










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 no.8 Pretoria Ago. 2020
http://dx.doi.org/10.7196/SAMJ.2020.v110i8.13466
RESEARCH
Nicotine dependence, socioeconomic status, lifestyle behaviours and lifetime quit attempts among adult smokers in South Africa
O A Ayo-YusufI; O B OmoleII
IBDS, MPH, PhD; Africa Centre for Tobacco Industry Monitoring and Policy Research, Sefako Makgatho Health Sciences University, Pretoria, South Africa
IIMBBS, MCFP (SA), MMed (Fam Med); Division of Family Medicine, Department of Family Medicine and Primary Care, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Smoking cessation is a complex process influenced by factors such as smokers' nicotine dependence levels, socioeconomic status (SES) and other lifestyle behaviours. Little is known about these relationships in South Africa (SA).
OBJECTIVES. To explore the relationship between nicotine dependence, SES, lifestyle behaviours and lifetime quit attempts among adult smokers in SA.
METHODS. This study used data from 2 651 participants aged >16 years in the 2011 South African Social Attitudes Survey. Information on SES (measured by asset ownership), binge drinking, physical activity, fruit and vegetable intake, intention to quit smoking and lifetime quit attempts was extracted. Nicotine dependence was measured using the Heaviness of Smoking Index (HSI). All data were weighted to account for the complex survey design and to yield nationally representative estimates. Data analysis included binary logistic regression with high nicotine dependence (HND) defined as HSI >4 and lifetime quit attempts as separate outcomes.
RESULTS. The prevalence of smoking was 20.1% (31.6% for males and 9.5% for females), and was highest in the mixed-ancestry group (37.0%). Overall, 14.5% of smokers had HND, with a higher proportion in the high-SES group. The odds of HND increased with every 10 years of smoking history (odds ratio (OR) 2.05; 95% confidence interval (CI) 1.40 - 3.00) but decreased among participants who reported frequent physical activity (OR 0.4; 95% CI 0.18 - 0.86) and those who planned to quit (OR 0.37; 95% CI 0.19 - 0.75). Quit attempts were more likely among participants who reported frequent fruit and vegetable intake (OR 1.8; 95% CI 1.07 - 2.98) and less likely among those reporting binge drinking (OR 0.31; 95% CI 0.16 - 0.59) or assessed as having HND (OR 0.32; 95% CI 0.17 - 0.58).
CONCLUSIONS. Most adult smokers in SA have low nicotine dependence. However, the association of HND with high SES in this study suggests that although cessation treatment based on an integrated lifestyle behavioural intervention package may suffice for most smokers, a more intense cessation treatment package is needed for smokers of higher SES.
Smoking remains a leading cause of premature morbidity and mortality.[1] While most smokers wish to quit smoking,[2-3] the odds of a successful quit attempt decreases with higher nicotine dependence (HND).[4,5] Indeed, nicotine dependence measures such as the number of cigarettes smoked per day and smoking the first cigarette of the day within 30 minutes of awakening are strongly correlated with the intention and outcome of quit attempts.[6,7]
The relationship between nicotine dependence and smoking (or smoking cessation) is not simply linear but modulated by other influences such as socioeconomic status (SES) and other lifestyle behaviours that pose a risk to health.[8] In developed countries, not only do people of lower SES smoke more and have a higher level of nicotine dependence,[9] they are also less likely to quit than people of higher SES.[10] Smokers of high SES are less likely to have other smokers at home, and have unhindered access to smoking cessation treatments and social support and less likelihood of a relapse. In contrast, it is argued that those of lower SES are exposed to significantly greater sources of stress, have fewer supportive external resources and demonstrate less sense of agency for smoking cessation, and are therefore likely to need more intensive treatment support to make a successful quit attempt.[9] Lack of social support and neighbourhood disadvantage are prevalent among people of lower SES, promoting smoking and hindering smoking cessation. [8] While a lack of social support reduces self-efficacy and increases negative affect/stress, neighbourhood disadvantage disrupts social ties, exacerbates negative affect/stress, reduces a person's sense of agency and increases the use of harmful lifestyle behaviours to mitigate stress.[8]
