










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 n.2 Pretoria Feb. 2020
http://dx.doi.org/10.7196/samj.2020.v110i2.14024
RESEARCH
Maternal and neonatal outcomes following the introduction of oral hypoglycaemic agents for gestational diabetes mellitus were comparable to insulin monotherapy in two historical cohorts
V NicolaouI, II; L SoepnelIII, IV; K R HuddleV; N LevittVI; K Klipstein-GrobuschVII, VIII; S A NorrisIX, X
IMB BCh, DA, FCP (SA), FSEM, MMed (Endocrinology); South African Medical Research Council/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMB BCh, DA, FCP (SA), FSEM, MMed (Endocrinology); Department of Internal Medicine, Chris Hani Baragwanath Academic Hospital and Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIBSc, MSc, MD; South African Medical Research Council/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVBSc, MSc, MD; Julius Global Health, Julius Center of Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, The Netherlands
VMB BCh, FRCP (UK); Department of Internal Medicine, Chris Hani Baragwanath Academic Hospital and Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIMB ChB, MD, FCP (SA); Diabetic Medicine and Endocrinology, Department of Medicine, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
VIIMSc, PhD; Julius Global Health, Julius Center of Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, The Netherlands
VIIIMSc, PhD; Division of Epidemiology and Biostatistics, School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IXBA Hons, BSc Hons, MSc, PhD; South African Medical Research Council/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
XBA Hons, BSc Hons, MSc, PhD; Department of Paediatrics, School of Clinical Medicine, University of Cambridge, UK
ABSTRACT
BACKGROUND. Gestational diabetes mellitus (GDM), a disorder of glucose intolerance first encountered during pregnancy, has far-reaching implications for both mother and child. Insulin therapy remains the 'gold standard' of care, with oral hypoglycaemic agents (OHAs) increasingly being viewed as potential alternatives.
OBJECTIVES. To compare maternal and neonatal outcomes in two cohorts of women with GDM exposed to either insulin monotherapy or OHAs.
METHODS. A retrospective medical record review at Chris Hani Baragwanath Academic Hospital in South Africa was conducted for women with GDM diagnosed using the 100 g oral glucose tolerance test and/or random capillary blood glucose >11.1 mmol/L in 2010 - 2014. The findings were compared with a previous audit at the same clinic for the period 1992 - 2002. Variables of interest included maternal demographics, maternal comorbidities, glycaemic indices, treatments used during pregnancy, and obstetric and neonatal outcomes.
RESULTS. A total of 192 women with GDM were identified for 2010 - 2014, and there were 348 women in the previous audit (1992 - 2002). Baseline characteristics and outcomes of women in the two cohorts were similar apart from earlier presentation (mean (standard deviation) gestational age (GA) 27 (7.5) weeks v. 28.3 (6.4) weeks; p=0.04), lower GA at delivery (36.3 (3.6) weeks v. 37 (1.6) weeks); p=0.008) and lower macrosomia rates (12.5% v. 4.9%; p=0.011) in the later cohort. When comparing the individual OHAs against insulin in the later cohort, both agents were comparable to insulin in terms of maternal and neonatal outcomes.
CONCLUSIONS. This study contributes to the paucity of data on the safety of OHAs in GDM pregnancy in terms of maternal and neonatal outcomes. OHAs were shown to be an effective alternative to insulin for women with GDM in whom lifestyle measures fail, particularly in a resource-poor setting.
