










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.111 n.1 Pretoria Jan. 2021
http://dx.doi.org/10.7196/samj.2020.v111i1.14520
RESEARCH
Substance use and depressive and anxiety symptoms among out-of-school adolescent girls and young women in Cape Town, South Africa
C P BonnerI; T CarneyII; F A BrowneIII; J W NdiranguIV; B N HowardV; W M WechsbergVI, VII, VIII
IPhD; Substance Use, Gender, and Applied Research Program, RTI International, Atlanta, GA, USA
IIPhD; Alcohol, Tobacco and Other Drug Research Unit, South African Medical Research Council, Cape Town, South Africa
IIIScD; Substance Use, Gender, and Applied Research Program, RTI International, Research Triangle Park, NC, USA
IVMSc-GH;Substance Use, Gender, and Applied Research Program, RTI International, Research Triangle Park, NC, USA
VBA; Substance Use, Gender, and Applied Research Program, RTI International, Research Triangle Park, NC, USA
VIPhD; Department of Maternal and Child Health, Gillings School of Global Public Health, University of North Carolina, Chapel Hill, NC, USA
VIIPhD; Department of Psychology, North Carolina State University, Raleigh, NC, USA
VIIIPhD; Department of Psychiatry and Behavioral Sciences, Duke University School of Medicine, Durham, NC, USA
ABSTRACT
BACKGROUND: There is a high prevalence of substance use among youth in South Africa (SA), and adolescent girls and young women (AGYW) experience high rates of depression and anxiety. Substance use behaviours and mental health are associated with other public health problems among AGYW such as HIV and unintended pregnancy. Therefore, understanding the relationship between substance use and mental health is imperative to improve AGYW's health.
OBJECTIVES: To examine the association between heavy drinking, marijuana, methamphetamine and methaqualone (Mandrax) use and depressive and anxiety symptoms among AGYW aged 16 - 19 years who have dropped out of school in Cape Town, SA.
METHODS: Data for this report come from the baseline data of 500 participants of an ongoing cluster-randomised trial assessing the efficacy of a young woman-focused intervention to reduce substance use and HIV risk. After AGYW consented/assented to participate, they completed a urine drug screen and a baseline questionnaire.
RESULTS: Logistic and negative binomial regressions, controlling for clustering at the neighbourhood level, revealed that frequency of depressive symptoms was significantly and positively related to a positive drug screen for Mandrax (β=0.07; p=0.03). All other associations between the frequency of depressive symptoms and substance use were not statistically significant (ps>0.05). The associations between frequency of anxiety symptoms and substance use were not statistically significant (ps>0.05).
CONCLUSIONS: Our findings highlight the need to address substance use, especially Mandrax use and its associated risk, and depression in an integrated, youth-friendly setting.
South Africa (SA) is currently experiencing a high prevalence of substance use among young people.[1-3] Almost 50% of secondary learners or high school students report lifetime alcohol use, with 13% reporting their first drink before age 13. Approximately 13% of learners report lifetime use of marijuana (dagga), and 10% report using illicit drugs such as methamphetamine (tik) or methaqualone (Mandrax).[1] This high prevalence is concerning because substance use is associated with myriad adverse mental health outcomes among SA young people.[4-6]
The association between substance use and depression and anxiety disorders among adolescents and young adults in SA and other countries has been well documented.[5,7] However, little of this research has focused specifically on adolescent girls and young women (AGYW) in SA. Almost 62% of AGYW in SA experience depression,[8] and 11% of youth experience generalised anxiety disorder.[9] Furthermore, SA women are more likely to have a lifetime prevalence of depression or anxiety than men.[10] AGYW are an important population to consider because their substance use behaviours and mental health are intricately tied to other public health problems facing this population, such as HIV[11] and unintended pregnancy.[12] For example, methamphetamine use[13,14] and mental health problems[15] are associated with condomless sex among AGYW. Therefore, to fully curtail public health issues such as HIV and unintended pregnancies, substance use and mental health among AGYW must be addressed.
Objectives
Given the prevalence of depression and anxiety among AGYW in SA,[8,16] the high prevalence of alcohol and other substance use among youth,[16] and the impact of substance use and mental health on HIV,[17] understanding the relationship between substance use and mental health is imperative to improve the physical and psychological wellbeing among this population. The objective of the current study is to examine the association between heavy drinking, marijuana, methamphetamine and Mandrax (which is often mixed with cannabis) use, and depressive and anxiety symptoms among AGYW aged 16 - 19 years old who have dropped out of school in Cape Town, SA. These are commonly used substances among young people in SA.[4,16] Based on similar research with other populations of people who use substances, we hypothesise that AGYW who report engaging in heavy drinking, marijuana use and methamphetamine use will report more frequent anxiety and depressive symptoms.[4,16,18] Furthermore, given the relative dearth of research regarding the association between Mandrax use and mental health symptoms, we will explore this association to better understand how this specific substance may be associated with depressive and anxiety symptoms.
