










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 no.6 Pretoria jun. 2020
http://dx.doi.org/10.7196/SAMJ.2020.v110i6.14123
RESEARCH
Predictors of 1-year survival in South African transcatheter aortic valve implant candidates
J J LiebenbergI; A DoubellII; J van WykIII; M KiddIV; T MabinV; H WeichVI
IMB ChB; Division of Cardiology, Department of Internal Medicine, Tygerberg Hospital and Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
IIMB ChB, MMed (Int Med), FCP (SA), PhD; Division of Cardiology, Department of Internal Medicine, Tygerberg Hospital and Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
IIIMB ChB, MMed (Thorac), FCS (Cardio); Mediclinic Panorama, Bellville, Cape Town, South Africa
IVPhD (Statistics); Centre for Statistical Consultation, Stellenbosch University, South Africa
VMB ChB, FRCP, FACC, FESC; Mediclinic Vergelegen, Somerset West, South Africa
VIMB ChB, MRCP, MMed (Int), Cert Cardiol (SA); Division of Cardiology, Department of Internal Medicine, Tygerberg Hospital and Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
ABSTRACT
BACKGROUND. Transcatheter aortic valve implantation (TAVI) has undergone rapid expansion internationally over the past 15 years. In view of resource constraints in developing countries, a major challenge in applying this technology lies in identifying patients most likely to benefit. The development of a risk prediction model for TAVI has proved elusive, with a reported area under the curve (AUC) of 0.6 - 0.65. The available models were developed in a First-World setting and may not be applicable to South Africa (SA).
OBJECTIVES. To evaluate novel indicators and to develop a TAVI risk prediction model unique to the SA context. The current work represents the important initial steps of derivation cohort risk model development and internal validation.
METHODS. Seven-year experience with 244 successive TAVI implants in three centres in Western Cape Province, SA, was used to derive risk parameters. All outcomes are reported in accordance with the Valve Academic Research Consortium definitions. Multiple preprocedural variables were assessed for their impact on 1-year survival using univariate and multivariate models.
RESULTS. Factors found not to correlate with 1-year survival included age, renal function and aortic valve gradients. The commonly used surgical risk prediction models (Society of Thoracic Surgeons score and EuroSCORE) showed no correlation with outcomes. Factors found to correlate best with 1-year survival on multivariate analysis were preprocedural body mass index (BMI) (favouring higher BMI), preprocedural left ventricular end-diastolic dimension (LVED) and ejection fraction (EF) (favouring smaller LVED and higher EF), absence of atrial fibrillation, and three novel parameters: independent living, ability to drive a car, and independent food acquisition/ cooking. Discriminant analysis of these factors yielded an AUC of 0.8 (95% confidence interval 0.7 - 0.9) to predict 1-year survival, with resubstitution sensitivities and specificities of 72% and 71%, respectively.
CONCLUSIONS. Apart from existing predictors, we identified three novel risk predictors (independent living, ability to drive a car, and independent food acquisition/cooking) for 1-year survival in TAVI candidates. These novel parameters performed well in this early evaluation, with an AUC for predicting 1-year survival higher than the AUCs for many of the internationally derived parameters. The parameters are inexpensive and easy to obtain at the initial patient visit. If validated prospectively in external cohorts, they may be applicable to other resource-constrained environments.
The first successful transcatheter aortic valve implant (TAVI) in 2002[1] signalled the start of an era in which the definitive treatment of patients with aortic stenosis and a prohibitively high surgical risk became a reality. This exciting treatment modality has evolved from a salvage procedure in the extreme-risk patient to being investigated for patients at intermediate and even low surgical risk.[2-5] Despite the publication of local experience with TAVI over the past 7 years, demonstrating results comparable to those reported in the pivotal international PARTNER A trial in high-risk patients,[5] rapid expansion of the procedure as seen elsewhere has not been evident in South Africa (SA). An important obstacle is reluctance of many health funders to accept it as a valid alternative for the intermediate-or high-risk patient. A recent report shows success rates >90%, with low rates of adverse outcomes (stroke, vascular complications) and a 1-year survival rate of 81% with sustained improvement in clinical, functional and echocardiographic parameters.[6]
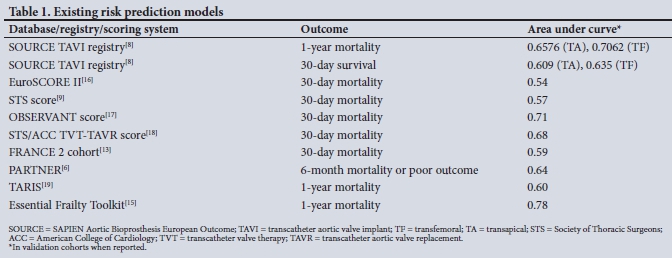
A major challenge in applying this new technology lies in the prediction of which patient is most likely to benefit. Over the decade and a half since the first TAVI, various attempts have been made to develop risk prediction models (Table 1). The predictive ability of most of these models was relatively disappointing, with inadequately powered area under the curve (AUC) values ranging from 0.6 to 0.65. These risk prediction scores (the logistic EuroSCORE,[7] EuroSCORE II[8] and Society of Thoracic Surgeons (STS) predicted risk of mortality[9]) are used routinely as there are few alternatives.