The landscape of gestational diabetes mellitus (GDM) has remained dynamic, with the prevalence, definition, screening protocols, diagnostic criteria and therapeutic modalities continuously changing from as early as the 1960s. Most recently, GDM has been defined as a disorder of glucose intolerance first encountered during pregnancy that is not clearly overt diabetes.[1] GDM has far-reaching and well-known ramifications for both mother and infant.[2] Global prevalence estimates are 16.9%,[3,4] with recent studies in South Africa (SA) showing prevalence figures ranging from 9.1% to 25.8%.[5,6]
Traditionally, GDM is initially managed with dietary and lifestyle interventions alone. However, insulin is introduced if glycaemic goals are not achieved.[7-9] Oral hypoglycaemic agents (OHAs) are an attractive alternative if lifestyle measures fail, particularly in resource-poor countries, because of their low cost and ease of administration. However, their use for GDM is surrounded by much debate regarding efficacy and safety, and they are recommended by some guidelines[9-11] and omitted in others.[12] One meta-analysis that included 13 studies utilising various diagnostic tests and criteria for GDM, with representation from both high- and low-income countries, investigated the safety of OHAs compared with insulin when treating GDM.[13] It demonstrated a higher preterm birth rate (relative risk (RR) 1.51) in patients exposed to metformin monotherapy, with a reduced risk of both gestational hypertension (RR 0.54) and lowered postprandial glucose levels. A further meta-analysis of 15 studies showed an increased risk of macrosomia and neonatal hypoglycaemia in patients exposed to glibenclamide.[14] Research from SA has generally shown reassuring safety outcomes in terms of fetal anomalies and maternal glycaemic control for both metformin and glibenclamide in patients with both type 2 diabetes in pregnancy and GDM.[15,16] However, a recent study showed notably increased perinatal mortality (PNM) in type 2 diabetes patients exposed to glibenclamide, which could not be explained.[15]
Objectives
To compare the fetal and maternal outcomes of two cohorts of patients with GDM treated at Chris Hani Baragwanath Academic Hospital (CHBAH) in Johannesburg, SA, a decade apart, where the first cohort (1992 - 2002) was exposed to insulin monotherapy and the more recent group (2010 - 2014) to one or more treatment combinations including OHA monotherapy (metformin alone), OHA dual therapy (metformin plus glibenclamide), or insulin monotherapy. Furthermore, the outcomes in the 2010 - 2014 cohort were compared between the insulin monotherapy group v. those exposed to OHAs.
Methods
Study population
This study retrospectively compared two cohorts of women attending the gestational endocrine clinic at CHBAH for GDM, the first between 1992 and 2002 and the second between 2010 and 2014. Characteristics and outcomes of the 1992 - 2002 cohort, where patients were exclusively exposed to insulin monotherapy, have been published previously[17] and are included for the purposes of the present study. A secondary analysis in the later cohort was performed with a medical record review of women exposed to OHAs v. insulin monotherapy, and their outcomes were compared.
CHBAH, a 3 000-bed teaching hospital with between 1 400 and 1 600 deliveries per month, serves the population of the sprawling township of Soweto, SA, ethnically predominantly black. All patients with singleton pregnancies treated at CHBAH for GDM between 1992 and 2002 and between 2010 and 2014, either diagnosed by random capillary blood glucose >11.1 mmol/L or fulfilling National Diabetes Data Group (NDDG) criteria following a 3-hour 100 g oral glucose tolerance test (OGTT), were included in the study. Both cohorts had similar screening strategies for GDM. Participants with twin pregnancies and other subtypes of diabetes, including pregestational diabetes, pancreatic diabetes and steroid-induced diabetes, were excluded. A control group was defined as patients who presented after 36 weeks' gestational age (GA) or received <2 weeks of medical intervention, and these patients were excluded for the purposes of the study. The study protocol was approved by the Human Research Ethics Committee of the University of the Witwatersrand (ref. no. M180316).
Definitions
Diabetes was considered gestational if the diagnosis was first made during pregnancy in women referred because of the presence of risk factors for diabetes: persistent glycosuria, first-degree family history of diabetes, previous unexplained perinatal losses, previous GDM, or history of a macrosomic baby. Selective screening for GDM was performed between 24 and 28 weeks' GA. GDM was diagnosed using a 100 g 3-hour OGTT and NDDG criteria, which required two or more of the following plasma glucose levels for the diagnosis of GDM: fasting plasma glucose (FPG) >5.8 mmol/L, 1-hour post-glucose load >10.6 mmol/L, 2-hour post-glucose load >9.2 mmol/L, or 3-hour post-glucose load >9.2 mmol/L. GDM was classified as 'overt' if the baseline FPG was >7.0 mmol/L.
