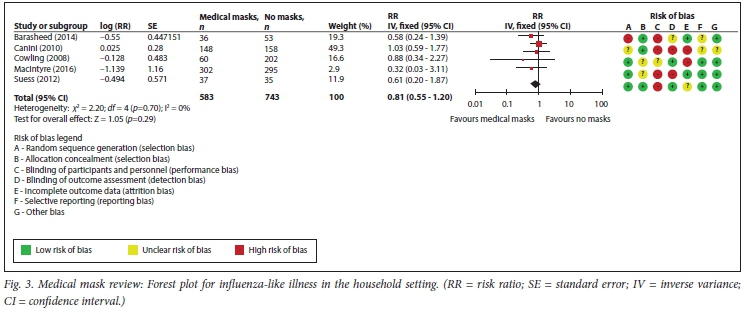
Household settings
There is low-certainty evidence that participants (mask group n=690; no mask group n=719) wearing medical masks were less likely to have ILI than those not wearing medical masks (RR 0.81; 95% CI 0.55 - 1.20) in five trials (Fig. 3).[17,18] The low certainty is partly due to imprecision because the confidence interval of the point estimate includes the null effect, appreciable benefit and some harm. The low certainty is also due to the high risk of performance bias because study participants were not blinded. The assessment of the outcomes relied on self-reported flu-like symptoms (possible detection bias).
As no adjustment for clustering was reported in the Barasheed et al.[23]trial, we adjusted the variance assuming an intraclass correlation coefficient (ICC) of 0.2 that was informed by the Suess et al.[22]trial and an average cluster size of 6 based on the Barasheed et al.[23] trial. Based on the aforementioned assumptions, we conducted a sensitivity analysis with and without the Barasheed et al.[23] trial in the meta-analysis and found a similar estimate of effect (RR 0.88; 95% CI 0.57 - 1.36).
Compliance in community settings
One trial reported that those wearing masks did so for an average (standard deviation (SD)) of 5.04 (2.2) hours per day,[18] while no compliance data were reported in the other trial.[17] Neither of the trials reported adverse effects.
Compliance in household settings
Compliance among trials varied. In the trials where only the ill household member wore a mask, the index patients reported wearing masks on average (SD) 3.7 hours (2.7) a day[19] and for 4.4 hours (95% CI 3.9 - 4.9) in the Maclntyre et al.[21]trial. Notably, in the latter trial, patients in the no-mask control arm also wore masks for an average of 1.4 hours (95% CI 0.9 - 1.8). In the Hajj-based trial, face mask compliance by pilgrims in the mask group was 76% (n=56/75), and 12% (n=11/89) in the no-mask control group.[23]
In the trials where both the ill household member and the rest of the household members were given masks, compliance was low in one of the trials, with more than 25% of the household contacts in the face-mask group not wearing a surgical mask at all during the follow-up period.[20] Moreover, more than 25% of index cases in the control and hand hygiene intervention arms reported wearing masks at home on their own accord, possibly contaminating the intervention. In the other trial where household contacts were advised to wear a mask only when they became ill, daily adherence was generally moderate and reached a plateau of over 50%.[22]
Three trials reported adverse effects. In the trial by Canini et al.[19] three-quarters (75%, /1=38) of the patients from the intervention arm reported discomfort with mask use, and the three main causes of discomfort were warmth (45%), respiratory difficulties (33%) and humidity (33%). Children wearing masks reported feeling pain more frequently (/1=3/12) than other participants wearingmasks (n=1/39).[19] In a trial by Suess et al.[22]adults (35%; n=10/29) and children (53%; n=18/34) complained about the heat/ humidity, followed by pain and shortness of breath when wearing a mask. Finally, a trial conducted by Barasheed et al.[23]reported that the most common reason for not wearing a face mask was discomfort (15%).
A sensitivity analysis including a more complete analysis of one of the studies[24] showed no change in the overall findings (http://medat.samrc.ac.za/index.php/catalog/42).
