










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 no.6 Pretoria Jun. 2020
http://dx.doi.org/10.7196/SAMJ.2020.v110i6.14332
RESEARCH
Lessons learnt during the national introduction of human papillomavirus (HPV) vaccination programmes in 6 African countries: Stakeholders' perspectives
L H AbdullahiI, II; G D HusseyIII, IV; C S WiysongeV, VI; B M KaginaVII, VIII
IMPH, PhD; African Institute for Development Policy (AFIDEP), Nairobi, Kenya
IIMPH, PhD; Vaccines for Africa Initiative, Faculty of Health Sciences, University of Cape Town, South Africa
IIIMB ChB, MMed (Public Health), MSc, FFCH, DTM&H; Vaccines for Africa Initiative, Faculty of Health Sciences, University of Cape Town, South Africa
IVMB ChB, MMed (Public Health), MSc, FFCH, DTM&H; Division of Medical Microbiology, Department of Clinical Laboratory Sciences, Faculty of Health Sciences, University of Cape Town, South Africa
VMD, MPhil, PhD; Cochrane South Africa, South African Medical Research Council, Cape Town, South Africa
VIMD, MPhil, PhD; School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
VIIMSc, PhD; Vaccines for Africa Initiative, Faculty of Health Sciences, University of Cape Town, South Africa
VIIIMSc, PhD; School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND. Infection with human papillomavirus (HPV) significantly increases the risk of developing cervical cancer later in life. Therefore, globally, HPV vaccines targeted to pre-adolescent and adolescent girls have been on the rise since the licensure in 2006. However, the introduction of HPV vaccines has been relatively slow in Africa. At the end of 2016, only 8 of the 54 countries in Africa were reported to have introduced HPV vaccination at a national level. By 2019, the number of countries had grown marginally to 11.
OBJECTIVES. To investigate stakeholders' perspectives on the experiences, challenges and lessons learnt during national HPV vaccine introduction in Africa.
METHODS. A questionnaire was administered to selected participants from 8 African countries. These countries had successfully introduced HPV vaccination at a national level by the end of 2016. We used in-depth interviews and self-administered online questionnaires for data collection and analysis. Data are presented without naming the country or participants; therefore, readers will not be able to identify the results that are specific to individual countries. Narrative and thematic reporting were used to describe the results.
RESULTS. We obtained results from 6 of the 8 targeted countries. The challenges reported during HPV vaccination programmes were: identifying the target population, using a school-based vaccine-delivery strategy, obtaining political support, the need to integrate HPV vaccination with existing school health programmes and engaging multiple stakeholders. These challenges were similar in all 6 countries. The lessons learnt were that a school-based delivery strategy is a successful approach for national HPV vaccination, and that identifying girls for vaccination at schools was less challenging if implemented through a class-based instead of an age-based approach.
CONCLUSIONS. Most African countries do not have established platforms to deliver vaccines to pre-adolescent and adolescent populations. The successful introduction of the HPV vaccine through school-based vaccination strategies in African countries may have created a platform to deliver other adolescent vaccines. The similarity of the study findings across the 6 participating countries further strengthens the need to document and disseminate the challenges and lessons learnt during HPV vaccine introduction in Africa. Documentation and dissemination of the challenges and lessons learnt are useful to other countries in Africa that plan to introduce an HPV vaccination programme, and possibly other adolescent vaccines.
Immunisation programmes play a critical role in the advancement of the public health of communities. Timely and high-quality evidence-informed immunisation policies are critical to strengthen immunisation programmes. Therefore, implementation of global, regional and national immunisation policies plays an important role in combating the burden of vaccine-preventable diseases (VPDs).[1] An important policy strategy to combat VPDs in many countries is the strengthening of the Expanded Programme on Immunisation (EPI) and the introduction of new vaccines. African countries routinely lag behind high-income countries in the introduction of new vaccines.[2] It is therefore not surprising that in 2016, 10 years after human papillomavirus (HPV) vaccine licensure, only a handful of African countries had introduced the vaccine.[3] We conducted a case study to document the experiences and perspectives of key stakeholders during the national HPV vaccine introduction by a few African countries.
Although the EPI mainly targets children, adolescents are a new target population for vaccination.[4] Because the EPI focuses on children, structured delivery of immunisation services to adolescents is suboptimal in many African countries.[5] New vaccines that target adolescents, e.g. against HPV, are now available.[6] Therefore, there is a need to expand the delivery of immunisation services to adolescents in all settings.
