










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 n.5 Pretoria May. 2020
http://dx.doi.org/10.7196/SAMJ.2020.v110i5.14252
RESEARCH
It's contrary - comorbidity does not affect survival of South Africans with colorectal cancer: An analysis from the Colorectal Cancer in South Africa cohort
C BouterI; B BebingtonII, III; S MaphosaIV; H MaherIV; P GaylardV; H R EtheredgeVI, VII; J FabianVIII, IX; L ProdehlX; D SurridgeXI, XII; R L FourieXIII; N HarranXIV; D LutrinXV, XVI; D BizosXVII, XVIII, XIX; P RuffXX, XXI
IBHSc, PDM; Wits Donald Gordon Medical Centre, University of the Witwatersrand, Johannesburg, South Africa
IIMB ChB, FCS (SA); Wits Donald Gordon Medical Centre, University of the Witwatersrand, Johannesburg, South Africa
IIIMB ChB, FCS (SA); Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVRegistered Nurse; Wits Donald Gordon Medical Centre, University of the Witwatersrand, Johannesburg, South Africa
VPhD; Data Management and Statistical Analysis, Johannesburg, South Africa
VIPhD; Wits Donald Gordon Medical Centre, University of the Witwatersrand, Johannesburg, South Africa
VIIPhD; Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIIIMB ChB, FCP (SA), Cert Nephrology (SA); Wits Donald Gordon Medical Centre, University of the Witwatersrand, Johannesburg, South Africa
IXMB ChB, FCP (SA), Cert Nephrology (SA); Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
XMB ChB, MMed (Surg), FCS (SA), Cert Gastroenterology (SA) Surg; Surgical Gastroenterology Unit, Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
XIMB ChB, FCS (SA), MMed (Surg), Cert Gastroenterology (SA) Surg; Wits Donald Gordon Medical Centre, University of the Witwatersrand, Johannesburg, South Africa
XIIMB ChB, FCS (SA), MMed (Surg), Cert Gastroenterology (SA) Surg; Colorectal Surgery Unit, Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa
XIIIMB ChB, FCS (SA), MBA, Cert Gastroenterology (SA) Surg; Surgical Gastroenterology Unit, Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
XIVMB BCh, MMed (Surg), FCS (SA), Cert Gastroenterology (SA) Surg; Wits Donald Gordon Medical Centre, University of the Witwatersrand, Johannesburg, South Africa
XVMB BCh, DA (SA), FCS (SA), Cert Gastroenterology (SA) Surg, MMed (Surg); Wits Donald Gordon Medical Centre, University of the Witwatersrand, Johannesburg, South Africa
XVIMB BCh, DA (SA), FCS (SA), Cert Gastroenterology (SA) Surg, MMed (Surg); Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
XVIIMB BCh, MMed (Surg), FCS (SA), Cert Gastroenterology (SA) Surg; Wits Donald Gordon Medical Centre, University of the Witwatersrand, Johannesburg, South Africa
XVIIIMB BCh, MMed (Surg), FCS (SA), Cert Gastroenterology (SA) Surg; Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
XIXMB BCh, MMed (Surg), FCS (SA), Cert Gastroenterology (SA) Surg; Surgical Gastroenterology Unit, Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
XXMB BCh, MMed (Int Med), FCP (SA); Wits Donald Gordon Medical Centre, University of the Witwatersrand, Johannesburg, South Africa
XXIMB BCh, MMed (Int Med), FCP (SA); Division of Medical Oncology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. The Colorectal Cancer South Africa (CRCSA) study is an observational cohort of patients with colorectal cancer (CRC) in Johannesburg, South Africa (SA). We found that the mean age at the time of CRC diagnosis was 56.6 years, consistent with studies from SA and sub-Saharan Africa. In high-income settings, comorbidity adversely affects CRC survival, and patients are substantially older at the time of CRC diagnosis. Given the younger age at CRC diagnosis in the CRCSA cohort, we hypothesised that comorbidity may be less prevalent and have little impact on CRC survival.
OBJECTIVES. To determine the prevalence of comorbidity and whether comorbidity adversely affects overall survival (OS) of CRC patients.
METHODS. Patients enrolled in the CRCSA study between January 2016 and July 2018 were included. The cohort comprised a convenience sample of adults with histologically confirmed CRC, treated at the University of the Witwatersrand Academic Teaching Hospital Complex. Demographic, clinical and histological variables were collected at baseline and participants were followed up for OS. The Charlson comorbidity index (CCI) scoring system was used to classify participants as 'no comorbidity' (CCI score 0) and '1 or more comorbidities' (CCI score >1). A descriptive analysis of the cohort was undertaken, while survival across comorbidity groups was compared by the Kaplan-Meier method and Cox proportional hazards (PH) regression models. Multivariable Cox PH regression was performed to examine the effect of comorbidity on survival (unadjusted) and then adjusted for variables.
