










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 n.8 Pretoria Aug. 2020
http://dx.doi.org/10.7196/SAMJ.2020.v110i8.14881
REVIEW
Diabetes mellitus and COVID-19: A review and management guidance for South Africa
A CoetzeeI; J J TaljaardII; S S HugoIII; M ConradieIV; M Conradie-SmitV; J A DaveVI
IMB ChB, FCP, MMed (Internal Medicine), Cert Endocrinology and Metabolism (SA), MPhil (Endocrinology); Division of Endocrinology, Department of Medicine, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
IIMB ChB, MMed (Internal Medicine), DTM&H; Department of Medicine and Centre for Infectious Diseases, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
IIIMB ChB, Dip HIV Man (SA); Department of Medicine and Centre for Infectious Diseases, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
IVMB ChB, PhD (Endocrinology); Division of Endocrinology, Department of Medicine, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
VMB ChB, FCP, MMed (Internal Medicine), Cert Endocrinology and Metabolism (SA); Division of Endocrinology, Department of Medicine, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
VIMB ChB, FCP, Cert Endocrinology and Metabolism (SA), PhD Division of Endocrinology, Department of Medicine, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
This article reviews the association between diabetes mellitus (DM) and COVID-19. We report on the convergence of infectious diseases such as coronavirus infections and non-communicable diseases including DM. The mechanisms for the interaction between COVID-19 and DM are explored, and suggestions for the management of DM in patients with COVID-19 in South Africa are offered.
Diabetes mellitus (DM), cancer, cardiovascular diseases and chronic respiratory diseases, collectively referred to as non-communicable diseases (NCDs), are the leading causes of mortality worldwide. DM is a major driving force behind the escalating prevalence of NCDs and the increasing mortality and morbidity attributable to them, especially in lower- and middle-income regions. A predisposition to development and poor outcome of infectious diseases in the presence of NCDs has been noted and explains the association between DM and both tuberculosis (TB) and HIV infection.[1,2] DM places an enormous burden on health budgets and health systems globally. This is especially concerning in South Africa (SA), where the healthcare system is not only overwhelmed by the escalating prevalence of DM, but carries an additional burden of disease due to TB and HIV.
The COVID-19 pandemic is infamous for crippling healthcare systems. Environments with limited resources are particularly vulnerable.[3] The mismatch between healthcare demand and supply in SA predates the COVID-19 pandemic.[4] With the expected widespread community transmission of SARS-CoV-2 infection in SA, preparedness will depend on the implementation of equitable and effective strategies derived from the experiences of countries that are up front in the COVID-19 fight.[5-7] Increased morbidity and mortality from COVID-19 in patients with DM have been noted in countries hardest hit by the pandemic, and this association and the optimal management of infected patients with DM deserve close scrutiny.
DM is one of the leading causes of morbidity and mortality worldwide, mostly attributed to cardiovascular disease (CVD).[8] Globally, DM and obesity accounted for 43.4% of all deaths in 2012, compared with 33.6% of deaths from HIV/AIDS and TB combined.[8,9] In SA, high body mass indexes (BMIs) and DM are the second and third leading risk factors for early death and disability, respectively, and the increasing overlap with infectious diseases is a growing concern.[10-12] When the co-presence of COVID-19 and NCDs was investigated in Italy, hypertension and DM were identified as the two most prevalent comorbidities with rates of 73.8% and 33.9%, respectively, DM being three times more prevalent in patients with severe COVID-19 than in the background population.[13]In 2019, the International Diabetes Federation reported a DM prevalence of 12.8% in SA adults (20 - 79 years), but cautioned that this may be an underestimate, as DM in Africa remains largely undiagnosed (3/5 persons with DM; 60%).[14] Based on available evidence from China and Italy, people living with diabetes (PLWD) do not have an increased risk of being infected with SARS-CoV-2, as the prevalence of COVID-19 in PLWD was similar to that of the background population in these geographical areas.[15,16]
Assessment of the impact of the convergence of these two diseases in SA will be challenging. Many PLWD remain undiagnosed in this country, limiting the ability to truly estimate the background prevalence of DM. There are also people with SARS-CoV-2 infection who remain asymptomatic. There are theoretical reasons why PLWD may be at increased risk of acquiring SARS-CoV-2 infection and potentially have a more severe and complicated disease course. In general, PLWD are at increased risk of infections due to an impaired immune response with reductions in cytokines, T-cell activation, neutrophil function and macrophage activity.[17,18] DM is also a chronic inflammatory condition that in itself is associated with adverse outcomes.[19] The vast majority of patients in our setting with type 2 DM (T2DM) are obese, and obesity was identified as an independent risk factor for severe infection during the influenza A H1N1 epidemic in 2009.[20] Obesity is associated with respiratory problems that include reduced ventilation of basal lung segments, ventilation-perfusion mismatches and suboptimal blood oxygenation, all of which can potentially contribute to the complexities involved in managing PLWD who have COVID-19.[21]
