










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 n.6 Pretoria Jun. 2020
http://dx.doi.org/10.7196/SAMJ.2020.v110i6.14751
REVIEW
Transmission of respiratory viruses when using public ground transport: A rapid review to inform public health recommendations during the COVID-19 pandemic
J ZhenI,*; C ChanI,*; A SchooneesII,*; E ApatuIII; L ThabaneIV; T YoungV
IHBSc; Department of Health Research Methods, Evidence, and Impact, Faculty of Health Sciences, McMaster University, Hamilton, Ontario, Canada
IIMSc; Centre for Evidence-based Health Care, Department of Global Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
IIIDrPH, MPH; Department of Health Research Methods, Evidence, and Impact, Faculty of Health Sciences, McMaster University, Hamilton, Ontario, Canada
IVPhD; Department of Health Research Methods, Evidence, and Impact, Faculty of Health Sciences, McMaster University, Hamilton, Ontario, Canada
VMB ChB, FCPHM, MMed (Public Health), PhD; Centre for Evidence-based Health Care, Department of Global Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa
ABSTRACT
In response to the COVID-19 pandemic, numerous countries worldwide declared national states of emergency and implemented interventions to minimise the risk of transmission among the public. Evidence was needed to inform strategies for limiting COVID-19 transmission on public transport. On 20 March 2020, we searched MEDLINE, CENTRAL, Web of Science and the World Health Organization's database of 'Global research on coronavirus disease (COVID-19)' to conduct a rapid review on interventions that reduce viral transmission on public ground transport. After screening 74 records, we identified 4 eligible studies. These studies suggest an increased risk of viral transmission with public transportation use that may be reduced with improved ventilation. International and national guidelines suggest the following strategies: keep the public informed, stay at home when sick, and minimise public transport use. Where use is unavoidable, environmental control, respiratory etiquette and hand hygiene are recommended, while a risk-based approach needs to guide the use of non-medical masks.
Coronavirus (CoV) represents a large family of viruses that affect the respiratory system. Some examples of these viruses are Middle East respiratory syndrome (MERS-CoV) and severe acute respiratory syndrome (SARS-CoV). In December 2019, seemingly unexplain-able respiratory infections suddenly arose in Wuhan, China. On 11 February 2020, the World Health Organization (WHO) classified the disease caused by the novel CoV as COVID-19.[1]
Realising the serious public health risks posed by the novel CoV, the WHO declared COVID-19 a pandemic on 11 March 2020. Shortly afterwards, on 15 March 2020, the President of South Africa (SA), Cyril Ramaphosa, declared a national State of Disaster in response to the COVID-19 pandemic. Consequently, the SA government implemented several interventions to minimise the risk of COVID-19 transmission among the public, including school closures, foreign travel bans, and bans on social gatherings of over 100 people.[2] As COVID-19 continued its spread throughout SA, President Ramaphosa announced a 21-day nation-wide lockdown starting at 00h00 on 27 March 2020. At this point, the public was permitted only to leave their homes to seek medical care, buy food or collect a social grant. The lockdown also included the closure of all stores and businesses except for essential services (such as pharmacies, laboratories, banks, the Johannesburg Stock Exchange, supermarkets, petrol stations and healthcare providers), as well as the halt of non-essential transport services.[3,4]
The goal of these interventions was to limit viral transmission by limiting the risk of exposure to infected persons.[5,6] Limiting such risk may be difficult for members of the public who rely on the use of public ground transport during the pandemic. During the lockdown in SA, buses and minibus taxis continued to transport essential service workers and members of the public doing the aforementioned permitted activities.[4] The continued use of public ground transport poses a risk of viral transmission because countless numbers of people are put in close proximity to one another. The belief that public transport may pose a risk for increasing viral transmission is based on high occupant density, overcrowding in an enclosed space, inadequate ventilation, recirculation of contaminated air, and increased duration of exposure to infected individuals. [7,8]
As COVID-19 can be transmitted through droplets produced by coughing or sneezing, the general public and healthcare providers have taken to using facemasks, particularly N95 respirators, in the hope of reducing the risk of infection. The supply of N95 respirators has therefore run low, necessitating the limited and optimised use of these masks.[9] These low supplies have caused panic among the general public and healthcare providers alike. However, a study by Loeb et al.[10] has shown that N95 respirators may not confer additional protection against influenza infection compared with the use of a surgical mask, suggesting that the panic surrounding the shortage of N95 respirators may not be warranted. Loeb et al.[10] stressed the importance of assessing the true value of endorsing and implementing interventions. Consequently, the present review had two objectives: (i) to better understand the role of public ground transport in COVID-19 transmission; and (ii) to assess interventions that may reduce the transmission of COVID-19 infections in public ground transport. Empirical evidence should be the basis on which recommendations are made with regard to how best to deal with the pandemic. We therefore performed a rapid review of the current literature in order to assess the abilities of different interventions to decrease the incidence of droplet-based infections among people using public ground transport.
