










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 no.8 Pretoria Ago. 2020
http://dx.doi.org/10.7196/SAMJ.2020.v110i8.15024
CME
Prevention of community-acquired pneumonia in children: South African Thoracic Society guidelines (part 4)
H J ZarI, II; D P MooreIII; S AndronikouI, IV; A C ArgentV; T AvenantVI; C CohenVII; R J GreenVIII; G ItzikowitzIX; P JeenaX; M P NicolXI; A PillayVII; G ReubensonXIII; R MasekelaVII; S A MadhiXV, XVI
IPhD; Department of Paediatrics and Child Health, Red Cross War Memorial Children's Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
IIPhD; South African Medical Research Council Unit on Child and Adolescent Health, University of Cape Town, South Africa
IIIPhD; Department of Paediatrics and Child Health, Chris Hani Baragwanath Academic Hospital, and Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVPhD; Department of Pediatric Radiology, Perelman School of Medicine, University of Pennsylvania, and Children's Hospital of Philadelphia, PA, USA
VMD (Paediatrics); Department of Paediatrics and Child Health, Red Cross War Memorial Children's Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
VIFCPaed (SA); Department of Paediatrics and Child Health, Faculty of Health Sciences, University of Pretoria, South Africa
VIIPhD; Centre for Respiratory Diseases and Meningitis, National Institute for Communicable Diseases, Johannesburg, South Africa
VIIIPhD; Department of Paediatrics and Child Health, Faculty of Health Sciences, University of Pretoria, South Africa
IXMSc; Department of Paediatrics and Child Health, Red Cross War Memorial Children's Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
XFCPaed (SA); Department of Paediatrics and Child Health, Nelson R Mandela School of Medicine, School of Clinical Medicine, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
XIPhD; Division of Medical Microbiology, Department of Pathology, Faculty of Health Sciences, University of Cape Town, South Africa; and Division of Infection and Immunity, School of Biomedical Sciences, University of Western Australia, Perth, Australia
XIICert ID Paed (SA); Department of Paediatrics and Child Health, Nelson R Mandela School of Medicine, School of Clinical Medicine, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
XIIIFCPaed (SA); Department of Paediatrics and Child Health, Rahima Moosa Mother and Child Hospital, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
XIVPhD;. Department of Paediatrics and Child Health, Nelson R Mandela School of Medicine, School of Clinical Medicine, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
XVPhD; South African Medical Research Council Vaccine and Infectious Diseases Analytics Unit, University of the Witwatersrand, Johannesburg, South Africa
XVIPhD; Department of Science and Technology/National Research Foundation: South African Research Chair in Vaccine Preventable Diseases, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. More comprehensive immunisation regimens, strengthening of HIV prevention and management programmes and improved socioeconomic conditions have impacted on the epidemiology of paediatric community-acquired pneumonia (CAP) in South Africa (SA).
OBJECTIVES. To summarise effective preventive strategies to reduce the burden of childhood CAP.
METHODS. An expert subgroup reviewed existing SA guidelines and new publications focusing on prevention. Published evidence on pneumonia prevention informed the revisions; in the absence of evidence, expert opinion was used. Evidence was graded using the British Thoracic Society (BTS) grading system.
RECOMMENDATIONS. General measures for prevention include minimising exposure to tobacco smoke or air pollution, breastfeeding, optimising nutrition, optimising maternal health from pregnancy onwards, adequate antenatal care and improvement in socioeconomic and living conditions. Prevention of viral transmission, including SARS-CoV-2, can be achieved by hand hygiene, environmental decontamination, use of masks and isolation of infected people. Specific preventive measures include vaccines as contained in the Expanded Programme on Immunisation schedule, isoniazid prophylaxis for tuberculosis, co-trimoxazole prophylaxis for HIV-infected infants and children who are immunosuppressed, and timely diagnosis of HIV, as well as antiretroviral therapy (ART) initiation. HIV-infected children treated with ART from early infancy, and HIV-exposed children, have similar immunogenicity and immune responses to most childhood vaccines as HIV-unexposed infants.
VALIDATION. These recommendations are based on available published evidence supplemented by the consensus opinion of SA paediatric experts, and are consistent with those in published international guidelines.
Advances in the prevention of paediatric pneumonia have led to a reduction in the burden of disease and have lowered the case fatality risk and mortality over the past two decades. Socioeconomic improvements, reduction in perinatal HIV transmission, effective antiretroviral therapy (ART) programmes, introduction of bacterial-conjugate vaccines and improved immunisation coverage have changed the epidemiology and aetiology of childhood pneumonia in South Africa (SA). This section of the revised SA paediatric pneumonia guidelines presents current evidence aimed at prevention of childhood community-acquired pneumonia (CAP).