DM and coronaviruses
DM was a risk factor for severe disease and excess mortality in severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), and the associated viruses were found to be an aetiological factor in the development of DM by damaging pancreatic islet cells.[22-25] Based on the experience with SARS and MERS, it is anticipated that DM will predispose to increased severity of COVID-19. Infection with SARS-CoV-2 may also adversely affect endocrine pancreatic function and worsen glycaemic control. The reported prevalence of DM in people with COVID-19 varies and is influenced by geographical area, age of the population and severity of disease. A meta-analysis of 12 studies that included 2 108 Chinese patients with COVID-19 noted a DM prevalence of 10.3%, a figure not dissimilar to the known prevalence of diabetes in the background general population.[15] However, the disease was notably more severe and the mortality rate higher in PLWD in China. This finding is supported by a report by Yang et al.,[26] who showed the prevalence of DM in patients requiring intensive care unit (ICU) admission for severe COVID-19 to be as high as 22%. Studies from China documented an overall mortality rate of 2.3%, compared with a three times higher mortality rate of 7.3% in PLWDJ2728 Similarly, in Italy, Grasselli et al.[29] reported a high prevalence of DM (17%) in 1 591 patients infected with SARS-CoV-2 who required ICU admission. The reported prevalence in Italy increased even further to a very concerning 35.5% of PLWD who had a fatal outcome following ICU admission.[301 In a case series of 5 700 hospitalised patients in the New York City area, the most common comorbidities were hypertension (n=3 026; 56.6%), obesity (n=1 737; 41.7%) and DM (n=1 808; 33.8%).[31] Compared with patients without DM, PLWD had a more protracted illness, there was a longer period of viral shedding, the requirement for mechanical ventilation increased, and more deaths were reported.[32]
Effect of abnormal glucose on outcome with COVID-19
Hyperglycaemia is a robust predictor of severity of illness and mortality in patients infected with various viruses, including influenza A (H1N1), SARS and MERS, in part owing to the catecholamine response associated with systemic infections.[22-241 Poorly controlled DM and chronic hyperglycaemia are linked to defects in lymphocyte proliferation as well as impaired monocyte/macrophage and neutrophil function.[171 Furthermore, hyperglycaemia in the pulmonary vasculature at the time of infection has been shown to increase local influenza viral replication in lung tissue.[331 Poor DM control is therefore expected to predispose to infection and a more adverse outcome with increased complications in persons exposed to the SARS-CoV-2 virus. DM and/or uncontrolled hyperglycaemia (defined as two or more blood glucose levels >10 mmol/L/24 h) in 1 122 hospitalised patients was associated with increased mortality and a longer hospital stay in an observational study in the USA.[341 In the same study, a mortality rate of 28.8% was noted in patients with uncontrolled hyperglycaemia (with or without known DM; n=570) compared with 6.2% mortality in the absence of these comorbidities. Among the 184 patients with known DM, 40 of 96 (41.7%) with uncontrolled hyperglycaemia died, compared with 13 of 88 (14.8%) patients with DM that was controlled.[34] An analysis of COVID-19-related hospital deaths in the linked electronic health records of over 17 million adult National Health Service patients showed increasing BMI, DM and poorly controlled DM to be associated with increased mortality.[35]
Glycated haemoglobin (HbA1c) reflects mean glucose status for the preceding 12 weeks. It does not replace glucose monitoring in the acutely ill, but is a reliable indicator of the glycaemic environment prior to the onset of an illness or disease process.[36] Measured HbA1c has been validated for case finding for DM in hospitalised patients.[371 HbA1c-based score models have been used to predict cardiovascular outcome and mortality in PLWD and may prove to be a useful aid in defining risk and allocating resources in PLWD who have COVID-19.
Conversely, a retrospective study from Wuhan reported that ~10% of patients with T2DM and SARS-CoV-2 infection experienced at least one episode of hypoglycaemia (<3.9 mmol/L).[38] Since hypoglycaemia is a predictor of an adverse outcome, partly attributable to a robust inflammatory response with consequences such as hypercoagulability and cardiac arrhythmias, it would also be important to avoid it when managing PLWD who are infected with SARS-CoV-2.