An important factor influencing the local validity of existing prediction models is the heterogeneity of the elderly populations and medical landscapes in TAVI registries globally. Significant differences exist between numerous indicators of health in developed countries and SA, including socioeconomic status, access to medical care, level of education and health-seeking behaviour. For example, there may be a big difference between an 85-year-old living independently in SA and one in the UK, or an 80-year-old who drives a car in SA and an age-matched counterpart in Japan. Further to that, in terms of the medical landscape, healthcare funding and access to specialised investigations and functional assessments are less readily available here compared with countries where many of the existing models were developed.
Objectives
We postulate that unique prediction parameters exist for the SA TAVI community, stemming from the local patient profile as well as from the SA healthcare system. We used the data from a 7-year experience with TAVI in a private-public partnership initiative to develop the initial phases of a risk prediction model specific to the SA TAVI patient cohort. The ultimate goal is to develop a validated and operational risk prediction model. In this article we address the important initial steps of derivation cohort model development and internal validation.
The process of developing a risk prediction model includes multivariate analyses of factors thought to predict outcome, followed by an internal validation process. Once a model has been established from the derivation cohort, it is subjected to external validation processes using larger patient cohorts. The model can then undergo updating and revisions. Finally, the model has to be subjected to impact studies to assess influence on behaviour and (self-) management of doctors and individuals, and subsequently on health outcomes and cost-effectiveness, before being fully operational.[10]
Methods
The research was approved by the Health Research and Ethics Committee of Stellenbosch University on 23 June 2016 (ref. no. N16/01/005). All processes were conducted in accordance with the Declaration of Helsinki. No patient interaction was sought during the course of the research, as we retrospectively reported from a registry that was kept during the course of good clinical practice. All patient data were anonymised and aggregated at the point of data entry.
The data used to develop this derivation cohort risk prediction model came from 7-year experience (October 2009 - September 2016) with 244 consecutive TAVI procedures at two hospitals (Panorama Mediclinic and Vergelegen Mediclinic) in Western Cape Province, SA. From November 2014 onwards, the patients' data were also entered into a parallel national registry (SHARE-TAVI registry), which was not used for the current report. A multiplicity of preprocedural parameters as well as 1-year outcomes were collected prospectively as part of routine practice and clinical audit. All definitions are reported in accordance with the Valve Academic Research Consortium recommendation, which reflects validated and comparable measures of outcome and clinical efficacy.[11]
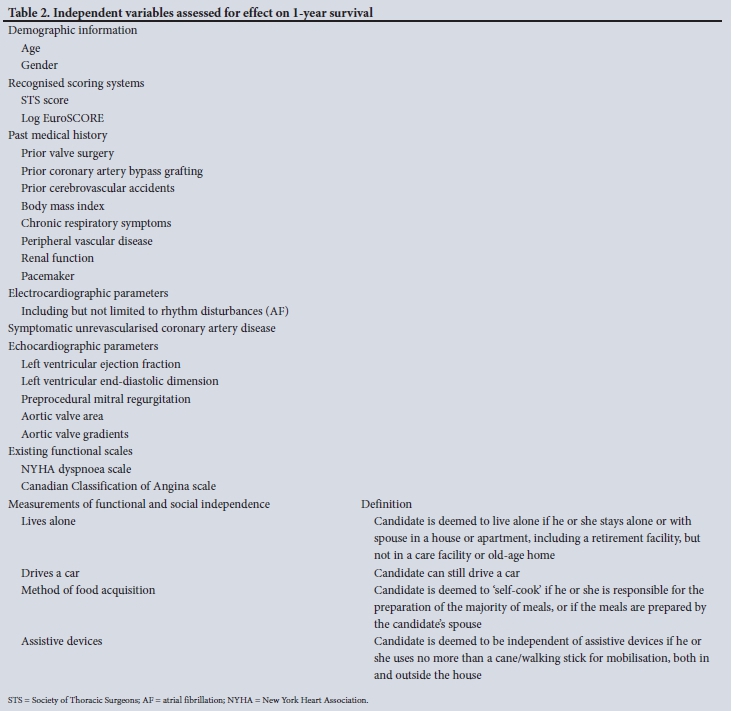
The independent variables that were assessed for their associations with 1-year survival included a wide array of clinical, standard anthropometric, echocardiographic and biochemical data. Importantly, because of limited formal support structures in SA, we included a number of unique parameters listed under 'Measurements of functional and social independence' (see Table 2 for independent variables assessed with definitions). The composite endpoint/ dependent variable was 1-year all-cause mortality/survival rates.
