










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 no.1 Pretoria Jan. 2020
http://dx.doi.org/10.7196/samj.2020.v110i1.13954
RESEARCH
Dose-related adverse events in South African patients prescribed clofazimine for drug-resistant tuberculosis
N MisraI; N PadayatchiII; P NaidooIII
IBPharm, MMedSc (Clinical Pharmacology); Discipline of Pharmaceutical Sciences, School of Health Sciences, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IIMB ChB, PhD; HIV-TB Pathogenesis and Treatment Research Unit, Centre for the AIDS Programme of Research in South Africa (CAPRISA), South African Medical Research Council, Durban, South Africa
IIIBPharm, MMedSc (Pharmacology), PhD; Discipline of Pharmaceutical Sciences, School of Health Sciences, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND. Optimal drug levels and minimal toxicity are critical factors in improving treatment outcomes for patients prescribed new and repurposed medicine for drug-resistant (DR) tuberculosis (TB). The optimal dose and dose-related safety of clofazimine (CFZ), a repurposed medicine for DR TB, in the South African (SA) population are unknown.
OBJECTIVES. To report on dose-related adverse events in patients receiving CFZ plus a background regimen for DR TB.
METHODS. In a retrospective review of patient folders from 2012 to 2014, adverse events documented for patients receiving high- (>200 mg) and low-dose (100 mg) CFZ in a centralised DR TB hospital in KwaZulu-Natal Province, SA, were investigated for an association between dose-weight interactions and adverse events.
RESULTS. Of 600 patients included, 78.7% (n=472) weighed >50 kg. Of these, 17.4% (n=82) received 100 mg CFZ and 82.6% (n=390) received >200 mg. Of 128 patients (21.3%) who weighed <50 kg, 68.0% (n=87) received 100 mg CFZ and 32.0% (n=41) received >200 mg. Of 463 patients (77.2%) who were HIV-positive, 94.0% were on antiretrovirals. There was no difference between the dose-weight cohorts in the background regimen given in addition to high- or low-dose CFZ. The frequency and types of adverse events observed were similar to the published literature. When analysed per dose-weight cohort, patients weighing <50 kg and receiving high-dose CFZ (>200 mg) had a 2.6 times higher risk of any adverse event (adjusted odds ratio (aOR) 2.57; 95% confidence interval (CI) 1.02 - 6.05; p=0.05: reference category <50 kg and 100 mg). Patients weighing <50 kg and receiving high-dose CFZ had a 3.3 times higher risk of gastrointestinal adverse events than patients weighing <50 kg and receiving 100 mg CFZ (aOR 3.30; 95% CI 1.51 - 7.19; p=0.003). A high risk of chest pain was observed in patients receiving high- and low-dose CFZ, irrespective of weight. Patients weighing <50 kg receiving high-dose CFZ had a slightly higher risk of adverse events related to the skin (aOR 1.2; 95% CI 0.55 - 2.62; p=0.7) There were no documented reports of the CFZ dose being reduced or the drug being stopped due to adverse events in the sample population.
CONCLUSIONS. There is an association between dose-weight interaction and adverse events. The odds of any adverse event occurring were higher when low-weight patients (<50 kg) received high-dose CFZ (>200 mg). Gastrointestinal and skin-related adverse events were more common when high-dose CFZ was used in patients weighing <50 kg. Chest pain was reported in patients receiving high- and low-dose CFZ, irrespective of weight, and may be a symptom of cardiac toxicity. Plasma concentrations of CFZ may be affected by drug-drug interactions, so active drug safety monitoring including electrocardiograms is recommended routinely when CFZ is part of the regimen.
Worldwide, tuberculosis (TB) remains one of the top 10 causes of death, with drug-resistant (DR) TB continuing to be a public health crisis.[1] Despite huge investments in combating this highly infectious disease, the 2019 Global Tuberculosis Report[1] indicates that new cases of DR TB are being reported at an alarming rate, with low treatment success rates, high loss to treatment follow-up and high death rates. Bedaquiline (BDQ) and delaminid, two new medicines developed in the past five decades, and repurposed medicines such as linezolid (LZD) and clofazimine (CFZ), form the backbone of new regimens aimed at improving treatment outcomes.[2-4] South Africa (SA) has made bold decisions to roll out new and repurposed medicines as well as a novel short-course injection-free regimen that aims to improve patient outcomes.[5] In order to improve access to the new and repurposed medicines, registration with regulatory authorities has been fast-tracked despite low-quality safety and efficacy data generated under research conditions or compassionate-use models.[6,7] The World Health Organization (WHO) recommends active drug safety monitoring and management as new and repurposed medicines are rolled out.[8] The focus of monitoring is on adverse events, defined as any untoward medical occurrence that may present in a TB patient during treatment with a pharmaceutical product, but does not necessarily have a causal relationship with this treatment.[8]
Recent WHO updates on the clinical management of DR TB have reclassified CFZ from a group 5 medicine with unclear safety and efficacy to a core medicine as part of a DR TB treatment regimen.[9-12] SA is currently reviewing its guidelines to include CFZ as a core medicine to treat multidrug-resistant TB, despite CFZ not being registered or included in published SA standard treatment guidelines and essential medicines lists.[13,14] Special authorisation is obtained from the South African Health Products Regulatory Authority to import CFZ into SA for use in DR TB.[15,16] Evidence of safety and the optimal effective dose of CFZ in the SA population are lacking to inform registration.