Obesity is causally related to hypertension, T2DM and cardiovascular diseases, and was also associated with adverse outcome during the H1N1 pandemic.[39] A retrospective study from France indicated that the odds ratio for mechanical ventilation in COVID-19 patients categorised as severely obese (BMI >35 kg/m2) was 7.36 (p=0.02) compared with individuals with a BMI in the normal weight category (<25 kg/m2).[40] Multivariate analysis confirmed the association to be independent of age, T2DM status and hypertension.[401 Restricted pulmonary function, immunological aberrations including raised interleukin-6 and other pro-inflammatory cytokines, chronic low-grade inflammation and hypercoagulability are all implicated as potential contributors to the adverse outcome in the obese.[39] The level of human angiotensin-converting enzyme 2 (ACE2) receptor expression in adipose tissue is higher than in lung tissue, and obese individuals consequently have a larger total amount of ACE2.[41] While obesity and DM are intricately linked and both are associated with more severe COVID-19, glucose control is generally achievable in a shorter time period than weight loss. Well-controlled blood glucose was correlated with improved 28-day outcomes following admission for COVID-19 in individuals with T2DM and the in-hospital death rate was reduced ten-fold (1.1% v. 11%) compared with individuals with uncontrolled blood glucose.[42]
Management of PLWD without current COVID-19
Poor glycaemic control in DM is associated with more severe infectious disease, including pneumonia and other bacterial infections.[43]In vitro exposure of pulmonary epithelial cells to elevated glucose concentrations significantly increased influenza virus infection and replication in a dose-response fashion, suggesting that hyperglycaemia may increase viral replication.[33] Higher HbA1c values (>7.5%) reflecting suboptimal glucose control before COVID-19 were associated with an increased risk (adjusted hazard ratio (AHR) 2.36; 95% confidence interval (CI) 2.18 - 2.56) of in-hospital deaths in England compared with HbA1c values <7.5% (AHR 1.5; 95% CI 1.40 - 1.60).[35] It is therefore advised that glucose control should be prioritised according to best practice guidelines. This is applicable to all PLWD with COVID-19.
Chronic management of DM and mild COVID-19
It is important that PLWD minimise their risk by being proactive with regard to both prevention strategies for SARS-CoV-2 infection and the control of comorbid medical conditions. The majority of PLWD with COVID-19 are likely to have mild disease that can be managed at home, provided they can adhere to public health measures and self-manage glycaemia. PLWD with mild COVID-19 who are recovering at home should consult their healthcare providers on effective blood glucose management. It is therefore important that clinicians caring for PLWD familiarise themselves with pharmacotherapy frequently used in PLWD and COVID-19. The disease course of patients with COVID-19 and DM is highly variable. It is therefore advised that the management plan, including use of glucose-lowering agents, is revisited with any change in clinical condition.
Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers
While outcomes remain to be clarified in SARS-CoV-2 infection, angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) have been shown to improve outcome in various subpopulations of PLWD.[44-46] The pathophysiological basis of concern regarding using ACE inhibitors in people infected with SARS-CoV-2 lies in the binding of SARS-CoV-2 to the ACE2 receptor, thereby gaining entry into target cells.[47] Under normal physiological conditions, ACE2 is expressed in the pulmonary epithelium, vasculature and intestine, and is upregulated in patients treated with ACE inhibitors and ARBs. It has therefore been suggested that increased ACE2 expression in PLWD could facilitate infection and increase severity.[48] While association does not prove causality, it is interesting to note that ACE inhibitor and ARB use in patients with hypertension admitted with SARS-CoV-2 infection in China were not associated with adverse outcomes.[49] At this time there are insufficient data to inform the clinician on whether these agents should or should not be used in PLWD who have COVID-19. However, there could potentially be more harm in stopping these agents, especially in patients with mild COVID-19 disease and concomitant hypertension, renal disease, heart failure and cardiovascular disease. Many societies, including the International Society of Hypertension and the European Society of Hypertension, are in agreement that, based on available evidence, ACE inhibitors and ARBs should not be discontinued in people with COVID-19.[50,51-
Oral glucose-lowering agents
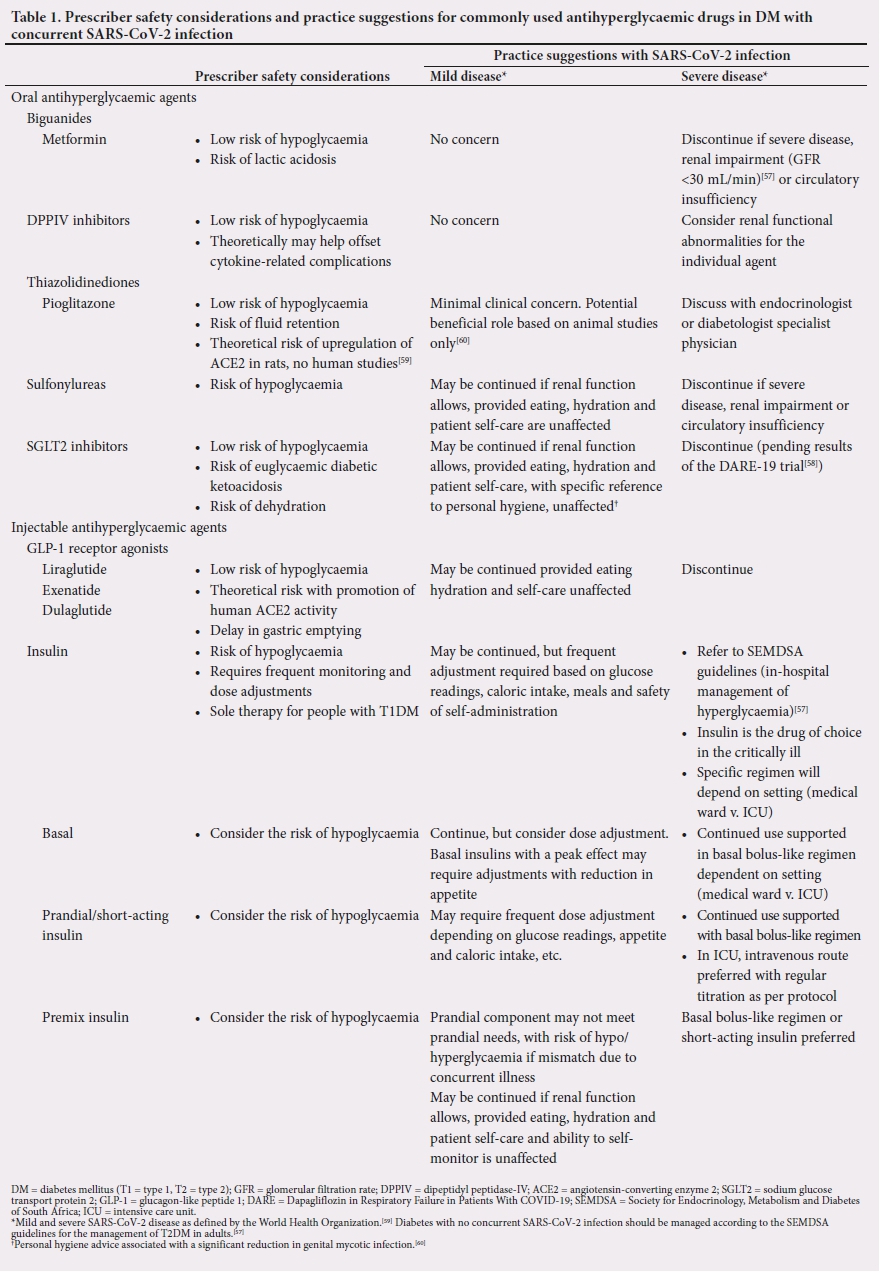
From an oral glucose-lowering perspective, metformin is a commonly used agent, and usually the foundation of the treatment cascade for managing patients with T2DM. Metformin has been shown to have anti-inflammatory properties, albeit with questionable clinical relevance, and can safely be continued in PLWD with mild concomitant COVID-19.[52] However, the risk/benefit ratio in individuals with severe illness favours discontinuation.[53] A dipeptidyl peptidase-IV (DPPIV) enzyme inhibitor is often used in the management of patients with T2DM. The DPPIV enzyme has been localised to type 1 and type 2 pneumocytes and has been shown to be increased in smoking and chronic lung disease and decreased in people with HIV and MERS.[54] The membrane-associated DPPIV receptor is a functional coronavirus receptor, and anti-DPPIV antibodies have been shown to decrease susceptibility to coronavirus infection.[55] Similarly, decreased expression of cell-surface DPPIV correlates with reduced disease susceptibility, suggesting that DPPIV inhibitors may have pathophysiological significance; however, genetic polymorphisms, adequate plasma levels and concomitant renal function in SARS-CoV-2 infection are among the undefined variables that remain to be resolved.[54] Glucagon-like peptide-1 (GLP-1) receptor agonists have been shown to have anti-inflammatory activity, and some in vitro data show a reduction in pulmonary inflammation and cytokine reduction.[54] However, there are no data on their safety and efficacy in PLWD who have COVID-19. The same is true for sulfonylureas and sodium glucose transport 2 (SGLT2) inhibitors. Acute kidney injury can develop at any time during COVID-19, and this should be considered when antihyperglycaemic agents are prescribed. Kidney injury may be due to indirect causes such as volume depletion, direct injury due to glomerular or tubular infection with SARS-CoV-2, thrombosis and rhabdomyolysis.[56] The safety of many antihyperglycaemic drugs is compromised in the presence of renal impairment, albeit to a varying extent. As glomerular filtration rate (GFR) cut-offs differ between and within antihyperglycaemic classes and agents, it is advised that prescribers familiarise themselves with the GFR cut-offs of the specific therapeutic agent and/or drug class used. Since COVID-19 has a wide spectrum of disease severity, the treating clinician will have to optimise glycaemic control using clinical judgement as well as obeying the standard contraindications for each drug class. Prescriber safety considerations for the use of antihyperglycaemic agents in PLWD with COVID-19 are addressed in Table 1.