Methods
Design
Data for this report come from the baseline data provided by participants of a cluster-randomised trial assessing the efficacy of a young woman-focused intervention to reduce substance use and HIV risk.
Setting
Participants were recruited from 24 community clusters across Cape Town, SA. Twelve communities were comprised predominately of those who self-identify as black African, and 12 were comprised predominately of those who self-identify as coloured (racial categories created during the Apartheid era in SA).
Participants and recruitment
Female adolescent peer role models were identified through the Western Cape Province's Department of Social Development's Expanded Public Works Programme (EPWP). The EPWP is a government programme that employs individuals from economically disadvantaged communities in a range of public and community services. EPWP beneficiaries, in combination with trained outreach workers, recruited participants using established community-based outreach methods that have been successful in other studies engaging young women.[19] The EPWP beneficiaries marketed the study by describing the study and the non-monetary benefits (e.g. HIV testing) of study participation, and helped to identify potential participants, but did not screen. Trained study outreach workers conducted the screening with AGYW individually, ensuring privacy and confidentiality. Study staff were multilingual in English, Afrikaans and/or isiXhosa. Eligibility criteria were the following: (i) aged between 16 and 19 years; (ii) self-identified as a woman; (iii) reported consuming 2 - 3 alcoholic drinks at least once in the past 30 days, or using illicit drugs at least once a week in the past 30 days; (iv) currently dropped out of school; (v) had been out of school for at least 6 months; (vi) had not completed matriculation (high school) or did not have an N3 (National Technical Certificate) certificate; (vii) reported condomless sex with a male partner in the past 90 days; (viii) reported living in one of the 24 target disadvantaged communities; (ix) had lived in the target community for at least 6 months; (x) planned to reside in the target community for the next year and could provide verifiable locator information; and (xi) provided verbal and written consent/ assent. A short cognitive test was given at the end of the eligibility screen,[20] and individuals were excluded if they had a score that indicated cognitive impairment. A total of 500 young women were enrolled in the study.
Procedures
If individuals were eligible and interested in participating in the study, they were scheduled for an intake appointment. During the intake appointment, young women were rescreened to ensure eligibility and given detailed information about the study through the consent/ assent process. Those who were interested in participating in the study and were >18 years of age provided consent. Those who were <18 years of age provided assent and were required to obtain written permission to participate by a trusted woman who was >25 years of age. Young women could identify this trusted woman (e.g. a sister) or
could agree to be introduced to a trusted female community member who had been identified by the study's staff. These trusted women consented for those <18 years of age in loco parentis (in place of the parent). This approach was used because if parents were to learn about a participant's substance use and sexual activity, it could result in conflict or violence in the family. The in loco parentis process has been used successfully in previous SA research with adolescents.[19]
Once they consented/assented to participate, participants underwent a breathalyser test for recent alcohol use and provided locator information (including having a photograph taken to identify the participant) to be used to contact them for follow-up. Participants then completed the baseline questionnaire via computer-assisted personal-interviewing technology, and audio computer-assisted self-interviewing in the language of their choice (English, Afrikaans or isiXhosa) for sensitive topics, such as experiences of abuse. Next, participants provided urine samples and staff conducted pregnancy testing, screening for recent drug use (e.g. marijuana, opioids, Mandrax, cocaine, methamphetamine) using a rapid urine drug screen, conducted pre- and post-HIV counselling and rapid testing via finger prick, and provided participants with the test results. This appointment lasted approximately 2 hours, and participants were remunerated ZAR150 (~USD10.00) for their time.
Participants residing in communities that were randomised to the intervention arm were scheduled to participate in two group workshops focused on substance use and sexual risk reduction over the next ~2 weeks post enrollment. All participants were scheduled to return 6 and 12 months post intake for follow-up assessments. This article only reports data from the baseline appointment.
The SA co-investigator, SA co-project director, and the US principal investigator of this study are all psychologists who have extensive experience assisting with distressed participants (e.g. experiencing suicidal ideation). In addition, all staff were trained on a standard protocol to assist distressed participants, which included consulting with senior staff. All procedures were approved by ethics review boards at RTI International (ref. no. 0214954) and the SA Medical Research Council (ref. no. EC006-3/2016).