Maternal characteristics and outcomes were defined as follows. GA was determined using an early ultrasound scan. Glycaemic control: mean blood glucose (MBG) <7.1 mmol/L for the third trimester, calculated as a mean of daily self-monitored six-point profiles, including both fasting and 1-hour post-prandial. Dietary failure: failing to achieve glycaemic control after 2 weeks of dietary intervention. Diabetic nephropathy: microalbuminuria, with a microalbumin-creatinine ratio >30 mg/mmol on repeated testing, in the absence of urinary tract infection and other renal disease. Body mass index (BMI): the patient was considered obese if the BMI was >30 kg/m2 at the first visit. Anaemia: haemoglobin concentration <11 g/dL. HIV-positive: based on results from rapid or antibody tests before or at the time of initial presentation. Obstetric complications included premature labour, caesarean section (CS), miscarriage, hypertensive disorders of pregnancy (HDP), urinary tract infection, polyhydramnios, oligohydramnios and maternal death. Hypertension was diagnosed when blood pressure readings were elevated (>140/90 mmHg) for at least two measurements. This was further categorised into HDP and chronic hypertension. HDP was further classified into pregnancy-induced hypertension (PIH), where hypertension developed after 20 weeks of pregnancy, pre-eclampsia, where PIH was found in the presence of proteinuria on more than one occasion, and eclampsia, where PIH was found in the presence of proteinuria and seizures. Chronic hypertension was defined as hypertension diagnosed prior to the pregnancy. Maternal hypoglycaemia was defined as one or more episodes of hypoglycaemia severe enough to necessitate the administration of intravenous dextrose.
Neonatal outcomes were defined as follows. Prematurity/preterm birth: delivery at <37 completed weeks' GA. Miscarriage: loss in pregnancy occurring at <28 completed weeks' GA. Stillbirth: loss in pregnancy occurring at >29 weeks' GA. Early neonatal death: neonatal death occurring in the first week. PNM: the number of stillbirths and early neonatal deaths out of the total number of deliveries (successful deliveries and stillbirths). Low birth weight (LBW): birth weight <2 500 g. Macrosomia: birth weight >4 000 g. Major congenital anomalies: spinal, cardiac, central nervous system, renal or digestive system anomalies.
Definitions applied to both study cohorts except for MBG and nephropathy, where the MBG in the earlier cohort was calculated as a mean of the fasting and 1-hour plasma glucose levels, and nephropathy was defined as dipstick urinalysis positive for proteinuria (protein >0.3 g/L) on repeated testing.
Clinical practice
The specialist clinic at CHBAH was established in 1983 and is staffed by a physician, an obstetrician, a paediatrician and a diabetes nurse educator. The initial visit comprised a full clinical assessment with ultrasound and treatment initiation. Initial ultrasound was used to assess GA and to rule out any major fetal anomalies. All patients were screened for target organ damage, including retinopathy and nephropathy. Newly diagnosed women with GDM (as per the NDDG criteria) were hospitalised for glycaemic stabilisation. Patients were taught blood glucose monitoring by the nurse educator. Fingerprick capillary blood samples were obtained using lancets, and blood glucose levels were read using various glucometers for the later cohort. In the earlier cohort, glucose levels were read visually using Haemo-glukotest 20-800R strips (Roche Diagnostics, Germany). Dietary advice was provided on an ongoing basis by a dietician and/ or a nurse educator, with a 2-week trial of dietary monotherapy being prescribed where the fasting glucose level was <7.0 mmol/L. For the period 1990 - 2010, insulin monotherapy was prescribed in the event of dietary failure. From 2010 onward, OHAs (metformin and/or glibenclamide) were introduced as follows: metformin monotherapy was prescribed in the event of dietary failure, then therapy was escalated with either the addition of glibenclamide or a switch to insulin monotherapy. Insulin was initiated at the outset in patients whose fasting glucose exceeded 7.0 mmol/L or if maternal or fetal complications were present. Glycaemic targets were <5.3 mmol/L for fasting glucose and <7.8 mmol/L for a 1-hour postprandial reading for the later cohort, levels between 4 and 7 mmol/L being accepted for the earlier cohort. Combined MBG, which included an average of the fasting and 1-hour postprandial readings of <7.1 mmol/L, was included to assess glycaemic control as per institutional practice. Patient-monitored daily six-point profiles were also assessed based on Society for Endocrinology, Metabolism and Diabetes of South Africa (SEMDSA) criteria.[11,18]