Methods
Rapid reviews aim to provide a summary of the evidence in a short space of time.[11] The participants of interest were humans using public transportation (taxis, buses, trains and subways) and exposed to viruses such as influenza, SARS-CoV or MERS-CoV. The study designs that aligned best with our goals involved the inclusion of systematic reviews, clinical trials (including but not limited to randomised controlled trials), comparative observational studies and modelling studies. We included only studies published between 2000 and 2020 in English to maintain relevance to modern society. We excluded studies where the participants/context of the intervention were healthcare workers in healthcare facilities, owing to the high possibility of confounding variables presented by their work. This review was concerned with investigating interventions such as the use of personal protective equipment, hand hygiene, social distancing and surface sanitisation and their relationship to the incidence of infections.
Identifying studies for inclusion
On 20 March 2020, we searched MEDLINE (PubMed), CENTRAL (Cochrane Library) and Web of Science (Clarivate Analytics) to identify studies or systematic reviews that were relevant to our research question. Studies were not excluded based on geographical location or type of public ground transport. The search strategy can be found in Fig. 1 (accessible at http://www.samj.org.za/public/sup/14751.docx). In addition, we screened reference lists of relevant reviews in order to identify any additional relevant studies, and searched the WHO's database 'Global research on coronavirus disease (COVID-19)'.[12]
Making use of reference management software (Endnote), one researcher screened through all 74 records (titles and abstracts) identified by the search and excluded all obviously ineligible records. Seven records remained potentially eligible, and two other researchers then screened through these and identified four relevant studies/reviews that met this rapid review's eligibility criteria. The three records not meeting the eligibility criteria were not specific to interventions. For each of the included records, we thoroughly analysed the full text manuscripts.
Data extraction
Each included study/review was extracted by one researcher. The following data were extracted: publication details (year, author(s)), location, method of transport, virus, details of the interventions and comparisons, diagnostic tests, number of infected persons, number of tested contacts, transmission rate, and number of cases with active disease. We examined other factors that may affect the transmission of viral diseases such as travel time and environmental factors (ventilation and air conditioning systems, seating position, distance to contact person).
Results
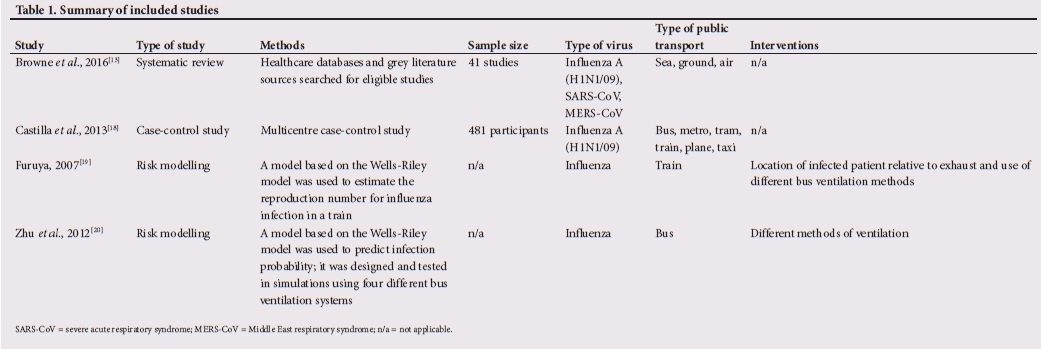
We identified one systematic review, two modelling studies and one case-control study (Table 1).