Prevention of childhood pneumonia
General preventive strategies
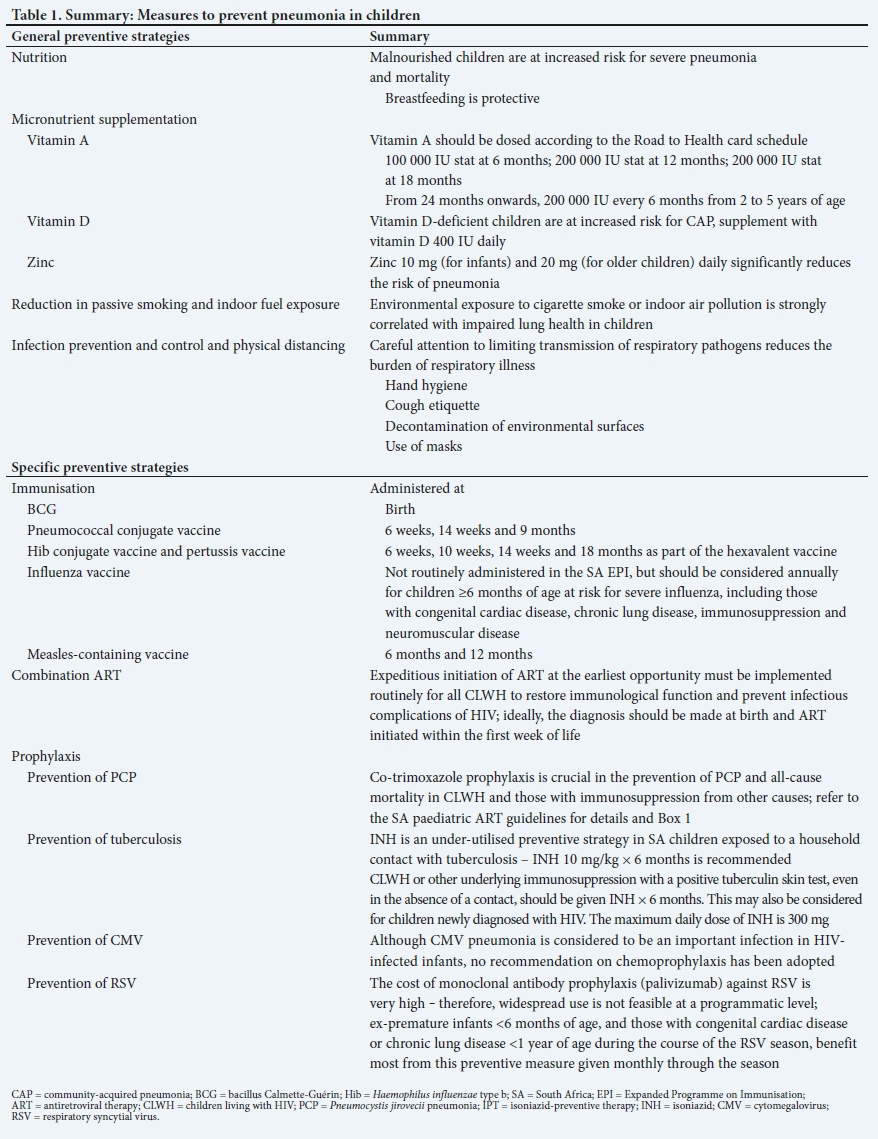
General preventive strategies that reduce the incidence and severity of pneumonia are the following, and are summarised in Table 1.
Nutrition
Adequate nutrition and growth monitoring should be encouraged, as malnutrition predisposes children to pneumonia and severe illness. Breastfeeding has been shown to decrease the incidence of pneumonia in young children by up to 32%.[1] Shorter duration of breastfeeding is associated with pneumonia mortality, particularly among infants <5 months of age.[2] Mortality among infants who are not breastfed compared with exclusively breastfed infants through 5 months of age is ~15-fold higher (relative risk (RR) 14.97; 95% confidence interval (CI) 0.67 - 332.74).[2] Breastfeeding should be encouraged for the first 6 months of a child's life, irrespective of maternal HIV or ART use,[3] and may be considered for the first 2 years in children living with HIV (CLWH).[4]
Micronutrient supplementation
Specific micronutrients that may play a role in the prevention of pneumonia are discussed below:
Vitamin A. Vitamin A supplementation reduces severity of respiratory complications of measles.[5] However, a meta-analysis of the impact of vitamin A supplementation on all-cause pneumonia morbidity and mortality showed no consistent effect on pneumonia-specific mortality.[6] Provision of vitamin A supplementation in children with vitamin A deficiency has been associated with improved outcomes.
Vitamin D. While empiric therapy using vitamin D in hospitalised children with CAP is not beneficial, observational studies have identified an increased risk of pneumonia in children <5 years old with subclinical vitamin D deficiency (evidence level III).[7-A meta-analysis of the role of vitamin D supplementation in pneumonia prevention found a significant protective effect (evidence level Ia).[8 However, in a clinical trial conducted in Asian children <5 years of age, oral doses of vitamin D had no protective effect on the incidence of the first episode of pneumonia (evidence level Ib).[9-
Vitamin E. There is very little evidence to support vitamin E supplementation for the prevention of pneumonia in children (evidence level IVa).[10,n
Zinc. Daily prophylactic elemental zinc, 10 mg (infants) and 20 mg (older children), may substantially reduce the incidence of pneumonia, particularly in malnourished children.[12] A pooled analysis of randomised controlled trials of zinc supplementation in well-nourished and malnourished children found that children who received zinc supplementation had a significant reduction in pneumonia incidence compared with those who received placebo (odds ratio (OR) 0.59; CI 0.41 - 0.83) (evidence level Ia).[13]
Reduction in tobacco smoke or indoor fuel exposure
Active and passive exposure to tobacco should be strongly discouraged in women of child-bearing age, particularly among pregnant women,[14] and more generally in the household.[15]
Exposure to fumes from indoor cooking fuels should be limited by opening windows and doors when cooking; the chimney should function well; the stove should be cleaned and maintained; and there should be safe child location practices while fires are burning in the house.[16] The practice of carrying children on caregivers' backs while cooking is an independent risk factor for pneumonia morbidity and mortality.[17] Children should sleep in rooms separate from where food is cooked (evidence level Ib).
