










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.111 n.2 Pretoria Feb. 2021
http://dx.doi.org/10.7196/samj.2021.v111i2.15498
GUEST EDITORIAL
The Scientists' Collective 10-point proposal for equitable and timeous access to COVID-19 vaccine in South Africa
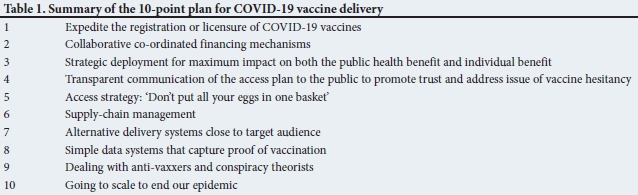
Recent announcements of the efficacy of four vaccines have sparked enormous hope that the world and individual countries will rapidly be able to bring the COVID-19 pandemic under control. South Africa (SA) must crystallise this hope with a smart, ambitious and effective plan to deliver the vaccine to the population in the shortest possible time frame, as suggested in Table 1.
The development of COVID-19 vaccines has been a spectacular scientific achievement, culminating in vaccines being authorised for use within 11 months of discovery of the SARS-CoV-2 virus (cause of COVID-19). In contrast, it has taken an average of 10.5 years for most other vaccines to be licensed from the time of discovery in the laboratory. The success in development of a COVID-19 vaccine has been fuelled by use of novel technology that is adaptable to quick modification to target new pathogens, hence shortening the timespan between pathogen discovery and vaccine development. Furthermore, the traditional approach of undertaking clinical development of the vaccine in series has been short-circuited by undertaking different phases of studies in parallel. Notably, this has been done under stringent regulatory authority and independent scientific oversight to ensure data integrity on both safety and efficacy.
Regulatory authorities set thresholds for vaccine efficacy to qualify for licensure. The recent announcement that four COVID-19 vaccines have achieved the efficacy threshold against COVID-19 illness, generally beyond expectations, represents a potential sustainable turning point in the pandemic. However, this will only materialise with timely, equitable and substantial access to vaccines that are suitable to being deployed globally, including in resource-constrained low- and middle-income country (LMIC) settings at an affordable price.
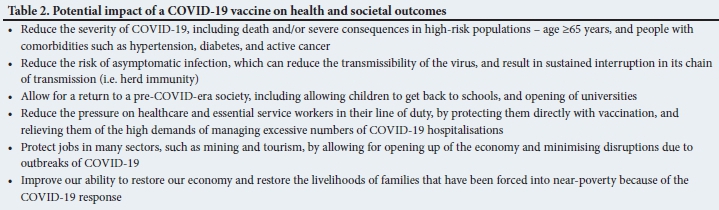
COVID-19 vaccines have the ability to modify our pandemic in two ways, with the potential to impact on disease outcomes and our ability to re-open our society, as summarised in Table 2:
1. Individual health benefits: Vaccines modify disease at an individual level, which translates into better outcomes for that specific person. The person has a milder illness, which will impact on hospitalisation and death. COVID-19 vaccine efficacy in reducing the risk of serious illness has been between 62% and 95%.
2. Public health benefits: By controlling transmission. If the vaccine also reduces the risk of infection (including mild illness and asymptomatic infection) by mass immunisation of between 60% and 70% of the population, herd immunity can be achieved. This means that we have the potential to limit transmission of SARS-CoV-2 and sustainably interrupt the chain of transmission of the virus.
Four COVID-19 vaccines have been found to be effective, and Emergency Use Authorization (EUA) in various countries will expedite the deployment of vaccines in these countries. EUAs are granted by a country's regulator, which in SA's case is the South African Health Products Regulatory Authority (SAHPRA). The UK's regulatory body has already granted an EUA for the first COVID-19 vaccine to be rolled out immediately (early December 2020) to their elderly population in care facilities, and to healthcare workers (HCWs). Further licensure in the UK and the USA (also targeting HCWs and high-risk groups) is expected by mid-December 2020.