Discussion
No RCTs specific for the prevention of transmission of SARS-CoV-2 in the community were identified for either medical or cloth masks. A single cluster RCT among healthcare workers comparing medical masks with cloth masks provided indirect evidence to the general population, indicating that cloth-mask users were probably more likely to exhibit CRI or ILI v. medical masks users with a moderate and low degree of certainty, respectively Furthermore, users wearing cloth masks may be more likely to have laboratory-confirmed virus infections compared with wearers of medical masks.
In the medical-mask review, evidence from two trials assessing respiratory viral infections indicated that wearing medical masks may not be effective in preventing widespread community transmission of ILI. Data from five trials indicated that wearing medical masks may prevent transmission of ILI from ill to healthy members of the households. The generalisability of these results to the current SARS-CoV-2 pandemic remains unclear but at the onset of the epidemic in April 2020, they were deemed to provide reasonable indirect evidence to inform policy and guidance.
A recent systematic review by Jefferson et al.[26]updated a previous Cochrane review assessing the effectiveness of medical masks,[25] included 9 RCTs investigating the effect of masks in healthcare workers and the general population, and concluded that there is a lack of evidence for a protective effect of medical masks in all populations. However, their meta-analysis of the effect of masks on ILI and lab-confirmed influenza included trials in both the general population and healthcare settings. The separate effect of masks on ILI was only presented for the healthcare setting. Our results differ as we excluded trials conducted in healthcare settings, we sub-grouped trials by household and community setting rather than combining these, adjusted for clustering where necessary, and conducted sensitivity analysis due to the assumptions made in our clustering analyses. Importantly, our interpretation of the evidence, which included a GRADE assessment, differs to their conclusion as we concluded that in the household setting, medical masks may provide some protection to other members of the household.
In a recent systematic review and meta-analysis of observational studies evaluating measures to reduce SARS-CoV-2 and beta coronaviruses, a physical distance of a minimum 1 m was strongly associated with reduction of infection risk and a distance of 2 m was more effective. Data indicated that disposable surgical masks or reusable 12 - 16-layer cotton face masks were associated with protection, even in non-healthcare settings for the general public. No intervention, even when properly used, was associated with complete protection from infection.[27] Other basic measures such as hand hygiene are still needed with physical distancing, face masks and eye protection. These data also highlighted a need for further research on the effectiveness of different combinations of bundled interventions including variations in masks, physical distancing, handwashing and others as SARS-CoV-2 transmission dynamics are likely to change in different community settings depending on factors such as population density and the size of the population at risk. These interventions need to also be assessed for their acceptability affordability and impact on social, economic and environmental endpoints in addition to clinical outcomes.
Our rapid review findings highlight the urgent need for community-based controlled studies that compare the effectiveness of different facial coverings on mitigating the acquisition of SARS-CoV-2. Furthermore, given the possibility of subsequent COVID-19 waves, more comprehensive systematic reviews need to be conducted as new evidence becomes available.
There were several limitations in both rapid reviews. Firstly, only one trial was identified for the review assessing cloth masks v. medical masksandusualpractice.[16] The RCT was not community-based, providing only indirect evidence. However, the RCT design is one of the study strengths and we assume that the confounders and effect modifiers were equally distributed between trial arms. The authors of the study noted that 'the finding of a much higher rate of infection in the cloth mask group could be interpreted as harm caused by cloth masks, the efficacy of medical masks, or most likely a combination of both'.[16] The trial did not objectively assess self-contamination through repeated and improper doffing and handwashing techniques. Prior modelling studies have quantified the contamination level of face masks[28] and viruses may survive on the surface of face masks.[29] Pathogen transfer from cloth or medical masks to the bare hands of the wearer is plausible if doffing techniques in the RCT were inappropriate. Notably the study did not have a no-mask control group because it was deemed unethical to ask participants not to wear a mask, and the control group followed standard practice, which may or may not have included mask use.
In the medical-mask review, the two community-based trials assessing the effectiveness of medical masks v. no masks in preventing ILI acquisition took place at university residences. This limits the generalisability of the findings to community settings other than university residences, so the evidence was downgraded for indirectness. In the trials of household transmission, mask-wearing compliance varied, with some participants in the no-mask control group also wearing masks, signalling contamination and potentially reducing the estimate of effectiveness.