Main outcome measures
The Revised Risk Behavior Assessment[21] tool was used to collect behavioural data. This instrument includes measures of sexual risk, mental health symptoms and substance use behaviours, and was modified for use in SA and combined with instrumentation from the US National Institute on Drug Abuse (NIDA) data harmonisation effort.[22]
Substance use
Participants' heavy alcohol use was defined by the extent to which participants reported the consumption of four or more alcoholic drinks a day. Heavy alcohol use was measured by assessing the number of days that participants had consumed four or more drinks in the past 30 days. Recent drug use was measured using a urine drug screen to detect metabolites of recent use of cocaine, methamphetamines, amphetamines, opioids, ecstasy and marijuana. Mandrax was measured through a separate urinalysis test. Participants also self-reported their lifetime and past-month use (use/not used; frequency of use in the past month) of marijuana, methamphetamines, heroin, cocaine, inhalants, ecstasy, other amphetamines, non-medical use of prescription medications and other drugs. Based on the results of the urine drug screen, participants were coded as 1 = positive or 0 = negative for each drug tested. This variable was used as the outcome of the main analyses.
Depressive and anxiety symptoms
The frequency of participants' depressive and anxiety symptoms was assessed using the Drug Abuse Treatment for AIDS Risks Reduction depression scale (a 7-item scale; α = 0.70) and anxiety scale (a 7-item scale; α = 0.79).[23] Responses indicated the extent to which participants had experienced each symptom in the past 90 days and were on a Likert scale (0 = never to 4 = almost always). Higher scores indicated more frequent depressive or anxiety symptoms. This scale has demonstrated satisfactory reliability in other samples of women in SA.[24,25]
Covariates
Participants' engagement in sex work was assessed using the question, 'Have you ever traded sex to get the things you need (like drugs, money, food, clothing, shelter, transport, or any other goods)? This would include sex work.' Participants responded 1 = yes or 0 = no. Ethnicity was assessed using the question 'Do you consider yourself to be black African, coloured (i.e. mixed ancestry), Asian/Indian, white South African or another race or ethnic group?' from the screener. These racial categories represent classifications that were developed during the Apartheid era in SA.[26] Given the ethnic make-up of the targeted communities, all participants identified as either black African (coded as 0) or coloured (coded as 1). HIV status was assessed using a minimum of two rapid HIV tests (via finger prick). If the two results were concordant positive or negative, then no additional testing was done. If they were discordant, a third confirmatory test was done. Participants were classified as HIVpositive if two tests were positive. Results were coded as 0 = HIVnegative or 1 = HIV-positive.
Analysis
We used Stata version 15 (StataCorp, USA) for all the analyses. Descriptive analyses were performed and the associations among the outcomes of interest (heavy drinking, marijuana use, methamphetamine use and Mandrax use) as well as conceptually meaningful covariates (e.g. engagement in sex work, HIV status and ethnicity) were explored first. Next, separate logistic regression models were conducted to explore the association between biologically confirmed marijuana, methamphetamine and Mandrax use and the frequency of depressive and anxiety symptoms. Then, separate negative binomial regression models were conducted to examine the association between frequency of depressive and anxiety symptoms and days of heavy drinking. All analyses controlled for clustering at the neighbourhood level using a robust cluster estimator. P-values <0.05 and confidence intervals that did not include 1 indicated significance.