There will be a high demand for COVID-19 vaccines, and manufacturing bottlenecks are expected. SA therefore has to be proactive, as supplies will be limited. It appears that more than 51% of the initial supply of COVID-19 vaccines likely to be available in 2021 has already been pre-purchased by countries such as Canada, the European block, the UK, the USA and Japan, where only 13% of the global population lives. This reality has brought calls for an urgent review of vaccine access for countries that lack the financial muscle to be competitive for vaccine procurement on the open market. In SA, the government will have to work in public-private partnerships to ensure timeous access to COVID-19 vaccines.
First and foremost, the government should prioritise vaccine access to HCWs and other front-line workers such as police and teachers, as well as our elderly and those at risk of severe COVID-19.
So what needs to be done for SA to get timeous and equitable access to COVID-19 vaccines (Table 1)?
1. Expedite the registration or licensure of COVID-19 vaccines
A vaccine can only be formally used in SA if it is authorised for use by SAHPRA, its regulator. SAHPRA will either have to authorise use under an EUA, or register any COVID-19 vaccine before it can be used in this country. Irrespective of who provides the vaccine, SAHPRA determines the conditions for its use in our country. Access can be fast-tracked in SA in the following manner:
• Section 21 authorisations - to satisfy an unmet emergency public health need for a defined target population(s)
• Conditional Registration (marketing authorisation) - for emergency use in a pandemic
• Full Domestic Registration - following an application by the pharmaceutical company to SAHPRA
• Domestic Registration under EUA - using the SAHPRA-adopted guidelines (2019) enabling the regulator to 'rely' on the work and decisions of other 'recognised' regulatory authorities (e.g. the Food and Drug Administration (FDA)) and the World Health Organization (WHO) pre-qualification process in making domestic registration decisions for a specific vaccine. SAHPRA and the vaccine developer and named distributor will need to work together to expedite the process. SAHPRA can approve the vaccine based on the European Medicines Agency (EMA), Medicines and Healthcare Products Regulatory Agency (MHRA) and FDA approval for EUA.
Once a vaccine is registered in-country, the state can put out tenders, or utilise sole-source service provision to procure the vaccine from the manufacturer or pharmaceutical company for the state sector, under the prescripts of the Public Finance Management Act. The state can use its infrastructure to make it available through the health system, the education system, correctional services, etc., and through mass vaccination strategies at community level. If licensed in-country, the vaccine could also be made available at out-of-pocket cost to the individual, through medical aids or workplace vaccination programmes. However, the supply of COVID-19 vaccines is likely to be highly restricted at least until the end of 2021, so there needs to be prioritisation of who to target for vaccination, at least until adequate supply becomes more predictable.
2. Collaborative co-ordinated financing mechanisms
SA has limited public resources and fiscal resilience to foot the bill for vaccine access. Public-private partnerships will be key to strengthening the bargaining power for bulk commitment, purchase and access.
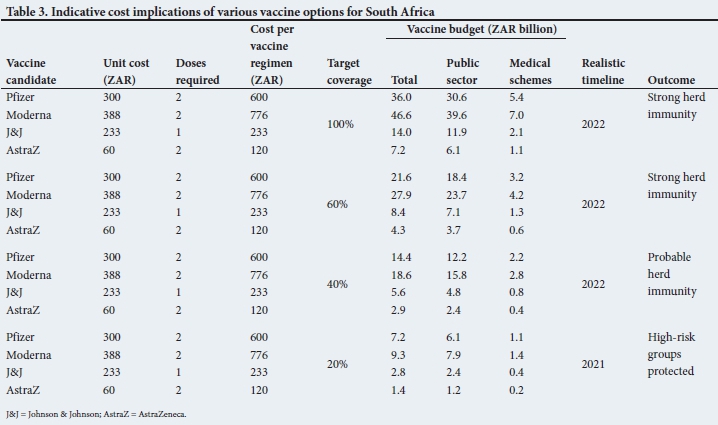
While we can expect a distribution of vaccine costs, a single dose of the Pfizer vaccine, for example, is estimated to cost ZAR300, resulting in a total cost of ZAR600 for two doses per person vaccinated. Vaccinating the entire population would cost roughly ZAR36 billion.