Following the initial assessment, patients were seen fortnightly or sooner if indicated. At each visit, patients were clinically assessed, the results of home blood glucose monitoring were noted, and treatment was adjusted if necessary. Ultrasound scans were repeated at intervals to assess fetal growth and anomalies. A point-of-care glycated haemoglobin (HbA1c) test was performed monthly using the DCA Vantage Analyzer (Siemens, Germany), which had been standardised and was traceable to the Diabetes Complications and Control Trial. All patients had an HbA1c test within a month prior to delivery. After 32 weeks' GA the visits were weekly until 37 - 38 completed weeks, when labour was induced. Time and mode of delivery were dictated by obstetric factors and glycaemic control, with the goal of 38 completed weeks of pregnancy unless complications arose. During labour, glucose levels were monitored hourly and controlled using dextrose-insulin infusions. Oral and/or insulin therapy was stopped postpartum, and only reinitiated based on results from inpatient self-glucose monitoring. All GDM patients not requiring ongoing therapy were asked to return for a 6-week 75 g OGTT at the maternity clinic. All neonates were assessed for clinical or biochemical abnormalities by paediatric staff in the neonatal unit and managed accordingly.
The control group defined above was excluded for the purposes of this study.
Statistical analysis
Data were captured and entered directly into an electronic database (REDCap, USA), cleaned and imported into Stata 13 (StataCorp, USA) for statistical analysis. Comparison of the 1992 - 2002 v. 2010 - 2014 cohort was expressed as numbers and percentages for categorical variables and means and standard deviations (SDs) for continuous variables. Comparisons between the two cohorts were made using an online statistical calculator, MedCalc (version 16.4.3; www.medcalc.org), where a χ2 test was used for categorical outcomes and a f-test was employed for the purpose of continuous variables, to determine statistical significance.
Baseline characteristics of the 2010 - 2014 cohort were described using numbers and percentages for categorical variables and, depending on normality, means and SDs or medians and interquartile ranges (IQRs) for continuous variables. To test for normality, a skewness-kurtosis test was performed if the mean and median were substantially different. Statistical significance testing in the 2010 -2014 group was done using Student's f-test or the non-parametric Mann-Whitney (7-test for continuous outcomes, and a χ2 statistic or Fisher's exact test for categorical outcomes. For analysis across more than two groups, analysis of variance (ANOVA) or the non-parametric Kruskal-Wallis test was used. Statistical significance was set at p<0.05.
Results
Comparison of the two cohorts of GDM patients Maternal profiles
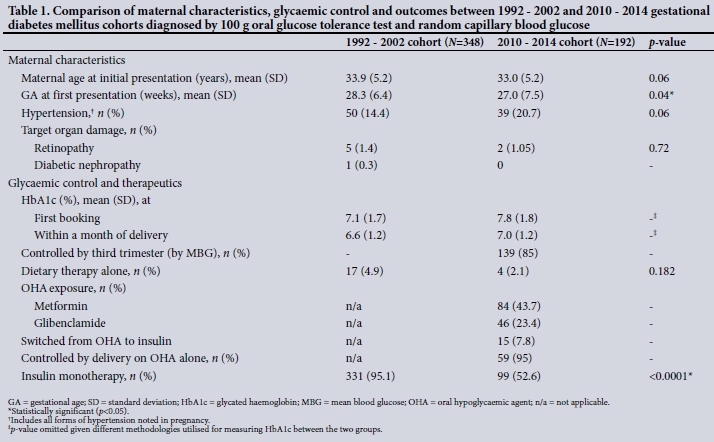
Table 1 presents maternal profiles of the 348 GDM patients in the period 1992 - 2002 and the 192 GDM patients in the period 2010 - 2014. The two cohorts were comparable in terms of maternal age at presentation, overall rates of hypertension (20.7% v. 14.4%; p=0.06) and the significant decrease from HbA1c at first booking to HbA1c within a month of delivery (earlier cohort mean (SD) 7.1% (1.7) to 6.6% (1.2); p=0.0001 and later cohort 7.8% (1.8) to 7.1% (1.4); p=0.000). In the later cohort, first presentation was earlier (mean (SD) 27 (7.5) weeks v. 28 (6.4) weeks; p=0.04), and >85% of all patients in this cohort achieved their glycaemic goals as measured by their MBG for the third trimester, with >95% of those on oral agents alone achieving good control by delivery. Failure rates for dietary monotherapy were high for both cohorts (97.9% v. 95.1%). The need for insulin monotherapy was lower for the later cohort than for the earlier cohort (52.6% v. 95.1%).