African countries are recording a more rapid increase in the number of adolescents than countries on other continents.[7] Therefore, African policymakers should give HPV immunisation the attention it deserves. There is evidence of the benefits of vaccinating adolescents, which include boosting of the waning immunity induced during childhood.[8,9] Furthermore, initiatives on immunisation, such as the Global Immunisation Vision and Strategy (GIVS), Global Vaccine Action Plan (GVAP) and Sustainable Development Goals (SDGs), all supported the call to extend immunisation services to adolescents.[10-12] Therefore, Africa will need to invest more resources and develop national immunisation policies that specifically target adolescents.
Adolescents are infected with HPV through sexual activity. Following HPV infection, there is an increased risk of developing cervical cancer later in life.[13] Therefore, a preventive strategy against HPV infection aims to vaccinate adolescents before sexual debut. Moreover, adolescents are at an increased risk of HIV infection. HIV-infected men and men who have sex with men have an increased risk of anal, penile and throat cancers associated with HPV infection.[14] Worryingly, sub-Saharan Africa and Asia have the highest number of HIV-positive adolescents.[15] Therefore, HPV vaccination policies in Africa should be given due attention to facilitate the introduction of the HPV vaccine that targets adolescents.
Slow uptake of new vaccines in Africa is well documented and HPV vaccine is not an exception.[16] Girls aged 9 - 13 years are the primary target group for HPV vaccination.[17] The rationale for the target age group is prior onset of sexual activity and, therefore, vaccination before infection with the virus.[18,19] Despite the HPV vaccine's proven safety, efficacy and cost-effectiveness, only 8 African countries had reported HPV vaccine introduction at a national level by the end of 2016.[20] These were Libya, Lesotho, Rwanda, Uganda, South Africa (SA), Botswana, Mauritius and Seychelles.[20] By December 2018, 3 additional countries, i.e. Senegal, Zimbabwe and Tanzania, reported implementation of a national vaccination programme against HPV.[21-23] The delay in HPV vaccine introduction in African countries could be due to many reasons, such as the current state of the EPI and health systems, resource limitations and absence of adolescent immunisation programmes.[24] In this study, we evaluated the stakeholders' perspectives on national implementation of a vaccination programme against HPV by 6 African countries.
Specific issues of HPV vaccination delivery include a new target population, costs of the vaccine, most optimal delivery strategy and advocacy.[18] The national departments of health, funding and implementation partners all play a crucial role in the introduction of new vaccines. We are aware of other studies that have documented experiences and guidelines on HPV vaccine introduction in many settings.[25-28] Our study is unique, as we purposefully selected the only African countries that had nationally introduced HPV vaccines during the study period (2015 - 2016). Also, we purposively selected key stakeholders involved in the roll-out of the HPV immunisation programme from the 6 participating countries. The selected key stakeholders had a broader and high-level view of the programme. Our study findings add more context-specific knowledge that is useful to other countries planning to nationally introduce HPV vaccines in Africa.
Objectives
To investigate stakeholders' perspectives during national HPV vaccine introduction by African countries.
Methods
Study design and period
We conducted a cross-sectional study between 2015 and 2016. Mixed methods (quantitative and qualitative) were used for data collection and reporting.
Inclusion criteria
The inclusion criteria comprised all countries in Africa that had implemented national HPV vaccination programmes in 2016.
Sample size
This was not a hypothesis testing study. Hence, we did not calculate the required sample size. Our target sample size included all countries in Africa with national HPV vaccination programmes in 2016. From the 8 African countries that had implemented such a programme, one key representative (convenient sampling) was invited to participate.
Recruitment of stakeholders
In November 2015, we identified and invited key stakeholders representing 5 countries known to have introduced the HPV vaccine nationally as per the Global Alliance for Vaccines and Immunisation (GAVI) website (https://www.gavi.org/). GAVI supports the financing of the HPV vaccine. In November 2016, we invited key stakeholders representing 3 additional countries that had nationally introduced HPV vaccination in 2016. The selection of stakeholders was done through referral sampling (contacts from academics, implementing agencies and governments). Key stakeholders were defined as members of the National Immunization Technical Advisory Group (NITAG), senior officials from the departments of health at national level, as well as representatives from international organisations, such as the World Health Organization (WHO) and United Nations Children's Fund (UNICEF).
Questionnaire administration
The questionnaire was developed and pretested for clarity and accuracy. During the pretesting process, we also developed a guide document with a set of questions aimed at helping the researcher to standardise the process of administering the questionnaires, especially for open-ended questions. The main domains/areas of inquiry in the questionnaire included the following:
• costs of HPV vaccines
• political influence that played a role during introduction of the HPV vaccine
• strategies used during HPV vaccination implementation
• factors that hindered introduction of the HPV vaccine
• challenges and lessons learnt during HPV introduction.
