










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 n.1 Pretoria Jan. 2020
http://dx.doi.org/10.7196/samj.2020.v110i1.14051
RESEARCH
A multicentre prospective observational study of the prevalence of preoperative anaemia and iron deficiency in adult elective surgical patients in hospitals in Western Cape Province, South Africa
W S ConradieI; T Biesman-SimonsI; F RoodtII; M NejthardtIII; J DavidsIV; T PretoriusV; G DaviesVI; E CloeteVII, VIII; Z FullertonIX; J RoosX; M FlintXI; J L SwanevelderXII; R A DyerXIII; B M BiccardXIV
IMB ChB, DA (SA); Department of Anaesthesia and Perioperative Medicine, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
IIMB ChB, FCA (SA); Department of Anaesthesiology, George Regional Hospital, Western Cape Province, South Africa
IIIBSc Hons (Physiology), MB BCh, DA (SA), FCA (SA); Department of Anaesthesia and Perioperative Medicine, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
IVMB ChB, DA (SA), MMed, FCA (SA); Department of Anaesthesiology, George Regional Hospital, Western Cape Province, South Africa
IXMB ChB, DA (SA), FCA (SA), MMed; Department of Anaesthesiology, Victoria Hospital, Cape Town, South Africa
VMB ChB, DA (SA), FCA (SA), MMed; Department of Anaesthesiology, Paarl Provincial Hospital, Western Cape Province, South Africa
VIMB ChB, FCA (SA); Department of Anaesthesiology, Paarl Provincial Hospital, Western Cape Province, South Africa
VIIMB ChB, DA (SA), FCA (SA); Department of Anaesthesia and Perioperative Medicine, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
VIIIMB ChB, DA (SA), FCA (SA); Department of Anaesthesiology, New Somerset Hospital, Cape Town, South Africa
XMB ChB, DA (SA), MMed, FCA (SA); Department of Anaesthesiology, Mitchell's Plain Hospital, Cape Town, South Africa
XIBSc HSc, MSc (Medical Physiology), PhD; Department of Anaesthesia and Perioperative Medicine, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
XIIMB ChB, DA (SA), FCA (SA), MMed, FRCA; Department of Anaesthesia and Perioperative Medicine, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
XIIIMB ChB, FCA (SA), PhD; Department of Anaesthesia and Perioperative Medicine, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
XIVMB ChB, MMedSci, FCA (SA), PhD; Department of Anaesthesia and Perioperative Medicine, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND. Preoperative anaemia has been shown to be an independent risk factor for postoperative morbidity and mortality. Iron deficiency is the leading cause of anaemia globally. There are limited data describing the burden of perioperative anaemia and the relative contribution of iron deficiency in South Africa (SA).
OBJECTIVES. To determine the prevalence and severity of preoperative anaemia in adults presenting for elective surgery in Western Cape Province, SA, and to investigate the contribution of iron deficiency as a cause of the anaemia. For this purpose, an investigative protocol from a recent consensus statement on the management of perioperative anaemia was applied.
METHODS. We performed a prospective, observational study in adult patients presenting for elective non-cardiac, non-obstetric surgery over a 5-day period at six Western Cape government-funded hospitals. The World Health Organization patient classification was applied, and patients with anaemia were investigated for iron deficiency.
RESULTS. The prevalence of preoperative anaemia was 28% (105/375; 95% confidence interval (CI) 23.5 - 32.5); 55/105 patients (52%) had moderate and 11/105 (11%) severe anaemia. Iron deficiency was the cause of anaemia in 37% (32/87; 95% CI 26.6 - 46.9), but only 9% of iron-deficient patients received iron supplementation prior to surgery.
CONCLUSIONS. Preoperative anaemia was common in this study, and more than half of the affected patients had moderate to severe anaemia. Iron deficiency was responsible for almost 40% of cases. Iron supplementation was under-utilised in the preoperative period as a means of increasing haemoglobin. The introduction of system-wide policies would empower perioperative physicians to mitigate the risk associated with preoperative anaemia in the Western Cape.