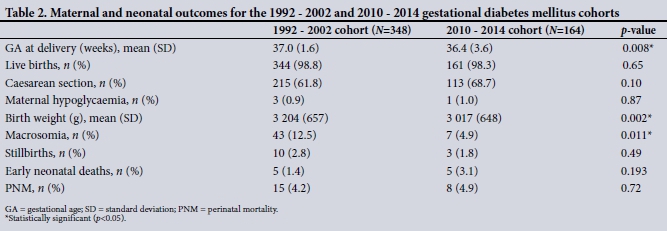
Maternal and neonatal outcomes (Table 2)
GA at delivery in the recent cohort was lower (mean (SD) 36.4 (3.65) weeks v. 37 (1.6) weeks; p=0.008), with a higher number of preterm deliveries. Birth weight and macrosomia rates were statistically lower in the most recent cohort (3 017 (648) g v. 3 204 (657) g; p=0.002 and 12.5% v. 4.9%; p=0.01, respectively). PNM was comparable between the cohorts (4.2% v. 4.9%; p=0.72), with fewer stillbirths and a nonsignificant increase in early neonatal deaths in the recent cohort.
Effect of oral agents on maternal and neonatal outcomes in the 2010 - 2014 cohort
In the 2010 - 2014 cohort, 'overt' GDM was diagnosed in 43.8% of patients based on a baseline FPG >7.0 mmol/L. The mean (SD) FPG at first visit for the cohort was 7.3 (2.14) mmol/L. Ninety-nine patients (53.8%) required insulin monotherapy at first diagnosis, with 45.0% requiring OHAs and 2.1% dietary monotherapy. Of those initiated on diet alone, 97.8% failed and required a switch to OHAs. Eighty-four patients (43.7%) were exposed to metformin and 45 (23.4%) to glibenclamide, with 7.8% of the OHA group requiring a switch to insulin. Within the cohort treatment groups, no significant differences were observed in maternal age and BMI in the groups exposed to OHA compared with insulin monotherapy. For the insulin- v. glibenclamide-exposed groups, initial HbA1c (median (IQR) 8.9% (7.2 - 10.1) v. 6.7% (6.3 - 7.1); p=0.001) and weight gain during pregnancy (median 5 (2.2 - 9.6) kg v. 2 (0 - 4) kg; p=0.00) were significantly higher in the insulin group.
Of the 192 files recorded, outcomes were available for 162 patients, given a 16.7% loss-to-follow-up rate. There were no differences in maternal and neonatal outcomes in terms of each oral agent v. insulin. When comparing metformin with insulin, the incidences of prematurity, macrosomia, LBW and PNM were all non-significantly lower with metformin therapy. Outcomes for the glibenclamide-v. insulin-exposed groups were comparable, including rates of macrosomia (11.4% v. 3.3%; p=0.19) and LBW (22.2% v. 14.6%; p=0.35). CS rates, although not different among the groups, were high (78.6%, 77.7% and 64.7%, respectively), with failed induction of labour being the commonest indication. No maternal mortality was reported for the cohort.