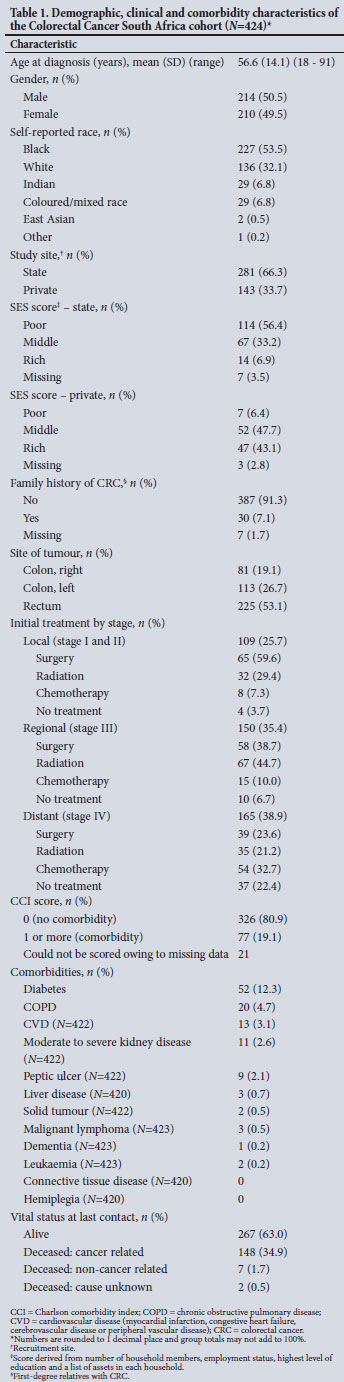
RESULTS. There were 424 participants, and the mean (standard deviation) age was 56.6 (14.1) years (range 18 - 91). Only 19.1% of participants had >1 comorbidities, of which diabetes mellitus was most frequent (12.3%), followed by chronic obstructive pulmonary disease (4.7%) and cardiovascular disease (3.1%). There was no significant difference in unadjusted and adjusted risk of death for the group with >1 comorbidities compared with those with no comorbidity. However, an incidental finding showed a significantly increased risk of death for those receiving potentially curative treatment later than 40 days after CRC diagnosis.
CONCLUSIONS. In the CRCSA cohort from Johannesburg, comorbidity is uncommon, with no significant adverse effect on OS. If potentially curative treatment is initiated within 40 days of CRC diagnosis, OS could be improved. To fully understand the epidemiology of CRC in SA, population-based registries are essential, and future research should aim to identify health system failures that lead to delays in intervention beyond 40 days in patients with CRC.
According to GLOBOCAN, colorectal cancer (CRC) is the third most common cancer and the fourth most common cause of cancer-related death, with 1.85 million new cases diagnosed worldwide in 2018.[1,2] The incidence of CRC appears to be increasing in emerging low- and middle-income countries (LMICs) owing to socioepidemiological transitions, including dietary changes, with countries in sub-Saharan Africa (SSA) reporting a notable increase in colorectal, breast and prostate cancer.[3,4] South Africa (SA) is no exception - the incidence of CRC is increasing steadily, and it was the sixth leading cause of cancer-related death in 2018.[1] It is noteworthy that apart from increasing incidence, the average age of CRC patients at the time of diagnosis in SSA is ~10 years younger than that observed in high-income countries (HICs).[5,6] In addition, other non-communicable diseases (NCDs), including diabetes and respiratory and cardiovascular disease, are on the rise, with the prevalence in SA being reported as two to three times higher than in HICs.[7]
While there are no published data on comorbidity with CRC from SSA, many CRC cohorts from HICs describe a considerable comorbidity burden that adversely affects short- (30-day) and long-term (1- and 5-year) survival.[8-14] Comorbidity, defined as concurrent conditions present at the time of diagnosis of the index malignancy, not only contributes to physiological burden and poor survival, but also affects treatment choices.[13] With the rising incidence of CRC and the high burden of NCDs reported in SA, we can expect to see a similar trend.
Objectives
To determine whether comorbidity adversely affects overall survival (OS) in CRC in SA, as is seen in HICs.