At the high end the Moderna vaccine is calculated at ZAR776 per person vaccinated, which translates into ZAR46.6 billion to fully vaccinate SA's population. Johnson & Johnson may come in at around ZAR233 per person vaccinated, or ZAR14 billion to fully vaccinate SA. AstraZeneca's COVID-19 vaccine has been estimated to cost around ZAR60 per dose, with a requirement for two doses per person vaccinated. This is the most affordable option for SA, and it is the vaccine likely to be the most accessible in the early part of 2021.
Although a national vaccine strategy may fall short of the total population, it must at least achieve sufficient coverage to attain herd immunity. In order to control the pandemic in SA, we estimate that we require: at least (i) 40 - 60% of the population to be vaccinated, and/or (ii) up to 40% of people to have been infected by and recovered from COVID-19. Already we are seeing high rates of exposure to SARS-CoV-2 in many communities (20 - 40% antibodies to SARS-CoV-2), although these are potentially quite localised.
Adopting the 40% vaccine coverage assumption, the cost of an effective vaccination strategy may range between ZAR2.9 billion and ZAR18.6 billion (Table 3). However, it is likely that any strategy aimed at attaining herd immunity will only be achieved in 2022. The question, therefore, is what are the target coverage and financial implications for 2021?
While 20% coverage is not enough to achieve herd immunity, it should result in the vaccination of the population most susceptible to severe forms of the disease, frontline health workers and other high-risk individuals. The 2021 strategy could range in cost between ZAR1.4 billion and ZAR9.3 billion (Table 3). How the vaccination strategy is divided between the public and private systems is the next issue to resolve.
While the public health system faces budget cuts at the moment, the medical schemes system counter-intuitively benefited financially from the pandemic. Given the fee-for-service reimbursement system, reductions in ambulatory and hospital-based activities for medical scheme-covered members saved billions for schemes during 2020. While these funds cannot be expropriated for public use, they can be accessed to ensure that government does not pay for any vaccine expenses that can be funded by medical schemes on behalf of their members. It is worth noting that all frontline health workers are members of medical schemes.
If the private sector foots the vaccination bill for their members (the Minister of Health would be required to add the COVID-19 vaccine as a prescribed minimum benefit), the budget for public sector vaccination of 20% coverage using the lowest priced vaccines on the market would be ZAR1.4 billion, a ninth of what one day of the level 5 lockdown cost SA. During 2021, medical schemes would only need to spend ZAR200 million to fund 20% of members. Even using the most expensive vaccine (Moderna), the total cost for 2021 would come to less than one day of the general lockdown (Table 3).
3. Strategic deployment for maximum impact on both the public health benefit and individual benefit
To maximise the impact of a COVID-19 vaccine, SA needs to focus on both effective scale-up and deployment of the vaccine, in addition to strategies that will give us maximum public health impact. In the immediate future, in the context of likely limited supply of COVID-19 vaccine throughout 2021, these efforts need to be focused on safeguarding our healthcare systems and protecting individuals at greatest risk of morbidity and mortality, and we propose a sequential immunisation strategy that balances both public health benefit and individual benefit, which is summarised in Table 4.
4. Transparent communication of the access plan to the public to promote trust and address the issue of vaccine hesitancy
Myths and misconceptions abound when it comes to the COVID-19 vaccine, and government needs to take special measures to share its plans and strategies to source and deliver the vaccine to the target population in a fair and rational manner. It needs to know (and to explain) how it will navigate the complex mechanisms of competitive pricing, patent protection, generic manufacturing and licensure in a way that benefits SA, how it will leverage the contribution that our scientists have made to development of these vaccines, and how it will participate in global pooled procurement mechanisms such as COVAX. What donation programmes will we access? Countries such as Canada have already placed orders for more vaccines than they need so possible proactive strategies could include engaging with countries with surpluses to ensure we don't fall to the back of the queue in favour of poorer countries, despite our burden of disease.