One of the study team members (LHA) administered the questionnaires to all participants. Five stakeholders from 5 countries completed the questionnaires via face-to-face meetings held in November 2015 in SA. The last stakeholder from the 6th country could not attend the meeting, and therefore completed the questionnaire via email. Two stakeholders representing 2 countries were unable to attend the meeting or complete the questionnaire via email.
Missing data
Two representatives from the 7th and 8th countries did not respond to the questionnaires sent to them via email. Follow-up telephone calls to these representatives were unsuccessful.
Data management and analysis
Five of the face-to-face interviews were digitally recorded. These data were coded with ATLAS version 6 (ATLAS.ti, Germany) for analysis. From the questionnaire completed and sent via email, data were abstracted for analysis and reporting. Given the small sample size, data reporting was blinded to the readership - no naming of the country or the participant. Narrative reporting and grouped themes were used to describe the results, based on the most common words and terms that were similar and repetitively used by key representatives.
Ethical approval
Prior to the start of the study, ethical approval was obtained from the Human Research Ethics Committee (HREC) of the Faculty of Health Sciences, University of Cape Town (ref. no. 703/2015). Written participation consent forms were obtained from the stakeholders. Confidentiality was observed during the interview process with the use of blinded transcripts.
Results
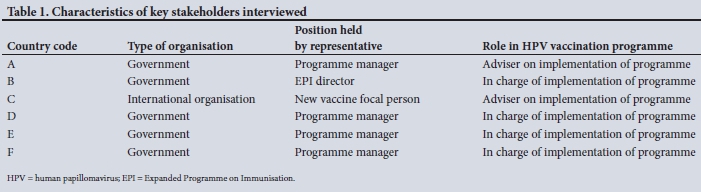
In total, 6 key stakeholders of the 8 targeted stakeholders provided data for this study. The 6 representatives were from 6 different countries. The descriptive characteristics of the 6 representatives interviewed are shown in Table 1.
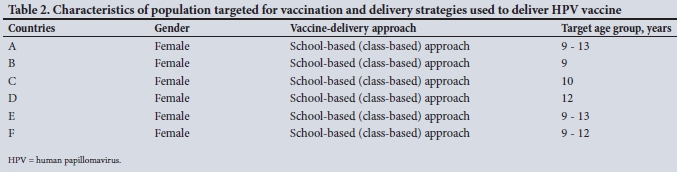
From the 6 participants interviewed, information about the targeted population for vaccination and the HPV vaccination delivery strategy used is provided in Table 2.
Challenges during the implementation of the national HPV vaccination programme
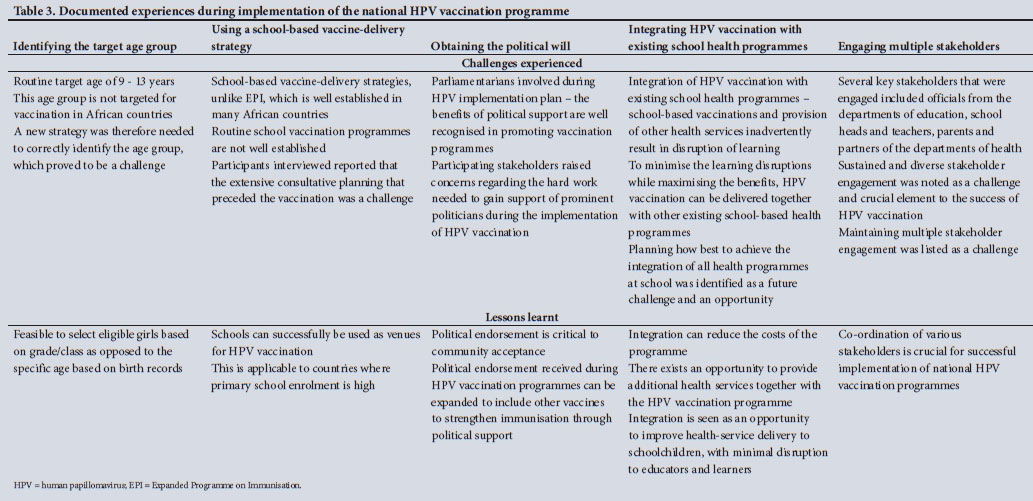
Using data collected from the 6 countries, we grouped the challenges and lessons learnt during the implementation of the national HPV vaccination programme into themes. Thematic challenges and lessons reported by stakeholders were very similar in all 6 countries (Table 3).