Results
Demographics
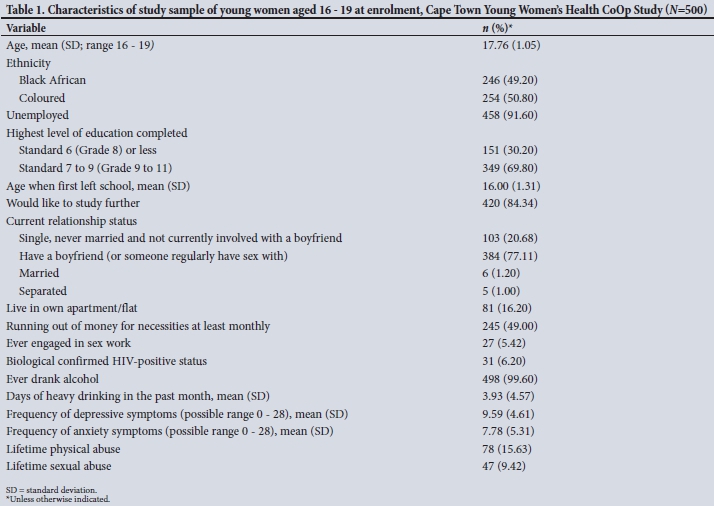
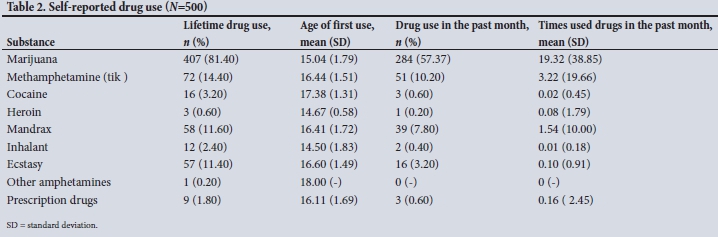
Characteristics of the sample are shown in Table 1. The mean (standard deviation (SD)) age of the participants was 17.8 (1.1). Approximately half of the participants identified as coloured and the other half identified as black African. Of note, almost half of the AGYW in the study reported that their household ran out of necessities at least monthly. Most participants tested positive for marijuana (38.6%) during the drug screen. Participants' mean (SD) scores regarding the frequency of depressive and anxiety symptoms were 9.6 (4.6) and 7.8 (5.3), respectively. These scores indicate that on average, participants experienced depressive or anxiety symptoms slightly more than rarely. Alcohol (99.6%) and marijuana (81.4%) were the most commonly self-reported substances used during participants' lifetime. Table 2 displays information about the self-reported drug use of the sample.
Primary analysis
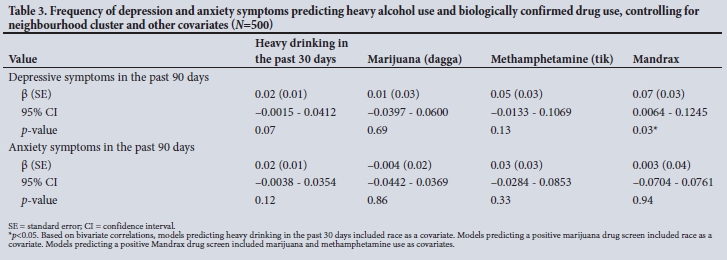
As shown in Table 3, negative binomial regression, controlling for neighbourhood cluster, revealed that the frequency of depressive symptoms was related to an increase in the number of days of self-reported heavy drinking in the past 30 days (β=0.02, p=0.07); however, this trend was not significant. Logistic regression revealed that self-reported frequency of depressive symptoms in the past 90 days was not significantly related to a positive drug screen for marijuana (p=0.69) or methamphetamine (p=0.13). However, frequency of depressive symptoms was significantly related to a positive drug screen for Mandrax, such that an increase in the frequency of depressive symptoms was related to a greater likelihood of testing positive for Mandrax (β=0.07; p=0.03). Frequency of anxiety symptoms was not significantly related to the number of heavy drinking days in the past month, use of marijuana, use of methamphetamine or use of Mandrax (ps>0.05).
Discussion
Globally, substance use and mental health disorders are public health epidemics.[27] SA, in particular, has a considerable disease burden attributable to substance use and mental health disorders,[28] and a substantial number of those affected are youth.[4,9,16] Moreover, AGYW are more likely to suffer from mental health disorders such as depression and anxiety. However, little research has specifically examined the association between substance use and depression and anxiety among AGYW in SA. This is problematic because research suggests that the age of onset for many substance use and mental health disorders occurs before the age of 24, and those who are most vulnerable often experience these problems simultaneously.[29,30] This study fills this gap by examining the correlates of depressive and anxiety symptoms among vulnerable AGYW in SA.
Statement of principal findings
Findings from the present study suggest that the frequency of depressive symptoms may be positively related to the use of Mandrax. Depressive symptoms and heavy alcohol use were also positively related, although this association was not significant. This study did not find significant associations between the frequency of depressive symptoms and marijuana and methamphetamine use. Similarly, there were no statistically significant associations between frequency of anxiety symptoms and the use of any substance examined.
Mandrax use as an illicit drug is unique to SA.[31,32] Some research has linked Mandrax to sexual risk.[33] Still, the association with mental health and Mandrax use has not been thoroughly examined. Therefore, our finding highlighting the association between depressive symptoms and Mandrax use is novel. This study illustrates the need for and potential benefit of further examination of the link between depressive symptoms and Mandrax use - and related outcomes such as sexual risk - among AGYW in SA.