Wearing of masks has become highly politicised and polarised and was complicated by concerns that widespread wearing of medical masks by the general population may result in a shortage of masks for healthcare workers. To our knowledge, little attention has been given to considerations around the provision of what is optimal for individual and population health, rather than what is currently possible, feasible or necessary. Greenhalgh et al.[30] argues that traditionally designed studies may not be suitable for assessing the complexity of health services and systems and that there is a moral argument for applying the 'precautionary principle' of acting in the absence of evidence given the potential protective benefit of face masks in the face of rising COVID-19 mortality. Traditional studies should be complemented by studies which account for the instability and emergent causality' in a real-world setting allowing for adaptation to changing contexts.[31]
Chu et al.[27]recommend robust randomised trials of the effectiveness of several mask types in a community setting and for healthcare workers' protection. However, the authors also acknowledge that scientific uncertainty and contextual considerations require a more nuanced approach. However, Greenhalgh et al.[31] argued that the 'search for perfect evidence may be the enemy of good policy' and they proposed conducting two natural experiments: one to determine compliance with proper mask use and the second to overcome mask shortages by repurposing manufacturing capacity. If research confirms that wearing of medical masks is more protective than cloth masks in a community setting, greater advocacy for increasing manufacturing of sufficient medical masks for widescale distribution is warranted in the context of the current pandemic. Preparedness for the ongoing spread of the pandemic and future pandemics should include measures to scale-up global manufacturing of masks of proven efficacy, efficient supply chains and mitigation of environmental threats posed by disposable masks. Improved materials for cloth masks are therefore also an urgent consideration, but these need to be tested in comparative effectiveness studies in community settings. Like with the harmonisation of current SARS-CoV-2 vaccine and treatment trials,[32] studies testing the effectiveness of these masks will need to consider a harmonised approach to facilitate evidence synthesis. We believe these are urgently needed in South Africa to determine the specificities to our setting, the additional implementation considerations around appropriate contextual messaging and feasibility.
Conclusions
There is currently no evidence from RCTs demonstrating that the use of cloth or medical masks prevents the transmission of SARS-CoV-2 in the community setting. Indirect evidence from a single trial indicates that wearing cloth masks is associated with a higher risk of respiratory illness compared with medical masks. Medical masks may offer some protection to prevent household transmission of respiratory viral illnesses. The lack of direct evidence supportive of the efficacy, effectiveness and safety of masks in the community setting is an obstacle to evidence-based decision-making, particularly with a possible increase in emergent infectious viruses. There is a scope for comparative research into better-designed cloth masks and a need of controlled studies evaluating the efficacy of medical v. cloth masks conducted in the community setting where effects can be monitored, and potential harms identified early.
Declaration. None.
Acknowledgements. We would like to thank Alishka Rajman, Dishiki Kalonji, Jim Te Water Naude, Rene English, Kerrin Begg, Solange Durao, Bey-Marrie Schmidt and Ameer Hohlfeld for participating in the review of medical masks and independently conducting duplicate risk of bias assessments. Joy Oliver developed and conducted the search strategy. The rapid reviews were conducted to inform guidance documents developed by the College of Public Health Medicine of South Africa COVID-19 Evidence-based Task Team and were approved by the Colleges of Medicine of South Africa (http://medat.samrc.ac.za/index.php/catalog/42).
Author contributions. NS developed the protocol. TC and TK independently screened the records to identify eligible studies. KR, NS, CM and VR conducted duplicate data extraction and risk of bias assessment. NS conducted analysis and YB advised on adjusted statistical analysis. NS and TK conducted GRADE assessment. TC and VR wrote the draft manuscript. TC and VR contributed equally to the manuscript. All the authors approved the manuscript for publication.
Funding. None.
Conflicts of interest. None.