In SA there is currently wide speculation about vaccination plans, with some of the opinion that SA has no plan, no money, and no clue about how to finance and distribute a vaccine. These perceptions are important, as they shape the public view on vaccination and result in lack of confidence in vaccination programmes. There are efforts afoot to assess strategies for the state to fund a vaccine, as this represents an important public health priority, with broad-reaching implications for all sectors. Prioritising funds to protect our healthcare and essential workers, as well as preventing morbidity and mortality for the elderly and people with comorbidities, should be central in the government's response to COVID-19.
Multi-stakeholder engagement, such as involvement of trade unions, is central in highlighting the demand for both personal protective equipment and vaccines. To build confidence, the governmental structures dedicated to vaccine roll-out should immediately embark on further engagement with the relevant stakeholders to draft a roadmap as to how SA will access and roll out vaccines. Included in this should be the issue of vaccine hesitancy. Structured education and awareness programmes should be crafted with science communication entities such as the South African Agency for Science and Technology Advancement, which already has engagement activities around vaccines. Working with media houses such as public TV channels and community radio, experts should be called on to inform the public about the benefits of vaccination. In addition, informal communication methods should be optimised.
Appended to national and local communication efforts should be a concerted effort by national government to build trust and share information on plans to procure vaccines. These are important issues. Vaccine hesitancy has the ability to undermine our efforts to control COVID-19 in SA, as a vaccine can only work if the greater proportion of the populace firmly believe in the benefits.
5. Access strategy: 'Don't put all your eggs in one basket'
There are three components to this, and each has its pros and cons.
Access mechanisms
There are pros and cons to everything in life and there is no such thing as a free lunch!
COVAX, launched in April by the WHO, Gavi, the Vaccine Alliance, and the Coalition for Epidemic Preparedness Innovations, brings together governments, global health organisations, manufacturers, scientists, private sector, civil society and philanthropy. Slated as the only true global solution to equitable distribution of COVID-19 vaccines during the pandemic, the 'devil' is always in the detail. COVAX aims to have 2 billion doses of vaccine available by the end of 2021, enough to protect those at high risk and vulnerable people such as front-line workers, including in LMICs. The target is for countries to be able to access adequate vaccine for at least 5 - 20% of their population, should they make an upfront contribution to the COVAX facility.
The COVAX initiative is largely aimed at supporting affordable access to LMICs, while upper-middle-income countries and high-income countries will cross-subsidise funding for those with lower resources. However, many high-income countries have already entered into bilateral agreements with manufacturers (pharmaceuticals), which are likely to consume more than 50% of COVID-19 vaccines that will be available in the first half of 2021. Nevertheless, the rationale for high-income countries to invest in COVAX is to demonstrate solidarity with LMICs, and also the recognition that the pandemic will only end if there is widespread immunity to the virus, considering that we live in a highly interconnected world. For upper-middle-income countries such as SA, particularly where the economy is in the doldrums, procurement of COVID-19 vaccine will be at the same price charged for high-income countries. Inadvertently, the COVAX facility would undermine the ability of government in SA to access a large number of doses of COVID-19 vaccines at a more competitive price through bilateral agreements than what will be sourced through the COVAX facility. This is an oddity that SA (purportedly the country most affected by the COVID-19 pandemic on the continent) cannot afford - even if it inadvertently breaches a show of solidarity with other African countries. The poor will subsidise the poorer. The rich countries will not blink an eye, as most of them have already secured more than a fair size of their share of COVID-19 vaccines.
COVAX will give countries access to sufficient vaccines to vaccinate between 5% and 20% of their population. It is also not clear that we will be able to choose what vaccine we get.