Systematic review
The systematic review by Browne et al. (2016)[13] estimated the risk of transmission related to the use of transport systems. The search was done in June 2014, and the authors found 41 studies. For our review, we did not consider studies that were already included in the systematic review separately. The majority of studies investigated transmission related to air transport (n=30), while 6 studies were on sea transport and 6 were on ground transport. The studies were undertaken across Europe (UK, Germany and Spain), Asia (China, Korea, Japan and Singapore), North America (USA and Canada) and Australasia (New Zealand and Australia). Twenty-nine studies were on influenza, 5 were on SARS-CoV and 2 were on MERS-CoV. Three did not specify the virus transmitted, and 2 were on both influenza and SARS-CoV. In this systematic review, 4 quantitative studies discussed the risk for viral transmission on ground transport. A study by Piso et al. (2011)[14] did contact tracing of one H1N1 influenza-infected individual who undertook a long-distance bus journey, and identified a laboratory-confirmed secondary case 3 days later. Pestre et al. (2012)[15] investigated the spread of H1N1 influenza among a group of 24 individuals travelling together, and showed that 84% of a group travelling together contracted the virus. Their study also suggested that rail transport was important in accelerating the spread of influenza to new areas in the 1918 influenza A (H1N1) pandemic.[15] Cui et al. (2011)[16] described a study involving 2 555 passengers on a train with 2 H1N1-positive individuals. This study demonstrated that risk of transmission was associated with seating proximity to the index case and duration spent aboard, and that there was transmission to persons in previously unaffected destinations from arriving rail passengers.[16] A case-control study by Troko et al. (2011)[17] followed 72 cases of individuals with acute respiratory infections and compared them with 66 controls. After adjusting for confounders, persons reporting to the general practitioner with acute respiratory infection were almost six times as likely to have used public transport during the previous 5 days than controls (odds ratio (OR) 5.94; p<0.05).
Case-control study
Researchers in Spain (Castilla et al., 2013[18]) did a multi-centre case-control study in which they evaluated the effect of various factors or situations that could lead to an increased risk of infection, including the use of public transport. From 36 medical facilities, 481 adult outpatients with laboratory-confirmed influenza A (H1N1/09) in the 2009 - 2010 season were the cases. Community-based controls were used, matched to cases by age, area and consultation date. Medical records were thoroughly reviewed, interviews were conducted with participants, and information on risk situations was collected. Specifically, information on the use of metropolitan public transport (bus, metro, tram or local train), long-distance transport (train or plane), and having taken a taxi during the 7 days before the onset of symptoms in cases or the medical consultation in controls was collected. In spite of matching, cases were slightly younger than controls and more often had secondary or higher education, were pregnant women, or had more than one major risk condition. The use of various modes of public transport (specifically metro, bus, tram or local train) showed a lower probability of being diagnosed with influenza (OR 0.45; 95% confidence interval (CI) 0.30 - 0.68).
Meanwhile, travelling by train (typically longer distances), aeroplane (OR 0.80; 95% CI 0.50 - 1.28), or taxi (OR 1.19; 95% CI 0.70 - 2.04) did not show an association with influenza diagnosis. This study has a moderate risk of bias, which means that there are some concerns about the robustness of the methods. Furthermore, it is important to note that the public transport context in which this study took place may differ from those elsewhere. Differences between countries may include types of ventilation systems, rider density, seating arrangements, and time spent in the vehicle. Decision-makers worldwide need to consider the applicability of public transport studies carefully.