The participants from all the countries reported the following challenges: identifying the target population group for HPV vaccination, obtaining political support, using a school-based vaccine-delivery strategy, integrating the HPV vaccination programme with existing school health programmes and engaging multiple stakeholders.
Identifying the target age group
All the countries represented in this study opted to deliver HPV vaccination through the school-based strategy and targeted girls only. At the schools, there was a need to correctly identify girls aged between 10 and 13 years, who are the target group for HPV. However, a challenge was encountered, i.e. whether to use a grade-based or age-based approach to identify the girls for HPV vaccination.
For example, during the piloting of HPV vaccination, country A (Table 3) started with the age group 9 - 18 years, but due to logistical constraints, this target age group could not be optimally reached. Hence, some girls missed the intended HPV vaccination at school and were referred to the nearest health facility. Subsequently, during the national roll-out, all 6 countries reported that the HPV vaccination programme was implemented using a class-based approach. This approach presumed that the targeted age group (10 - 13 years) would be in a given class. The WHO recommends this age group for HPV vaccination, and their guidelines stipulate the HPV vaccination target group by age.[17] In our study, countries that implemented HPV vaccination reported that it was difficult to establish girls' ages. For example, in country B, where 10-year-olds in class 4 were targeted, most girls did not have birth records. As a result, it was difficult to know which girls in the class were 10 years old.
HPV vaccination schedules were synchronised with the academic calendar to avoid loss to follow-up. Furthermore, school teachers played a crucial role to assist in the follow-up, and regularly communicated information on the vaccination dates to the targeted girls. Primary schooling in all 6 participating countries is compulsory; hence, the school-based strategy was chosen as the most efficient to reach the highest number of targeted girls. The school-based delivery strategy was complemented by an outreach strategy, similar to health facility strategies, to vaccinate non-schoolgoing girls.
Using the school-based vaccine-delivery strategy
In Africa, as in the rest of the world, the EPI routinely focuses on delivering vaccination services to children. In the absence of an existing vaccination platform to reach pre-adolescent and adolescent girls with HPV vaccines, a new vaccine-delivery strategy was needed. During the period of HPV vaccine introduction by African countries, there was evidence from high-income countries, e.g. Canada, showing that the school-based programme is feasible.[29]
Participants in our study reported that the introduction of HPV vaccines through the school-based strategy required the departments of health and education to develop a new collaborative partnership. The latter involved that the departments of health EPI programme take the lead with HPV vaccine demonstration initiatives, while the departments of education led the school-based initiatives, such as engagements with learners and parents. The co-ordination of these interdepartmental initiatives for optimal delivery of HPV vaccination was reported as a challenge. Prior engagement meetings between officials from both departments were necessary to ensure complete and on-time dosing of HPV vaccines to the targeted girls. Such engagement meetings were reported to be operationally demanding and time consuming.
Obtaining political support
During the pilot phase, all 6 countries reported that the demonstration results of the HPV vaccination programme were shared with parliamentarians to solicit political support. They showed interest from the start - the political support thus facilitated the necessary commitment from government for upscaling to national level. The 2014 -2020 Africa's Regional Strategic Plan for Immunization was endorsed by ministers of health from the region. [30] The plan is an example of how political will shapes immunisation policies at regional and, by extension, national level. Country C, for example, reported to have received endorsement from the national parliament during HPV vaccine introduction. In country C, the vaccination was launched by the First Lady. Due to political support, it was possible to expedite the planning process, as well as resource mobilisation. Political leadership may change after a limited period, whereas the vaccination programme is a long-term intervention. The participants indicated that a possible lack of political support in the future could compromise the national HPV vaccination programme.
Integrating HPV vaccination with existing school health programmes
Some countries have existing school health programmes (such as vision screening, deworming and nutritional supplementation) for school-aged children who may also be the target group for HPV vaccination. Country B, for example, reported having a vision screening programme among grade 5 learners at primary schools. Grade 5 learners were also targeted by the HPV vaccination programme in the country. Most of the existing school health programmes are characterised by a single visit to the institution by the healthcare providers as opposed to HPV vaccination that, depending on whether there is administration of 2 or 3 doses, requires more than a single visit. Furthermore, health service teams from the health department, and not the HPV vaccination teams, are involved with the existing school health programmes. Two different teams from one department of health visiting the same school with different aims was reported as a challenge. In country B, for example, there was an observed need to harmonise the implementation of these two health programmes (vision screening and HPV vaccination). Although this was reported as a challenge in terms of logistics, it can also be an opportunity to integrate the provision of school health services. Therefore, future plans of many countries are to have new school-based health interventions piggyback on the HPV vaccination programme, provided the additional logistical challenges are addressed.