Most smokers concurrently engage in other lifestyle behaviours that pose a risk to health, such as excessive alcohol intake, a sedentary lifestyle and an unhealthy diet.[11] Like smoking, these behaviours are important risk factors for morbidity and mortality in themselves, and apart from their combined effects to increase morbidity and mortality, they may also influence one another regarding the intensity of use and risk of negative behavioural outcomes during quit attempts. [12,13] For example, dual use of alcohol and cigarettes increases the risk of intense use and dependence on both substances, reduces the odds of making a quit attempt, and increases the risk of relapse.[3,14-16] Also, although evidence is sparse on the effect of physical exercise on alcohol use,[17] available data suggest that moderate and binge alcohol drinkers are more likely to smoke more, to experience failed cessation attempts and to relapse.[18] Conversely, not only is the adoption of a healthy lifestyle associated with a reduction in or reversal of poor health outcomes, but the adoption of one may increase uptake of the other. For instance, physical exercise that allows for the development of physical fitness has been reported to promote smoking cessation by acutely reducing cravings and withdrawal symptoms and increasing the latency period till the next cigarette.[17,19-20] Similarly, reductions in smoking have been found to be associated with simultaneous improvements in fruit and/or vegetable intake and physical exercise.[13,20]
Studies reporting on the influence of SES, nicotine dependence and the adoption of a healthy lifestyle on smoking cessation have mostly originated from developed countries.[20-22] These studies suggest that higher levels of nicotine dependence are associated with lower SES and concurrent engagement in unhealthy lifestyle behaviours. Although the above associations are not linear (but may be explained through several other sociobehavioural factors), they influence the initiation and outcomes of quit attempts adversely. It is not clear whether the findings of these studies can be generalised to developing countries, where different sociodemographic and smoking patterns exist. One of few studies conducted in the African region on the association of SES and tobacco use suggests that people of lower SES were more likely to be smokers.[21] This finding is reiterated by a recent systematic review focused on lifestyle behavioural risk factors in low- and lower-middle-income countries.[23] However, of the 75 studies included in this review, only 2 were conducted in Africa, indicating the paucity of nationally representative data on the relationship between SES and lifestyle behavioural health risks in the African region. Considering that the prevalence of both tobacco use and non-communicable diseases is on the increase in Africa, data on this relationship is important for developing national strategies for addressing both problems.
Objectives
To explore the influence of SES and other lifestyle behaviours on nicotine dependence and lifetime quit attempts among adult smokers in South Africa (SA).
Methods
Study design and population sample
This secondary data analysis involved a nationally representative sample of adult South Africans aged >16 years who participated in the 2011 South African Social Attitude Survey (SASAS). The dataset contained no personal identifiers. The detailed sampling procedure has been published[24,25] and involved a multistage cluster sampling technique used to obtain a representative sample of South Africans by population group and geographical location. Although the primary survey was part of the Human Sciences Research Council (HSRC)'s annual SASAS (N=3 003; 85% response rate) for 2011, this secondary data analysis was also part of another study that used only a sample of those who had complete data on the main variables of interest, namely smoking status and/or other lifestyle behaviours - binge drinking, physical activity, and fruit and/or vegetable intake (N=2 651). The primary sample was drawn from the master sample frame of the HSRC, from which 3 500 households/visiting points were randomly selected. One person was then randomly selected from each household, without replacement. Efforts were made to secure an interview with the selected person by making three visits before registering the person as non-responding.
Measures
Tobacco smoking, nicotine dependence and quit attempts
Current tobacco smokers were defined as respondents who reported that they were currently smoking hand-rolled or commercially manufactured cigarettes, cigars, pipes or water pipes daily or on some days. Participants were asked to indicate the number of years since they had started smoking, the number of cigarettes smoked per day (CPD) (subsequently coded as 0 (1 - 10), 1 (11 - 20), 2 (21 - 30) or 3 (>30)), and the time from waking up in the morning to smoking their first cigarette of the day (coded 3 (<5 minutes), 2 (6 - 30 minutes), 1 (31 - 60 minutes) or 0 (>60 minutes). The level of nicotine dependence among current smokers was assessed using the Heaviness of Smoking Index (HSI), a 6-point scale calculated from the CPD and the time to the first cigarette after awakening.[26] Smokers with scores of >4 were considered to have HND. A lifetime quit attempt among current smokers was defined as any response of 'once', 'twice' or 'three times or more' (v. 'never') to the question 'Have you ever tried to quit smoking?'