Modelling studies
Furuya (2007)[19] published a modelling study that used a model based on the Wells-Riley equation to quantify the risk associated with the inhalation of indoor airborne infection on trains. The output of this risk equation was the probability of infection for susceptible people in an enclosed environment. This probability could then be used to calculate the estimated reproduction number (Ra), where a higher Ra indicates a greater risk of disease transmission. In using this risk equation to estimate the influence of interventions on risk reduction, it was shown that use of a facemask and improved ventilation of a railway carriage could reduce risk of disease transmission. They found that a crowded train may increase the eventual number of infections by 2 - 3 times and cause an earlier peak of the epidemic curve by 30 days. The model demonstrated that if healthy passengers wore a surgical mask, the median of distribution for Ra decreased from 2.22 to 2.08, while use of high-efficiency particulate air (HEPA) masks showed a decrease to 1.13. However, doubling the rate of ventilation reduced the median of distribution for Ra to 1.17, which is a cost-effective intervention. The author suggests that, while they may be effective at reducing infection risk, HEPA masks may not be available to all passengers, and improved ventilation of railway carriages may be a more effective and feasible intervention.
Zhu et al. (2012)[20] used a computational fluid dynamics-based numerical model integrated within a Wells-Riley equation. They used this to numerically assess the risk of airborne transmission of influenza in buses. They modelled three very common ventilation methods used in buses, where the location of the air supply and air exhaust openings were varied. They also modelled an air-recirculation mode that included a high-efficiency filter and compared it with complete (100%) ventilation, termed non-air-recirculation modes. They found that in the common ventilation methods, the location of the infected person in combination with the location of the air supply/exhaust openings was important, i.e. the passengers located between the infected passenger and the air exhaust had a higher risk of infection. The probability of infection varied from 0.05% to 10.1% for seated passengers and up to 27.2% for standing passengers, depending on location and ventilation mode. For displacement ventilation (air supply near the ground and air exhaust at the top of the bus), the probability of infection remained at 0.05% despite changes in location. Furthermore, when the ventilation system was operated with the parameters 25% air recirculation and 75% efficiency filtration system, the probability of infection increased by only 0.05% compared with complete ventilation, regardless of ventilation method/passenger locations. However, since recirculation is beneficial for thermal comfort, a filtration system or displacement ventilation may be beneficial.
Discussion
The SA government has implemented several measures to keep members of the public away from each other in order to minimise the risk of COVID-19 transmission.[2,3] However, there are instances where being in close proximity may be unavoidable, such as when people use buses and minibus taxis which are available for necessary commutes, even during the nation-wide lockdown.[3,4] Since COVID-19 spreads from person to person through the respiratory droplets produced when an infected person coughs or sneezes, and from touching contaminated surfaces, the use of public transport may contribute to the transmission of COVID-19 by bringing people together in high densities. The goal of this rapid review was to investigate the evidence surrounding interventions that may decrease the risk of viral transmission while using public ground transport.
Few empirical research studies have explored the effectiveness of risk reduction strategies in this context. Only two modelling studies were found. One study demonstrated that crowded trains can increase the number of infections by 2 - 3 times and cause an earlier peak of the epidemic curve by 30 days. This same study showed that the use of facemasks and ventilation on trains can reduce the risk of airborne infection.[19] The other modelling study demonstrated that filtration of recirculated air may decrease the risk of viral transmission if non-recirculated air cannot be provided, and that, in the case of common ventilation methods on public transport, the probability of passengers contracting a viral respiratory infection from an infected passenger is decreased when the infected person is situated closer to the exhaust opening.[20] The systematic review included in our review found that use of public transport increased the risk of influenza transmission.[13] In particular, a study included in the systematic review showed that the risk of transmission aboard a train was associated with seating proximity to the index case and duration of time spent aboard.[16] Also included in the systematic review, a case-control study showed that the use of public transportation during the 5 days prior to symptom onset was associated with a significantly higher frequency of influenza A (H1N1/09), while another study suggested that rail transport was important in accelerating the spread of influenza to new areas in the 1918 influenza A (H1N1) pandemic.[13,15,17]
In contrast to the above findings, we identified a case-control study conducted in Spain which demonstrated that the use of public transport 7 days prior to the onset of respiratory symptoms was associated with a normal or lower probability of a diagnosis of influenza.[18] The authors suggest that this finding may be due to the development of protective antibodies in public transport users as a result of previous exposures to influenza virus during their commute. However, these results should be viewed with caution owing to the limitations of the study linked to case and control selection, recall bias and confounding factors. Potential confounding factors may include the possibility that people with influenza are less likely to travel using public transport, and the implicit bias that case-control studies bring when implying reverse causation. Furthermore, the cases in the study were individuals who presented to their doctor with influenza. People who rely solely on public transport may have more difficulty accessing and consulting with their physician. Also, while the study adjusted for age during comparisons, it did not adjust for confounding factors such as diet and exercise. Overall, these factors contribute to decreasing the quality of the evidence.