Infection prevention, control, use of masks and physical distancing
Hand hygiene and respiratory etiquette are crucial in limiting interpersonal transmission of respiratory pathogens.[18,19] Reinforcement of hand hygiene decreases the prevalence of respiratory tract illness in adults by 14% (95% CI 11 - 17) in non-pandemic influenza seasons.[20] A systematic review and meta-analysis of the effect of hand hygiene in limiting illness in children suggested that in primary and secondary schools, hand hygiene may decrease the incidence of respiratory tract infections among learners (evidence level Ia).[21] Although young children are not generally able to adhere to respiratory etiquette practices,[22] older children, caregivers and health workers should adopt these practices to limit the transmission of respiratory pathogens.[18]
Universal use of cloth face masks by children and adults in public is an effective public health intervention to reduce transmission of respiratory viruses, including SARS-CoV-2, in addition to other public health measures.[23] In health facilities, all healthcare workers should wear a surgical mask in addition to practising hand hygiene, physical distancing and environmental decontamination to prevent SARS-CoV-2 transmission.[23]
Specific preventive strategies
Immunisation
Routine immunisations
All children should receive routine vaccines, including bacillus Calmette-Guérin (BCG), measles, diphtheria-pertussis-tetanus (DPT) toxoid, Haemophilus influenzae type b (Hib), polysaccharide-protein conjugate vaccine (HibCV) and pneumococcal polysaccharide-protein conjugate vaccine (PCV) as per the SA immunisation schedule.[24] The nature and degree of immunosuppression in CLWH may impact on the efficacy and duration of vaccine-induced protection.[25-29] CLWH treated with ART from early infancy, and responding well to such therapy, demonstrate similar immunogenicity and anamnestic immune responses to most childhood vaccines compared with HIV-unexposed infants.[30,31] HIV-exposed uninfected (HEU) infants may have lower concentrations of transplacental acquired antibodies for some vaccine-preventable diseases,[32,33] which could increase their susceptibility to pneumonia during early infancy. The immune responses to all vaccines are, however, similar or more immunogenic for HEU than for HIV-unexposed infants,[30,31] and there is similar persistence of protective antibody concentrations and memory responses.[34]
Specific vaccines
BCG vaccine. Mycobacterium tuberculosis may be a direct pathogen in pneumonia or may predispose to bacterial infection (including from pneumococcus).[35,36] A birth dose of BCG vaccine is effective in preventing disseminated tuberculosis in young children, but has variable effectiveness (average 50%; range 0 - 84% effectiveness) in prevention of pulmonary tuberculosis, with lower effectiveness in studies on children from tropical countries.[37,38] A birth dose has also been shown to have nonspecific benefits in improving overall child survival in some settings.[39]
Pneumococcal vaccine. Multiple post-licensure effectiveness studies (using 10- and 13-valent PCV) in a diversity of settings have demonstrated a 17% (95% CI 11 - 22) and 31% (95% CI 26 - 35) reduction in hospitalisation rates for clinically and radiologically confirmed pneumonia, respectively.[40] In children aged 24 - 59 months a meta-analysis found a reduction of 9% (95% CI 5 - 14) and 24% (95% CI 12 - 33) in hospitalisation rates for clinically and radiologically confirmed pneumonia, respectively (evidence level Ia).[40]
In SA, PCV (currently 13-valent) is administered at 6 and 14 weeks of age, followed by a booster dose at 9 months of age (evidence level Ib). This schedule has been shown to be effective in reducing all-cause pneumonia hospitalisation by 33% and 39% in CLWH and HIV-uninfected children, respectively.[41]
The 23-valent pneumococcal polysaccharide vaccine (Pneumovax 23) is recommended for children >2 years old, who are at risk of developing invasive pneumococcal disease, including those with sickle cell disease, chronic pulmonary disease and cardiovascular disease,[42,43] and is included in the SA Essential Drugs List for paediatrics for administration to such patients. It should be preceded by a single dose of PCV, given at least 1 month before (evidence level III).[44,45-
The need for further booster doses of PCV in older CLWH remains to be determined, but the indirect effect of childhood PCV immunisation in reducing transmission and circulation of vaccine-serotype pneumococci could mitigate waning of immunity in CLWH and other high-risk groups that remain susceptible to developing severe pneumonia in later childhood.[46] The World Health Organization (WHO) currently recommends that a booster dose of PCV may be considered in the second year of life in CLWH (evidence level II).[47]
Hib conjugate vaccine. Vaccination with HibCV, as part of a combination vaccine, is recommended as a 3-dose primary series, and includes a booster dose at 15 - 18 months of age in SA. HibCV is less effective in CLWH not on ART;[48] however, the immunogenicity of the vaccine and persistence of memory responses in the second year of life are similar in CLWH vaccinated when already initiated on ART at the time of immunisation.[49]
Pertussis vaccine. Pertussis remains one of the most poorly controlled vaccine-preventable diseases globally and causes severe disease in young infants (especially in those <3 months of age) and incompletely immunised children (evidence level Ib).[50,51]
Pertussis vaccine formulations include whole-cell containing (wP) and Bordetella pertussis protein-only component acellular vaccines (aP). Whole-cell pertussis vaccines, but not aP protein-containing vaccines, induce mucosal immunity and protect against B. pertussis mucosal infection and transmission.!521 Furthermore, the duration of protection of wP is 8 - 12 years compared with 4 - 5 years for aP vaccines.[53] Currently, only aP-containing combination vaccines are available in SA.
Pertussis outbreaks have been temporally associated with transitioning from wP to aP formulations in many high-resource settings, attributed to the waning of immunity in the absence of repeat booster doses at school entry and beyond.[531 Children primed with aP-containing vaccines should receive booster doses of aP vaccines (dTaP) at school entry and possibly every 10 years thereafter (not yet part of the Expanded Programme on Immunisation (EPI)) (evidence level II).[54
Prevention of pertussis in very young infants, who are at greatest risk of severe disease, is not achievable through infant immunisation, and transitioning from wP to aP could increase the burden of pertussis in this group.[531 Acellular pertussis vaccination of pregnant women is 90% effective in reducing pertussis in infants <3 months of age (evidence level Ia).[55]
Influenza vaccine. Only the sub-unit inactivated influenza vaccine is available in SA for annual administration. There are limited data on its efficacy in children, ranging from 33% to 73%, depending on vaccine preparation and influenza subtype targeted.[561 Current evidence suggests that influenza vaccination is safe in CLWH; however, a randomised controlled trial failed to demonstrate vaccine efficacy.[571 Nonetheless, there remains a recommendation that CLWH should be offered influenza vaccination before the start of winter, particularly if they have underlying chronic lung disease (evidence level III).