Engaging multiple stakeholders
Multiple stakeholder engagement was mentioned as a challenge by all participants. Unlike an established EPI, where delivery of vaccination services is routinely common and generally accepted, HPV vaccination was different in many ways, among these being the targeted population (adolescents) and delivery through schools. The multiple stakeholders engaged included parliamentarians, key officials from the departments of education, school heads and teachers, learners and parents. Engaging these multiple stakeholders was reported as time consuming and laborious. Obtaining assents (from learners) or consents (from parents) for vaccination (which is not the case with EPI) was reported as a challenge.
The participating stakeholders highlighted funding challenges that required collaboration of local and international organisations to secure complementary financial, technical and operational support.
Lessons learnt during the implementation of national HPV vaccination programmes in 6 countries
Lesson 1. In school, identifying eligible girls for HPV vaccination based on grade/class is more feasible than by age. However, some eligible girls born after mid-year are likely to be missed during HPV vaccination if already in a higher grade. The proportion of the missed population needs to be quantified.
Lesson 2. School-based delivery strategies can be successfully used to deliver HPV vaccines to learners in African countries with high primary school enrolment. In case of missed vaccination opportunities, healthcare facilities can be used as venues for catchup vaccinations. Delivery of HPV vaccines through school-based programmes may also achieve high coverage levels if there is high-school enrolment in the targeted age group.
Lesson 3. Obtaining political support during the implementation of the HPV vaccination programme is crucial. Political endorsement by national and district government leaders is also critical for community acceptance.
Lesson 4. Integrating an HPV vaccination programme with existing school-based health programmes is a logistical challenge, but also an opportunity, as the integration can reduce the costs of health programmes delivered to school-aged learners.
Lesson 5. Adequate preparation, engaging diverse and relevant stakeholders, including teachers and parents, is crucial to ensure the successful implementation of an HPV vaccination programme.
Lesson 6. Additional support from local and international partners is needed to ensure sustainability of HPV vaccination programmes. Support by local partners is crucial to ensure HPV vaccines reach the hard-to-reach populations in a timely manner.
Discussion
In this study, we identified the challenges and lessons learnt during the implementation of HPV vaccination programmes. Interdepartmental co-ordination, identifying the target age group for HPV vaccination, obtaining political support and engaging multiple stakeholders were reported as the main challenges. These were similar among the African countries that implemented HPV vaccination programmes. The similarities of the challenges across the study countries were surprising, as the continent's immunisation challenges are not homogeneous.[31] However, generally, countries in Africa have many similar competing public health priorities and the continent has lagged behind with diphtheria-tetanus-pertussis (DTP3) immunisation coverage.[31-33]
The delivery of HPV vaccines to schoolgirls required prior engagement and the co-ordination of the departments of health and education. Both departments had to plan around the timing of vaccinating girls during the school day. Additionally, the departments of health had to plan around the logistical delivery of the vaccines and transporting health workers to the schools. Despite these challenges, our results suggest that good leadership and careful co-ordination can overcome these challenges. Furthermore, lessons learnt from this co-ordination can be used to integrate existing and future school-based health interventions with HPV vaccination to expand the delivery of vaccines to adolescents.[34,35]
The WHO guidelines recommend the ideal target population for HPV vaccination as 9 - 13-year-olds, before onset of sexual activity.[17] However, among the participating countries, it was difficult to accurately establish the age of the girls before sexual activity. This is likely to be the case in many African countries that did not participate in the study. Research on sexual debut years for adolescents in Africa can guide optimal choice of age to initiate HPV vaccination.
A few African countries that started to pilot HPV vaccination with an age-based approach used birthdate records to identify the age of girls eligible for vaccination. The age-based approach presented a challenge, as the birthdates were often not available on school records. However, the challenge with the class-based approach was that children who are born mid-year might miss vaccination, as they would have moved to the next class not targeted for HPV vaccination. Hence, if the missed targeted population is large, the effectiveness of HPV vaccination programmes in such countries will be suboptimal, not forgetting that boys are not targeted by the programme. The approach to select girls for HPV vaccination based on grade as opposed to age through a school-based vaccination strategy appeared universally ideal in our study.