It is important to note that the studies included in this review are based mainly on influenza and/or non-COVID-19 CoVs. These viruses have different characteristics from those of COVID-19 and may need to be handled differently. The WHO has described key differences between influenza viruses and COVID-19. Important factors to note are that influenza has a shorter incubation period, shorter serial interval, lower reproductive number and lower mortality rate than COVID-19.[21] Together, these factors suggest that COVID-19 is more contagious and potentially more dangerous than influenza. A limitation of this review is therefore that we cannot be confident that studies involving influenza can accurately inform guidelines about COVID-19 owing to the novelty of this new CoV.
Given the limited scientific evidence on the topic, we examined international and national guidance documents that recommend public education and the adoption of various strategies (Table 2).
In Canada, the Public Health Agency of Canada in collaboration with Canadian public health experts developed guidance for federal, provincial or territorial public health authorities on the use of public health measures to reduce and delay transmission of COVID-19 in the community.[22] The European Centre for Disease Prevention and Control guidelines for the use of non-pharmaceutical measures to delay and mitigate the impact of 2019-nCoV was based on knowledge of 2019-nCoV and evidence available on other viral respiratory pathogens - SARS-CoV, MERS-CoV and seasonal or pandemic influenza viruses.[23] Public Health England provides guidance for staff in the transport sector in order to reduce risk of COVID-19 transmission.[24] Additionally, the National Academies of Sciences, Engineering, and Medicine has produced a guide to aid in public transportation pandemic planning and response with a chapter dedicated to the prevention of the spread of disease associated with use of public transport.[25] The WHO 'Infection prevention and control of epidemic- and pandemic-prone acute respiratory infections in health care' guidelines provide recommendations, best practices and principles for non-pharmacological aspects of infection prevention and control for acute respiratory infections in healthcare, with special emphasis on those that can present as epidemics or pandemics.[26] As the wide use of masks by healthy people in the community setting is not supported by current evidence and carries uncertainties, the WHO advises that decision-makers apply a risk-based approach taking into account a number of factors: the purpose of mask use; risk of exposure to COVID-19 in the local setting; vulnerability of the person to develop severe disease; the setting in which the population lives in terms of population density, ability to carry out physical distancing, and risk of rapid spread; and feasibility and type of mask (with medical masks reserved for healthcare workers).[27] In SA, the National Institute for Communicable Diseases produced an environmental health guideline to supplement the guideline on case finding, diagnosis, management and public health response to COVID-19.[28] The recommendations from these guidelines are set out in Table 3. The box on the same page provides a summary of the key findings from the current review.
Conclusions
Findings from this review suggest that the use of public transport increases the risk of viral transmission owing to the correlation between recent use of public transport and presentation of influenza symptoms, and that risk of transmission increases with an increase in trip duration and proximity to an infected individual. The review also identified two modelling studies suggesting that adequate ventilation could reduce the probability of passengers contracting a viral respiratory infection from an infected passenger.
Ultimately, there is limited empirical evidence surrounding risk reduction interventions to be used on public ground transport in order to slow the transmission of COVID-19. However, national and international guidelines have suggested that limiting the use of public transport, environmental control, respiratory etiquette, hand hygiene, and active communication and information sharing by public health are conducive to limiting transmission. Overall, further investigations surrounding the efficacy and plausibility of various interventions involving public transportation may provide key information in limiting the spread of COVID-19.
Declaration. None.
Acknowledgements. We thank Drs Mark Loeb and Gordon Guyatt for their technical advice, which greatly improved our approach to the review.