Other lifestyle risk behaviours
Frequent binge drinkers were defined as those who responded 'daily' or 'several times a week' to the question: 'How often to you drink four or more alcoholic drinks on the same day?' Similarly, the study participants were asked to indicate how often they did physical activity for at least 20 minutes that made them sweat or breathe more heavily than usual, and how often they ate fresh fruit and/or vegetables. The response options were 'never', 'once a month or less often', 'several times a month', 'several times a week' and 'daily'. As with binge drinking, those who indicated participation in physical activity and intake of fruit and/or vegetables several times a week or daily were considered frequently physically active and as frequently eating fresh fruit and/or vegetables, respectively.
Sociodemographic characteristics, general health status and health insurance coverage
The sociodemographic characteristics assessed included age, educational level (no schooling, lower than grade 12, grade 12, or higher than grade 12), sex (male or female), ethnicity in terms of self-identification as black African, coloured (of mixed ancestry), Indian/Asian or white, location of residence (urban or rural), and employment status ('never worked', 'worked in past 12 months but not currently' or 'currently working').
Socioeconomic status (SES) was derived from the Asset Index, a highly reliable tool for assessing SES with a Cronbach alpha of 0.91. This index was obtained from the best-fitting items, following a principal component analysis of owning several household items. These household items were an electric stove, television set, washing machine, microwave oven, DSTV/cable network, home theatre system, landline telephone, radio, DVD player, vacuum cleaner, fridge, hot running water, computer and car. For the purposes of our analysis, the asset scores were auto-ranked into tertiles, with the upper tertile representing those with the highest SES and the lowest tertile representing those with the lowest SES.
The study participants were also asked to rate their general health (coded 1 (excellent/very good/good) or 0 (fair/poor) and to indicate whether they had private health insurance.
Analyses