Anaemia is a common condition, affecting almost a third of the global population, and is the most frequently observed impairment worldwide according to the Global Burden of Disease study.[1] This high prevalence has consequences for surgical patients. There is a growing body of literature carefully detailing the impact of preoperative anaemia on postoperative outcomes. Anaemia is independently associated with increased in-hospital mortality, allogeneic blood transfusions, length of hospital stay, intensive care admissions, surgical site infections and readmission to hospital. [2-6] Preoperative anaemia is inextricably linked to blood product utilisation in the surgical period and has become one of the three pillars of patient blood management (PBM) programmes, where the goal is to curb unnecessary blood product use and improve outcomes.[7-9] Despite increased awareness of its negative impact, preoperative anaemia remains a common finding in patients presenting for surgery, with a reported prevalence as high as 75% for certain patient groups.[2,10]
Early diagnosis and management of the underlying cause of anaemia is necessary to mitigate the associated perioperative risk. Iron deficiency is the leading cause of anaemia in the general population, accounting for approximately half of all cases worldwide,[1] and up to 62% of preoperative anaemia.[11]
The South African Surgical Outcomes Study (SASOS) showed that the national surgical population carries a higher perioperative risk, when matched for age and comorbidities, compared with high-income countries.[12] The overall prevalence of preoperative anaemia in the SASOS cohort was 47.8%, and anaemia was independently associated with in-hospital mortality and intensive care admissions.[13]
However, the proportional contribution of specific causes of anaemia in the SASOS cohort was unknown, and there remains a paucity of literature on this topic in surgical patients.
Objectives
To determine the prevalence and severity of preoperative anaemia and iron deficiency anaemia (IDA) in patients presenting for elective surgery in Western Cape Province, South Africa (SA). For the investigation of IDA, the recommendations of a recent international consensus statement on the perioperative management of anaemia and iron deficiency were followed.[3]
Methods
We performed a multicentre, prospective, observational cohort study of all adult elective surgical patients over the period of 1 working week, 16 - 20 October 2017, in six public sector (one tertiary and five secondary) government-funded hospitals in the Western Cape. Groote Schuur, Paarl, Victoria, Mitchell's Plain, George and New Somerset hospitals participated. The study was approved by the Human Research Ethics Committee of the Faculty of Health Sciences of the University of Cape Town (ref. no. HREC 385/2017) and registered on clinicaltrials.gov (ref. no. NCT03318055). The Western Cape Department of Health as well as the individual institutions also approved the study (provincial approval ref. no. WC_201709_018).
Inclusion criteria were all adult (>18 years) patients presenting for elective non-obstetric, non-cardiac surgery. Emergency and paediatric surgery and radiological procedures were further exclusions. Eligible patients were informed about the study during their routine preoperative anaesthesia assessment. All patients provided written informed consent and received a handout with additional information regarding anaemia, and a referral letter to their primary healthcare facility for further workup and management should the condition be identified. Baseline demographic and clinical data were recorded on a paper case report form for all participating patients. This information included age, gender, ethnicity, American Society of Anesthesiology (ASA) status, weight, height, known comorbidities and medication, smoking and functional status. The type of surgery was classified as major or non-major. Iron supplementation was specifically documented. Preoperative haemoglobin (Hb) levels, mean corpuscular volume, serum ferritin level, transferrin saturation (TSAT) and serum creatinine level were recorded if available. In the small proportion of patients in whom the preoperative Hb was unavailable, a point-of-care Hb measurement was done prior to arrival in theatre. A single reading was obtained using the HemoCue Hb 201+ system (HemoCue, SA), which if in the range of anaemia indicated a full blood count. Patients were only classified as anaemic and investigated for iron deficiency on the basis of the laboratory result.