The Colorectal Cancer in South Africa study
To address the paucity of information on CRC in SA, the Colorectal Cancer in South Africa (CRCSA) study was established in 2016.[15] It is the first prospective, longitudinal cohort study to describe the clinical presentation, management and outcomes of CRC in SA patients. The study is based in Johannesburg, Gauteng, the largest and wealthiest city in SA, with a population of ~5.7 million people.[16] The recruitment/study sites are part of the Academic Teaching Hospital Complex, Faculty of Health Sciences, University of the Witwatersrand, which comprises five state sector hospitals: Charlotte Maxeke Johannesburg Academic Hospital, Chris Hani Baragwanath Academic Hospital, Edenvale Hospital and the Klerksdorp/Tshepong Complex, and one private sector hospital, Wits Donald Gordon Medical Centre. The state sector hospitals service people without medical insurance (84% of the population), while those who have insurance (16% of the population) access the private sector.[17] Participants were referred for study enrolment if they were aged >18 years, had histologically confirmed primary adenocarcinoma of the colon or rectum, diagnosed within the past 12 months, and were willing and able to give written informed consent. Specifically, this article presents our analysis of the impact of comorbidity as well as other patient factors on CRC outcomes, including OS. Comorbidity is particularly important because our preliminary analyses indicate a mean age at the time of diagnosis of 56.6 years, which is substantially younger than cohorts described in HICs, suggesting that patients in our cohort may have a different comorbidity profile.[8-10,12,14,18]
Methods
The CRCSA cohort is a combined cross-sectional and longitudinal cohort of adults with CRC treated in Johannesburg, as described above.[15] Ethics approval for the study was obtained from the Human Research Ethics Committee (Medical) of the University of the Witwatersrand (ref. no. M150446). The cross-sectional component, which generates the baseline data, consists of an initial visit where consenting participants complete a comprehensive questionnaire administered by trained research assistants.
Study sample
Patients enrolled between January 2016 and July 2018, with at least 6 months' follow-up data, were included in this analysis; those with recurrence of CRC at initial presentation to a recruitment site were excluded. For the analysis, the following variables from the CRCSA study were included: (i) age at first visit (to a recruitment site); (ii) gender; (iii) self-reported race; (iv) socioeconomic indicators: number of household members, employment status, highest level of education (HLOE) and a list of assets in each household;[19] ( v) family history of cancer, defined as first-degree relatives diagnosed with CRC; (vi) anatomical location of the primary lesion; ( vii) tumour staging at presentation, classified as local, regional or distant based on available information from the AJCC (American Joint Committee on Cancer classification system), TNM (done on histology or radiology) and Duke's staging; (viii) urgency of surgery (elective or urgent/emergency); (ix) site of recruitment (hospital); (x) time to initial treatment, defined as time from diagnosis of CRC to first potentially curative treatment (analysed in approximate quartiles); and (xi) first potentially curative treatment (radiotherapy, chemotherapy, surgical, excluding palliative treatment or treatment of complications relating to CRC). Trained research assistants followed up participants telephonically at 6, 12, 24 and 36 months after the first visit for details related to completion of therapy, remission, recurrence and vital status. Participant information was corroborated through multidisciplinary team (MDT) meetings and clinical records.
Sample size
Sample size estimation was based on the key research objective, which was to examine the effect of comorbidity on patient survival. As a starting point, we used recently published survival data for a CRCSA study group of 60% at 3 years. Based on a comorbidity group comprising 10% of the total sample, with accrual and final follow-up periods of 2.5 years and 0.5 years, respectively, the detection of a hazard ratio of at least 1.8 with 80% power at the 5% significance level required a minimum sample size of 417 patients.[20,21]
Data analysis
The Charlson comorbidity index (CCI) has been validated for assessing the prognostic impact of comorbidity on CRC and for use with data collected from both administrative records and self-reported surveys.[8-10,22,23] As per the CCI scoring system, each condition, such as cardiovascular disease, diabetes or renal disease, is assigned a weighted score and then added to arrive at a total CCI score per patient. Higher CCI scores tend to be associated with a worse prognosis.[8-10,12,13] In the present study, an adapted version of the CCI was used to assess comorbidity in a once-off self-reported questionnaire and from patient clinical records. AIDS and metastatic tumours at diagnosis were excluded, solid tumours were defined as all solid tumours other than CRC, all liver disease was scored as mild (score of 1), and age was used as a covariate rather than part of the CCI. After arriving at individual CCI scores, participants were grouped into 'no comorbidity' (CCI score 0) and '1 or more comorbidities' (CCI score >1) for survival analysis.