In-hospital management of DM and SARS-CoV-2 infection
There are currently no robust data from randomised controlled trials detailing the optimal in-hospital care of patients with DM and SARS-CoV-2 infection. Observational studies emerging from areas of the world that have large numbers of patients with diabetes admitted with SARS-CoV-2 infection report a more complicated clinical course and a worse outcome in patients with DM, especially if the diabetes is poorly controlled. Furthermore, non-diabetic patients with hyperglycaemia have higher mortality than those with normoglycaemia.[34] These studies also suggest a high prevalence of diabetic ketoacidosis (DKA), which is not unexpected in patients with infection, but what seems to be unique is that the DKA is occurring at or slightly above normal glucose values.[61] The contribution of ketosis due to anorexia and a metabolic acidosis due to severe dehydration and sepsis is difficult to dissect out from the presentation of DKA at this time.[62] Data indicating that optimal control of glycaemia in PLWD before and during admission with SARS-CoV-2 infection improves outcome are emerging.[34,35,43] Clinicians must attempt to optimise blood glucose control in these patients while limiting the risk of hypoglycaemia and weight gain. Since many of these patients are admitted with anorexia and clinical signs of dehydration and infection, the optimal method of control in these patients would be administration of subcutaneous or intravenous insulin, depending on the clinical status of the patient and resources. Considering the infection risk, it would be best to limit exposure of healthcare workers by empowering PLWD with SARS-CoV-2 infection to perform self-monitoring of blood glucose and self-administer insulin if clinical status permits. The ongoing use of oral medication depends on the clinical status of the patient, the expected adverse effects of the specific agent, and glucose readings. It would be preferable to discontinue agents with an added risk of hypoglycaemia, dehydration and acidosis in PLWD and severe SARS-CoV-2 infection. Additionally, clinical vigilance should prevail with regard to variation in renal function, use of radiographic contrast agents, and factors increasing the likelihood of a suboptimal outcome. Furthermore, clinicians may encounter PLWD who receive therapeutic agents directed at SARS-CoV-2 that affect glucose levels per se, requiring an adjustment of antidiabetic medication. The drugs directed at SARS-CoV-2 that are expected to alter glucose levels include the immunomodulators and antiviral agents. From an immunomodulatory perspective, chloroquine/ hydroxychloroquine and glucocorticoids have opposing effects on blood glucose, with an increased risk of hypo- and hyperglycaemia, respectively. The antiviral agent lopinavir/ritonavir is associated with hyperglycaemia. Drug-drug interactions such as the concomitant use of statins and the antiviral agents lopinavir/ritonavir and remdesivir should also be carefully considered.
Conclusions
The convergence of the DM epidemic and COVID-19 pandemic will significantly increase the demands on the SA healthcare system. The available evidence identifies obesity, and hyperglycaemia in patients without diabetes, as well as poorly controlled DM as important modifiable host factors associated with adverse outcomes. Clinicians should remain vigilant with regard to the glucose fluctuations in SARS-CoV-2 infection and address them proactively. HbA1c determination at the time of diagnosis of COVID-19 and/or on admission may clarify DM status and allow for the early initiation of therapies to best manage hyperglycaemia.
Declaration. None.
Acknowledgements. None.
Author contributions. AC conceptualised and drafted the manuscript. JAD was the primary supervisor and provided external mentorship. JJT, SSH, MC and MC-S assisted with the preparation, creation and/or presentation of the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Levitt NS, Steyn K, Dave J, Bradshaw D. Chronic noncommunicable diseases and HIV-AIDS on a collision course: Relevance for health care delivery, particularly in low-resource settings - insights from South Africa. Am J Clin Nutr 2011;94(6):1690S-1696S. https://doi.org/10.3945/ajcn.111.019075 [ Links ]
