










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 n.5 Pretoria May. 2020
http://dx.doi.org/10.7196/SAMJ.2020.v110i5.14739
CORRESPONDENCE
Decisive and strong leadership and intersectoral action from South Africa in response to the COVID-19 virus
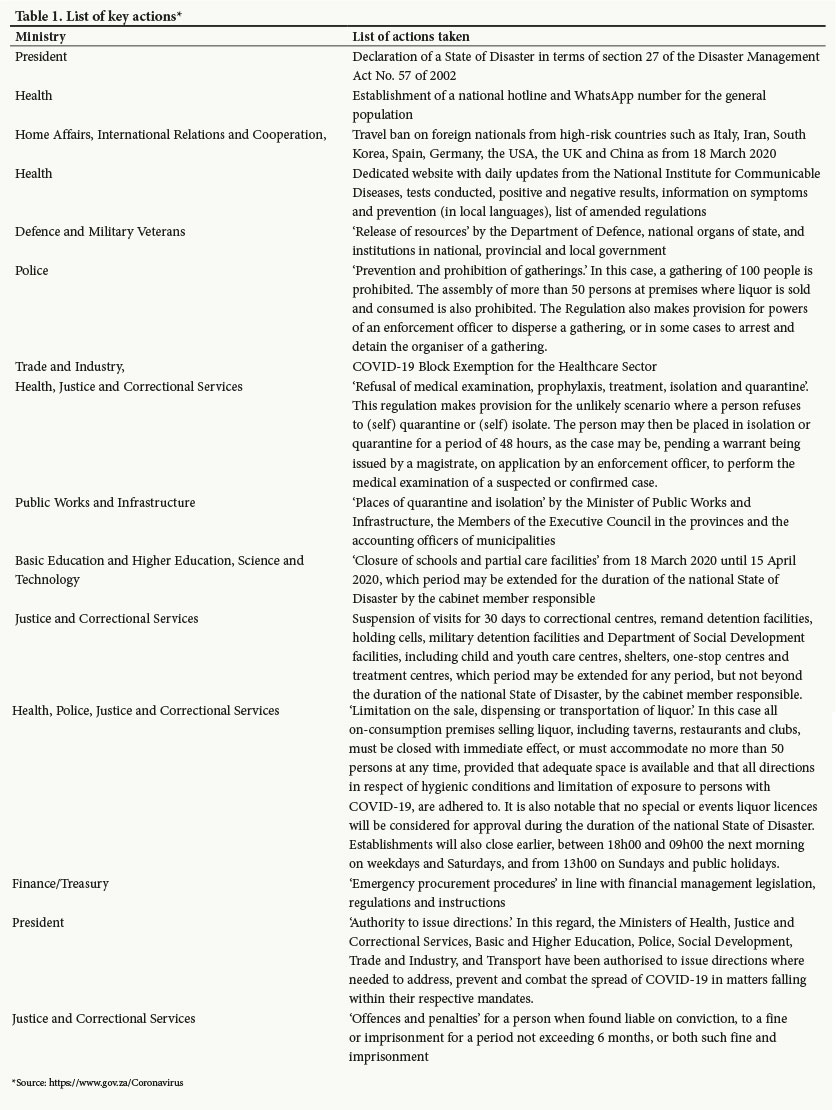
To the Editor: South Africa (SA) reported its first case of coronavirus disease 2019 (COVID-19) on 5 March 2020. For the 14 days from then until the time of writing (5 - 19 March), we have seen decisive, strong leadership from the President, and significant, important and necessary co-ordination between different ministries including Education, Justice, Health, Trade and Industry, Transport, Public Works and Infrastructure, Finance, Cooperative Governance and Traditional Affairs, and International Relations and Cooperation. In these 14 days, SA has rapidly produced and implemented a number of action items (Table 1). This intersectoral action and co-ordination is something that has been needed for a long time to address development in SA.
On 19 March 2020, the Competition Commission published a COVID-19 block exemption for the healthcare sector.[1] The exemption is aimed at promoting co-ordination, sharing of information and standardisation of practice across the entire healthcare sector. It also seeks to facilitate cost reduction measures, in particular costs of diagnostic tests, treatment and other preventive measures. Finally, the exemption seeks to promote agreements between the National
Department of Health and the private sector, with the sole purpose of making additional capacity at healthcare facilities available to the public sector and ensuring adequate medical supplies. COVID-19 has dramatically highlighted the need for a significantly more integrated healthcare system.
The Health Market Inquiry (HMI) made recommendations that will promote standardisation and knowledge sharing as well as a method to deal with pricing within the functions of the proposed supply-side regulator. Perhaps this exemption can build trust between players and will ease us into a more rational and integrated healthcare system.
Evidence from the HMI showed an excess capacity of high-care and intensive care unit (ICU) beds in the private healthcare sector, and the HMI concluded that there was inappropriate use of these beds.[2] To free up private sector ICU beds will require the private sector to change its criteria of how they are used. Hospitals will also have to improve general ward care if this is one of the reasons doctors prefer to admit to an ICU, as was reported to the HMI. Improving general ward care will improve efficiency to the benefit of all.
Another area that requires coherence between the public and private sectors is COVID-19 testing. Public sector testing at the moment is in our opinion correctly restricted to individuals who meet the case definition. A live broadcast of a question and answer session organised by the South African Medical Association and the Minister of Health revealed that general practitioners were inundated with requests for testing that the GPs thought was not indicated. There were also reports that some employers demanded that employees arrive at work with a confirmed negative test result. This is irrational - a negative test today does not mean a negative test tomorrow - and furthermore it is not constitutional. SA's experience with HIV testing has confirmed the unconstitutionality of demanding people's confidential medical results through the courts. Education of some employers is clearly required. Over and above this, testing the worried well for COVID-19 is a waste of resources.
We should not be naive, and must consider that profiteers both from the public and private sectors, in equal measure, may try to take advantage of this situation. Oversight of the resources that are being invested in protecting SA from the COVID-19 virus must be exercised.
The threat that COVID-19 presents has resulted in leadership from government and apparent willingness of all South Africans to play their part. However, SA faces just as real a threat to its health, its economy and its development: the crises of poverty, inequality and unemployment are the social determinants that threaten our wellbeing as individuals and as a society at large. We would have a healthier country if we could demonstrate the same degree of intersectoral action and social mobilisation across the public/ private divide in the form of meaningful social compacts. There are excellent lessons to be learnt here, and this opportunity should not be wasted.
Lungiswa Nkonki
Department of Global Health, Division of Health Systems and Public Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa inkonki@sun.ac.za
Sharon Fonn
School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
References
1. Ngcobo S, Fonn S, Bhengu N, van Gent C, Nkonki L. Health Market Inquiry: Final Findings and Recommendations Report. Pretoria: Competition Commission of South Africa, 2019. http://www.compcom.co.za/wp-content/uploads/2020/01/Final-Findings-and-recommendations-report-Health-Market-Inquiry.pdf (accessed 24 March 2020). [ Links ]
2. Department of Trade and Industry, South Africa. Competition Act (89/1998), as amended: COVID-19 Block Exemption for the Healthcare Sector, 2020. Government Gazette No. 43114, 19 March 2020. (Published under Government Notice R. 349.) https://www.gov.za/sites/default/files/gcis_document/202003/4311419-3dti.pdf (accessed 19 March 2020). S Afr Med J. Published online 27 March 2020. [ Links ]


{kind=link}