Survival across comorbidity groups was compared by the Kaplan-Meier method and Cox proportional hazards (PH) regression models. Multivariable Cox PH regression was performed to examine the effect of comorbidity on survival (unadjusted) and then adjusted for age at diagnosis, gender, ethnicity, study site (state/private), cancer site, urgency of presentation, stage, initial treatment, and time to initial treatment. Before undertaking survival analysis, statistical examination of the association between the covariates revealed that initial treatment received was strongly confounded with both surgical urgency and time to initial treatment, as expected. Consequently, these variables could not be used together as covariates, and surgical urgency was omitted as a covariate as only 9% of patients had urgent/emergency surgeries. Initial treatment (model 1) and time to initial treatment (model 2) were used separately as covariates in two adjusted models. Data analysis was carried out using SAS version 9.4 for Windows (SAS Institute, USA). A 5% significance level was used.
Outcome was defined as all-cause mortality including both cancer-related and non-cancer-related deaths. OS was determined from the date of diagnosis to the date of death or date last seen. An overall socioeconomic score (SES) was derived from employment status, HLOE, number of people in the household, and 11 household assets (for data collected from November 2016 onwards) using principal components analysis.[24] The first component was used as the SES score, in terms of which the lowest 40% of households were categorised as 'poor', the highest 20% as 'rich', and the rest as the 'middle' group.[25]
Results
A total of 444 potential participants were enrolled, of whom 424 fulfilled eligibility criteria for the analysis period. Overall, at the time of presentation 38.9% of participants had distant disease and only 19.1% had any comorbidity. Diabetes was the most frequent comorbidity (12.3%), followed by chronic obstructive pulmonary disease (4.7%) and cardiovascular disease (3.1%). Demographic, clinical and comorbidity characteristics are presented in Table 1. The mean (standard deviation) age at diagnosis was 56.6 (14.1) years (range 18 - 91). There were almost equal proportions of men and women, and half (53.5%) were self-reported as black. Malignant lesions were most commonly identified in the rectum (53.1%), followed by the left (26.6%) and right (19.1%) colon.
Survival
In our cohort, with a median follow-up time of 1.1 years, the unadjusted median survival was 2.0 years (95% confidence interval 1.8 - 2.6). There was no significant difference in unadjusted and adjusted risk of death for the group with >1 comorbidities compared with those with no comorbidity (Table 2). Gender, ethnicity and location of malignancy had no impact on survival; however, study hospital site, tumour stage, initial treatment and time to initial treatment were found to have significant impact on outcome (OS). The effect of comorbidity and significant covariates on OS is illustrated by Kaplan-Meier survival plots in Fig. 1. An unexpected result was the significant increase in risk of death among patients who received treatment later than 40 days after diagnosis.

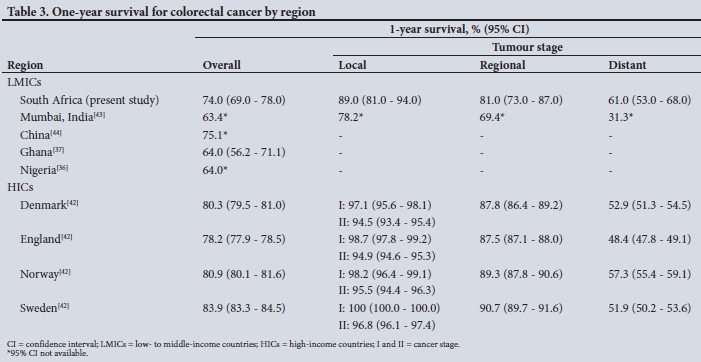
To contextualise the survival of our cohort and to benchmark outcomes, Table 3 sets out 1-year OS and OS by stage at presentation for this cohort and those in comparable studies conducted in LMICs and HICs. One-year OS in LMICs was inferior to rates observed in HICs. As expected, across all income settings, 1-year OS for patients with distant disease was poor. However, those who presented with local and regional disease in SA and India had inferior 1-year survival when compared with HICs.