Children >6 months of age with underlying medical conditions are considered a high risk for complications of influenza, and are prioritised for annual vaccination. Such children comprise those with chronic pulmonary disease (including asthma), cardiac disease, chronic renal or hepatic diseases, diabetes mellitus, metabolic disorders, sickle cell anaemia and other haemoglobinopathies, morbid obesity, immunosuppression, cerebral palsy or other neuromuscular conditions.[581 Family members and siblings of such patients should also be vaccinated.[58] Two doses of inactivated influenza vaccine, administered 1 month apart, are recommended for children 6 months - 9 years of age who have never been vaccinated; and a single dose if immunised in previous seasons.[58]
Recent randomised controlled trials have demonstrated that influenza vaccination of pregnant women was 50% efficacious in reducing polymerase chain reaction (PCR)-confirmed influenza illness in their infants until 24 weeks of age. In SA and Mali, vaccination of pregnant women was more effective in preventing influenza illness in infants during the first 3 months of life (vaccine efficacy - 85%), with subsequent waning and a non-significant reduction between 3 and 6 months of age.[591 Maternal influenza vaccination also reduced all-cause clinically diagnosed severe pneumonia or pneumonia hospitalisation by 30% in infants during the first 6 months.[59,60]
Influenza immunisation should ideally be administered prior to the onset of the influenza season (which typically occurs from May to September in SA),[61,621 but can also be given during the influenza season. Due to the potential of year-on-year genetic drift of seasonal influenza virus strains, current vaccine formulations are updated annually, and a repeat vaccination is required each year.
Measles vaccine. Measles remains a public health concern, and failure to achieve and sustain high immunisation coverage rates (>95%) against this highly contagious virus results in ongoing outbreaks in a diversity of settings, including SA.[63,641 Recent changes in the epidemiology of measles include a greater susceptibility of disease in very young infants (as early as 4 months of age).[64] This is due to lower antibody concentrations in pregnant women who have acquired immunity through vaccination, rather than through wild-type virus exposure, as well as possible waning of immunity in women living with HIV.[65,66]
The WHO recommends that children receive 2 doses of the measles vaccine, the first at 9 months of age and a booster dose at 15 - 18 months of age.[67] However, for infants born to women living with HIV, and in settings with a high risk of measles in young infants, an additional dose is recommended at 6 months of age.[671 In SA, a 2-dose measles vaccination schedule is recommended, administered at 6 and 12 months of age. This induces seroprotective titres in ~55% of infants following the first dose of vaccine, and in >98% in HIV-exposed and HIV-unexposed children after the second dose of vaccine.[68]
Combination antiretroviral therapy
The use of ART to reconstitute immunity is very effective for decreasing the incidence of pneumonia and opportunistic infections in CLWH. Combination ART should be initiated on diagnosis of HIV in all children, irrespective of clinical or immunological staging. Screening for HIV infection in newborns of HIV-infected women by means of PCR testing at birth and repeated PCR testing during the infant and breastfeeding period is standard of care in SA, with initiation of ART as soon as possible after confirmation of HIV infection, and continued lifelong thereafter.
Prophylaxis
Prevention oiPneumocystis jirovecii pneumonia. Updated recommendations for the management of CLWH were published in 2019 (South African ART guidelines) (Box 1).[69]

Although the WHO recommends Pneumocystis jirovecii pneumonia (PCP) prophylaxis for HEU infants from 4 to 6 weeks of age until HIV infection has been excluded after complete cessation of breastfeeding, two southern African randomised controlled trials have shown that co-trimoxazole confers no survival advantage over placebo in this subset of children; therefore, this is not recommended in SA.[70,71]
Prevention of tuberculosis. All children <5 years of age exposed to a household tuberculosis contact or other close tuberculosis contact should be given isoniazid preventive therapy (IPT) (10 mg/kg; maximum dose 300 mg) daily for 6 months once tuberculosis disease has been excluded. CLWH exposed to a household contact should be given prophylaxis for 6 months, irrespective of their age. A 6-month course of IPT should also be given to tuberculin skin test (TST)-positive CLWH, even in the absence of a known household contact.[72]
There are conflicting data on the use of primary IPT in CLWH in the absence of a tuberculosis contact.[73,74] Newly HIV-diagnosed and clinically symptomatic CLWH may benefit from a 6-month course of IPT, irrespective of TST results.
Short-course preventive therapy using rifampicin and isoniazid must not be used in the context of tuberculosis prevention in HIV-exposed neonates born to mothers with active tuberculosis, as the rifampicin component interferes with the prevention of mother-to-child transmission (PMTCT) regimens.[75]
Current WHO guidelines encourage use of preventive therapy with multidrug-resistant tuberculosis (MDR-TB) based on individualised risk assessment for children exposed to source cases. In children exposed to a source case with ofloxacin-susceptible M. tuberculosis, a 6-month course of ofloxacin, ethambutol and high-dose isoniazid has been found to be well tolerated.[76]
Prevention of cytomegalovirus disease in HIV-infected children. There is no evidence to support a specific intervention in the prevention of cytomegalovirus (CMV) disease in CLWH.[77]
Prevention of respiratory syncytial virus. Although the humanised monoclonal-specific antibody for the prevention of respiratory syncytial virus (RSV) infections (palivizumab) is available, it is very expensive. Children most likely to benefit are those at risk of severe RSV infection, i.e. babies born prematurely who are <6 months of chronological age at the onset of the RSV season, or children with chronic lung disease or congenital cardiac disease who are <1 year of age at the onset of the RSV season.[78] A meta-analysis on the effectiveness of palivizumab against RSV hospitalisation reported 71% (95% CI 46 - 84) effectiveness in infants born at <35 weeks' gestational age, and ~45% in those with chronic lung disease and congenital heart disease (evidence level Ia).[79] Palivizumab should be given monthly for the duration of the RSV season (from February to July) in most of SA.[80,81]
Other strategies for prevention of severe RSV disease in infants, including antenatal vaccination of expectant mothers and long-acting monoclonal antibody preparations, are currently under investigation.
Conclusions
Improvements in the EPI, through inclusion of protein-polysaccharide conjugate vaccines targeting Hib and pneumococcus, and expansion of the ART programme to prevent paediatric HIV infection and treat CLWH, have reduced the burden of CAP in SA children. However, the socioeconomic determinants of health still place the majority of children in SA at risk of becoming ill with pneumonia, and concerted efforts are needed for intersectoral collaboration to bring about sustained reductions in the pneumonia burden of SA children. Pneumonia-specific preventive strategies are highly effective and require ongoing implementation and monitoring.