In order to ensure the benefits of including new and repurposed medicine in the DR TB treatment regimen, the optimal dose must be established, with a strong focus on safety.[8] The optimal (effective and safe) dose of CFZ is still under debate, with most articles citing this as an area for further research.[9,12,17-19] The dose of CFZ prescribed across studies ranges from 50 mg to 300 mg, with many studies not reporting the dose used. All systematic reviews concluded that the optimal dose of CFZ requires further investigation.[18,20] Population-based pharmacokinetics must be considered when making decisions on the optimal dose of CFZ to include in the SA DR TB guidelines.
The unique pharmacokinetic properties of CFZ have been widely documented, with many studies reporting an unclear mechanism of action, a lag in absorption, low serum concentrations even in the setting of adequate tissue concentrations, a long terminal half-life, and interpatient variability in absorption, distribution and elimination, which have implications for the treatment regimen.[21-25] Schaad-Lanyi et al.[24] suggested that in order to avoid the long-lasting accumulation towards steady state, higher daily loading doses are recommended at the beginning of therapy, followed by a daily maintenance dose. A recent study on the impact of CFZ dosing on treatment shortening in a mouse model suggests that CFZ at low exposures may have negative impacts on treatment outcomes, an effect that was evident only after the first 3 months of treatment.[26] Previous WHO guidance documents recommended weight-based dosing of CFZ, which was adopted globally.[9-12] The current published SA treatment guidelines for DR TB include CFZ at high doses (200 mg in patients weighing <50 kg and 300 mg in those weighing >50 kg) for long periods of time (18 - 20 months) in pre-extensively drug-resistant and extensively drug-resistant TB.[27] This decision was made despite there being no conclusive evidence on the safety and efficacy of CFZ at high doses for long periods of time in the SA population. Concerns and debate regarding the overlapping toxicity associated with the use of CFZ, BDQ and fluoroquinolones have emerged, and it is important to provide evidence of the safety of CFZ at different doses.[7,28-30] No studies have reported on the impact of different doses of CFZ on safety and efficacy. Weighing the risk-benefit of varying doses of CFZ is important to ensure that the dose prescribed is able to achieve minimum inhibitory concentrations, thus preventing further resistance from emerging, and is safe.
Objectives
To determine the association between the dose of CFZ prescribed at different weight bands and the chance of any adverse event occurring in the SA population.
Methods
This was a retrospective cohort study of adult patients in KwaZulu-Natal Province, SA, treated between 2012 and 2014 with a CFZ-containing regimen for DR TB at doses ranging from low (100 mg) to high (>200 mg). Patients were selected from the pharmacy database, in which all patients initiated on a CFZ-containing regimen were recorded. The database was reviewed for duplicate entries, and adult patients aged >18 years with a traceable DR TB number that enabled retrieval of their clinical folder were selected. Patients who met the study inclusion criteria of age >18 years, bacteriologically confirmed rifampicin-resistant TB, and availability of a clinical folder with treatment outcomes and dose of CFZ recorded were selected. Of the 1 018 patients in the pharmacy database, 600 met the inclusion criteria and were included in the study.
Data were extracted using manual data collection forms. In addition to reports of adverse events documented in the clinical notes, information on the starting dose of CFZ, demographics, HIV status and antiretroviral therapy, previous TB history, drug exposure, baseline tests, drug resistance patterns, background regimen and treatment outcomes at 24 months was collected. Missing information was sourced from the National Health Laboratory Service database, where applicable. The prescription charts were reviewed for starting dose of CFZ as well as any reduction in dose or stoppage of the drug. The clinical notes were scrutinised for any reports of adverse events experienced. Blood results were checked to assess whether there were objective data available to verify the clinical notes made by the doctor. Electrocardiograms (ECGs) were reviewed, and in the absence of objective data, chest pain was used as a surrogate marker of a possible cardiac event.
The results of routine blood tests that should have been done were reviewed to assess whether kidney function, liver function or the blood system were affected following the start of treatment with CFZ. ECG results were sought if available to confirm cardiac events.
The frequency and types of adverse events observed in patients receiving 100 mg and >200 mg CFZ were compared. Multivariate logistic regression analysis compared the risk of any adverse events in each cohort, taking into account possible confounders that could have contributed to the adverse event. An adverse event was defined as a documented side-effect in the patient's clinical folder, irrespective of grading or intervention that affected a body system in a negative way.