Discussion
While most participants did not have any comorbidity by CCI classification, among those who did, there was no significant adverse effect on OS. The most common comorbid conditions observed were diabetes, chronic obstructive pulmonary disease and cardiovascular disease, in keeping with published data.[8,9,13,26,27] To the best of our knowledge, this is the first study of its kind from SA with our findings appearing to be similar to those from West and Central Africa. A CRC study in Kumasi, Ghana, reported a 24.9% prevalence of comorbidity, which did not significantly affect OS. In a cross-sectional study of Nigerian patients with various cancers, comorbidity occurred in 26.9% of participants, but unfortunately there were no OS data. When compared with HICs, a possible explanation for the lower prevalence of comorbid disease in our study and other studies from SSA may be the younger mean ages at presentation (53 - 56 years).[27-33] Aside from SSA, younger mean ages (45 - 67 years) have been observed in South Asia, China and Brazil.[34,35] Collectively, these findings from LMICs contrast with those from HICs, where median ages are ~10 -15 years older, and comorbidity is twice as high and adversely affects CRC outcomes.[8-10,12,14] The 1-year OS in the present study (74%) is consistent with that of other LMICs (63 - 75%) but inferior to HICs (79 - 83%).[36-41] This trend of earlier age at presentation and poorer outcomes observed in SSA has also been observed in African Americans compared with non-Hispanic white Americans.[42]
Although comorbidity did not affect OS in the present study, our analysis produced other unexpected findings that warrant further discussion. It is well described that outcomes are universally poor in patients who present with an advanced (distant) stage of CRC, in all income settings. However, for those presenting with earlier disease (local or regional), outcomes in LMIC settings were worse than in HICs - this was clearly demonstrated in our cohort, as well as in a study from Mumbai, India.[39] For patients presenting with earlier disease, this disparity in outcomes from relatively under-resourced LMIC settings could be explained by: (i) healthcare expenditure bias favouring screening, prevention and management of communicable diseases rather than NCDs; (ii) lack of access to basic chemotherapeutic agents; and (iii) poor health system infrastructure for managing resource-intensive illnesses.[43] CRC is a case in point here, as it requires substantial infrastructure (computed tomography, magnetic resonance imaging, colonoscopy services, histopathology) and integrated MDT management with capacity to offer any combination of radiation oncology, chemotherapy (including targeted therapy) and surgery of the primary tumour as well as liver metastases. Of relevance for the SA healthcare system, we demonstrated that when first treatment was delayed by longer than 40 days after diagnosis, the risk of dying from CRC doubled. A large study from Taiwan showed similar adverse effects on outcome with treatment delays >30 days.[44]
As well as being relatively young with little comorbidity, almost 40% of our cohort had distant disease at time of presentation. These data concur with a cohort from a healthcare funder's database in Johannesburg and the abovementioned studies from South Asia, Nigeria and Ghana, where 25 - 58% of CRC patients had advanced disease at presentation.[20,29,30,33,35-37] However, distant disease at time of presentation is not unique to LMIC settings, and has been extensively described in HICs, albeit in older persons.[8,9,12,14,18] The trend of younger people presenting with advanced disease in our setting may be attributed to a number of contextual factors. Some pertain to an individual's health-seeking behaviour, and others relate to health system failure that may occur at various levels. [17,45] These factors include absent/limited capacity for screening and prevention (even for unaffected family members of those with CRC), missed/delayed diagnosis in the young because healthcare practitioners misinterpret the signs and symptoms of CRC, circuitous referral mechanisms from primary practitioner to specialist referral centres, and few specialist referral facilities with MDTs to manage CRC.[43,46,47]
Interestingly, the rectum was the predominant location of the primary cancer in our cohort. This finding was analogous with findings in the abovementioned studies from LMICs, where approximately half of the participants had rectal cancer, and differed from HIC studies, where less than a third had rectal cancer.[29,30,33,35-37]
Study limitations and strengths
In the absence of a population-based cancer registry, this sample of CRC cases from a large urban metropole may not be representative of the overall SA population including rural patients. For survival outcomes, the relatively short median follow-up time is a limitation. Compared with large population-based registries in HICs, our sample size is relatively small, although analytical power was shown to be sufficient for the research questions addressed. The major strength of this study is the longitudinal design of the CRCSA cohort that enabled follow-up for survival data, which are lacking from many SSA studies.
Conclusions
Comorbidity was uncommon and had no significant adverse effect on OS in our CRCSA cohort. Our patients tended to present at a relatively young age, and with more rectal than colon cancer. For those in our cohort presenting with local and regional disease, survival was worse compared with HICs. However, if colorectal cancer patients are treated timeously, OS may be improved significantly. While our results appear to differ from those from HICs, they are consistent with those from other LMICs, particularly in sub-Saharan Africa.
To fully understand the epidemiology of CRC in SA, population-based registries are essential and future research exploring genetic, environmental and gene-environment interactions that predispose to CRC in our region is needed. Population registries will enable development of risk scores for predicting risk of CRC, particularly in younger people. Health systems research would help to focus interventions to improve OS through early detection and fast-tracking for initiation of treatment within 40 days. The exact points of contact patients have with the healthcare system that delay management therefore need to be identified and addressed.
Declaration. None.
Acknowledgements. None.