This study did not demonstrate a link between the frequency of depressive symptoms and heavy alcohol use, marijuana use or methamphetamine use, nor between anxiety symptoms and the substance use outcomes of interest. While these findings did not support our hypotheses, there are plausible explanations for these findings. The assessments of depressive and anxiety symptoms focused on frequency and not necessarily duration, severity, onset or impairment related to the symptoms. While frequency and these other dimensions of symptoms are related, they are not synonymous. Therefore, the association between symptoms of depression and anxiety and substance use may differ based on the dimension (e.g. frequency, severity, duration, impairment) that is assessed. For example, one may frequently experience trouble sleeping (a common symptom of depression and anxiety), but the association between sleep and substance misuse may be accounted for by impairments in functioning such as reductions in emotion regulation - which may be a stronger predictor of substance use than the frequency of the symptoms.[34] As it relates to anxiety, the association between substance use and symptoms may depend on the particular type of anxiety disorder that one experiences. For example, the link between post-traumatic stress disorder and substance use has been consistently demonstrated among other populations such as adult women,[35] survivors of natural disasters[36] and survivors of victimisation.[37] Therefore, the associations may be more nuanced than the current article can examine due to the limitations of secondary data analysis.
Strengths
The present study may be among the first to explore the associations between depressive and anxiety symptoms and heavy drinking, marijuana, methamphetamine and Mandrax use among vulnerable AGYW in Cape Town. The examination of Mandrax use as a correlate of depressive and anxiety symptoms is a particular strength of this paper, given its prevalence among South Africans.[32,33,38] Additionally, our focus on out-of-school AGYW - a hard-to-reach population that has been understudied regarding their mental health - is a strength. Understanding substance use and mental health among this population is important given their role in HIV risk and unintended pregnancy among AGYW in SA.[39] Our sample was also recruited from communities in SA, which strengthens the external validity of the findings. As it relates to measurement, we used assessments that have been utilised and validated in similar samples in SA. Relatedly, recent substance use was assessed using a urine drug screen, which typically detects drug metabolites up to 2 - 30 days after use, depending on the substance of use[40] - which is more accurate than self-report. Collectively, these strengths contribute to the validity of our findings.
Limitations
The strengths and implications should be interpreted considering study limitations. The data for this study were taken from baseline data of a larger trial examining the efficacy of a young woman-focused HIV prevention intervention. The assessment period for depressive and anxiety symptoms was the past 90 days, and the assessment period for heavy alcohol use was the past 30 days. The urine drug screen has an assessment period of up to 30 days. Given the assessment periods of each outcome, temporality may be suggested, but causality cannot be inferred. For example, it may be reasonable to believe that depressive symptoms in the past 90 days may predict Mandrax use in the past 30 days. However, drug use may also precipitate or exacerbate mental health symptoms. For example, Mandrax use or withdrawal could contribute to anxiety symptoms. Therefore, longitudinal assessments of substance use and mental health symptom assessments of substance use and mental health are necessary for future research to understand the causality of these associations. The assessment of depressive and anxiety symptoms was not diagnostic. Therefore, we are unable to discern if clinically diagnosed depression or anxiety are related to substance use. Future research should examine these associations using more diagnostic tools. Relatedly, future research may benefit from examining how different types of mood and anxiety disorders may be related to the use of different substances. The biological assessment of recent substance use also has some limitations. While rapid urine drug screens are more reliable than self-report, there is the risk of false-positives due to secondary exposure to marijuana and the use of other medications (e.g. antidepressants, such as may result in false-positive tests for methamphetamine).[41] We did not conduct a comprehensive assessment of the medications that participants were taking, therefore we could not address this risk. Lastly, we did not assess how the composition of Mandrax that AGYW reported using was related to their mental health symptoms. Mandrax is often mixed with cannabis and smoked, and may be used with other substances.[2] Therefore, it will be important for future research to understand how the composition of Mandrax may differentially affect AGYW's mental health symptoms. These limitations notwithstanding, this study adds to the existing literature and serves as a basis to explore the nuanced associations between substance use and mental health among AGYW in Cape Town, SA.
Contributions
This study contributes to the nascent literature on the prevalence and correlates of depressive and anxiety symptoms among vulnerable young people in SA.[4,5,16] Overall, our results demonstrate the link between Mandrax and the frequency of depressive symptoms among AGYW in SA. Recently, this population has received much attention related to the need for HIV prevention because of the high incidence among this group. Also, access to reproductive health services to reduce unintended pregnancy among AGYW is of great concern in SA. Substance use has often been examined in the context of sexual risk behaviour. However, our findings suggest that depressive symptoms may also be important in understanding substance use.