Statistical analysis
For univariate analysis of possible predictors of 1-year survival, receiver operating characteristic (ROC) curve analyses were used for continuous predictors, and cross-tabulation with the x2 test for categorical predictors. Factors predictive of 1-year outcomes using univariate analysis were used in multivariate analysis. Multivariate models were fitted using logistic regression to report odds ratios (ORs), and discriminant analysis to get an indication of prediction accuracy. For the latter, leave-one-out cross-validation was used as a measure of prediction accuracy (sensitivity and specificity). In the abovementioned measure, cases are omitted one by one, and prediction models (excluding the selected case) are used to predict the selected case.
Results
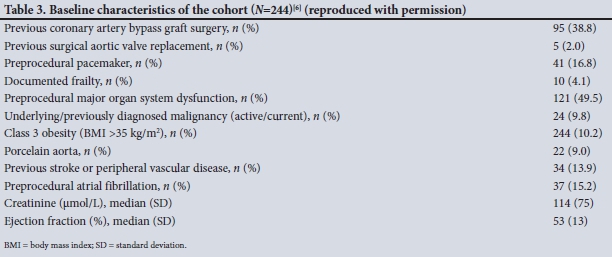
The patient profile and outcomes of this cohort have been reported previously.[6] In brief, all participants were assessed by the heart valve team and found to have a prohibitively high risk for surgical valve replacement. The baseline characteristics demonstrated a male preponderance (56%) and a mean age of 80 years. The average EuroSCORE and STS score was 26.5% and 7.89%, respectively, which is comparable to previous flagship TAVI trials.[2] Of the 244 patients who received TAVI during this period, 75% received the Edwards SAPIEN valve and the remaining 25% received the Medtronic CoreValve. The preferred vascular access route was the transfemoral (73%), followed by transapical (17%) and transaortic (10%). The baseline comorbidity rates are shown in Table 3. For the current analysis, 1-year outcome data were available for 95% of the 244 participants.
Univariate results
Continuous variables. Table 4 shows univariate associations that continuous variables had with 1-year survival. The direction of effect was such that higher body mass index (BMI), smaller left ventricular end-diastolic diameter (LVED), higher ejection fraction (EF) and smaller aortic valve area (AVA) were associated with better 1-year survival. Notably, the majority of the factors, including age and renal function, were not associated with 1-year survival. There was no demonstrable association between the EuroSCORE and STS score and outcomes.
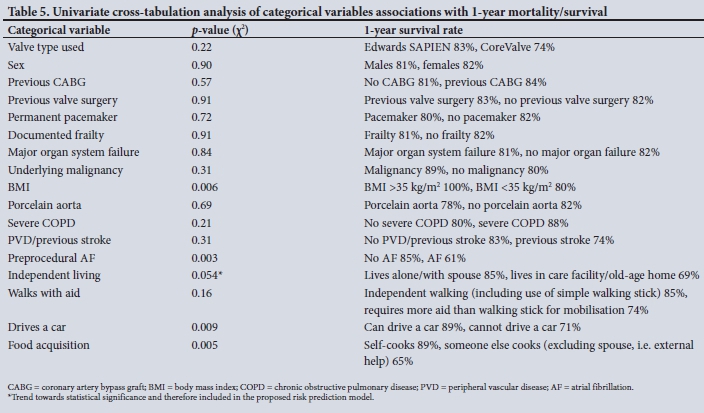
Categorical variables. Table 5 shows univariate associations that categorical variables had with 1-year survival. The level of the effect was such that 1-year survival was favoured by BMI >35 kg/m2, absence of atrial fibrillation, independent living, ability to drive a car, and self-acquisition (or via spouse) of most meals (see definitions).