Author contributions. CB: conceptualised the study, wrote the first draft of the article, incorporated edits and redrafted the article to its final format, and submitted the article; BB: conceptualised the study and revised the final draft of the article; SM: oversaw participant recruitment and follow-up, data collection and quality control, and revised the final draft of the article; HM: managed the database and data entry and revised the final draft of the article; PG: performed statistical analysis of the study data and revised the final draft of the article; HRE: conceptualised the study, oversaw the ethics approval, contributed to the first draft and revised subsequent drafts of the article; JF: conceptualised the article, and contributed to the first and subsequent drafts of the article; LP, DS, RLF, NH, DL: all contributed to patient recruitment and management and data collection, and revised the final draft of the article; DB: revised the final draft of the article; PR: principal investigator on the study and the grant holder, and revised the final draft of the article.
Funding. The CRCSA study is funded by the Medical Research Council of South Africa, through the Wits/SAMRC Common Epithelial Cancer Research Centre (CECRC) Grant (PR, principal investigator).
Conflicts of interest. None.
References
1. International Agency for Research on Cancer. Colorectal cancer (from GLOBOCAN 2018). 2018. http://gco.iarc.fr/today/data/factsheets/cancers/10_8_9-Colorectum-fact-sheet.pdf (accessed 18 February 2019). [ Links ]
2. Favoriti P, Carbone G, Greco M, Pirozzi F, Pirozzi REM, Corcione F. Worldwide burden of colorectal cancer: A review. Updates Surg 2016;68(1):7-11. https://doi.org/10.1007/s13304-016-0359-y [ Links ]
3. Bray F, Jemal A, Grey N, Ferlay J, Forman D. Global cancer transitions according to the Human Development Index (2008 - 2030): A population-based study. Lancet Oncol 2012;13(8):790-801. https://doi.org/10.1016/S1470-2045(12)70211-5 [ Links ]
4. Bray F, Soerjomataram I. The changing global burden of cancer: Transitions in human development and implications for cancer prevention and control. In: Gelband H, Jha P, Sankaranarayanan R, Horton S, eds. Cancer: Disease Control Priorities (vol. 3). 3rd ed. Washington, DC: International Bank for Reconstruction and Development/World Bank, 2015. http://www.ncbi.nlm.nih.gov/books/NBK343643/ (accessed 15 March 2019). [ Links ]
5. Kelly P, Katema M, Amadi B, et al Gastrointestinal pathology in the University Teaching Hospital, Lusaka, Zambia: Review of endoscopic and pathology records. Trans R Soc Trop Med Hyg 2008;102(2):194-199. https://doi.org/10.1016/j.trstmh.2007.10.006 [ Links ]
6. Angelo N, Dreyer L. Colorectal carcinoma - a new threat to black patients? A retrospective analysis of colorectal carcinoma received by the Institute for Pathology, University of Pretoria. S Afr Med J 2001;91(8):689-693. [ Links ]
7. Mayosi BM, Flisher AJ, Lalloo UG, Sitas F, Tollman SM, Bradshaw D. The burden of non-communicable diseases in South Africa. Lancet 2009;374(9693):934-947. https://doi.org/10.1016/S0140-6736(09)61087-4 [ Links ]
8. Cuthbert CA, Hemmelgarn BR, Xu Y, Cheung WY. The effect of comorbidities on outcomes in colorectal cancer survivors: A population-based cohort study. J Cancer Surviv 2018;12(6):733-743. https://doi.org/10.1007/s11764-018-0710-z [ Links ]
9. Erichsen R, Horváth-Puhó E, Iversen LH, Lash TL, S0rensen HT. Does comorbidity interact with colorectal cancer to increase mortality? A nationwide population-based cohort study. Br J Cancer 2013;109(7):2005-2013. https://doi.org/10.1038/bjc.2013.541 [ Links ]
10. Boakye D, Rillmann B, Walter V, Jansen L, Hoffmeister M, Brenner H. Impact of comorbidity and frailty on prognosis in colorectal cancer patients: A systematic review and meta-analysis. Cancer Treat Rev 2018;64:30-39. https://doi.org/10.1016/j.ctrv.2018.02.003 [ Links ]
11. Sarfati D, Tan L, Blakely T, Pearce N. Comorbidity among patients with colon cancer in New Zealand. N Z Med J 2011;124(1338):76-88. [ Links ]