All data were weighted to account for the complex survey design and to yield nationally representative estimates. The proportions of the sample who were current smokers, who had HND, and who had ever made a quit attempt or planned to quit were determined. In addition, smokers were further stratified by the aforementioned sociodemographic characteristics and other lifestyle behaviours.
To determine factors associated with smoking, HND and quit attempts, multivariable-adjusted logistic regression analyses were performed, adjusting for age, smoking history (years), education, sex, ethnicity and location of residence. The level of significance was set at p<0.05. All analyses were performed with SPSS version 24 (IBM, USA).
Results
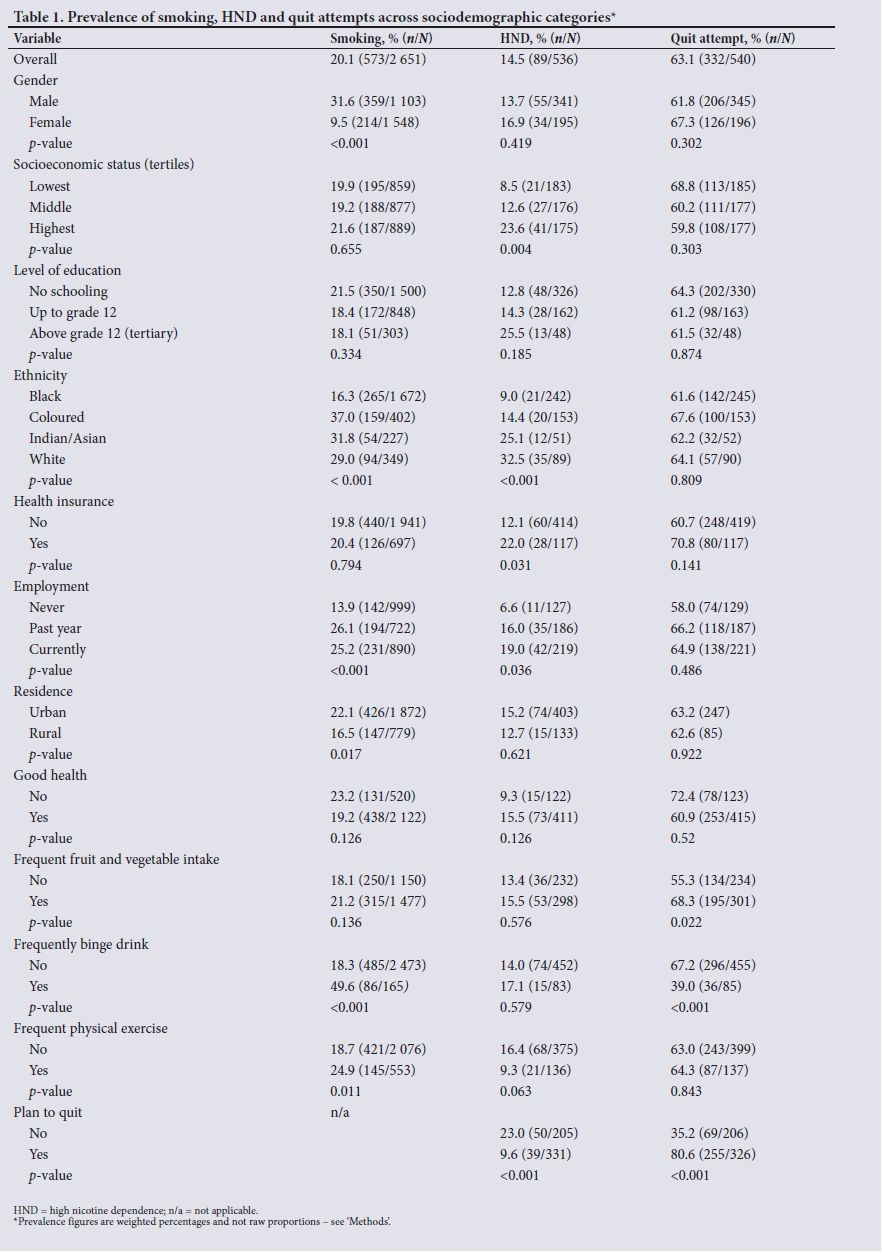
The prevalence of smoking among all participants was 20.1% (n=573), with a figure of 31.6% (359/1 103) for men and 9.5% (214/1 548) for women. Smoking rates were lowest among black Africans (16.3%) and highest among coloureds (mixed ancestry) (37.0%). Only 14.5% of smokers were found to have HND, with a higher proportion among smokers of high SES. All the other sociodemographic characteristics of those with HND and those who had made past quit attempts are shown in Table 1.
Table 2 shows factors that were independently associated with HND and past quit attempts. The odds of HND increased significantly with every 10 years of smoking history (odds ratio (OR) 2.05; 95% confidence interval (CI) 1.40 - 3.00) and being of high SES (OR 3.8; 95% CI 1.56 - 8.82). It decreased significantly with reported frequent physical activity (OR 0.4; 95% CI 0.18 - 0.86) and planning to quit (OR 0.37; 95% CI 0.19 - 0.75). Quit attempts were more likely among those who reported frequent fruit and/or vegetable intake (OR 1.8; 95% CI 1.07 - 2.98) and less likely among those who reported binge drinking (OR 0.31; 95% CI 0.16 - 0.59) or those assessed as having HND (OR 0.32; 95% CI 0.17 - 0.58).
Discussion
The study found that most participants had low nicotine dependence (LND) and that HND was independently associated with high SES, physical inactivity, no plans to quit, and a long smoking history. Similarly, reporting a past quit attempt was predicted by low SES, LND, infrequent alcohol intake and frequent fruit and/ or vegetable intake. These findings have clinical, policy and public health implications and suggest the necessity of integrating lifestyle modification interventions into nicotine dependence treatment in SA and other low-resource settings.