Clinical and policy implications and recommendations
These findings have practical and policy implications. Recently, there has been an increase in the demand for substance use treatment among young people, with 37% of patients being <25 years of age.[42] There have also been efforts by the SA government to increase the provision of youth-friendly services in public health clinics.[39] Our findings highlight the need to address substance use and mental health challenges among AGYW. Given that there is a need for substance use treatment centres to see young people and that public health clinics are providing more youth-friendly services, these may be ideal settings for integrated care to treat substance use and mental health disorders. However, currently, in Cape Town, there are few substance use treatment centres that can treat those under 18. The results of the current study suggest that government stakeholders should consider providing substance use treatment centres with the resources to increase their capacity to treat youth and incorporate mental health treatment into their efforts to meet the demands of an increasingly younger client base. Furthermore, key decision-makers should extend efforts to increase the provision of youth-friendly services to include substance use treatment facilities. Lastly, it may also be important to build the capacity of public health clinics to provide youth-friendly mental health and substance use treatment.
Conclusions
Our findings highlight how depressive symptoms may contribute to Mandrax use among SA AGYW. Efforts seeking to reduce substance use among AGYW may consider addressing mental health challenges, especially given the high rate of depression among this population. Key decision-makers may consider incorporating mental health treatment within substance use treatment centres and equipping these centres with the resources to provide youth-friendly services. Addressing substance use and mental health among AGYW may also help to curtail public health challenges such as HIV and unintended pregnancy.
Declaration. None.
Acknowledgements. We would like to acknowledge the contributions of the project staff and the young women who participated in the study.
Author contributions. All authors participated in the research and article preparation. WMW conceived of the study, oversaw drafts and finalised the manuscript; CPB conducted the analyses and led the development of the manuscript; TC, FAB, JWN and BNH contributed to writing and reviewing the manuscript.
Funding. This work was supported by the National Institutes of Health, National Institute on Drug Abuse under grant number R01DA041227-03S1. The funding source had no role in the analysis of the data, in writing the report or in the decision to submit the article for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. A portion of this paper was presented during a poster presentation at the NIDA, National Institute on Alcohol Abuse and Alcoholism (NIAAA), and National Institute of Mental Health (NIMH) Diversity Supplement Professional Development Workshop on April 8-9, 2019.
Conflicts of interest. None.
References
1. Reddy S, James S, Sewpaul R, et al. Umthente uhlaba usamila: The 3rd South African National Youth Risk Behaviour Survey 2011. Cape Town: South African Medical Research Council, 2013. [ Links ]
2. Peltzer K, Phaswana-Mafuya N. Drug use among youth and adults in a population-based survey in South Africa. S Afr J Psychiatr 2018;24:aa138. https://doi.org/10.4102/sajpsychiatry.v24i0.1139 [ Links ]
3. Morojele NK, Ramsoomar L. Addressing adolescent alcohol use in South Africa. S Afr Med J 2016;106(6):551-553. https://doi.org/10.7196/samj.2016.v106i6.10944 [ Links ]
4. Saban A, Flisher A, Laubscher R, London L, Morojele N. The association between psychopathology and substance use: Adolescent and young adult substance users in inpatient treatment in Cape Town, South Africa. Pan Afr Med J 2014;17(Suppl 1):8. https://doi.org/10.11694/pamj.supp.2014.17.1.3044 [ Links ]
5. Saban A, Flisher AJ. The association between psychopathology and substance use in young people: A review of the literature. J Psychoactive Drugs 2010;42(1):37-47. https://doi.org/10.1080/02791072.2010.10399784 [ Links ]