2. Remais JV, Zeng G, Li G, Tian L, Engelgau MM. Convergence of non-communicable and infectious diseases in low- and middle-income countries. Int J Epidemiol 2013;42(1):221-227. https://doi.org/10.1093/ije/dys135 [ Links ]
3. Emanuel EJ, Persad G, Upshur R, et al. Fair allocation of scarce medical resources in the time of Covid-19. N Engl J Med 2020;382(21):2049-2055. https://doi.org/10.1056/NEJMsb2005114 [ Links ]
4. McIntyre D, Thiede M, Nkosi M, et al Shield Work Package 1 Report: A critical analysis of the current South African health system. 2006. http://dteseerx.istpsu.edu/viewdoc/download?doi=10.1.1.192.5891&rep=rep1&type=pdf (accessed 29 May 2020). [ Links ]
5. White DB, Lo B. A framework for rationing ventilators and critical care beds during the COVID-19 pandemic. JAMA 2020;323(18):1773-1774. https://doi.org/10.1001/jama.2020.5046 [ Links ]
6. Grasselli G, Pesenti A, Cecconi M. Critical care utilization for the COVID-19 outbreak in Lombardy, Italy: Early experience and forecast during an emergency response. JAMA 2020;323(16):1545-1546. https://doi.org/10.1001/jama.2020.4031 [ Links ]
7. Ji Y, Ma Z, Peppelenbosch MP, Pan Q. Potential association between COVID-19 mortality and health-care resource availability. Lancet Glob Health 2020;8(4):e480. https://doi.org/10.1016/S2214-109X(20)30068-1 [ Links ]
8. GBD 2016 Cause of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980 - 2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017;390(10100):1151-1210. https://doi.org/10.1016/S0140-6736(17)32152-9 [ Links ]
9. GBD 2017 Cause of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980 - 2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018;392(10159):1736-1788. https://doi.org/10.1016/S0140-6736(18)32203-7 [ Links ]
10. Pillay-van Wyk V, Msemburi W, Laubscher R, et al. Mortality trends and differentials in South Africa from 1997 to 2012: Second National Burden of Disease Study. Lancet Glob Health 2016;4(9):e642-e653. https://doi.org/10.1016/S2214-109X(16)30113-9 [ Links ]
11. Adeboye B, Bermano G, Rolland C. Obesity and its health impact in Africa: A systematic review. Cardiovasc J Afr 2012;23(9):512-521. https://doi.org/10.5830/CVJA-2012-040 [ Links ]
12. Statistics South Africa. Mortality and causes of death in South Africa: Findings from death notification, 2017. Statistical release P0309.3. Pretoria: Stats SA, 2020. http://www.statssa.gov.za/publications/P03093/P030932017.pdf (accessed 20 May 2020). [ Links ]
13. Gentile S, Strollo F, Ceriello A. COVID-19 infection in Italian people with diabetes: Lessons learned for our future (an experience to be used). Diabetes Res Clin Pract 2020;162:108137. https://doi.org/10.1016/j.diabres.2020.108137 [ Links ]
14. International Diabetes Federation. IDF Diabetes Atlas. 9th ed. Brussels, Belgium: IDF, 2019. https://www.diabetesatlas.org (accessed 18 May 2020). [ Links ]
15. Fadini GP, Morieri ML, Longato E, Avogaro A. Prevalence and impact of diabetes among people infected with SARS-CoV-2. J Endocrinol Invest 2020;43(6):867-869. https://doi.org/10.1007/s40618-020-01236-2 [ Links ]
16. Singh AK, Gupta R, Ghosh A, Misra A. Diabetes in COVID-19: Prevalence, pathophysiology, prognosis and practical considerations. Diabetes Metab Syndr 2020;14(4):303-310. https://doi.org/10.1016/j. [ Links ]
17. Shah BR, Hux JE. Quantifying the risk of infectious diseases for people with diabetes. Diabetes Care 2003;26(2):510-513. https://doi.org/10.2337/diacare.26.2.510 [ Links ]
18. Muller LM, Gorter KJ, Hak E, et al Increased risk of common infections in patients with type 1 and type 2 diabetes mellitus. Clin Infect Dis 2005;41(3):281-288. https://doi.org/10.1086/431587 [ Links ]
19. Casqueiro J, Casqueiro J, Alves C. Infections in patients with diabetes mellitus: A review of pathogenesis. Indian J Endocrinol Metab 2012;16(Suppl 1):S27-S36. https://doi.org/10.4103/2230-8210.94253 [ Links ]
20. Allard R, Leclerc P, Tremblay C, Tannenbaum TN. Diabetes and the severity of pandemic influenza A (H1N1) infection. Diabetes Care 2010;33(7):1491-1493. https://doi.org/10.2337/dc09-2215 [ Links ]
21. El-Solh A, Sikka P, Bozkanat E, Jaafar W, Davies J. Morbid obesity in the medical ICU. Chest 2001;120(6):1989-1997. https://doi.org/10.1378/chest.120.6.1989 [ Links ]
22. Badawi A, Ryoo SG. Prevalence of diabetes in the 2009 influenza A (H1N1) and the Middle East respiratory syndrome coronavirus: A systematic review and meta-analysis. J Public Health Res 2016;5(3):733. https://doi.org/10.4081/jphr.2016.733 [ Links ]