The finding that most smokers in this study had LND confirms the findings of previous community-based studies conducted in SA[27] and among mental health patients elsewhere in Africa.[28] More importantly, considering that smokers with LND are more likely than those with HND to quit and to do so without pharmacotherapy,[29] this finding suggests that most smokers in SA would be amenable to being assisted with counselling and/or behavioural therapy only. However, the 14.5% assessed as having HND (Table 1) amount to a considerable number of smokers at a population level and underscore the need for the SA health system to consider providing pharmacotherapy for smokers who are motivated to quit but may find it difficult to do so with non-pharmacological interventions alone.
In developed countries, smokers of low SES are likely to smoke more, to have higher levels of nicotine dependence, and to be less likely to want to quit.[29] While a recent study in Malawi had similar findings,[21] our study found the opposite. Smokers of high SES in our study were significantly more likely to have HND and lower odds of quit attempts. The explanation that smokers of lower SES smoke more because of their 'social disadvantages' and the need for 'anxiolysis' arising from social and financial stress[9] may therefore not hold true for SA. Rather, the observed relationship in our study may reflect the differential effects of price and tax increases on smokers across socioeconomic strata in SA,[30] meaning that smokers of higher
SES still find cigarettes affordable and continue to smoke at the same rate as previously, and therefore make fewer attempts to quit. Additional non-pharmacological and pharmacological interventions may therefore be necessary to promote smoking cessation effectively in this group of smokers.
In the present study, the odds of HND increased with a longer smoking history, but decreased with increasing age. Taken together, these findings may imply that those who started smoking at an early age (although they may still be young) and have a longer smoking history are more likely to have HND. Indeed, previous studies have suggested that smoking initiation at an earlier age is significantly associated with a higher level of nicotine dependence.[31] On the other hand, the lower likelihood of HND with increasing age may partly be explained by the increased likelihood of comorbidity in later life, which may motivate older smokers to reduce their cigarette consumption.
In the present study, smokers who planned to quit were more likely to have made a quit attempt in the past, suggesting that past experiences may reinforce the need for future quit attempts. Planning has also been shown to increase the chances of positive experience and success in future quit attempts.[32] Planning should be encouraged among smokers who are motivated to quit and should include setting a quit date, exploring how to navigate barriers, and recruiting resources needed for support during the actual quit attempt.
Although the mechanism is not entirely clear, regular physical exercise, especially of moderate and vigorous intensity, may affect regulatory changes in the neurotransmitters that affect cravings, mood, endogenous rewards and relapse prevention.[33] Our findings support this suggestion and motivate for the adoption of physical exercise as an effective smoking cessation intervention,[17] particularly when most smokers are light smokers (and may not need pharmacotherapy) and in poorly resourced settings where access to pharmacotherapy is limited. Furthermore, the clinical benefits of physical exercise may extend beyond smoking cessation, since smokers of higher SES are more likely not only to have HND but also to be more physically inactive and therefore at risk of non-communicable diseases.[23]
Smokers who frequently binge drink alcohol were less likely to report making a quit attempt than those who did not binge drink, consistent with previous studies reporting that concurrent alcohol dependence may make smoking cessation difficult and may facilitate a relapse.[18,27] Addressing alcohol intake and other forms of co-dependence is therefore of crucial importance among SA smokers, most of whom, being light smokers, have a reasonable chance of successful cessation if they are supported, but who may be unable to quit if there is concurrent alcohol intake. Indeed, alcohol consumption is known to be significantly associated with increased positive smoking outcome expectancies that may increase the urge to smoke and make cessation less successful during a quit attempt.[34] This relationship is particularly important among smokers who drink higher amounts of alcohol before a quit attempt, since they are also significantly more likely to continue to drink more after quitting - a behaviour that may reduce the odds of success during a quit attempt and increase relapse thereafter.[35] However, the lack of a significant association between binge drinking and HND in the present study suggests that smokers continue to smoke for reasons unrelated to the negative effect of alcohol on nicotine dependence. It is also possible that smokers who binge drink also smoke more and would score higher on the nicotine dependence scale, especially the components related to social and environmental influences, which were not included in measuring nicotine dependence in this study. The latter explanation may support our hypothesis that the effects of binge drinking are not related to nicotine dosing but to other factors such as making fewer quit attempts.[18]
The finding of a positive relationship between smoking cessation and frequent fruit and/or vegetable intake in the present study aligns with what has been reported previously[13] Although this relationship has been explained by a possible antidepressive effect of fruit and/or vegetable intake mediated via monoamine oxidase inhibition,[36] it may also be due to a 'gateway effect',[12] the adoption of one positive behaviour (such as healthy eating) promoting the attainment of another (such as quitting smoking) through reinforced motivation or improved confidence. This understanding could be used by healthcare providers to exploit positive spin-offs in one good behaviour such as frequent fruit and vegetable intake, to promote cessation of other undesirable lifestyle behaviours such as smoking.