Declaration. None.
Acknowledgements. None.
Author contributions. The prevention group was chaired by SAM, with members DPM and HJZ. This group reviewed the evidence and wrote the manuscript. RM led a group on HIV considerations, with AP; findings from this group have been incorporated into this manuscript. All authors reviewed and contributed to the final manuscript.
Funding. HJZ and SAM are supported by the South African Medical Research Council.
Conflicts of interest. None.
References
1. Wright AL, Bauer M, Naylor A, Sutcliffe E, Clark L. Increasing breastfeeding rates to reduce infant illness at the community level. Pediatrics 1998;101(5):837-844. https://doi.org/10.1542/peds.10L5.837 [ Links ]
2. Lamberti LM, Zakarija-Grkovic I, Fischer Walker CL, et al. Breastfeeding for reducing the risk of pneumonia morbidity and mortality in children under two: A systematic literature review and meta-analysis. BMC Public Health 2013;13(Suppl 3):S18. https://doi.org/10.1186/1471-2458-13-S3-S18 [ Links ]
3. Doherty T, Sanders D, Goga A, Jackson D. Implications of the new WHO guidelines on HIV and infant feeding for child survival in South Africa. Bull World Health Organ 2011;89(1):62-67. https://doi.org/10.2471/BLT.10.079798 [ Links ]
4. Kuhn L, Kroon M. Breastfeeding and the 2015 South African guidelines for prevention of mother-to-child transmission of HIV S Aft J HIV Med 2015;16(1). https://doi.org/10.4102/sajhivmed.v16i1.377 [ Links ]
5. Hussey GD, Klein M. A randomized, controlled trial of vitamin A in children with severe measles. N Engl J Med 1990;323(3):160-164. https://doi.org/10.1056/NEJM199007193230304 [ Links ]
6. Kirkwood BR, Gove S, Rogers S, Lob-Levyt J, Arthur P, Campbell H. Potential interventions for the prevention of childhood pneumonia in developing countries: A systematic review. Bull World Health Organ 1995;73(6):793-798. [ Links ]
7. Wayse V, Yousafzai A, Mogale K, Filteau S. Association of subclinical vitamin D deficiency with severe acute lower respiratory infection in Indian children under 5 y. Eur J Clin Nutr 2004;58(4):563-567. https://doi.org/10.1038/sj.ejcn.1601845 [ Links ]
8. Charan J, Goyal JP, Saxena D, Yadav P. Vitamin D for prevention of respiratory tract infections: A systematic review and meta-analysis. J Pharmacol Pharmacother 2012;3(4):300-303. https://doi.org/10.4103/0976-500X.103685 [ Links ]
9. Choudhary N, Gupta P. Vitamin D supplementation for severe pneumonia - a randomized controlled trial. Indian Pediatr 2012;49(6):449-454. https://doi.org/10.1007/s13312-012-0073-x [ Links ]
10. Theodoratou E, Al-Jilaihawi S, Woodward F, et al. The effect of case management on childhood pneumonia mortality in developing countries. Int J Epidemiol 2010;39(Suppl 1):i155-i171. https://doi.org/10.1093/ije/dyq032 [ Links ]
11. Lee GY, Han SN. The role ofvitamin E in immunity. Nutrients 2018;10(11):1614. https://doi.org/10.3390/nu10111614 [ Links ]
12. Bhandari N, Bahl R, Taneja S, et al. Effect of routine zinc supplementation on pneumonia in children aged 6 months to 3 years: Randomised controlled trial in an urban slum. BMJ 2002;324(7350):1358. https://doi.org/10.1136/bmj.324.7350.1358 [ Links ]
13. Bhutta ZA, Black RE, Brown KH, et al. Prevention of diarrhea and pneumonia by zinc supplementation in children in developing countries: Pooled analysis of randomized controlled trials. J Pediatr 1999;135(6):689-697. https://doi.org/10.1016/s0022-3476(99)70086-7 [ Links ]
14. Gibbs K, Collaco JM, McGrath-Morrow SA. Impact of tobacco smoke and nicotine exposure on lung development. Chest 2016;149(2):552-561. https://doi.org/10.1378/chest.15-1858 [ Links ]
15. Steyn K, Yach D, Stander I, Fourie JM. Smoking in urban pregnant women in South Africa. S Afr Med J 1997;87(4):460-463. [ Links ]
16. Baumgartner J, Schauer JJ, Ezzati M, et al. Patterns and predictors of personal exposure to indoor air pollution from biomass combustion among women and children in rural China. Indoor Air 2011;21(6):479-488. https://doi.org/10.1111/j.1600-0668.2011.00730.x [ Links ]
17. Admasie A, Kumie A, Worku A. Children under five from houses of unclean fuel sources and poorly ventilated houses have higher odds of suffering from acute respiratory infection in Wolaita-Sodo, Southern Ethiopia: A case-control study. J Environ Public Health 2018;2018:9320603. https://doi.org/10.1155/2018/9320603 [ Links ]
18. American Academy of Pediatrics Committee on Infectious Diseases. Infection prevention and control in pediatric ambulatory settings. Pediatrics 2007;120(3):650-665. https://doi.org/10.1542/peds.2007-1734 [ Links ]
19. Hellewell J, Abbott S, Gimma A, et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob Health 2020;8(4):E488-E496. https://doi.org/10.1016/S2214-109X(20)30074-7 [ Links ]
20. Little P, Stuart B, Hobbs FDR, et al. An internet-delivered handwashing intervention to modify influenzalike illness and respiratory infection transmission (PRIMIT): A primary care randomised trial. Lancet 2015;386(10004):1631-1639. https://doi.org/https://doi.org/10.1016/S0140-6736(15)60127-1 [ Links ]