23. Garbati MA, Fagbo SF, Fang VJ, et al. A comparative study of clinical presentation and risk factors for adverse outcome in patients hospitalised with acute respiratory disease due to MERS coronavirus or other causes. PLoS ONE 2016;11(11):e0165978. https://doi.org/10.1371/journal.pone.0165978 [ Links ]
24. Yang JK, Feng Y, Yuan MY, et al. Plasma glucose levels and diabetes are independent predictors for mortality and morbidity in patients with SARS. Diabet Med 2006;23(6):623-628. https://doi.org/10.1111/j.1464-5491.2006.01861.x [ Links ]
25. Yang JK, Lin SS, Ji XJ, Guo LM. Binding of SARS coronavirus to its receptor damages islets and causes acute diabetes. Acta Diabetol 2010;47(3):193-199. https://doi.org/10.1007/s00592-009-0109-4 [ Links ]
26. Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir Med 2020;8(5):475-481. https://doi.org/10.1016/S2213-2600(20)30079-5 [ Links ]
27. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020;323(13):1239-1242. https://doi.org/10.1001/jama.2020.2648 [ Links ]
28. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020;395(10229):1054-1062. https://doi.org/10.1016/s0140-6736(20)30566-3 [ Links ]
29. Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA 2020 (epub 6 April 2020). https://doi.org/10.1001/jama.2020.5394 [ Links ]
30. Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 2020;323(18):1775-1776. https://doi.org/10.1001/jama.2020.4683 [ Links ]
31. Richardson S, Hirsch JS, Narasimhan M, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020 (epub 22 April 2020). https://doi.org/10.1001/jama.2020.6775 [ Links ]
32. Chen X, Hu W, Ling J, et al. Hypertension and diabetes delay the viral clearance in COVID-19 patients. medRxiv 2020 (epub 24 March 2020). https://doi.org/10.1101/2020.03.22.20040774 [ Links ]
33. Kohio HP, Adamson AL. Glycolytic control of vacuolar-type ATPase activity: A mechanism to regulate influenza viral infection. Virology 2013;444(1-2):301-309. https://doi.org/10.1016/j.virol.2013.06.026 [ Links ]
34. Bode B, Garrett V, Messler J, et al. Glycemic characteristics and clinical outcomes of COVID-19 patients hospitalized in the United States. J Diabetes Sci Technol 2020 (epub 9 May 2020). https://doi.org/10.1177/1932296820924469 [ Links ]
35. Williamson E, Walker AJ, Bhaskaran KJ, et al. OpenSAFELY: Factors associated with COVID- 19-related hospital death in the linked electronic health records of 17 million adult NHS patients. medRxiv 2020 (epub 7 May 2020). https://doi.org/10.1101/2020.05.06.20092999 [ Links ]
36. Thakker U, Ellman T, Magleby R, Graff K, Kelson J, Silverman RA. The impact of acute illness on HbA(1c) determination of undiagnosed diabetes. Diabetes Metab Res Rev 2012;28(7):603-607. https://doi.org/10.1002/dmrr.2315 [ Links ]
37. Greci LS, Kailasam M, Malkani S, et al. Utility of HbA(1c) levels for diabetes case finding in hospitalized patients with hyperglycemia. Diabetes Care 2003;26(4):1064-1068. https://doi.org/10.2337/diacare.26.4.1064 [ Links ]
38. Yakubovich N, Gerstein HC. Serious cardiovascular outcomes in diabetes: The role of hypoglycemia. Circulation 2011;123(3):342-348. https://doi.org/10.1161/CIRCULATIONAHA.110.948489 [ Links ]
39. Fezeu L, Julia C, Henegar A, et al. Obesity is associated with higher risk of intensive care unit admission and death in influenza A (H1N1) patients: A systematic review and meta-analysis. Obes Rev 2011;12(8):653-659. https://doi.org/10.1111/j.1467-789X.2011.00864.x [ Links ]
40. Simonnet A, Chetboun M, Poissy J, et al. High prevalence of obesity in severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation. Obesity (Silver Spring) 2020 (epub 9 April 2020). https://doi.org/10.1002/oby.22831 [ Links ]
41. Jia X, Yin C, Lu S, et al. Two things about COVID-19 might need attention. Preprints.org, 23 February 2020. https://europepmc.org/article/ppr/ppr114553 (accessed 5 June 2020). [ Links ]
42. Zhu L, She ZG, Cheng X, et al. Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes. Cell Metab 2020;31(6):1068-1077.e1063. https://doi.org/10.1016/j.cmet.2020.04.021 [ Links ]
43. Kornum JB, Thomsen RW, Riis A, Lervang HH, Schonheyder HC, Sorensen HT. Diabetes, glycemic control, and risk of hospitalization with pneumonia: A population-based case-control study. Diabetes Care 2008;31(8):1541-1545. https://doi.org/10.2337/dc08-0138 [ Links ]