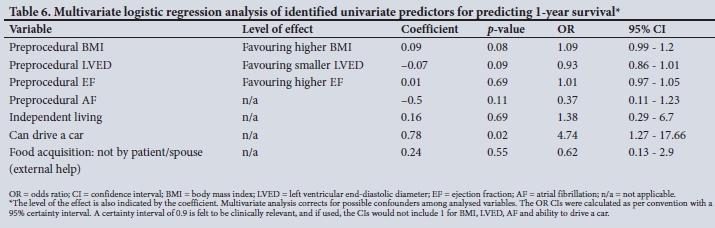
Multivariate results
The factors identified as correlating with outcome on the univariate analysis were used in multivariate testing. Table 6 shows respective p-values and ORs for predicting 1-year survival in a multivariate logistic regression model. Using discriminant analysis of predictors in Table 6 yielded an AUC of 0.8 (95% confidence interval (CI) 0.7 - 0.9) to predict 1-year survival, with resubstitution sensitivities and specificities of 72% and 71%, respectively (Fig. 1). Leave-one-out cross-validation yielded sensitivities and specificities for predicting 1-year survival of 63% and 67%, respectively.

Optimising the risk prediction model's sensitivity for detecting 1-year survival to a maximum of 85% yielded lower specificity for detecting 1-year survival of only 35%. Conversely, the model can be optimised to a maximum specificity of 88%, with a sensitivity of 58%.
Discussion
The factors identified as predictors of outcome and hence proposed components of a risk prediction model (subject to external validation) were derived from the largest SA TAVI outcome report.[6] The rationale for evaluating these locally derived factors was to address the lack of satisfactory prediction models as well as the global heterogeneity in the health of the elderly as well as in healthcare systems. Our results can be summarised as the identification of seven parameters, three of which are novel, yielding promising predictive abilities for 1-year survival. Importantly in the context of local constraints, all the parameters identified are easily obtained during the interview with the patient and with a good-quality transthoracic echocardiogram, and do not involve complex, laborious and expensive functional, biochemical and psychometric testing. The novel components of the model are not operator dependent. Our study adds to the growing body of evidence that functional parameters of self-care and independence in activities of daily living are of principal importance in predicting success or futility post TAVI.
Despite the enthusiasm for expansion of TAVI indications to lower-risk groups, it is possible that a number of patients fail to derive long-term benefit in terms of survival and functional improvement. [12] The importance of careful patient selection can therefore not be overemphasised, both to be responsible in terms of resources and to ensure favourable patient outcomes and avoid futile procedures.
The difficulty in predicting risk in the TAVI community was identified in earlier attempts from the SOURCE (SAPIEN Aortic Bioprosthesis European Outcome) registry, where a satisfactory risk prediction model remained elusive despite analysis of comprehensive data on >1 000 patients undergoing TAVI.[8] The SOURCE registry contains procedural, 3-day and 1-year follow-up data for 1 038 patients who had undergone TAVI at 32 European and African centres between November 2007 and January 2009. Multivariate analysis identified several factors that correlated with increased risk for 1-year mortality:
Transapical group. EuroSCORE, renal disease, liver disease, carotid artery stenosis >50% (in counterintuitive direction).
Transfemoral group. New York Heart Association (NYHA) class IV renal disease, smoking, hypercholesterolaemia (in counterintuitive direction), and complete absence of any cardiovascular condition.
These multivariate analysis prognostic factors achieved a modest C-statistic of 0.65 for the transapical patients and 0.70 for the transfemoral patients. A C-statistic of <0.7 is of little or no clinical significance, and a C-statistic of 0.5 would be similar to a chance outcome. The research concluded that the factors identified as prognostic factors in the SOURCE registry data are likely to be of only limited value in developing a clinical prediction model.