21. Willmott M, Nicholson A, Busse H, MacArthur GJ, Brookes S, Campbell R. Effectiveness of hand hygiene interventions in reducing illness absence among children in educational settings: A systematic review and meta-analysis. Arch Dis Childh 2016;101(1):42-50. https://doi.org/10.1136/archdischild-2015-308875 [ Links ]
22. Walker JH. Pediatric influenza and 'universal respiratory etiquette': Preparing and protecting your staff and the public. J Emerg Nurs 2004;30(4):367-370. https://doi.org/10.1016/j.jen.2004.04.006 [ Links ]
23. Chu DK, Akl EA, Duda S, Solo K, Yaacoub S, Schünemann HJ. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020;395(10242):1973-1987. https://doi.org/10.1016/s0140-6736(20)31142-9 [ Links ]
24. Hoest C, Seidman JC, Lee G, et al. Vaccine coverage and adherence to EPI schedules in eight resource poor settings in the MAL-ED cohort study. Vaccine 2017;35(3):443-451. https://doi.org/10.1016/j.vaccine.2016.11.075 [ Links ]
25. Madhi SA, Cumin E, Klugman KP. Defining the potential impact of conjugate bacterial polysaccharide-protein vaccines in reducing the burden of pneumonia in human immunodeficiency virus type 1-infected and -uninfected children. Pediatr Infect Dis J 2002;21(5):393-399. https://doi.org/10.1097/00006454-200205000-00009 [ Links ]
26. Madhi SA, Kuwanda L, Cutland C, Holm A, Käyhty H, Klugman KP. Quantitative and qualitative antibody response to pneumococcal conjugate vaccine among African human immunodeficiency virus-infected and uninfected children. Pediatr Infect Dis J 2005;24(5):410-416. https://doi.org/10.1097/01.inf.0000160942.84169.14 [ Links ]
27. Madhi SA, Kuwanda L, Saarinen L, et al Immunogenicity and effectiveness of Haemophilus influenzae type b conjugate vaccine in HIV infected and uninfected African children. Vaccine 2005;23(48-49):5517-5525. https://doi.org/10.1016/j.vaccine.2005.07.038 [ Links ]
28. Klugman KP, Madhi SA, Huebner RE, et al. A trial of a 9-valent pneumococcal conjugate vaccine in children with and those without HIV infection. N Engl J Med 2003;349(14):1341-1348. https://doi.org/10.1056/NEJMoa035060 [ Links ]
29. Madhi SA, Adrian P, Kuwanda L, et al Long-term immunogenicity and efficacy of a 9-valent conjugate pneumococcal vaccine in human immunodeficient virus infected and non-infected children in the absence of a booster dose of vaccine. Vaccine 2007;25(13):2451-2457. https://doi.org/10.1016/j.vaccine.2006.09.019 [ Links ]
30. Madhi SA, Adrian P, Cotton MF, et al. Effect of HIV infection status and anti-retroviral treatment on quantitative and qualitative antibody responses to pneumococcal conjugate vaccine in infants. J Infect Dis 2010;202(3):355-361. https://doi.org/10.1086/653704 [ Links ]
31. Simani OE, Izu A, Violari A, et al. Effect of HIV-1 exposure and antiretroviral treatment strategies in HIV-infected children on immunogenicity of vaccines during infancy. AIDS 2014;28(4):531-541. https://doi.org/10.1097/QAD.0000000000000127 [ Links ]
32. Dzanibe S, Adrian PV, Mlacha SZK, Dangor Z, Kwatra G, Madhi SA. Reduced transplacental transfer of group B Streptococcus surface protein antibodies in HIV-infected mother-newborn dyads. J Infect Dis 2017;215(3):415-419. https://doi.org/10.1093/infdis/jiw566 [ Links ]
33. Jallow S, Madhi SA. Pneumococcal conjugate vaccine in HIV-infected and HIV-exposed, uninfected children. Expert Rev Vaccines 2017;16(5):453-465. https://doi.org/10.1080/14760584.2017.1307740 [ Links ]
34. Simani OE, Izu A, Nunes MC, et al. Effect of HIV exposure and timing of antiretroviral therapy initiation on immune memory responses to diphtheria, tetanus, whole cell pertussis and hepatitis B vaccines. Expert Rev Vaccines 2019;18(1):95-104. https://doi.org/10.1080/14760584.2019.1547195 [ Links ]
35. Moore DP, Klugman KP, Madhi SA. Role of Streptococcus pneumoniae in hospitalization for acute community-acquired pneumonia associated with culture-confirmed Mycobacterium tuberculosis in children: A pneumococcal conjugate vaccine probe study. Pediatr Infect Dis J 2010;29(12):1099-1104. https://doi.org/10.1097/inf.0b013e3181eaefff [ Links ]
36. Oliwa JN, Karumbi JM, Marais BJ, Madhi SA, Graham SM. Tuberculosis as a cause or comorbidity of childhood pneumonia in tuberculosis-endemic areas: A systematic review. Lancet Respir Med 2015;3(3):235-243. https://doi.org/10.1016/S2213-2600(15)00028-4 [ Links ]
37. Colditz GA, Brewer TF, Berkey CS, et al. Efficacy of BCG vaccine in the prevention of tuberculosis. Meta-analysis of the published literature. JAMA 1994;271(9):698-702. [ Links ]
38. Brewer TF. Preventing tuberculosis with bacillus Calmette-Guérin vaccine: A meta-analysis of the literature. Clin Infect Dis 2000;31(Suppl 3):S64-S67. https://doi.org/10.1086/314072 [ Links ]
39. Schaltz-Buchholzer F, Biering-S0rensen S, Lund N, et al. Early BCG vaccination, hospitalizations, and hospital deaths: Analysis of a secondary outcome in 3 randomized trials from Guinea-Bissau. J Infect Dis 2019;219(4):624-632. https://doi.org/10.1093/infdis/jiy544 [ Links ]
40. Alicino C, Paganino C, Orsi A, et al. The impact of 10-valent and 13-valent pneumococcal conjugate vaccines on hospitalization for pneumonia in children: A systematic review and meta-analysis. Vaccine 2017;35(43):5776-5785. https://doi.org/10.1016/j.vaccine.2017.09.005 [ Links ]