The stakeholders alluded to the huge effort needed to obtain political support and reach consensus among diverse and key stakeholders. In all the participating countries, endorsement of the HPV vaccination programme by politicians was a prerequisite. Political leadership that understands and embraces the value and public health benefits of immunisation is therefore crucial for a national HPV vaccination programme in Africa.
Resource mobilisation for HPV vaccination programmes required engagement of diverse stakeholders. Broadly, advocacy and communication were needed to address this challenge. Many African countries, with support from international partners, have made considerable progress to strengthen advocacy and communication on immunisation services.[31] However, in Africa, as is the case globally, much more effort is still needed to improve advocacy and communication with regard to vaccination.[36,37] The lesson learnt from this challenge was that the support by local and international partners, including politicians, is crucial to initiate and sustain HPV vaccination programmes in Africa. The sustainability will need strengthened advocacy and communication, not just for HPV vaccination, but also for other routine immunisation services.
In this study, primary schooling in all 6 countries was compulsory. This made the school-based HPV vaccination strategy the preferred method to reach the highest number of targeted girls. However, school-based vaccination strategies may not be entirely successful in countries with a suboptimal school attendance rate. One study has shown that supplementary immunisation activities, including the use of outreach health facilities, could be an option to target non-school-going adolescents.[38]
We propose collaboration among African countries to document and share the lessons learnt during the introduction of HPV vaccination. A recent study showed high inter-country collaboration on immunisation research in Africa.[39] We identified collaborations that document and share immunisation research information as platforms to foster further discussions on the introduction of other adolescent vaccines. The lessons learnt by countries included in this study can be of great use to other African countries planning to introduce national HPV vaccination programmes.
Conclusions
All 6 countries used schools as the main site for vaccination. Most targeted girls attended school owing to the universal and free primary education programme in these countries. Schools therefore provided an easy and convenient site to access the eligible population. The school team, which included head teachers, teachers and school management, embraced the HPV vaccination programme. School teams worked closely with the departments of health to ensure that there was minimal disruption of classes and that the vaccination day does not coincide with important school programmes, such as examinations. For situations where targeted learners are inevitably absent on vaccination days, a health-facility approach can be used to catch up. As African countries continue to introduce HPV vaccines nationally, we recommend documentation and sharing of experiences. In this way, introduction of HPV vaccines will be guided by locally relevant experiences.
Study limitations and validity
Of 54 African countries, findings for this study are from 6 countries only for reasons provided in the abovementioned methods section. This limitation is further compounded by having interviewed only one representative per country. Therefore, extrapolation of the findings to the entire continent must be done with caution. Another limitation is the use of questionnaires alone to collect data, without conducting focus group discussions. This was because of resource limitations.
Study strengths
• The study focus is on countries in Africa implementing HPV vaccination. This has not been evaluated before by using a similar methodology to ours. Although few countries are represented, the experiences are rich and useful in the African context.
• There is a paucity of knowledge on adolescent immunisation in Africa. Therefore, this study contributes to the knowledge base in the field.
• Documentation and dissemination of the challenges and lessons learnt are useful to other countries in Africa that plan to introduce the HPV vaccination programme.
Study weaknesses
• HPV implementation in Africa is a new concept and its implementation is slow - therefore the small sample size. We have also not included the countries that have recently (2018 and 2019) introduced HPV vaccination.
• The respondents gave similar experiences and challenges of a school-based programme as a successful platform. Therefore, the study might not have information for the countries that need to attempt other methods of implementing HPV vaccination, such as health-facility-based programmes.
Declaration. None.
Acknowledgements. None.
Author contributions. GDH and BMK conceived the study and provided overall leadership. LHA conducted the study and wrote the drafts of the manuscript, with support from BMK, CSW and GDH. All authors reviewed and approved the final manuscript.
Funding. LHA and CSW were supported by the South African Medical Research Council.
Conflicts of interest. None.