Discussion
In this comparative study: (i) lower macrosomia rates and earlier GA at delivery were found in the later cohort exposed to both OHA and insulin therapy (2010 - 2014) v. the earlier cohort (1992 - 2002) exposed to insulin monotherapy; (ii) effectiveness of OHAs was evident in terms of the low number of patients who needed to be switched to insulin; and (iii) maternal and neonatal outcomes were comparable in the group exposed to OHAs and those exposed to insulin alone for the 2010 - 2014 cohort.
When comparing the historical cohorts, the introduction of OHAs in the later cohort was effective in achieving good glycaemic control at delivery, with favourable and comparable maternal and neonatal outcomes, including maternal hypoglycaemia, CS rates, macrosomia, major congenital anomalies and PNM, in women treated with OHAs. This finding is of public health relevance in SA, where limited resources and access to specialised care for GDM often translate into adverse outcomes, because it provides healthcare professionals with a cost-effective and less complex alternative to the 'gold standard' of care, insulin, with a similar safety profile.
Of interest were the lower birth weights and macrosomia rates in the cohort exposed to OHAs. One plausible explanation is the earlier GA at delivery, which may have numerous contributing factors. Metformin has been found to be protective against macrosomia in some studies,[19,20] although this was not evident in our study when metformin monotherapy was compared with insulin alone; however, numbers were small for this comparison. Our study did not corroborate a finding from a robust meta-analysis, including seven randomised controlled trials, of a significant relationship between glibenclamide exposure and higher birth weights, macrosomia rates and neonatal hypoglycaemia compared with insulin therapy.[14]
Lastly, PNM did not differ between the two cohorts (4.2% v. 4.9%; p=0.72), and no higher PNM was found in the OHA-exposed group. This PNM figure, while higher than the national rate of 3.3%[21] for all pregnancies, compares favourably with a recent audit of diabetic pregnancies from Cape Town[22] and those from elsewhere in Africa, which range from 5.2% to 25.4%.[23]
In the 2010 - 2014 cohort, GDM was detected earlier, possibly as a result of improved awareness both among the public and in the public health system through enhanced screening protocols at both primary- and secondary-level clinics. However, the high mean HbA1c at booking raises concern that many of the women had pre-gestational diabetes that had not been diagnosed before pregnancy, highlighting a potential gap in the diabetes screening programmes. Furthermore, this burden of type 2 diabetes mellitus occurs alongside a rising prevalence of obesity,[24] as is appreciated in the recent cohort, with 81.4% of the women having a BMI >30 kg/m2. Despite this high rate of obesity, most of our patients attained good glycaemic control by the third trimester (>85%), with similar outcomes to studies both internationally and locally.[19,20]
In the recent cohort, over half of the patients (53.8%) required insulin from their first visit owing to the severity of their initial dysglycaemia, explained by the fact that close to 50% of the cohort had 'overt' diabetes. In the patients initiated on OHAs, the effectiveness of these agents in this group was evident in the small number of patients who needed to be switched from OHA to insulin (7.8%), and the good glycaemic control at delivery. Notably, both cohorts demonstrated high dietary failure rates compared with figures elsewhere (95.1% and 97.9% v. 20.0 - 30.0%),[12] which is probably due to the presence of more severe cases of dysglycaemia (as indicated by the high initial HbA1c) because of risk factor-based screening rather than universal screening. Furthermore, financial challenges encourage patients to consume a carbohydrate-rich diet as opposed to fully embracing the proposed diet. Lastly, this discordance in the percentage of patients failing dietary measures may be attributed to differences in definitions of glycaemic control, population characteristics and the population responses.