References
1. World Health Organization. Corrigendum. Advice on the use of masks in the context of COVID-19: Interim guidance, 5 June 2020. Geneva. WHO, 2020. https://www.who.int/docs/default-source/coronaviruse/corrigendum-to-ig-2020-4-ipc-masks-2020-06-05-pp-15-16-2020-06-06-e.pdf?sfvrsn=c5992b89_22020 (accessed 9 June 2020). [ Links ]
2. Morawska L, Milton DK. It is time to address airborne transmission of COVID-19. Clin Infect Dis 2020;71(9):2311-2313. https://doi.org/10.1093/cid/ciaa939 [ Links ]
3. Wycliffe E, Wei M, Zongbin L, et al. Presymptomatic transmission of SARS-CoV-2 - Singapore, January 23 - March 16 2020. Morb Mortal Wkly Rep 2020;69(14):411-415. https://doi.org/10.15585/mmwr.mm6914e1 [ Links ]
4. Centers for Disease Control and Prevention. How to protect yourself and others. Atlanta. CDC, 2020. https://www.cdcgov/coronavirus/2019-ncov/prevent-gerang-sick/prevenuon.html (accessed 6 May 2020). [ Links ]
5. Centers for Disease Control and Prevention. Strategies for optimising the supply of facemasks. Atlanta. CDC, 2020. https://wwwcdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/face-masks.html (accessed 6 May 2020). [ Links ]
6. Centers for Disease Control and Prevention. Use personal protective equipment (PPE). Atlanta. CDC 2020. https://wwwcdc.gov/coronavirus/2019-ncov/hcp/using-ppe.html (accessed 9 June 2020). [ Links ]
7. Davies A, Thompson K, Giri K, Kafatos G, Walker J, Bennett A. Testing the efficacy of homemade masks. Would they protect in an influenza pandemic? Disaster Med Public Health Prep 2013;7(4):413-418. https://doi.org/10.1017/dmp.2013.43 [ Links ]
8. Neupane BB, Mainali S, Sharma A, Giri B. Optical microscopic study of surface morphology and filtering efficiency of face masks. Peer J 2019;7:e7142. https://doi.org/10.7717/peerj.7142 [ Links ]
9. Van der Sande M, Teunis P, Sabei R. Professional and homemade face masks reduce exposure to respiratory infections among the general population. PLoS ONE 2008;3(7):e2618. https://doi.org/10.1371/journal.pone.0002618 [ Links ]
10. Viola IM, Peterson B, Pisetta G, et al. Face coverings, aerosol dispersion and mitigation of virus transmission risk. AarXiv:200510720 2020. [ Links ]
11. Leung CC, Lam TH, Cheng KK. Mass masking in the COVID-19 epidemic People need guidance. Lancet 2020;395(10228):945. https://doi.org/10.1016/S0140-6736(20)30520-1 [ Links ]
12. Feng S, Shen C, Xia N, Song W, Fan M, Cowling BJ. Rational use of face masks in the COVID-19 pandemic Lancet Respir Med 2020;8(5):434-436. https://doi.org/10.1016/S2213-2600(20)30134-X [ Links ]
13. Garritty C, Gartlehner G, Kamel C, et al. Interim guidance from the Cochrane rapid reviews methods group. J Clin Epidimiol 2020;130:13-22. https://doi.10.1016/j.jclinepi.2020.10.007 [ Links ]
14. Sterne JAC, Savovic J, Page MJ, et al. RoB 2. A revised tool for assessing risk of bias in randomised trials. BMJ 2019;366:4898. https://doi.org/10.1136/bmj.14898 [ Links ]
15. Guyatt GH, Oxman AD, Vist GE, et al. GRADE. An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336(7650):924-926. https://doi.org/10.1136/bmj.39489.470347.AD [ Links ]
16. Maclntyre CR, Seale H, Dung TC, et al. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open 2015;5(4):e006577. https://doi.org/10.1136/bmjopen-2014-006577 [ Links ]
17. Aielio AE, Murray GF, Perez V, et aL Mask use, hand hygiene, and seasonal influenza-like illness among young adults. A randomised intervention trial. J Infect Dis 2010;201(4):491-498. https://doi.org/10.1086/650396 [ Links ]