References
1. World Health Organization. Immunization policy and strategies. 2017. http://www.who.int/immunization/programmes_systems/policies_strategies/en/ (accessed 15 December 2018). [ Links ]
2. Haddison E, Machingaidze S, Wiysonge C, Hussey G, Kagina B. Mapping the evidence-base of adolescent and adult vaccination in Africa: A slow but growing trend. J Vaccines Immunol 2019;5(1):011-017. https://doi.org/10.17352/JVI.000024 [ Links ]
3. Bruni L, Diaz M, Barrionuevo-Rosas L, et al. Global estimates of human papillomavirus vaccination coverage by region and income level: A pooled analysis. Lancet Glob Health 2016;4(7):e453-e463. https://doi.org/10.1016/S2214-109X(16)30099-7 [ Links ]
4. Okwo-Bele JM, Cherian T. The expanded programme on immunization: A lasting legacy of smallpox eradication. Vaccine 2011;29(Suppl 4):D74-D79. https://doi.org/10.1016/j.vaccine.2012.01.080 [ Links ]
5. World Health Organization/United Nations Children's Fund. Coverage estimates 2015 revision, for 194 WHO member states. 2016. http://www.who.int/immunisation/monitoring_surveillance/who-immuniz-2015.pdf?ua=1 (accessed 15 December 2018). [ Links ]
6. Serdobova I, Kieny MP. Assembling a global vaccine development pipeline for infectious diseases in the developing world. Am J Public Health 2006;96(9):1554-1559. https://doi.org/10.2105/AJPH.2005.074583 [ Links ]
7. United Nations Population Fund. States of the world population. The power of1.8 billion. 2014. http://www.unfpa.org/swop-2014 (accessed 15 December 2018). [ Links ]
8. World Health Organization. WHO Recommendations for Routine Immunization. Geneva: WHO, 2016. [ Links ]
9. Brabin L, Greenberg DP, Hessel L, Hyer R, Ivanoff B, van Damme P. Current issues in adolescent immunization. Vaccine 2008;26(33):4120-4134. https://doi.org/10.1016/j.vaccine.2008.04.055 [ Links ]
10. Wolfson LJ, Gasse F, Lee-Martin SP, et al. Estimating the costs of achieving the WHO-UNICEF global immunization vision and strategy, 2006 - 2015. Bull World Health Organ 2008;86(1):27-39. https://doi.org/10.2471/blt.07.045096 [ Links ]
11. Decade of Vaccines Collaboration. Global vaccine action plan. Vaccine 2013;31(Suppl 2):B5-B31. https://doi.org/10.1016/j.vaccine.2013.02.015 [ Links ]
12. United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. New York: UN, 2015. [ Links ]
13. World Health Organization. Human papillomavirus vaccines: WHO position paper. Weekly Epidemiol Rec 2014;43(89):465-492. [ Links ]
14. Palefsky JM, Moscicki A-B. HPV in men: An update. J Low Genit Tract Dis 2011;15(3):231-234. https://doi.org/10.1097/LGT.0b013e318203ae61 [ Links ]
15. Kharsany AB, Karim QA. HIV infection and AIDS in sub-Saharan Africa: Current status, challenges and opportunities. Open AIDS J 2016;10:34-48. https://doi.org/10.2174/1874613601610010034 [ Links ]
16. Greenwood B. The contribution of vaccination to global health: Past, present and future. Philos Trans R Soc Lond B Biol Sci 2014;369(1645):20130433. https://doi.org/10.1098/rstb.2013.0433 [ Links ]
17. World Health Organization. Summary of the WHO position paper on vaccines against human papillomavirus (HPV). 2017. http://www.who.int/immunization/policy/position_papers/pp_hpv_may2017_summary.pdf?ua=1 (accessed 15 December 2018). [ Links ]
18. Wigle J, Coast E, Watson-Jones D. Human papillomavirus (HPV) vaccine implementation in low- and middle-income countries (LMICs): Health system experiences and prospects. Vaccine 2013;31(37):3811-3817. https://doi.org/10.1016/j.vaccine.2013.06.016 [ Links ]
19. Jumaan AO, Ghanem S, Taher J, Braikat M, Al Awaidy S, Dbaibo GS. Prospects and challenges in the introduction of human papillomavirus vaccines in the extended Middle East and North Africa region. Vaccine 2013;31(Suppl 6):G58-G64. https://doi.org/10.1016/j.vaccine.2012.06.097 [ Links ]
20. Cervical Cancer Action. Global progress in HPV vaccination. 2017. http://www.cervicalcanceraction.org/comments/comments3.php (accessed 15 December 2018). [ Links ]
21. Learning network for countries in transition (LNCT). Senegal becomes the first GAVI-supported country in West Africa to introduce HPV vaccine into its routine immunization program. 2018. https://lnct.global/2018/11/12/senegal-becomes-the-first-gavi-supported-country-in-west-africa-to-introduce-hpv-vaccine-into-its-routine-immunization-program/ (accessed 15 December 2018). [ Links ]