Study limitations
This study has some potential limitations. Although it used the HSI, which has been validated as a highly sensitive tool for assessing nicotine dependence across several populations, its reliance on self-reporting may have led to information and social desirability biases that could affect several outcome estimates. Moreover, a little over 10% of the respondents had missing data, creating potential respondent bias. However, our sensitivity analysis showed no significant difference in sociodemographic characteristics between respondents with complete data and those without (data not displayed). Regardless of these limitations, the study used a large and nationally representative sample, and as far as the authors could ascertain, provides the first evidence in the African region on the influence of SES and other lifestyle behaviours (alcohol use, fruit and/ or vegetable intake and physical activity) on nicotine dependence and lifetime quit attempts among adult smokers.
Conclusions
The study demonstrates that most adult smokers in SA have a low level of nicotine dependence, and an integrated lifestyle behavioural modification intervention package (avoiding alcohol misuse, engaging in regular physical exercise and frequent intake of fruit and/or vegetables) may promote quit attempts and play a significant role in nicotine dependence treatment in this and similar settings. However, the independent association of HND with high SES highlights the need to target this population subset for more intense smoking cessation interventions.
Declaration. None.
Acknowledgements. The authors acknowledge the SASAS for granting access to the datasets.
Author contributions. OAA was involved in the conceptualisation, data analysis and manuscript development, and approved the final draft. OBO was involved in the data analysis and manuscript development and approved the final draft.
Funding. National Research Foundation grant to OAA (grant no. 93093).
Conflicts of interest. None.
References
1. Omole OB, Ngobale KNW, Ayo-Yusuf OA. Missed opportunities for tobacco use screening and brief cessation advice in South African primary health care: A cross-sectional study. BMC Fam Pract 2010;11:94. https://doi.org/10.1186/1471-2296-11-94 [ Links ]
2. Du Plooy J, Macharia M, Verster C. Cigarette smoking, nicotine dependence and motivation to quit in South African male psychiatric inpatients. BMC Psychiatry 2016;16:403. https://doi.org/10.1186/s12888-016-1123-z [ Links ]
3. Myung S, Seo1 HG, Cheong Y, Park S, Lee WB, Fong GT. Association of sociodemographic factors, smoking-related beliefs, and smoking restrictions with intention to quit smoking in Korean adults: Findings from the ITC Korea Survey. J Epidemiol 2012;22(1):21-27. https://doi.org/10.2188/jea.JE20110026 [ Links ]
4. Zhou X, Nonnemaker J, Sherrill B, Gilsenan AW, Coste F, West R. Attempts to quit smoking and relapse: Factors associated with success or failure from the ATTEMPT cohort study. Addict Behav 2009;34(4):365-373. https://doi.org/10.1016/j.addbeh.2008.11.013 [ Links ]
5. Hyland A, Borland R, Li Q. Individual-level predictors of cessation behaviours among participants in the International Tobacco Control (ITC) Four Country Survey. Tob Control 2006;15(Suppl III):iii83-iii94. https://doi.org/10.1136/tc.2005.013516 [ Links ]
6. Fagan P, Augustson E, Backinger CL, et al. Quit attempts and intention to quit cigarette smoking among young adults in the United States. Am J Public Health 2007;97(8):1412-1420. https://doi.org/10.2105/AJPH.2006.103697 [ Links ]