44. Ryden L, Armstrong PW, Cleland JG, et al. Efficacy and safety of high-dose lisinopril in chronic heart failure patients at high cardiovascular risk, including those with diabetes mellitus: Results from the ATLAS trial. Eur Heart J 2000;21(23):1967-1978. https://doi.org/10.1053/euhj.2000.2311 [ Links ]
45. Maggioni AP, Anand I, Gottlieb SO, et al. Effects of valsartan on morbidity and mortality in patients with heart failure not receiving angiotensin-converting enzyme inhibitors. J Am Coll Cardiol 2002;40(8):1414-1421. https://doi.org/10.1016/s0735-1097(02)02304-5 [ Links ]
46. ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002;288(23):2981-2997. https://doi.org/10.1001/jama.288.23.2981 [ Links ]
47. Zhang H, Penninger JM, Li Y, Zhong N, Slutsky AS. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: Molecular mechanisms and potential therapeutic target. Intensive Care Med 2020;46(4):586-590. https://doi.org/10.1007/s00134-020-05985-9 [ Links ]
48. Alifano M, Alifano P, Forgez P, Iannelli A. Renin-angiotensin system at the heart of COVID-19 pandemic. Biochimie 2020;174:30-33. https://doi.org/10.1016/j.biochi.2020.04.008 [ Links ]
49. Zhang P, Zhu L, Cai J, et al. Association of inpatient use of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers with mortality among patients with hypertension hospitalized with COVID-19. Circ Res 2020;126(12):1671-1681. https://doi.org/10.1161/CIRCRESAHA.120.317134 [ Links ]
50. International Society of Hypertension. A statement from the International Society of Hypertension on COVID-19. 2020. https://ish-world.com/news/a/A-statement-from-the-International-Society-of-Hypertension-on-COVID-19/ (accessed 5 June 2020). [ Links ]
51. European Society of Hypertension. ESH statement on COVID-19. 15 April 2020. https://www.eshonline.org/spotlights/esh-statement-COVID-19 (accessed 5 June 2020). [ Links ]
52. Hassan FI, Didari T, Khan F, Niaz K, Mojtahedzadeh M, Abdollahi M. A review on the protective effects of metformin in sepsis-induced organ failure. Cell J (Yakhteh) 2020;21(4):363-370. https://doi.org/10.22074/cellj.2020.6286 [ Links ]
53. Salvatore T, Pafundi PC, Marfella R, et al. Metformin lactic acidosis: Should we still be afraid? Diabetes Res Clin Pract 2019;157:107879. https://doi.org/10.1016/j.diabres.2019.107879 [ Links ]
54. Drucker DJ. Coronavirus infections and type 2 diabetes-shared pathways with therapeutic implications. Endocr Rev 2020;41(3):bnaa011. https://doi.org/10.1210/endrev/bnaa011 [ Links ]
55. Raj VS, Mou H, Smits SL, et al. Dipeptidyl peptidase 4 is a functional receptor for the emerging human coronavirus-EMC. Nature 2013;495(7440):251-254. https://doi.org/10.1038/nature12005 [ Links ]
56. Batlle D, Soler MJ, Sparks MA, et al. Acute kidney injury in COVID-19: Emerging evidence of a distinct pathophysiology. J Am Soc Nephrol 2020. https://doi.org/10.1681/ASN.2020040419 [ Links ]
57. Society for Endocrinology, Metabolism and Diabetes of South Africa: Type 2 Diabetes Guidelines Expert Committee. SEMDSA 2017 Guidelines for the Management of Type 2 Diabetes Mellitus. J Endocr Metab Diabetes S Afr 2017;22(1):S1-S196. [ Links ]
58. ClinicalTrials.gov. Dapagliflozin in respiratory failure in patients with COVID-19 (DARE-19). ClinicalTrials.gov identifier: NCT04350593. https://clinicaltrials.gov/ct2/show/NCT04350593?id=NCT04350593&draw=2&rank=1&load=cart (accessed 5 June 2020). [ Links ]
59. World Health Organization. Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected: Interim guidance, 25 January 2020. Geneva: World Health Organization, 2020. https://apps.who.int/iris/handle/10665/330854 (accessed 7 June 2020). [ Links ]
60. Fitchett D. A safety update on sodium glucose co-transporter 2 inhibitors. Diabetes Obes Metab 2019;21(Suppl 2):34-42. https://doi.org/10.1111/dom.13611 [ Links ]
61. Chee YJ, Ng SJH, Yeoh E. Diabetic ketoacidosis precipitated by Covid-19 in a patient with newly diagnosed diabetes mellitus. Diabetes Res Clin Pract 2020;164:108166. https://doi.org/10.1016/j.diabres.2020.108166 [ Links ]
62. Li J, Wang X, Chen J, Zuo X, Zhang H, Deng A. COVID-19 infection may cause ketosis and ketoacidosis. Diabetes Obes Metab 2020 (epub 20 April 2020). https://doi.org/10.1111/dom.14057 [ Links ]
 Correspondence:
Correspondence:
A Coetzee
ankiac@sun.ac.za
Accepted 9 June 2020.


{kind=link}