22. World Health Organization. Tanzania rolls out vaccination against cervical cancer. 2018. https://www.afro.who.int/news/tanzania-rolls-out-vaccination-against-cervical-cancer (accessed 15 December 2018). [ Links ]
23. JSI. Lessons learned - HPV vaccine nationwide introduction in Zimbabwe. 2018. https://jsi.com/JSIInternet/Inc/Common/_download_pub.cfm?id=21927&lid=3 (accessed 15 December 2018). [ Links ]
24. Zipursky S, Wiysonge CS, Hussey G. Knowledge and attitudes towards vaccines and immunization among adolescents in South Africa. Hum Vaccines 2010;6(6):455-461. https://doi.org/10.4161/hv.6.6.11660 [ Links ]
25. World Health Organization. Guide to introducing HPV vaccine into national immunization programmes. 2016. https://apps.who.int/iris/bitstream/handle/10665/253123/9789241549769-eng.pdf;jsessionid=584A2089CE3F3E4ACEE5398811ED4003?sequence=1 (accessed 15 December 2018). [ Links ]
26. World Health Organization. Scaling-up HPV vaccine introduction. 2016. https://apps.who.int/iris/bitstream/handle/10665/251909/9789241511544-eng.pdf?sequence=1 (accessed 15 December 2018). [ Links ]
27. World Health Organization. School vaccination readiness assessment tool. 2016. https://apps.who.int/iris/bitstream/handle/10665/90566/WHO_IVB_13.02_eng.pdf?sequence=1 (accessed 15 December 2018). [ Links ]
28. World Health Organization. Considerations regarding consent in vaccinating children and adolescents between 6 and 17 years old. 2016. https://apps.who.int/iris/bitstream/handle/10665/259418/WHO-IVB-14.04-eng.pdf?sequence=1 (accessed 15 December 2018). [ Links ]
29. Lim WT, Sears K, Smith LM, Liu GY, Levesque LE. Evidence of effective delivery of the human papillomavirus (HPV) vaccine through a publicly funded, school-based program: The Ontario Grade 8 HPV Vaccine Cohort Study. BMC Publ Health 2014;14:1029. https://doi.org/10.1186/1471-2458-14-1029 [ Links ]
30. World Health Organization. Regional Office for Africa. Regional Strategic Plan for Immunization 2014 - 2020. Brazzaville: WHO, 2015. [ Links ]
31. Arevshatian L, Clements CJ, Lwanga SK, et al. An evaluation of infant immunization in Africa: Is a transformation in progress? Bull World Health Organ 2007;85(6):449-457. https://doi.org/10.2471/blt.06.031526 [ Links ]
32. Wiysonge CS. Why Africa is lagging behind in child vaccination. 2015. The conversation. https://theconversation.com/why-africa-is-lagging-behind-in-child-vaccination-48699 (accessed 15 December 2018). [ Links ]
33. Mihigo R, Okeibunor J, Anya B, Mkanda P, Zawaira F. Challenges of immunisation in the African region. Pan Afr Med J 2017;27(3):12. https://doi.org/10.11604/pamj.supp.2017.27.3.12127 [ Links ]
34. Clayton S, Chin T, Blackburn S, Echeverria C. Different setting, different care: Integrating prevention and clinical care in school-based health centers. Am J Public Health 2010;100(9):1592-1596. https://doi.org/10.2105/AJPH.2009.186668 [ Links ]
35. Broutet N, Lehnertz N, Mehl G, et al. Effective health interventions for adolescents that could be integrated with human papillomavirus vaccination programs. J Adolesc Health 2013;53(1):6-13. [ Links ]
36. Wittet S, Aylward J, Cowal S, et al. Advocacy, communication, and partnerships: Mobilizing for effective, widespread cervical cancer prevention. Int J Gynecol Obstet 2017;138:57-62. https://doi.org/10.1002/ijgo.12189 [ Links ]
37. World Health Organization. HPV Vaccine Communication. Special Considerations for a Unique Vaccine. Geneva: WHO, 2016. [ Links ]
38. Haddison EC, Abdullahi LH, Muloiwa R, Hussey GD, Kagina BM. Comparison of school based and supplemental vaccination strategies in the delivery of vaccines to 5 - 19 year olds in Africa - a systematic review. F1000Res 2017;6:1833. https://doi.org/10.12688/f1000research.12804.1 [ Links ]
39. Haddison EC, Wiysonge CS, Hussey GD, Kagina BM. An update on trends in the types and quality of childhood immunization research outputs from Africa 2011 - 017: Mapping the evidence base. Vaccine X 2019;1:100001. https://doi.org/10.1016/j.jvacx.2018.100001 [ Links ]
 Correspondence:
Correspondence:
L H Abdullahi
leylaz@live.co.za
Accepted 21 November 2019


{kind=link}
{kind=link}
{kind=link}