7. Papadakis S, Tulloch HE, Gharib M, Pipe AL. Profile of tobacco users identified in primary care practice and predictors of readiness to quit: A cross-sectional survey. CMAJ Open 2016;4(1):E41-E47. https://doi.org/10.9778/cmajo.20150055 [ Links ]
8. Businelle MS, Kendzora DE, Reitzela LR, et al. Mechanisms linking socioeconomic status to smoking cessation: A structural equation modeling approach. Health Psychol 2010;29(3):262-273. https://doi.org/10.1037/a0019285 [ Links ]
9. Siahpush M, Borland R, Yong H. Sociodemographic and psychosocial correlates of smoking induced deprivation and its effect on quitting: Findings from the International Tobacco Control Policy Evaluation Survey. Tob Control 2007;16:e2. https://doi.org/10.1136/tc.2006.016279 [ Links ]
10. Moshin M, Bauman AE. Socio-demographic factors associated with smoking and smoking cessation among 426,344 pregnant women in New South Wales, Australia. BMC Public Health 2005;5:138. https://doi.org/10.1186/1471-2458-5-138 [ Links ]
11. Chiolero A, Wietlisbach V, Ruffieux C, Paccaud F, Cornuz J. Clustering of risk behaviors with cigarette smoking: A population-based survey. Prev Med 2006;42(5):348-353. https://doi.org/10.1016/j.ypmed.2006.01.011 [ Links ]
12. Paul C, Tzelepis F, Bisquera A, Noble N, Wiggers J. Just how high-risk are ongoing smokers? Exploring clusters of health risk behaviours among current and ex-smokers. Prev Med 2016;93:70-75. https://doi.org/10.1016/j.ypmed.2016.09.021 [ Links ]
13. Meader N, King K, Wright K, et al. Multiple risk behavior interventions: Meta-analyses of RCTs. Am J Prev Med 2017;53(1):e19-e30. https://doi.org/10.1016/j.amepre.2017.01.032 [ Links ]
14. Businelle MS, Lam CY, Kendzor D, et al. Alcohol consumption and urges to smoke among women during a smoking cessation attempt. Exp Clin Psychopharmacol 2013;21(1):29-37. https://doi.org/10.1037/a0031009 [ Links ]
15. Brown J, West R, Beard E, et al. Are recent attempts to quit smoking associated with reduced drinking in England? A cross-sectional population survey. BMC Public Health 2016;16:535. https://doi.org/10.1186/s12889-016-3223-6 [ Links ]
16. Kim Y. Predictors for successful smoking cessation in Korean adults. Asian Nurs Res 2014;8(1):1-7. https://doi.org/10.1016/j.anr.2013.09.004 [ Links ]
17. Zschucke E, Heinz A, Strohle A. Exercise and physical activity in the therapy of substance use disorders. Sci World J 2012; Article ID 901741. https://doi.org/10.1100/2012/901741 [ Links ]
18. Cook JW, Fucito LM, Piasecki TM, et al. Relations of alcohol consumption with smoking cessation milestones and tobacco dependence. J Consult Clin Psychol 2012;80(6):1075-1085. https://doi.org/10.1037/a0029931 [ Links ]
19. Haasova M, Warren FC, Ussher M, et al. The acute effects of physical activity on cigarette cravings: Systematic review and meta-analysis with individual participant data. Addiction 2013;108(1):26-37. https://doi.org/10.1111/j.1360-0443.2012.04034.x [ Links ]
20. Berg CJ, Thomas JL, Lawrence CA, et al. Change in smoking, diet, and walking for exercise in blacks. Health Educ Behav 2012;39(2):191-197. https://doi.org/10.1177/1090198111432252 [ Links ]
21. Yaya S, Bishwajit G, Shah V, Ekholuenetale M. Socioeconomic disparities in smoking behaviour and early smoking initiation among men in Malawi. Tob Use Insights 2017;10:1-7. https://doi.org/10.1177/1179173X17726297 [ Links ]
22. Levy DT, Romano E, Mumford E. The relationship of smoking cessation to sociodemographic characteristics, smoking intensity, and tobacco control policies. Nicotine Tob Res 2005;7(3):387-396. https://doi.org/10.1080/14622200500125443 [ Links ]