12. Baretti M, Rimassa L, Personeni N, et al Effect of comorbidities in stage II/III colorectal cancer patients treated with surgery and neoadjuvant/adjuvant chemotherapy: A single-center, observational study. Clin Colorectal Cancer 2018;17(3):e489-e498. https://doi.org/10.1016/j.clcc.2018.03.010 [ Links ]
13. Sarfati D, Hill S, Blakely T, Robson B, et al. The effect of comorbidity on the use of adjuvant chemotherapy and survival from colon cancer: A retrospective cohort study. BMC Cancer 2009;9:116. https://doi.org/10.1186/1471-2407-9-116 [ Links ]
14. Iversen LH, N0rgaard M, Jacobsen J, Laurberg S, S0rensen HT. The impact of comorbidity on survival of Danish colorectal cancer patients from 1995 to 2006 - a population-based cohort study. Dis Colon Rectum 2009;52(1):71-78. https://doi.org/10.1007/DCR.0b013e3181974384 [ Links ]
15. Bebington B, Singh E, Fabian J, et al. Design and methodology of a study on colorectal cancer in Johannesburg, South Africa. JGH Open 2018;2(4):139-143. https://doi.org/10.1002/jgh3.12061 [ Links ]
16. World Population Review. Johannesburg population. 2019. http://worldpopulationreview.com/world-cities/johannesburg-population/ (accessed 31 March 2019). [ Links ]
17. Mayosi BM, Benatar SR. Health and health care in South Africa - 20 years after Mandela. N Engl J Med 2014;371(14):1344-1353. https://doi.org/10.1056/NEJMsr1405012 [ Links ]
18. Lemmens VEPP, Janssen-Heijnen MLG, Houterman S, et al. Which comorbid conditions predict complications after surgery for colorectal cancer? World J Surg 2007;31(1):192-199. https://doi.org/10.1007/s00268-005-0711-8 [ Links ]
19. Kabudula CW, Houle B, Collinson MA, Kahn K, Tollman S, Clark S. Assessing changes in household socioeconomic status in rural South Africa, 2001 - 2013: A distributional analysis using household asset indicators. Soc Indic Res 2017;133(3):1047-1073. https://doi.org/10.1007/s11205-016-1397-z [ Links ]
20. Brand M, Gaylard P, Ramos J. Colorectal cancer in South Africa: An assessment of disease presentation, treatment pathways and 5-year survival. S Afr Med J 2018;108(2):118-122. https://doi.org/10.7196/SAMJ.2018.v108i2.12338 [ Links ]
21. Collett D. Modelling Survival Data in Medical Research. New York: Chapman & Hall/CRC, 2015. https://www.taylorfrancis.com/books/9780429196294 (accessed 9 May 2019). [ Links ]
22. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chronic Dis 1987;40(5):373-383. https://doi.org/10.1016/0021-9681(87)90171-8 [ Links ]
23. Katz JN, Chang LC, Sangha O, Fossel AH, Bates DW. Can comorbidity be measured by questionnaire rather than medical record review? Med Care 1996;34(1):73-84. https://doi.org/10.1097/00005650-199601000-00006 [ Links ]
24. Vyas S, Kumaranayake L. Constructing socio-economic status indices: How to use principal components analysis. Health Policy Plan 2006;21(6):459-468. https://doi.org/10.1093/heapol/cz1029 [ Links ]
25. Filmer D, Pritchett LH. Estimating wealth effects without expenditure data - or tears: An application to educational enrollments in states of India. Demography 2001;38(1):115-132. https://doi.org/10.1353/dem.2001.0003 [ Links ]
26. Luque-Fernandez MA, Redondo-Sanchez D, Rodríguez-Barranco M, Carmona-García MC, Marcos-Gragera R, Sánchez M-J. The pattern of comorbidities and multimorbidity among colorectal cancer patients in Spain: CoMCoR study. bioRxiv 2019;526673. https://doi.org/10.1101/526673 [ Links ]
27. Wang J-W, Sun L, Ding N, et al. The association between comorbidities and the quality of life among colorectal cancer survivors in the People's Republic of China. Patient Prefer Adherence 2016;10:1071-1077. https://doi.org/10.2147/PPA.S100873 [ Links ]
28. Katsidzira L, Gangaidzo IT, Mapingure MP, Matenga JA. Retrospective study of colorectal cancer in Zimbabwe: Colonoscopic and clinical correlates. World J Gastroenterol 2015;21(8):2374-2380. https://doi.org/10.3748/wjg.v21.i8.2374 [ Links ]
29. Agyemang-Yeboah F, Yorke J, Obirikorang C, et al. Patterns and presentations of colorectal cancer at Komfo-Anokye teaching hospital Kumasi, Ghana. Pan Afr Med J 2017;28:201. https://doi.org/10.11604/pamj.2017.28.121.12927 [ Links ]