Author contributions. TY and LT conceived the idea. JZ and CC designed and drafted the project proposal. AS designed the search strategy, screened studies, and did data extraction. EA provided public health expertise and suggestions. CC and JZ screened studies, did data extraction and wrote the manuscript. All authors provided edits and feedback throughout and approved the final manuscript.
Funding. AS and TY are supported in part by the Research, Evidence and Development Initiative (READ-It). READ-It (project number 300342-104) is funded by UK aid from the UK government; however, the views expressed do not necessarily reflect the UK government's official policies.
Conflicts of interest. None.
References
1. Cascella M, Rajnik M, Cuomo A, Dulebohn SC, di Napoli R. Features, evaluation and treatment coronavirus (COVID-19). StatPearls Publishing, 6 April 2020. http://www.ncbi.nlm.nih.gov/pubmed/32150360 (accessed 25 March 2020). [ Links ]
2. Daily Maverick. Covid-19: Ramaphosa declares national state of disaster, imposes travel bans. 15 March 2020. https://www.dailymaverick.co.za/article/2020-03-15-covid-19-ramaphosa-declares-national-state-of-disaster-imposes-travel-bans/ (accessed 26 March 2020). [ Links ]
3. Al Jazeera News | South Africa. South Africans brace for 21-day lockdown as virus cases rise. https://www.aljazeera.com/news/2020/03/south-africans-brace-21-day-lockdown-virus-cases-rise-200324073801136.html (accessed 26 March 2020). [ Links ]
4. South African Government. Minister Fikile Mbalula on unpacking implications for transport during the coronavirus COVID-19 lockdown. 25 March 2020. https://www.gov.za/speeches/minister-fikile-mbalula-unpacking-implications-transport-during-coronavirus-covid-19 (accessed 26 March 2020). [ Links ]
5. World Health Organization. WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March 2020. https://www.who.int/dg/speeches/detafl/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed 25 March 2020). [ Links ]
6. Centers for Disease Control and Prevention (CDC). How coronavirus spreads. 13 April 2020. https://www.cdc.gov/coronavirus/2019-ncov/prepare/transmission.html (accessed 25 March 2020). [ Links ]
7. Tatem AJ, Rogers DJ, Hay SI. Global Transport Networks and Infectious Disease Spread. Vol. 62, Advances in Parasitology. San Diego: Elsevier Academic Press, 2006:293-343. https://doi.org/10.1016/S0065-308X(05)62009-X [ Links ]
8. Nasir ZA, Campos LC, Christie N, Colbeck I. Airborne biological hazards and urban transport infrastructure: Current challenges and future directions. Environ Sci Pollut Res 2016;23(15):15757-15766. https://doi.org/10.1007/s11356-016-7064-8 [ Links ]
9. Centers for Disease Control and Prevention (CDC). Strategies for optimizing the supply of N95 respirators. 2 April 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/respirators-strategy/crisis-alternate-strategies.html (accessed 25 March 2020). [ Links ]
10. Loeb M, Dafoe N, Mahony J, et al. Surgical mask vs N95 respirator for preventing influenza among health care workers. JAMA 2009;302(17):1865-1871. https://doi.org/10.1001/jama.2009.1466 [ Links ]
11. Khangura S, Konnyu K, Cushman R, Grimshaw J, Moher D. Evidence summaries: The evolution of a rapid review approach. BMC Syst Rev 2012;1:10. https://doi.org/10.1186/2046-4053-1-10 [ Links ]
12. World Health Organization. Global research on coronavirus disease (COVID-19). 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/global-research-on-novel-coronavirus-2019-ncov (accessed 25 March 2020). [ Links ]
13. Browne A, St-Onge Ahmad S, Beck CR, Nguyen-Van-Tam JS. The roles of transportation and transportation hubs in the propagation of influenza and coronaviruses: A systematic review. J Travel Med 2016;18(23):1-7. https://doi.org/10.1093/jtm/tav002 [ Links ]