The most important baseline predictors of poor outcome in the PARTNER trial were reduced exercise capacity, lower mean aortic valve gradients, oxygen-dependent chronic lung disease, chronic kidney disease and poor baseline cognition. Yet these factors yielded modest discrimination ability, with C-statistics of 0.66 and 0.64 in derivation and validation cohorts, respectively.[4]
Another attempt by Gilard et al.[13] using the FRANCE 2 cohort identified nine factors correlating with 30-day post-TAVI outcomes. Similarly, relatively disappointing C-statistics of 0.67 and 0.59 were seen in the derivation and validation cohorts, respectively.[13]
The predictive ability and applicability of conventional risk models (EuroSCORE II and STS score), even in the surgical community, is a point of ongoing research owing to the changing risk profile of surgical patients, the marked improvement in surgical outcomes compared with the 1990s, and changes in surgical techniques. In a recent study evaluating the predictive ability of the STS score in surgical valve replacement, a C-statistic of 0.791 was found.[14] The STS score also possessed very modest predictive ability for 30-day TAVI mortality, with an area under the ROC curve of 0.674 (95% CI 0.541 - 0.807).[14]
Most recently, the role of cardiac biomarkers as possible predictors of unfavorable outcomes was assessed. The current understanding is that they may enrich current risk scores, but larger studies are still needed to clarify their role.[14] The most accurate outcome prediction model for TAVI candidates to date has come from the FRAILTY-AVR study. Afilalo et al.[15] propose the Essential Frailty Toolset (EFT) as the preferred frailty scale, with an AUC of 0.784 (95% CI 0.745 - 0.822).
The components of the model are lower-extremity weakness, cognitive impairment, anaemia and hypoalbuminaemia. The model was also a predictor of worsening disability at 1 year. [15] The applicability of these scores remains unclear in the SA community (see Table 1 for results of previous prediction models in the TAVI community).
In our current work we have shown no correlation between 1-year survival and the majority of univariate factors assessed; notably, no outcome correlation was found for EuroSCORE, age, renal function and STS score. This echoes the peculiarity that intuitive factors do not necessarily predict outcome well. We present seven independent variables, which in our cohort attained a C-statistic of 0.8 in predicting 1-year survival. Although it is known that risk prediction models often over-perform in the cohorts they were derived from, and hence real-life predictive ability may be poorer, our work not only represents an improvement in the risk-predictive abilities of the factors identified by the SOURCE registry, but also outperforms the STS score in predicting risk. The first two parameters (EF and LVED) are continuous variables and showed a linear correlation with 1-year survival, so that smaller LVED and higher EF favoured survival. The other five parameters are categorical variables. Each parameter has a relative contribution/weight based on the coefficient during the multivariate logistic regression. Although AVA was associated with 1-year survival on univariate testing, it did not contribute significantly in the multivariate analysis and was omitted in the final model. We have omitted the final mathematical depiction of the model and chose only to publish the seven variables, as the model cannot be regarded as operational yet and needs to be prospectively validated on an external cohort of TAVI candidates.
Study limitations
The first limitation is that data collection stretched over a 7-year period during which there has been significant improvement in patient outcomes, attributable to growing expertise of the heart valve team and device development. Second, the research was subjected to the limitations of a retrospective design, with the investigators being limited in assessing factors that we collected during the implantation period. Third, although this is the largest published local cohort of TAVI patients, the sample size is still relatively small (e.g. compared with the SOURCE registry) and is subject to the limitations of a relatively small sample size. Finally, it must be stressed that the current work should not be regarded as a functional risk prediction model, but merely as the first step towards developing such a model that has withstood external validation.
Conclusions
We present the initial phases in the development of a TAVI risk prediction model derived from SA data. We postulate that the model will have greater applicability to the local community than models derived from international literature. The seven parameters, three of which are novel in TAVI literature, are tailored for the constraints of the SA medical community and show promising results in their combined capacity to predict 1-year survival. If the predictive ability of these variables survives the scrutiny of prospective external validation, they could prove to be a valuable asset in the assessments of TAVI patients in SA.
Declaration. The research for this study was done in partial fulfilment of the requirements for JJL's MMed (Int Med) degree at Stellenbosch University.
Acknowledgements. None.
Author contributions. All authors contributed equally to this published work.
Funding. None.
Conflicts of interest. None.