6. Karim QA. Mental health of and substance use by adolescents. S Afr Med J 2016;106(6):547-548. https://doi.org/10.7196/SAMJ.2016.v106i6.11026 [ Links ]
7. Esmaeelzadeh S, Moraros J, Thorpe L, Bird Y. Examining the association and directionality between mental health disorders and substance use among adolescents and young adults in the US and Canada - a systematic review and meta-analysis. J Clin Med 2018;7(12):543. https://doi.org/10.3390/jcm7120543 [ Links ]
8. Cheng Y, Li X, Lou C, et al The association between social support and mental health among vulnerable adolescents in five cities: Findings from the study of the well-being of adolescents in vulnerable environments. J Adolesc Health 2014;55(6 Suppl):S31-S38. https://doi.org/10.1016/j.jadohealth.2014.08.020 [ Links ]
9. Kleintjes S, Flisher A, Fick M, et al The prevalence of mental disorders among children, adolescents and adults in the Western Cape, South Africa. Afr J Psychiatry 2006;9(3):157-160. https://doi.org/10.4314/ajpsy.v9i3.30217 [ Links ]
10. Tomlinson M, Grimsrud AT, Stein DJ, Williams DR, Myer L. The epidemiology of major depression in South Africa: Results from the South African stress and health study. S Afr Med J 2009;99(5 Pt 2):367-373. [ Links ]
11. Abdool Karim SS. Understanding high rates of HIV in young women in Africa: Implications of new epidemiological, phylogenetic, genomic and proteomic evidence. Oral presentation presented at AIDS 2016, Durban, South Africa. 2016. [ Links ]
12. Statistics South Africa. South Africa Demographic and Health Survey 2016 Key Indicators Report. Pretoria, South Africa, and Rockville, Maryland, USA: National Department of Health, Stats SA, SAMRC, and ICF, 2017. [ Links ]
13. Pluddemann A, Flisher AJ, Mathews C, Carney T, Lombard C. Adolescent methamphetamine use and sexual risk behaviour in secondary school students in Cape Town, South Africa. Drug Alcohol Rev 2008;27(6):687-692. https://doi.org/10.1080/09595230802245253 [ Links ]
14. Wechsberg WM, Jones HE, Zule W, et al. Methamphetamine ('tik') use and its association with condom use among out-of-school females in Cape Town, South Africa. Am J Drug Alcohol Abuse 2010;36(4):208-213. https://doi.org/10.3109/00952990.2010.493592 [ Links ]
15. Brawner BM, Gomes MM, Jemmott LS, Deatrick JA, Coleman CL. Clinical depression and HIV risk-related sexual behaviors among African-American adolescent females: unmasking the numbers. AIDS Care 2012;24(5):618-625. https://doi.org/10.1080/09540121.2011.630344 [ Links ]
16. Saban A, Flisher AJ, Grimsrud A, et al. The association between substance use and common mental disorders in young adults: Results from the South African Stress and Health (SASH) Survey. Pan Afr Med J 2014;17(Suppl 1):S11. https://doi.org/10.11694/pamj.supp.2014.17.1.3328 [ Links ]
17. Morris K, Parry C. South African methamphetamine boom could fuel further HIV. Lancet Infect Dis 2006;6(8):471. https://doi.org/10.1016/s1473-3099(06)70539-4 [ Links ]
18. McKetin R, Lubman DI, Lee NM, Ross JE, Slade TN. Major depression among methamphetamine users entering drug treatment programs. Med J Australia 2011;195(3):S51-S55. https://doi.org/10.5694/j.1326-5377.2011.tb03266.x [ Links ]
19. Carney T, Browne FA, Myers B, Kline TL, Howard B, Wechsberg WM. Adolescent female school dropouts who use drugs and engage in risky sex: Effects of a brief pilot intervention in Cape Town, South Africa. AIDS Care 2019;31(1):77-84. https://doi.org/10.1080/09540121.2018.1500008 [ Links ]
20. Dennis ML, Titus JC, White MK, Unsicker JI, Hodgkins D. Global appraisal of individual needs: Administration Guide for the GAIN and Related Measures. Bloomington, IL: Chestnut Health Systems, 2003. [ Links ]
21. Wechsberg WM. Revised Risk Behavior Assessment, Part I and Part II. Research Triangle Park, NC: Research Triangle Institute, 1998. [ Links ]
22. Chandler RK, Kahana SY, Fletcher B, et al Data collection and harmonization in HIV research: The Seek, Test, Treat and Retain initiative at the National Institute on Drug Abuse. Am J Public Health 2015;105(12):2416-2422. https://doi.org/10.2105/AJPH.2015.302788 [ Links ]
23. Simpson D, Chatham L. TCU/DATAR forms manual. Fort Worth, TX: Institute of Behavioral Research, Texas Christian University, 1995. [ Links ]