14. Piso RJ, Albrecht Y, Handschin P, Bassetti S. Low transmission rate of 2009 H1N1 influenza during a long-distance bus trip. Infection 2011;39(2):149-153. https://doi.org/10.1007/s15010-011-0084-x [ Links ]
15. Pestre V, Morel B, Encrenaz N, et al. Transmission by super-spreading event of pandemic A/H1N1 2009 influenza during road and train travel. Scand J Infect Dis 2012;44(3):225-227. https://doi.org/10.3109/00365548.2011.631936 [ Links ]
16. Cui F, Luo H, Zhou L, et al. Transmission of pandemic influenza A (H1N1) virus in a train in China. J Epidemiol 2011;21(4):271-277. https://doi.org/10.2188/jea.JE20100119 [ Links ]
17. Troko J, Myles P, Gibson J, et al. Is public transport a risk factor for acute respiratory infection? BMC Infect Dis 2011;11:16. https://doi.org/10.1186/1471-2334-11-16 [ Links ]
18. Castilla J, Godoy P, Domínguez Á, et al. Risk factors and effectiveness of preventive measures against influenza in the community. Influenza Other Respir Viruses 2013;7(2):177-183. https://doi.org/10.1111/j.1750-2659.2012.00361.x [ Links ]
19. Furuya H. Risk of transmission of airborne infection during train commute based on mathematical model. Environ Health Prev Med 2007;12(2):78-83. https://doi.org/10.1007/BF02898153 [ Links ]
20. Zhu S, Srebric J, Spengler JD, Demokritou P. An advanced numerical model for the assessment of airborne transmission of influenza in bus microenvironments. Build Environ 2012;47(1):67-75. [ Links ]
21. World Health Organization. Q&A: Similarities and differences - COVID-19 and influenza. 17 March 2020. https://www.who.int/news-room/q-a-detail/q-a-similarities-and-differences-covid-19-and-influenza (accessed 21 April 2020). [ Links ]
22. Government of Canada. Community-based measures to mitigate the spread of coronavirus disease (COVID-19) in Canada. Modified 3 April 2020. https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/health-professionals/public-health-measures-mitigate-covid-19.html (accessed 25 March 2020). [ Links ]
23. European Centre for Disease Prevention and Control (ECDC). Guidelines for the use of non-pharmaceutical measures to delay and mitigate the impact of 2019-nCoV. 10 February 2020. https://www.ecdc.europa.eu/en/publications-data/guidelines-use-non-pharmaceutical-measures-delay-and-mitigate-impact-2019-ncov (accessed 26 March 2020). [ Links ]
24. GOV.UK. COVID-19: Guidance for staff in the transport sector. 14 February 2020. https://www.gov.uk/government/publications/covid-19-guidance-for-staff-in-the-transport-sector/covid-19-guidance-for-staff-in-the-transport-sector (accessed 26 March 2020). [ Links ]
25. National Academies of Sciences, Engineering, and Medicine. A guide for public transportation pandemic planning and response. National Academies Press, 2014. https://www.nap.edu/read/22414/chapter/1 (accessed 26 April 2020). [ Links ]
26. World Health Organization. Infection prevention and control of epidemic- and pandemic-prone acute respiratory infections in health care: WHO Guidelines. April 2014. https://www.who.int/csr/bioriskreduction/infection_control/publication/en/ (accessed 25 March 2020). [ Links ]
27. World Health Organization. Advice on the use of masks in the community, during home care and in healthcare settings in the context of the novel coronavirus (COVID-19) outbreak. 6 April 2020. https://www.who.int/publications-detail/advice-on-the-use-of-masks-in-the-community-during-home-care-and-in-healthcare-settings-in-the-context-of-the-novel-coronavirus-(2019-ncov)-outbreak (accessed 26 April 2020). [ Links ]
28. National Department of Health, South Africa. COVID-19 environmental health guidelines. 16 March 2020. https://j9z5g3w2.stackpathcdn.com/wp-content/uploads/2020/04/COVID-19-ENVIRONMENTAL-HEALTH-GUIDELINE-1-3.pdf (accessed 25 March 2020). [ Links ]
 Correspondence:
Correspondence:
T Young
tyoung@sun.ac.za
Accepted 28 April 2020
* These authors contributed equally.


{kind=link}
{kind=link}
{kind=link}
{kind=link}