23. Allen L, Williams J, Townsend N, et al Socioeconomic status and non-communicable disease behavioural risk factors in low-income and lower-middle income countries: A systematic review. Lancet Glob Health 2017;5:e277-789. https://doi.org/10.1016/S2214-109X(17)30058-X [ Links ]
24. Ayo-Yusuf IJ, Naidoo S. Social gradient in the cost of oral pain and related dental service utilisation among South African adults. BMC Oral Health 2016;16:117. https://doi.org/10.1186/s12903-016-0313-x [ Links ]
25. Olutola BG, Ayo-Yusuf OA. Socio-environmental factors associated with self-rated oral health in South Africa: A multilevel effects model. Int J Environ Res Public Health 2012;9(10):3465-3483. https://doi.org/10.3390/ijerph9103465 [ Links ]
26. Heatherton TF, Kozlowski LT, Frecker RC, Rickert W, Robinson J. Measuring the heaviness of smoking: Using self-reported time to the first cigarette of the day and number of cigarettes smoked per day. Br J Addict 1989;84(7):791-799. https://doi.org/10.1111/j.1360-0443.1989.tb03059.x [ Links ]
27. Ayo-Yusuf OA, Szymanski B. Factors associated with smoking cessation in South Africa. S Afr Med J 2010;100(3):175-179. [ Links ]
28. Molla Z, Dube L, Krahl W, Soboka M. Tobacco dependence among people with mental illness: A facility-based cross sectional study from Southwest Ethiopia. BMC Res Notes 2017;10:289. https://doi.org/10.1186/s13104-017-2608-7 [ Links ]
29. Chandola T, Head J, Bartley M. Socio-demographic predictors of quitting smoking: How important are household factors? Addiction 2004;99(6):770-777. https://doi.org/10.1111/j.1360-0443.2004.00756.x [ Links ]
30. Van Walbeek C, Blecher E, Gilmore A, Ross H. Price and tax measures and illicit trade in the Framework Convention on Tobacco Control: What we know and what research is required. Nicotine Tob Res 2013;15(4):767-776. https://doi.org/10.1093/ntr/nts170 [ Links ]
31. Benowitz NL. Nicotine addiction. N Engl J Med 2010;362(24):2295-2303. https://doi.org/10.1056/NEJMra0809890 [ Links ]
32. Balmford J, Swift E, Borland R. Reported planning before and after quitting and quit success: Retrospective data from the ITC 4-Country Survey. Psychol Addict Behav 2014;28(3):899-906. https://doi.org/10.1037/a0035711 [ Links ]
33. Haasova M, Warren FC, Ussher M, et al. The acute effects of physical activity on cigarette cravings: Exploration of potential moderators, mediators and physical activity attributes using individual participant data (IPD) meta-analyses. Psychopharmacology (Berl) 2014;231:1267-1275. https://doi.org/10.1007/s00213-014-3450-4 [ Links ]
34. Lam CY, Businelle MS, Cofta-Woerpel L, McClure JB, Cinciripini PM, Wetter DW. Positive smoking outcome expectancies mediate the relation between alcohol consumption and smoking urge among women during a quit attempt. Psychol Addict Behav 2014;28(1):163-172. https://doi.org/10.1037/a0034816 [ Links ]
35. Berg KM, Piper ME, Smith SS, Fiore MC, Jorenby DE. Defining and predicting short-term alcohol use changes during a smoking cessation attempt. Addict Behav 2015;48:52-57. https://doi.org/10.1016/j.addbeh.2015.04.004 [ Links ]
36. Haibach JP, Homish GG, Collins L, Ambrosone CB, Giovino GA. Fruit and vegetable intake as a moderator of the association between depressive symptoms and cigarette smoking. Subst Abuse 2016;37(4):571-578. https://doi.org/10.1080/08897077.2016.1179703 [ Links ]
 Correspondence:
Correspondence:
O B Omole
alagbaomole@gmail.com
Accepted 20 February 2020.


{kind=link}
{kind=link}