24. Wechsberg WM, Luseno W, Riehman K, Karg R, Browne F, Parry C. Substance use and sexual risk within the context of gender inequality in South Africa. Substance Use Misuse 2008;43(8-9):1186-1201. https://doi.org/10.1080/10826080801918247 [ Links ]
25. Johnson JE, Carney T, Kline T, Browne FA, Wechsberg WM. Incarceration history relative to health, substance use, and violence in a sample of vulnerable South African women: Implications for health services in criminal justice settings. Subst Abuse Rehabil 2012;3(Suppl 1):S59-S69. https://doi.org/10.2147/SAR.S21351 [ Links ]
26. Posel D. Race as common sense: Racial classification in twentieth-century South Africa. Afr Stud Rev 2001;44(2):87-114. http://www.jstor.org/stable/525576?origin=JSTOR-pdf (accessed 8 December 2020). [ Links ]
27. Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: Findings from the Global Burden of Disease Study 2010. Lancet 2013;382(9904):1575-1586. http://www.jstor.org/stable/525576?origin=JSTOR-pdf10.1016/S0140-6736(13)61611-6 [ Links ]
28. Mayosi BM, Flisher AJ, Lalloo UG, Sitas F, Tollman SM, Bradshaw D. The burden of non-communicable diseases in South Africa. Lancet 2009;374(9693):934-947. https://doi.org/10.1016/S0140-6736(09)61087-4 [ Links ]
29. Kessler RC, Angermeyer M, Anthony JC, et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization's World Mental Health Survey Initiative. World Psychiatr 2007;6(3):168-176. [ Links ]
30. Myers B, Carney T, Browne FA, Wechsberg WM. A trauma-informed substance use and sexual risk reduction intervention for young South African women: A mixed-methods feasibility study. BMJ Open 2019;9:e024776. https://doi.org/10.1136/bmjopen-2018-024776 [ Links ]
31. Peltzer K, Ramlagan S, Johnson BD, Phaswana-Mafuya N. Illicit drug use and treatment in South Africa: A review. Substance Use Misuse 2010;45(13):2221-2243. https://doi.org/10.3109/10826084.2010.481594 [ Links ]
32. McCarthy G, Myers B, Siegfried N, McCarthy G. Treatment for Methaqualone dependence in adults. Cochrane Database System Rev 2005;18(2):CD004146. https://doi.org/10.1002/14651858.CD004146.pub2 [ Links ]
33. Wechsberg WM, Myers B, Kline TL, Carney T, Browne FA, Novak SP. The relationship of alcohol and other drug use typologies to sex risk behaviors among vulnerable women in Cape Town, South Africa. J AIDS Clin Res 2012;S1(15):015. https://doi.org/10.4172/2155-6113.S1-015 [ Links ]
34. Edwards S, Reeves GM, Fishbein D. Integrative model of the relationship between sleep problems and risk for youth substance use. Curr Addict Rep 2015;2:130-140. https://doi.org/10.1007/s40429-015-0052-0 [ Links ]
35. Hien DA, Wells EA, Jiang H, et al. Multisite randomized trial of behavioral interventions for women with co-occurring PTSD and substance use disorders. J Consult Clin Psychol 2009;77(4):607-619. https://doi.org/10.1037/a0016227 [ Links ]
36. Baral IA, Bhagawati K. Post traumatic stress disorder and coping strategies among adult survivors of earthquake, Nepal. BMC Psychiatr 2019;19(118). https://doi.org/10.1186/s12888-019-2090-y [ Links ]
37. Lee JY, Brook JS, Finch SJ, Brook DW. Pathways from victimization to substance use: Post traumatic stress disorder as a mediator. Psychiatr Res 2016;237:153-158. https://doi.org/10.1016/j.psychres.2016.01.049 [ Links ]
38. Bhana A, Parry CD, Myers B, Pluddemann A, Morojele NK, Flisher AJ. The South African Community Epidemiology Network on Drug Use (SACENDU) project, phases 1 - 8 - cannabis and Mandrax. S Afr Med J 2002;92(7):542-547. [ Links ]
39. National Department of Health, South Africa. National Adolescent and Youth Friendly Health Services Strategy 2012. Pretoria: NDoH, 2012. [ Links ]
40. Hadland SE, Levy S. Objective testing: Urine and other drug tests. Child Adolesc Psychiatr Clin N Am 2016;25(3):549-565. https://doi.org/10.1016/j.chc.2016.02.005 [ Links ]
41. Liu RH. Important considerations in the interpretation of forensic urine drug test results. Forens Sci Rev 1992;4(1):51-65. [ Links ]
42. South African Community Epidemiology Network on Drug Use. Monitoring alcohol, tobacco, and other drug abuse treatment admissions in South Africa. September 2016 (phase 39) http://hdl.handle.net/20.500.11910/10200 (accessed 8 December 2020). [ Links ]
 Correspondence:
Correspondence:
C P Bonner
cpbonner@rti.org
Accepted 11 May 2020


{kind=link}
{kind=link}
{kind=link}