41. Izu A, Solomon F, Nzenze SA, et al Pneumococcal conjugate vaccines and hospitalization of children for pneumonia: A time-series analysis, South Africa, 2006 - 2014. Bull World Health Organ 2017;95(9):618-628. https://doi.org/10.2471/BLT.16.187849 [ Links ]
42. World Health Organization. 23-valent pneumococcal polysaccharide vaccine WHO position paper. Wkly Epidemiol Rec 2008;42:373-384. [ Links ]
43. Wang Y, Li J, Wang Y, Gu W, Zhu F. Effectiveness and practical uses of 23-valent pneumococcal polysaccharide vaccine in healthy and special populations. Hum Vaccin Immunother 2018;14(4):1003-1012. https://doi.org/10.1080/21645515.2017.1409316 [ Links ]
44. Moore MR, Link-Gelles R, Schaffner W, et al Effect of use of 13-valent pneumococcal conjugate vaccine in children on invasive pneumococcal disease in children and adults in the USA: Analysis of multisite, population-based surveillance. Lancet Infect Dis 2015;15(3):301-309. https://doi.org/10.1016/S1473-3099(14)71081-3 [ Links ]
45. Berical AC, Harris D, Dela Cruz CS, Possick JD. Pneumococcal vaccination strategies. An update and perspective. Ann Am Thorac Soc 2016;13(6):933-944. https://doi.org/10.1513/AnnalsATS.201511-778FR [ Links ]
46. Tsaban G, Ben-Shimol S. Indirect (herd) protection, following pneumococcal conjugated vaccines introduction: A systematic review of the literature. Vaccine 2017;35(22):2882-2891. https://doi.org/10.1016/j.vaccine.2017.04.032 [ Links ]
47. World Health Organization. Pneumococcal conjugate vaccines in infants and children under 5 years of age: WHO position paper. Wkly Epidemiol Rec 2019;94(8):85-104. [ Links ]
48. Von Gottberg A, de Gouveia L, Madhi SA, et al. Impact of conjugate Haemophilus influenzae type b (Hib) vaccine introduction in South Africa. Bull World Health Organ 2006;84(10):811-818. https://doi.org/10.2471/blt.06.030361 [ Links ]
49. Von Gottberg A, Cohen C, Whitelaw A, et al. Invasive disease due to Haemophilus influenzae serotype b ten years after routine vaccination, South Africa, 2003 - 2009. Vaccine 2012;30(3):565-571. https://doi.org/10.1016/j.vaccine.2011.11.066 [ Links ]
50. Barger-Kamate B, Knoll MD, Kagucia EW, et al Pertussis-associated pneumonia in infants and children from low- and middle-income countries participating in the PERCH Study. Clin Infect Dis 2016;63(Suppl 4):S187-S196. https://doi.org/10.1093/cid/ciw546 [ Links ]
51. Soofie N, Nunes MC, Kgagudi P, et al. The burden of pertussis hospitalization in HIV-exposed and HIV-unexposed South African infants. Clin Infect Dis 2016;63(Suppl 4):S165-S173. https://doi.org/10.1093/cid/ciw545 [ Links ]
52. Warfel JM, Zimmerman LI, Merkel TJ. Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model. Proc Natl Acad Sci USA 2014;111(2):787-792. https://doi.org/10.1073/pnas.1314688110 [ Links ]
53. Van den Biggelaar AHJ, Poolman JT. Predicting future trends in the burden of pertussis in the 21st century: Implications for infant pertussis and the success of maternal immunization. Expert Rev Vaccines 2016;15(1):69-80. https://doi.org/10.1586/14760584.2016.1105136 [ Links ]
54. Marlow R, Kuriyakose S, Mesaros N, et al. A phase III, open-label, randomised multicentre study to evaluate the immunogenicity and safety of a booster dose of two different reduced antigen diphtheria-tetanus-acellular pertussis-polio vaccines, when co-administered with measles-mumps-rubella vaccine in 3 and 4-year-old healthy children in the UK. Vaccine 2018;36(17):2300-2306. https://doi.org/10.1016/j.vaccine.2018.03.021 [ Links ]
55. Campbell H, Gupta S, Dolan GP, et al. Review of vaccination in pregnancy to prevent pertussis in early infancy. J Med Microbiol 2018;67(10):1426-1456. https://doi.org/10.1099/jmm.0.000829 [ Links ]
56. Belongia EA, Simpson MD, King JP, et al. Variable influenza vaccine effectiveness by subtype: A systematic review and meta-analysis of test-negative design studies. Lancet Infect Dis 2016;16(8):942-951. https://doi.org/10.1016/S1473-3099(16)00129-8 [ Links ]
57. Madhi SA, Dittmer S, Kuwanda L, et al. Efficacy and immunogenicity of influenza vaccine in HIV- infected children: A randomized, double-blind, placebo controlled trial. AIDS 2013;27(3):369-379. https://doi.org/10.1097/QAD.0b013e32835ab5b2 [ Links ]
58. Grohskopf LA, Sokolow LZ, Broder KR, Walter EB, Fry AM, Jernigan DB. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices - United States, 2018 - 19 influenza season. MMWR Recomm Rep 2018;67(3):1-20. https://doi.org/10.15585/mmwr.rr6703a1 [ Links ]
59. Nunes MC, Cutland CL, Jones S, et al Duration of infant protection against influenza illness conferred by maternal immunization: Secondary analysis of a randomized clinical trial. JAMA Pediatr 2016;170(9):840-847. https://doi.org/10.1001/jamapediatrics.2016.0921 [ Links ]
60. Omer SB, Clark DR, Aqil AR, et al. Maternal influenza immunization and prevention of severe clinical pneumonia in young infants: Analysis of randomized controlled trials conducted in Nepal, Mali and South Africa. Pediatr Infect Dis J 2018;37(5):436-440. https://doi.org/10.1097/INF.0000000000001914 [ Links ]