30. Chandrasinghe PC, Ediriweera DS, Hewavisenthi J, Kumarage SK, Fernando FR, Deen KI. Colorectal cancer burden and trends in a South Asian cohort: Experience from a regional tertiary care center in Sri Lanka. BMC Res Notes 2017;10(1):535. https://doi.org/10.1186/s13104-017-2869-1 [ Links ]
31. Oh H-S, Chung H-J, Kim H-K, Choi J-S. Differences in overall survival when colorectal cancer patients are stratified into new TNM staging strategy. Cancer Res Treat 2007;39(2):61-64. https://doi.org/10.4143/crt.2007.39.2.61 [ Links ]
32. Salako O, Okediji PT, Habeebu MY, et al The pattern of comorbidities in cancer patients in Lagos, south-western Nigeria. Ecancermedicalscience 2018;12:843. https://doi.org/10.3332/ecancer.2018.843 [ Links ]
33. Saluja S, Alatise OI, Adewale A, et al. A comparison of colorectal cancer in West African and North American patients: Is the cancer biology different? Surgery 2014;156(2):305-310. https://doi.org/10.1016/j.surg.2014.03.036 [ Links ]
34. Maharaj R, Shukla PJ, Sakpal SV, Naraynsingh V, Dan D, Hariharan S. The impact of hereditary colorectal cancer on the Indian population. Indian J Cancer 2014;51(4):538. https://doi.org/10.4103/0019-509X.175307 [ Links ]
35. Deo SV, Shukla NK, Srinivas G, et al Colorectal cancers - experience at a regional cancer centre in India. Trop Gastroenterol 2001;22(2):83-86. [ Links ]
36. Adesanya AA, Da JR-A. Colorectal cancer in Lagos: A critical review of 100 cases. Niger Postgrad Med J 2000;7(3):129-136. [ Links ]
37. Agyemang-Yeboah F, Yorke J, Obirikorang C, et al. Colorectal cancer survival rates in Ghana: A retrospective hospital-based study. PLoS One 2018;13(12):e0209307. https://doi.org/10.1371/journal.pone.0209307 [ Links ]
38. Benitez Majano S, di Girolamo C, Rachet B, et al. Surgical treatment and survival from colorectal cancer in Denmark, England, Norway, and Sweden: A population-based study. Lancet Oncol 2019;20(1):74-87. https://doi.org/10.1016/S1470-2045(18)30646-6 [ Links ]
39. Yeole BB, Sunny L, Swaminathan R, Sankaranarayanan R, Parkin DM. Population-based survival from colorectal cancer in Mumbai (Bombay), India. Eur J Cancer 2001;37(11):1402-1408. https://doi.org/10.1016/S0959-8049(01)00108-3 [ Links ]
40. Chen J-G, Chen H-Z, Zhu J, et al. Cancer survival in patients from a hospital-based cancer registry, China. J Cancer 2018;9(5):851-860. https://doi.org/10.7150/jca.23039 [ Links ]
41. Crooke H, Kobayashi M, Mitchell B, et al. Estimating 1- and 5-year relative survival trends in colorectal cancer (CRC) in the United States: 2004 to 2014. J Clin Oncol 2018;36(4_suppl):587-587. https://doi.org/10.1200/JCO.2018.36.4_suppl.587 [ Links ]
42. Augustus GJ, Ellis NA. Colorectal cancer disparity in African Americans: Risk factors and carcinogenic mechanisms. Am J Pathol 2018;188(2):291-303. https://doi.org/10.1016/j.ajpath.2017.07.023 [ Links ]
43. Morhason-Bello IO, Odedina F, Rebbeck TR, et al. Challenges and opportunities in cancer control in Africa: A perspective from the African Organisation for Research and Training in Cancer. Lancet Oncol 2013;14(4):e142-e151. https://doi.org/10.1016/S1470-2045(12)70482-5 [ Links ]
44. Lee Y-H, Kung P-T, Wang Y-H, Kuo W-Y, Kao S-L, Tsai W-C. Effect of length of time from diagnosis to treatment on colorectal cancer survival: A population-based study. PLoS One 2019;14(1):e0210465. https://doi.org/10.1371/journal.pone.0210465 [ Links ]
45. Coovadia H, Jewkes R, Barron P, Sanders D, McIntyre D. The health and health system of South Africa: Historical roots of current public health challenges. Lancet 2009;374(9692):817-834. https://doi.org/10.1016/S0140-6736(09)60951-X [ Links ]
46. Irabor DO. Emergence of colorectal cancer in West Africa: Accepting the inevitable. Niger Med J 2017;58(3):87-91. https://doi.org/10.4103/0300-1652.234076 [ Links ]
47. O'Connell JB, Maggard MA, Livingston EH, Yo CK. Colorectal cancer in the young. Am J Surg 2004;187(3):343-348. https://doi.org/10.1016/j.amjsurg.2003.12.020 [ Links ]
 Correspondence:
Correspondence:
C Bouter
carolynbouter@outlook.com
Accepted 30 September 2019


{kind=link}
{kind=link}