All captured information was deidentified, anonymised and assigned a unique study number during the transcription process using Research Electronic Data Capture (REDCap) tools provided by Safe Surgery South Africa. Patients were classified as anaemic or not anaemic according to the World Health Organization (WHO) classification (Hb <13 g/dL for males and <12 g/dL for non-pregnant females), and the severity of anaemia was defined as mild (11 - 12.9 g/dL), moderate (8 - 10.9 g/dL) or severe (<8 g/dL).[14]
Anaemic patients were investigated for iron deficiency. The specimens were obtained in theatre, prior to induction of anaesthesia. Blood samples were processed and analysed by the National Health Laboratory Service and deidentified with a unique patient study number. Postoperatively, laboratory results were followed up by the investigators, and anaemic patients were classified as having IDA or anaemia without iron deficiency. Serum ferritin is regarded as the investigation of choice for the diagnosis of IDA.[15] However, it is an acute-phase protein and can be elevated in the presence of inflammation and other conditions, which makes its usefulness as a single investigation, when elevated, of limited value.[16] The combination of serum ferritin and TSAT is the most widely recognised approach for the diagnosis of IDA in the perioperative setting. The diagnosis was made if serum ferritin was <30 ug/L, or if it was 30 -100 ug/L in combination with TSAT <20%.[3,11,17]
Based on previous studies with a similar design, and known numbers of surgical cases at participating hospitals, we expected to recruit 500 patients.[18] Patients who had no Hb recorded were excluded from our study. Patients with missing iron study results were excluded from calculation of IDA, but included in calculations of the prevalence of anaemia.
Statistical analysis
Continuous variables were described as means (standard deviations (SDs)) if normally distributed. Comparisons of continuous variables were performed using Fisher's exact test or Pearson's x2 test, as appropriate. All p-values reported were two-sided, and p<0.05 was considered statistically significant. A sample size of ~500 patients and a prevalence of anaemia of ~30% would allow determination of the true prevalence with a 95% confidence interval (CI) of ±4.0%, i.e. 26.0 - 34.0. The Statistical Package for the Social Sciences (SPSS) version 24 (SPSS Inc., USA) was used for data analysis.
Results
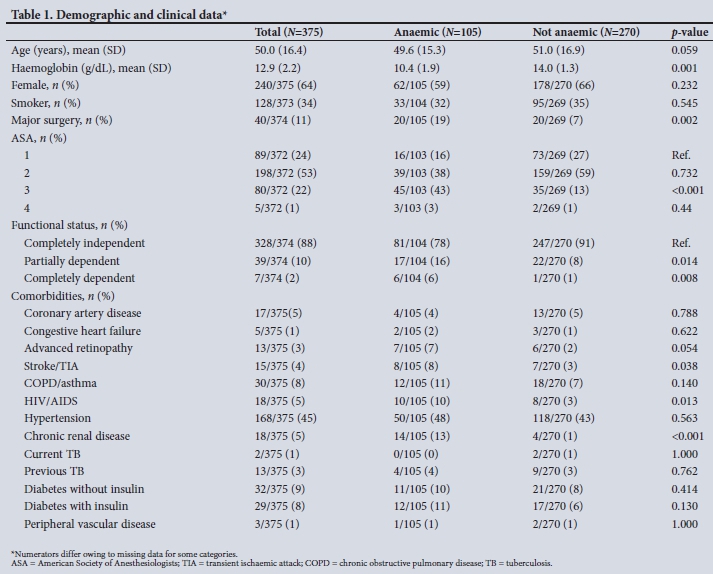
The study flow diagram is shown in Fig. 1, and baseline demographic data are displayed in Table 1. The primary outcome, the prevalence of preoperative anaemia, was 28% (105/375; 95% CI 23.5 - 32.5) with a mean (SD) Hb of 10.4 (1.9). Anaemia was most prevalent in the age group 40 - 49 years (mean 50%), with a higher prevalence in males (32%) than females (26%). According to the WHO classification, 39/105 (37%) had mild, 55/105 (52%) moderate and 11/105 (11%) severe anaemia. Higher rates of preoperative anaemia were found in patients who had an ASA score of 3 and 4, chronic renal disease and HIV/AIDS. Intestinal, peripheral vascular and other abdominal surgery had the highest incidences of anaemia (66%, 62% and 40%, respectively). Patients undergoing major surgery were more likely to be anaemic than those undergoing non-major surgery.