61. Cohen C, Walaza S, Treurnicht FK, et al. In- and out-of-hospital mortality associated with seasonal and pandemic influenza and respiratory syncytial virus in South Africa, 2009 - 2013. Clin Infect Dis 2018;66(1):95-103. https://doi.org/10.1093/cid/cix740 [ Links ]
62. McAnerney JM, Cohen C, Moyes J, et al. Twenty-five years of outpatient influenza surveillance in South Africa, 1984 - 2008. J Infect Dis 2012;206(Suppl 1):S153-S158. https://doi.org/10.1093/infdis/jis575 [ Links ]
63. World Health Organization. WHO Guidelines for Epidemic Preparedness and Response to Measles Outbreaks. Geneva: WHO, 1999. [ Links ]
64. Ntshoe GM, McAnerney JM, Archer BN, et al. Measles outbreak in South Africa: Epidemiology of laboratory-confirmed measles cases and assessment of intervention, 2009 - 2011. PLoS ONE 2013;8(2):e55682. https://doi.org/10.1371/journal.pone.0055682 [ Links ]
65. Simani OE, Adrian PV, Violari A, et al. Effect of in-utero HIV exposure and antiretroviral treatment strategies on measles susceptibility and immunogenicity of measles vaccine. AIDS 2013;27(10):1583-1591. https://doi.org/10.1097/QAD.0b013e32835fae26 [ Links ]
66. Jallow S, Cutland CL, Masbou AK, Adrian P, Madhi SA. Maternal HIV infection associated with reduced transplacental transfer of measles antibodies and increased susceptibility to disease. J Clin Virol2017;94:50-56. https://doi.org/10.1016/j.jcv.2017.07.009 [ Links ]
67. World Health Organization. Measles vaccines: WHO position paper. Wkly Epidemiol Rec 2017;92(17):205-228. [ Links ]
68. Mutsaerts EAML, Nunes MC, Bhikha S, et al. Immunogenicity and safety of an early measles vaccination schedule at 6 and 12 months of age in human immunodeficiency virus (HIV)-unexposed and HIV-exposed, uninfected South African children. J Infect Dis 2019;220(9):1529-1538. https://doi.org/10.1093/infdis/jiz348 [ Links ]
69. National Department of Health. 2019 ART Clinical Guidelines for the Management of HIV in Adults, Pregnancy, Adolescents, Children, Infants and Neonates. Pretoria: NDoH, 2019. [ Links ]
70. Lockman S, Hughes M, Powis K, et al. Effect of co-trimoxazole on mortality in HIV-exposed but uninfected children in Botswana (the Mpepu study): A double-blind, randomised, placebo-controlled trial. Lancet Glob Health 2017;5(5):e491-e500. https://doi.org/10.1016/S2214-109X(17)30143-2 [ Links ]
71. Daniels B, Coutsoudis A, Moodley-Govender E, et al. Effect of co-trimoxazole prophylaxis on morbidity and mortality of HIV-exposed, HIV-uninfected infants in South Africa: A randomised controlled, non-inferiority trial. Lancet Glob Health 2019;7(12):e1717-e1727. https://doi.org/10.1016/S2214-109X(19)30422-X [ Links ]
72. Schaaf HS, Cotton MF, Boon GPG, Jeena PM. Isoniazid preventive therapy in HIV-infected and-uninfected children (0 - 14 years) 2013. S Afr Med J 2013;103(10):714-715. https://doi.org/10.7196/SAMJ.7189 [ Links ]
73. Zar HJ, Cotton MF, Strauss S, et al. Effect of isoniazid prophylaxis on mortality and incidence of tuberculosis in children with HIV: Randomised controlled trial. BMJ 2007;334(7585):136. https://doi.org/10.1136/bmj.39000.486400.55 [ Links ]
74. Madhi SA, Nachman S, Violari A, et al. Primary isoniazid prophylaxis against tuberculosis in HIV-exposed children. N Engl J Med 2011;365(1):21-31. https://doi.org/10.1056/NEJMoa1011214 [ Links ]
75. McIlleron H, Denti P, Cohn S, et al. Prevention of TB using rifampicin plus isoniazid reduces nevirapine concentrations in HIV-exposed infants. J Antimicrob Chemother 2017;72(7):2028-2034. https://doi.org/10.1093/jac/dkx112 [ Links ]
76. Seddon JA, Hesseling AC, Finlayson H, et al. Preventive therapy for child contacts of multidrug-resistant tuberculosis: A prospective cohort study. Clin Infect Dis 2013;57(12):1676-1684. https://doi.org/10.1093/cid/cit655 [ Links ]
77. Mofenson LM, Brady MT, Danner SP, et al. Guidelines for the prevention and treatment of opportunistic infections among HIV-exposed and HIV-infected children: Recommendations from CDC, the National Institutes of Health, the HIV Medicine Association of the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the American Academy of Pediatrics. MMWR Recomm Rep 2009;58(Rr-11):1-166. [ Links ]
78. IMpact-RSV Study Group. Palivizumab, a humanized respiratory syncytial virus monoclonal antibody, reduces hospitalization from respiratory syncytial virus infection in high-risk infants. Pediatrics 1998;102(3):531-537. https://doi.org/10.1542/peds.102.3.531 [ Links ]
79. Morris SK, Dzolganovski B, Beyene J, Sung L. A meta-analysis of the effect of antibody therapy for the prevention of severe respiratory syncytial virus infection. BMC Infect Dis 2009;9:106. https://doi.org/10.1186/1471-2334-9-106 [ Links ]
80. Green RJ, Zar HJ, Jeena PM, Madhi SA, Lewis H. South African guideline for the diagnosis, management and prevention of acute viral bronchiolitis in children. S Afr Med J 2010;100(5):320-325.https://doi.org/10.7196/samj.4016 [ Links ]
81. Zar HJ, White DA, Morrow B, et al. The bronchiolitis season is upon us - recommendations for the management and prevention of acute viral bronchiolitis. S Afr Med J 2015;105(7):525-526. https://doi.org/10.7196/SAMJnew.8040 [ Links ]
 Correspondence:
Correspondence:
H J Zar
heather.zar@uct.ac.za
Accepted 10 June 2020.


{kind=link}