18. Aielio AE, Perez V, Couiborn RM, Davis BM, Uddin M, Monto AS. Facemasks, hand hygiene, and influenza among young adults. A randomised intervention trial. PLoS ONE 2012;7(1):e29744. https://doi.org/10.1371/journal.pone.0029744 [ Links ]
19. Canini L, Andreoletti L, Ferrari P, et al. Surgical mask to prevent influenza transmission in households. A cluster randomised trial. PLoS ONE 2010;5(1l):el3998 https://doi.org/10.1371/journal.pone.0013998 [ Links ]
20. Cowling BJ, Fung RO, Cheng CK, et al. Preliminary findings of a randomised trial of non-pharmaceutical interventions to prevent influenza transmission in households. PLoS ONE 2008;3(5):e2101. https://doi.org/10.1371/journal.pone.0002101 [ Links ]
21. Maclntyre CR, Zhang Y, Chughtai AA, et al. Cluster randomised controlled trial to examine medical mask use as source control for people with respiratory illness. BMJ Open 2016;6(12):e012330. https://doi.org/10.1136/bmjopen-2016-012330 [ Links ]
22. Suess T, Remschmidt C, Schink SB, et aL The role of facemasks and hand hygiene in the prevention of influenza transmission in households. Results from a cluster randomised trial, Berlin, Germany, 2009 -2011. BMC Infect Dis 2012;12:26. https://doi.org/10.1186/1471-2334-12-26 [ Links ]
23. Barasheed O, Almasri N, Badahdah AM, et al. Pilot randomised controlled trial to test effectiveness of facemasks in preventing influenza-like illness transmission among Australian Hajj pilgrims in 2011. Infect Disord Drug Targets 2014;14(2):110-116. https://doi.org/10.2174/1871526514666141021112855 [ Links ]
24. Cowling BJ, Chan KH, Fang VJ, et al. Facemasks and hand hygiene to prevent influenza transmission in households. A cluster randomised trial. Ann Intern Med 2009;151(7):437-446. https://doi.org/10.7326/0003-4819-151-7-200910060-00142 [ Links ]
25. Jefferson T, Del Mar CB, Dooley L, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst Rev 2011;(7):CDC006207. https://doi.org/10.1002/14651858.CD006207.pub4 [ Links ]
26. Jefferson T, Jones M, AI Ansari LA, et aL Physical interventions to interrupt or reduce the spread of respiratory viruses. Part 1. Face masks, eye protection and person distancing. Systematic review and meta-analysis. medRxiv 2020.2020.03.30.20047217. https://doi.org/10.1101/2020.03.30.20047217 [ Links ]
27. Chu DK, Akl EA, Duda S, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19. A systematic review and meta-analysis. Lancet 2020;395(10242):1973-1987. https://doi.org/10.1016/S0140-6736(20)31142-9 [ Links ]
28. Fisher EM, Noti JD, Lindsley WG, Blachere FM, Shaffer RE. Validation and application of models to predict facemask influenza contamination in healthcare settings. Risk Anal 2014;34(8):1423-1434. https://doi.org/10.1111/risa.12185 [ Links ]
29. Osterholm MT, Moore KA, Keliey NS, et al. Transmission of Ebola viruses. What we know and what we do not know? mBio 2015;6(2):e00137. https://doi.org/10.1128/mBio.00137-15 [ Links ]
30. Greenhalgh T, Papoutsi C. Studying complexity in health services research. Desperately seeking an overdue paradigm shift. BMC Med 2018;16(1):95. https://doi.org/10.1186/sl2916-018-1089-4 [ Links ]
31. Greenhalgh T, Schmid MB, Czypionka T, Bassler D, Gruer L. Face masks for the public during the COVID-19 crisis. BMJ 2020;369:ml435. https://doi.org/10.1136/bmj.ml435 [ Links ]
32. Corey L, Mascola JR, Fauci AS, Collins FS. A strategic approach to COVID-19 vaccine R& D. Science 2020;368(6494):948-950. https://doi.org/10.1126/science.abc5312 [ Links ]
 Correspondence:
Correspondence:
T Chetty
terusha.chetty@mrc.ac.za
V Ramokolo
vundli.ramokolo@mrc.ac.za
Accepted 24 November 2020


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}