The iron status of all anaemic patients was investigated. Owing to a prolonged time from collection to processing, 18 specimens were unsuitable for evaluation and therefore excluded. In total, 87 suitable specimens were investigated. Of these, 37% (32/87; 95% CI 26.6 -46.9) were classified as IDA. Subgroup analysis showed that 22% (7/32) of patients who had IDA were male and 78.1% (25/32) female (p=0.008). Of the patients with IDA, 3 were receiving oral iron supplementation preoperatively and 6 were on folate supplements. In the entire cohort, 12 patients received blood transfusions prior to their surgery. Of these, 10 were anaemic on admission, 3 of whom had IDA. There were 3 patients who did not undergo surgery for reasons other than anaemia.
Discussion
The results of the study showed that preoperative anaemia was common, with a prevalence of 28% in patients scheduled for elective surgery in the participating Western Cape government hospitals. This figure was lower than in elective surgery in the SASOS study population (38.2%).[13] An important finding in the present study was that the majority of patients with anaemia were in the moderate category. Increased severity is linked to worse outcomes. In-hospital mortality was four times higher in patients in the SASOS cohort with moderate and severe anaemia than in those with mild anaemia.[5,13,19]
In elective surgery, iron deficiency was the cause of preoperative anaemia in 37% of patients in our study. The higher proportion of women with IDA was in keeping with a recent study conducted in the healthy Western Cape population which showed that 11% of men had iron deficiency compared with almost 50% of women.[20] However, only 9% of patients with IDA received iron supplementation. There is therefore a large population that could benefit from preoperative iron therapy in order to replenish iron stores and increase the Hb prior to surgery. The cause of the anaemia in the remaining 63% of patients in our study was not investigated. However, in clinical practice a structured treatment algorithm should be followed to identify and treat these causes.[21]
Most guidelines and literature focus on optimising patients prior to major surgery.[3] In our study, major surgery was associated with an increased prevalence of preoperative anaemia; however, a substantial proportion of patients scheduled for non-major surgery were also anaemic, and would benefit from further investigation to identify the cause. HIV/AIDS and chronic kidney disease were associated with significant increases in the prevalence of preoperative anaemia, highlighting the need for investigation of the cause of anaemia in these groups.
There are many barriers preventing adequate correction of preoperative anaemia.[22] Guidelines aimed at managing preoperative anaemia and preventing allogeneic blood transfusions have been successfully implemented in many countries, particularly as part of PBM programmes. Where these programmes have been established, improvements in perioperative outcomes as well as significant economic benefits have been demonstrated.[23] The Western Cape healthcare system could benefit from the introduction of multidisciplinary anaemia clinics, with a view to increasing red cell mass in the preoperative period.
Study strengths and limitations
The strength of our study was the prospective, multicentre data collection. We also included major as well as non-major surgery. The criteria for iron deficiency were relatively strict, as there may have been patients with concomitant inflammatory disease or chronic kidney disease, whose ferritin level might be >100 ug/L but who could still have concomitant iron deficiency. The prevalence of iron deficiency noted should therefore be seen as a minimum estimate.
However, there were some weaknesses in our research approach. Our data reflect only a 5-day study period, and fewer patients were recruited than the initially anticipated 500. This limitation resulted in a slightly wider CI for the estimate than targeted in the sample size calculation. In addition, cancer was not listed as a comorbidity, so no conclusions can be drawn on the contribution of these patients to the prevalence of perioperative anaemia. Furthermore, the prevalence of IDA could have been influenced by the 18 specimens that were excluded due to processing errors.