References
1. Reardon MJ, van Mieghem NM, Popma JJ, et al. Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J Med 2017;376(14):1321-1331. https://doi.org/10.1056/NEJMoa1700456 [ Links ]
2. Rogers T, Thourani VH, Waksman R. Transcatheter aortic valve replacement in intermediate- and low-risk patients. J Am Heart Assoc 2018;7(10). https://doi.org/10.1161/JAHA.117.007147 [ Links ]
3. Leon MB, Smith CR, Mack MJ, et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med 2016;374(17):1609-1620. https://doi.org/10.1056/NEJMoa1514616 [ Links ]
4. Abdelghani M, Serruys PW. Transcatheter aortic valve implantation in lower-risk patients with aortic stenosis. Circ Cardiovasc Interv 2016;9(4):e002944. https://doi.org/10.1161/CIRCINTERVENTIONS.115.002944 [ Links ]
5. Arnold SV, Reynolds MR, Lei Y, et al. Predictors of poor outcomes after transcatheter aortic valve replacement: Results from the PARTNER Trial. Circulation 2014;129(25):2682-2690. https://doi.org/10.1161/CIRCULATIONAHA.113.007477 [ Links ]
6. Weich H, Liebenberg J, van Wyk J, et al. 7-year experience of transcatheter aortic valve implants (TAVI) in a Western Cape private healthcare setting. SA Heart 2019;16:6-12. [ Links ]
7. Swinkels BM, Plokker HW. Evaluating operative mortality of cardiac surgery: First define operative mortality. Neth Heart J 2010;18(7-8):344-345. https://doi.org/10.1007/bf03091788 [ Links ]
8. Thomas M, Schymik G, Walther T, et al. Thirty-day results of the SAPIEN Aortic Bioprosthesis European Outcome (SOURCE) Registry. Circulation 2010;122(1):62-69. https://doi.org/10.1161/CIRCULATIONAHA.109.907402 [ Links ]
9. Hermiller JB Jr, Yakubov SJ, Reardon MJ, et al.; CoreValve United States Clinical Investigators. Predicting early and late mortality after transcatheter aortic valve replacement. J Am Coll Cardiol 2016;68(4):343-352. https://doi.org/10.1016/j.jacc.2016.04.057 [ Links ]
10. Moons KGM, Kengne AP, Grobbee DE, et al. Risk prediction models: II. External validation, model updating, and impact assessment. Heart 2012;98(9):691-698. https://doi.org/10.1136/heartjnl-2011-301247 [ Links ]
11. Kappetein AP, Head SJ, Généreux P, et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document (VARC-2). Eur J Cardiothorac Surg 2012;42(5):S45-S60. https://doi.org/10.1093/ejcts/ezs533 [ Links ]
12. Puri R, Iung B, Cohen DJ, Rodés-Cabau J. TAVI or no TAVI: Identifying patients unlikely to benefit from transcatheter aortic valve implantation. Eur Heart J 2016;37(28):2217-2225. https://doi.org/10.1093/eurheartj/ehv756 [ Links ]
13. Gilard M, Eltchaninoff H, Iung B, et al. Registry of transcatheter aortic-valve implantation in high-risk patients. Surv Anesthesiol 2013;57(2):62-63. https://doi.org/10.1097/01.SA.0000426523.25196.4e [ Links ]
14. Balan P, Zhao Y, Johnson S, et al. The Society of Thoracic Surgery Risk Score as a predictor of 30-day mortality in transcatheter vs surgical aortic valve replacement: A single-center experience and its implications for the development of a TAVR risk-prediction model. J Invasive Cardiol 2017;29(3):109-114. [ Links ]
15. Afilalo J, Lauck S, Kim DH, et al. Frailty in older adults undergoing aortic valve replacement: The FRAILTY-AVR Study. J Am Coll Cardiol 2017;70(6):689-700. https://doi.org/10.1016/j.jacc.2017.06.024 [ Links ]
16. Nashef SAM, Roques F, Sharples LD, et al. EuroSCORE II. Eur J Cardiothorac Surg 2012;41(4):734-745. https://doi.org/10.1093/ejcts/ezs043 [ Links ]
17. Capodanno D, Barbanti M, Tamburino C, et al. A simple risk tool (the OBSERVANT score) for prediction of 30-day mortality after transcatheter aortic valve replacement. Am J Cardiol 2014;113(11):1851-1858. https://doi.org/10.1016/j.amjcard.2014.03.014 [ Links ]
18. Reiff C, Gurevich S, Bertog S, Sorajja P, Kelly R, Garcia S. Validation of STS/ACC TVT-TAVR score in veterans undergoing transcatheter aortic valve replacement. J Invasive Cardiol 2018;30(12):447-451. [ Links ]
19. Seiffert M, Sinning J-M, Meyer A, et al. Development of a risk score for outcome after transcatheter aortic valve implantation. Clin Res Cardiol 2014;103(8):631-640. https://doi.org/10.1007/s00392-014-0692-4 [ Links ]
 Correspondence:
Correspondence:
J J Liebenberg
liebjurg@gmail.com
Accepted 18 October 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}