Study limitations and strengths
Limitations of the current study include its retrospective nature and small numbers of patients in the cohorts. The diagnostic criteria employed, although relevant at the time, are no longer applicable and may limit reproducibility of the study. Furthermore, comparison of certain variables between the two cohorts was limited. We did not have access to the earlier cohort's database and hence could not merge the insulin monotherapy group with the later cohorts for the purposes of analysis. In addition, the definitions of nephropathy and the MBG calculations were different. Different assays for HbA1c were used at the two time points, with an immunoassay (Roche Diagnostics, Germany) being performed on whole blood by the National Health Laboratory Service in the earlier cohort and point-of-care testing being employed in the later cohort, making comparison of HbA1c between the cohorts problematic. As the prevalence rate of anaemia in the later cohort was high (11%), decreased reliability of this test cannot be ruled out. Comparison of maternal and neonatal outcomes between cohorts was restricted to the variables obtained for the earlier cohort. This prevented us from exploring whether the lower GA at delivery in the recent cohort may have translated into more cases of prematurity. Various confounders for outcomes were either poorly reported, like BMI, or not at all, like HIV status, in one or both of the cohorts. Strengths of the study include the comparison of patients from the same clinic 10 years apart, diagnosed utilising the same test and criteria, where the only difference was the introduction of oral hypoglycaemic agents.
Conclusions
After the introduction of OHAs at the CHBAH gestational endocrine clinic, patients achieved similar levels of glycaemic control at delivery and showed similar outcomes compared with patients receiving insulin therapy. This is reassuring, particularly for low- and middle-income countries, where the OHAs are cheaper, more accessible, easier to use and eliminate the availability and storage issues associated with insulin therapy. Further prospective studies with adequate sample sizes are needed to confirm our findings and to determine the impact of OHA on pregnancy outcomes, both in the short and long term.
Declaration. This publication was part of the requirements for VN's PhD degree.
Acknowledgements. The South African Medical Research Council supported this study. SAN is supported by the DST-NRF Centre of Excellence in Human Development at the University of the Witwatersrand, Johannesburg. We thank Chris Hani Baragwanath Academic Hospital for access to the patient records.
Author contributions. All authors contributed to conceptualisation of the study. VN contributed to planning, data capturing and analysis, and manuscript writing and editing. LS, KK-G, NL and SAN contributed to planning, interpretation of data, and manuscript writing and editing. KRH contributed to manuscript writing and editing.
Funding. None.
Conflicts of interest. None.
References
1. Metzger BE, Gabbe SG, Persson B, et al.; International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010;33(3):676-682. https://doi.org/10.2337/dc09-1848 [ Links ]
2. Metzger BE, Lowe LP, Dyer AR, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med 2008;358(19):1991-2002. https://doi.org/10.1056/NEJMoa0707943 [ Links ]
3. Guariguata L, Linnenkamp U, Beagley J, et al. Global estimates of the prevalence of hyperglycaemia in pregnancy. Diabetes Res Clin Pract 2014;103(2):176-185. https://doi.org/10.1016/j.diabres.2013.11.003 [ Links ]
4. Jiwani A, Marseille E, Lohse N, et al. Gestational diabetes mellitus: Results from a survey of country prevalence and practices. J Matern Neonatal Med 2012;25(6):600-610. https://doi.org/10.3109/14767058.2011.587921 [ Links ]
5. Macaulay S, Ngobeni M, Dunger DB, et al. The prevalence of gestational diabetes mellitus amongst black South African women is a public health concern. Diabetes Res Clin Pract 2018;139:278-287. https://doi.org/10.1016/j.diabres.2018.03.012 [ Links ]