Conclusions
This study provides a strong indication of the current prevalence of preoperative anaemia and iron deficiency in the elective surgical population in the Western Cape. Preoperative anaemia is common, and the frequency of moderate anaemia is concerning. The condition is correctable, and failure to consider or attempt optimisation for patients undergoing major surgery is inadmissible. Iron supplementation in the preoperative period was under-utilised. Improvement in the management of preoperative anaemia would benefit patients, but requires timeous recognition of the problem and education of role-players, as well as implementation of institutional and system-wide policies. Such protocols would empower perioperative physicians to mitigate risk in patients undergoing elective surgery.
Declaration. This study formed part of the requirements of WSC's MMed (Anaesth) degree.
Acknowledgements. The investigators thank the various hospitals for their participation and the members of the anaesthesia departments for collecting and capturing data at these institutions.
Author contributions. WSC: overall conception and study design, data collection at Groote Schuur Hospital (GSH), interpretation, drafting of the manuscript. TB-S: overall conception and study design, data collection at GSH, interpretation. FR: overall conception and study design, analysis and interpretation. MN: overall conception and study design, analysis. JD, TP, GD, EC, ZF, JR, MF: data acquisition at George, Paarl, New Somerset, Victoria and Mitchell's Plain hospitals and GSH, respectively. JLS: overall conception and study design. RAD: overall conception and study design, interpretation. BMB: overall conception and study design, analysis and interpretation of results. All authors were involved in critical revision and approval of the final manuscript.
Funding. The study was funded by the Jan Pretorius Fund of the South African Society of Anaesthetists. Resources from the Department of Anaesthesia and Perioperative Medicine of the University of Cape Town were also made available for the conduction of the study.
Conflicts of interest. None.
References
1. Vos T, Allen C, Arora M, et al Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990 - 2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388(10053):1545-1602. https://doi.org/10.1016/S0140-6736(16)31678-6 [ Links ]
2. Spahn DR. Anemia and patient blood management in hip and knee surgery. Anesthesiology 2010;113(2):482-495. https://doi.org/10.1097/ALN.0b013e3181e08e97 [ Links ]
3. Munoz M, Acheson AG, Auerbach M, et al. International consensus statement on the peri-operative management of anaemia and iron deficiency. Anaesthesia 2017;72(2):233-247. https://doi.org/10.1111/anae.13773 [ Links ]
4. Munoz M, Gómez-Ramírez S, Campos A, Ruiz J, Liumbruno GM. Pre-operative anaemia: Prevalence, consequences and approaches to management. Blood Transfus 2015;13(3):370-379. https://doi.org/10.2450/2015.0014-15 [ Links ]
5. Musallam KM, Tamim HM, Richards T, et al. Preoperative anaemia and postoperative outcomes in non-cardiac surgery: A retrospective cohort study. Lancet 2011;378(9800):1396-1407. https://doi.org/10.1016/S0140-6736(11)61381-0 [ Links ]
6. Beattie WS, Karkouti K, Wijeysundera DN, Tait G. Risk associated with preoperative anemia in noncardiac surgery. Anesthesiology 2009;110(3):574-581. https://doi.org/10.1097/ALN.0b013e31819878d3 [ Links ]
7. Gombotz H, Rehak PH, Shander A, Hofmann A. Blood use in elective surgery: The Austrian benchmark study. Transfusion 2007;47(8):1468-1480. https://doi.org/10.1111/j.1537-2995.2007.01286.x [ Links ]