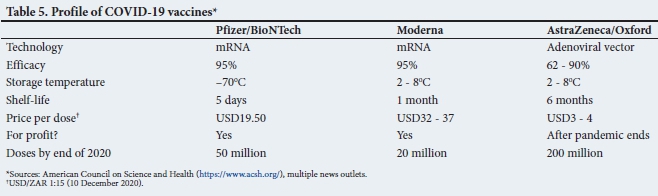
Other access mechanisms include 'bilaterals' with Pharma. Some pharmaceutical companies have promised break-even prices and also tech transfer to manufacture the vaccine locally. The state should prioritise these deals and ensure that locally produced vaccine is also destined for the local market. The COVID-19 vaccine trials being undertaken in SA should offer an opportunity for government to negotiate early access to meaningful quantities of vaccines at an affordable price with the companies whose vaccines are being evaluated (Table 5). Appended to this should be a programme to ensure that local manufacture capacity is poised to act as soon as a decision is made on which vaccine(s) will be rolled out. However, local manufacture of a COVID-19 vaccine is unlikely to materialise before 2022.
Bilaterals with countries, e.g. Russia and China, are potential strategies to access vaccines. This would still have to have SAHPRA approval, and our regulator will be charged with the responsibility of making sure the vaccine is safe and effective. There will still need to be a licence holder, who will take overall responsibility for vaccine safety, efficacy and delivery. Any vaccine used in SA, however, should be shown to have undergone rigorous evaluation for safety and efficacy, before it is considered for in-country use.
Vaccine choice
Different vaccines will have different mechanisms of action and will impact on different outcomes. Table 5 summarises some of the challenges for access. The volume of vaccine available for distribution is critical. Data on the impact of COVID-19 vaccine on severe infection and death are accumulating, and may influence choice in high- to middle-income countries.
Our choice of vaccine will impact on public health outcomes. It is important to note that individual benefit may be different depending on the vaccine choice.
Tech transfer and manufacturability
For SA, the ability to be involved in a tech transfer deal will consolidate local access. Ease of manufacture will influence volume of doses. Local manufacturing scale-up is unlikely to happen in SA in 2021. SAHPRA has yet to accredit a vaccine manufacturing site in SA.
6. Supply-chain management
Supply-chain planning will depend on the cold-chain requirements of the particular vaccine, the complexity of which will increase as we move from 2 - 8°C to -80°C (Table 5). Planning should ensue now, routing with review of holding hubs, distribution models and costs thereof. Transport conditions will need to be more sophisticated, requiring electronic support, together with cold-chain monitoring and confirmation of delivery. There are several systems that could be co-opted to assist: current medicine delivery routes, and laboratory transport capacity in both the public and private sectors. Significant planning and innovative delivery mechanisms will be required. New design applications for monitoring the process are already available for review.
Supply-chain management requires early planning, from warehouse to vaccination point. Maintaining the cold chain is imperative for the stability of the vaccine (Table 5).
7. Alternative delivery systems close to the target audience
Alternative delivery options include the delivery and network services on large e-commerce platforms that have efficient and cost-effective mechanisms to move material across the country with strong monitoring systems. Many airlines have been grounded as a result of travel restrictions. For a brief period, planes could be repurposed to rapidly transport vaccines to large metropoles for further distribution into communities. Substantive effort has been placed in developing track-and-trace systems in communities, and these could easily be repurposed for distribution of vaccines.
Given the speed and the high levels of population coverage needed in delivery of the vaccines, it would be unwise to rely entirely on the health system to take on the entire burden of vaccine roll-out. As it is common cause that health workers should be the first target group, it is obvious that the first batch of vaccines should be administered to health workers through the public and private healthcare systems. As significant numbers of health workers have medical insurance, there is an opportunity for the bill to be shared across the public and private sectors.
The elderly and those with comorbidities will be a more difficult group to access, and multiple strategies will need to be employed to reach them, including clinics where they receive chronic medication, social grants delivery points, old-age homes and churches. Community health worker outreach teams have huge potential here. This is a massive operation and will require detailed planning and resourcing.
The schools and universities have the ability to play an important role in reaching the adolescent and young adult populations that are globally proving unable to abide by non-pharmaceutical interventions. Targeting this population could be key to breaking the cycles of transmission in many communities and within families, and the order in which they are prioritised will be influenced by estimates of the public health benefits of vaccinating this group for the benefit of the entire population.