6. Adam S, Rheeder P. Screening for gestational diabetes mellitus in a South African population: Prevalence, comparison of diagnostic criteria and the role of risk factors. S Afr Med J 2017;107(6):523-527. https://doi.org/10.7196/SAMJ.2017.v107i6.12043 [ Links ]
7. Blumer I, Hadar E, Hadden DR, et al. Diabetes and pregnancy: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2013;98(11):4227-4249. https://doi.org/10.1210/jc.2013-2465 [ Links ]
8. Hod M, Kapur A, Sacks DA, et al. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care. Int J Gynecol Obstet 2015;131(Suppl 3):S173-S211. https://doi.org/10.1016/S0020-7292(15)30007-2 [ Links ]
9. National Institute for Health and Care Excellence. Diabetes in pregnancy: Management from preconception to the postnatal period: NICE guideline. 15 February 2015. http://www.nice.org.uk/guidance/ng3/resources/diabetes-in-pregnancy-management-from-preconception-to-the-postnatal-period-51038446021 (accessed 6 May 2019). [ Links ]
10. ACOG Releases. Updated ACOG guidance on gestational diabetes. 2017. https://www.obgproject.com/2017/06/25/acog-releases-updated-guidance-gestational-diabetes/ (accessed 2 May 2019). [ Links ]
11. Nicolaou V, Huddle KR. SEMDSA 2017 guidelines for the management of type 2 diabetes mellitus. J Endocr Metab Diabetes S Afr 2017;22(1):S99-S103. http://www.jemdsa.co.za/index.php/JEMDSA/article/view/647 (accessed 8 January 2020). [ Links ]
12. Riddle MC, Bakris G, Blonde L, et al.; American Diabetes Association. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes - 2018. Diabetes Care 2018;41(Suppl 1):S13-S27. https://doi.org/10.2337/dc18-S002 [ Links ]
13. Poolsup N, Suksomboon N, Amin M. Efficacy and safety of oral antidiabetic drugs in comparison to insulin in treating gestational diabetes mellitus: A meta-analysis. PLoS One 2014;9(10):e109985. https://doi.org/10.1371/journal.pone.0109985 [ Links ]
14. Balsells M, Garcia-Patterson A, Sola I, et al. Glibenclamide, metformin, and insulin for the treatment of gestational diabetes: A systematic review and meta-analysis. BMJ 2015;350:h102. https://doi.org/10.1136/bmj.h102 [ Links ]
15. Ekpebegh CO, Coetzee EJ, van der Merwe L, et al. A 10-year retrospective analysis of pregnancy outcome in pregestational type 2 diabetes: Comparison of insulin and oral glucose-lowering agents. Diabet Med 2007;24(3):253-258. https://doi.org/10.1111/j.1464-5491.2007.02053.x [ Links ]
16. Coetzee EJ, Jackson WP. Diabetes newly diagnosed during pregnancy: A 4-year study at Groote Schuur Hospital. S Afr Med J 1979;56(12):467-475. [ Links ]
17. Huddle KR. Audit of the outcome of pregnancy in diabetic women in Soweto, South Africa, 1992 - 2002. S Afr Med J 2005;95(10):789-794. [ Links ]
18. Amod A. The 2012 SEMDSA guideline for the management of type 2 diabetes. J Endocrinol Metab Diabetes S Afr 2012;17(1):61-62. https://doi.org/10.1080/22201009.2012.10872276 [ Links ]
19. Hasan JA, Karim N, Sheikh Z. Metformin prevents macrosomia and neonatal morbidity in gestational diabetes. Pakistan J Med Sci 2012;28(3):384-389. [ Links ]
20. Balani J, Hyer S, Johnson A. Pregnancy outcomes after metformin treatment for gestational diabetes: A case-control study. Obstet Med 2012;5(2):78-82. https://doi.org/10.1258/om.2012.110092 [ Links ]
21. Pattinson R, Rhoda N. Saving Babies 2012 - 2013: Ninth Report on Perinatal Care in South Africa. Pretoria: Tshepesa Press. 2014. www.ppip.co.za. (accessed 19 October 2018). [ Links ]
22. Van Zyl H, Levitt NS. Pregnancy outcome in patients attending Groote Schuur Hospital with pregestational and gestational diabetes. BJOG 2017;124(9):153. https://doi.org/10.1111/1471-0528.9_14572 [ Links ]
23. McLarty DG, Pollitt C, Swai ABM. Diabetes in Africa. Diabet Med 1990;7(8):670-684. https://doi.org/10.1111/j.1464-5491.1990.tb01470.x [ Links ]
24. Cois A, Day C. Obesity trends and risk factors in the South African adult population. BMC Obes 2015;2(1):1-10. https://doi.org/10.1186/s40608-015-0072-2 [ Links ]
 Correspondence:
Correspondence:
VNicolaou
docvic9@gmail.com
Accepted 1 July 2019


{kind=link}
{kind=link}