8. Gombotz H, Rehak PH, Shander A, Hofmann A. The second Austrian benchmark study for blood use in elective surgery: Results and practice change. Transfusion 2014;54(10pt2):2646-2657. https://doi.org/10.1111/trf.12687 [ Links ]
9. Jans O, J0rgensen C, Kehlet H, Johansson PI. Role of preoperative anemia for risk of transfusion and postoperative morbidity in fast-track hip and knee arthroplasty. Transfusion 2014;54(3):717-726. https://doi.org/10.1111/trf.12332 [ Links ]
10. Goodnough LT, Shander A, Spivak JL, et al. Detection, evaluation, and management of anemia in the elective surgical patient. Anesth Analg 2005;101(6):1858-1861. https://doi.org/10.1097/01.sa.0000234704.07366.b2 [ Links ]
11. Munoz M, Laso-Morales MJ, Gómez-Ramírez S, Cadellas M, Núâez-Matas MJ, García-Erce JA. Pre-operative haemoglobin levels and iron status in a large multicentre cohort of patients undergoing major elective surgery. Anaesthesia 2017;72(7):826-834. https://doi.org/10.1111/anae.13840 [ Links ]
12. Biccard BM, Madiba TE. The South African Surgical Outcomes Study: A 7-day prospective observational cohort study. S Afr Med J 2015;105(6):465-475. https://doi.org/10.7196/SAMJ.9435 [ Links ]
13. Marsicano D, Hauser N, Roodt F, et al. Preoperative anaemia and clinical outcomes in the South African Surgical Outcomes Study. S Afr Med J 2018;108(10):839-846. https://doi.org/10.7196/SAMJ.2018.v108i10.13148 [ Links ]
14. World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Geneva: Vitamin and Mineral Nutrition Information System, WHO, 2011. http://www.who.int/vmnis/indicators/haemoglobin/en/ (accessed 29 November 2017). [ Links ]
15. DeLoughery TG. Iron deficiency anemia. Med Clin North Am 2017;101(2):319-332. https://doi.org/10.1016/j.mcna.2016.09.004 [ Links ]
16. Goddard AF, James MW, McIntyre AS, Scott BB. Guidelines for the management of iron deficiency anaemia. Gut 2011;60(10):1309-1316. https://doi.org/10.1136/gut.2010.228874 [ Links ]
17. Thomas DW, Hinchliffe RF, Briggs C, Macdougall IC, Littlewood T, Cavill I. Guideline for the laboratory diagnosis of functional iron deficiency. Br J Haematol 2013;161(5):639-648. https://doi.org/10.1111/bjh.12311 [ Links ]
18. Crowther M, van der Spuy K, Roodt F, et al. The relationship between pre-operative hypertension and intra-operative haemodynamic changes known to be associated with postoperative morbidity. Anaesthesia 2018;73(7):812-818. https://doi.org/10.1111/anae.14239 [ Links ]
19. Baron DM, Hochrieser H, Posch M, et al. Preoperative anaemia is associated with poor clinical outcome in non-cardiac surgery patients. Br J Anaesth 2014;113(3):416-423. https://doi.org/10.1093/bja/aeu098 [ Links ]
20. Phatlhane DV, Zemlin AE, Matsha TE, et al. The iron status of a healthy South African adult population. Clin Chim Acta 2016;460:240-245. https://doi.org/10.1016/j.cca.2016.06.019 [ Links ]
21. Munting KE, Klein AA. Optimisation of pre-operative anaemia in patients before elective major surgery - why, who, when and how? Anaesthesia 2019;74(S1):49-57. https://doi.org/10.1111/anae.14466 [ Links ]
22. Munoz M, Gómez-Ramírez S, Kozek-Langeneker S, et al. 'Fit to fly': Overcoming barriers to preoperative haemoglobin optimization in surgical patients. Br J Anaesth 2015;115(1):15-24. https://doi.org/10.1093/bja/aev165 [ Links ]
23. Leahy MF, Hofmann A, Towler S, et al. Improved outcomes and reduced costs associated with a health-system-wide patient blood management program: A retrospective observational study in four major adult tertiary-care hospitals. Transfusion 2017;57(6):1347-1358. https://doi.org/10.1111/trf.14006 [ Links ]
 Correspondence:
Correspondence:
W S Conradie
wsc238@gmail.com
Accepted 29 July 2019


{kind=link}