The programmes above could take a year or even 2 years to execute and are insufficiently expeditious to capitalise on an effective vaccine intervention that moves the COVID-19 needle quickly enough, so it is imperative that new innovations are considered. Accelerating access should be our overall objective. Thinking outside the box, such as using the Independent Electoral Commission to use their infrastructure, organisation and IT capability to get vaccine to millions of people in one day. All that would be needed is an ID document that is scanned to record participation and a nurse in the polling booth. Many thousands of people could be vaccinated in a single day. This would exclude groups such as foreign nationals, who could be accommodated through alternative service delivery mechanisms. Using the Post Office, South African Social Security Agency outlets and other places where the elderly queue would be options to get them vaccinated rapidly.
8. Simple data systems that capture proof of vaccination
Digital technologies to monitor vaccine uptake and usage of doses will be critical to ensure continuity and integrity of the logistic supply chain. These could be linked to electronic dashboards that provide a nationwide view of vaccine uptake, which could then be further useful to monitor incidence of disease. Similar dashboards already exist to monitor diagnosis of infectious diseases such as tuberculosis. Data systems would also enhance the country's ability to evaluate long-term safety and efficacy of the vaccine.
9. Dealing with anti-vaxxers and conspiracy theorists
The anti-vaccination movement (anti-vaxxers) and the propagation of conspiracy theories are impediments to SA's ambitions to achieve herd immunity using vaccination as an accelerator. However, anti-vaxxers and conspiracy theorists will not be negated merely by attempts to discredit them in the media. We need to build basic, simple communication of the evidence, delivered to the public in a way that maximises its transfer and its impact. That will include bringing all facets of society with us on this journey and ensuring that trusted givers of information are prioritised, be they traditional healers, respected leaders in civil society, religion and government, role models, 'influencers', clinicians, public health specialists, or scientists. Government needs to work with all stakeholders and experts in communication to achieve this delivery of trusted, evidence-based information. Westernised traditional forms of communication need to be augmented with informal means such as oral, folk and theatrical delivery of accurate information, woven into a culture- and context-specific model.
10. Going to scale to end our epidemic
Already at the time of writing, four vaccines have demonstrated effectiveness. To control an epidemic, we need herd immunity. If we don't have any vaccine by winter, our country will not be able to go back to normal. If we put vaccines together with all the tools we have, we could reduce mortality and stop transmission and get our lives back. We cannot afford to let this opportunity go to waste.
We need all hands on deck. Without co-ordination, we will see chaos and duplications of effort similar to those that were evident at the beginning of our local epidemic. We cannot only rely on the National Department of Health and the public sector. We need the private sector, labour, and entities such as Médecins Sans Frontières, the Red Cross and Gift of the Givers to support the national roll-out of vaccines. This is an endeavour that requires all our resources and effort.
Glenda Gray, South African Medical Research Council glenda.gray@mrc.ac.za
Alex van der Heever, Wits School of Governance, University of the Witwatersrand, Johannesburg
Shabir Madhi, MRC Vaccines and Infectious Diseases Analytics Research Unit, University of Witwatersrand, Johannesburg
James McIntyre, Anova Health Institute, Johannesburg, and School of Public Health and Family Medicine, University of Cape Town
Bavesh Kana, University of the Witwatersrand and National Health Laboratory Service, Johannesburg
Wendy Stevens, University of the Witwatersrand and National Health Laboratory Service, Johannesburg
Ian Sanne, Right to Care and University of the Witwatersrand, Johannesburg
Guy Richards, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg
Fareed Abdullah, South African Medical Research Council
Marc Mendelson, University of Cape Town
Aslam Dasoo, Progressive Health Forum
Jeremy Nel, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg
Adrienne Wulfsohn, Inkosi Albert Luthuli Central Hospital, Durban
Lucille Blumberg, National Institute for Communicable Diseases, National Health Laboratory Service
Francois Venter, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}