Statistical analysis
Data were captured into an Excel 2010 spreadsheet (Microsoft Corp., USA). Data quality was ensured by double entry using research assistants during the data extraction process, with any discordances that were identified resolved through verification with the original paper records. The validated database was analysed using Stata version 13.0 (StataCorp, USA). Patients were stratified into two groups: those receiving 100 mg CFZ (low dose) and those receiving >200 mg (high dose). Logistic regression analysis was used to assess the effect of risk factors on adverse events experienced by patients. Univariate and multivariate statistics, 95% confidence intervals (CIs) and p-values were used where appropriate to analyse the data. Statistical significance was set at p<0.05.
Ethical considerations
Ethics approval to conduct the study was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee (ref. no. BE466/14). The study was also approved by the KwaZulu-Natal Health Research Unit (ref. no. KZ 2015RP43_384).
Results
A total of 600 patients met the inclusion criteria and were included in the study population. The demographic and clinical characteristics of patients in each dose cohort are indicated in Table 1.
The number of medicines, including CFZ, used in the treatment regimens ranged from 5 to 11. The majority of the patients (n=277, 46.2%) received a combination of 8 medicines including CFZ as part of their DR TB treatment regimen, 249 (41.5%) received 7 medicines, 30 (5.0%) received 9 medicines, 11 (1.8%) received 10 medicines and 8 (1.3%) received 11 medicines. Medicines included in the background regimen with CFZ were pyrazinamide (99.5% of patients), fluoroquinolones (moxifloxacin or levofloxacin) (99.0%), ethionamide (98.2%), ethambutol (98.5%), terizidone
(97.7%), aminoglycosides (kanamycin or capreomycin) (95.2%), para-aminosalicylic acid (48.5%), isoniazid (17.2%), BDQ (6.0%) and LZD (3.2%). There was no difference between the background regimens prescribed for patients receiving high- and low-dose CFZ.
Of the patients, 400 (66.7%) had an adverse event documented in the clinical folder (Table 2). The majority of documented adverse events occurred in patients weighing <50 kg and receiving >200 mg CFZ, as documented in Table 2. Adverse events recorded in the clinical folders were categorised according to body system. Documented adverse events affected the muscular system, gastrointestinal tract, eyes, skin, central nervous system, ears, feet, kidneys, heart and liver.
Table 3 depicts the frequency of adverse events per body system in patients at different weight bands (<50 kg or >50 kg) who received 100 mg or >200 mg CFZ. The most common adverse events recorded related to the gastrointestinal tract (n=238, 39.67%), followed by chest pain as a surrogate marker of a cardiac event (n=136, 22.7%) and skin-related adverse events (n=107, 17.8%).
Weakness, loss of appetite, coughing of blood and dyspnoea were recorded and viewed as symptoms of DR TB and not classified as an adverse event caused by a medicine.
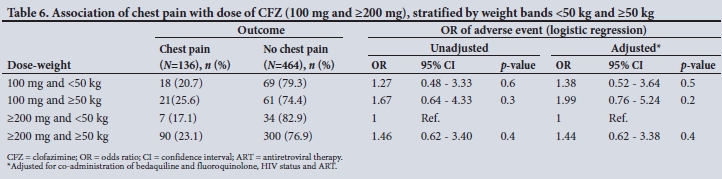
Multivariate logistic regression analysis was used to assess the risk of any adverse event occurring at different dose-weight categories. The logistics regression model was also used to assess the risk of the top three reported adverse events documented (gastrointestinal adverse events, cardiac events and adverse events related to the skin). Table 4 shows the association between dose of CFZ prescribed per weight band and the odds of an adverse event occurring. Table 5 shows the multivariate analysis related to the gastrointestinal tract, Table 6 the multivariate analysis related to chest pain and Table 7 the association between dose and weight and the risk of skin-related adverse events.
Patients weighing <50 kg who received high-dose CFZ (>200 mg) were at an increased risk of experiencing any adverse event. It was observed that patients in this weight-dose category were 2.57 times more likely to experience an adverse event (aOR 2.57; 95% CI 1.02 -6.50; p=0.05). The same dose used in patients weighing >50 kg was found to be as safe as the reference category.
Patients weighing <50 kg and receiving high-dose CFZ (>200 mg) had a 3.3 times higher risk of gastrointestinal adverse events than patients weighing <50 kg and receiving 100 mg CFZ (aOR 3.30; 95% CI 1.51 - 7.19; p=0.003). The OR was adjusted for co-administration of ethionamide and para-aminosalicylic acid, as these two medicines are known to contribute significantly to gastrointestinal adverse events.
Patients weighing >50 kg and receiving >200 mg CFZ had a slightly higher risk compared with the reference category, but this was not significant (aOR 1.23; 95% CI 0.75 - 2.1; p=0.4).
On multivariate analysis it was observed that there was an increased risk of chest pain across weight bands, as indicated in Table 6.
Multivariate analysis indicated that patients of low weight (<50 kg) who received high doses of CFZ were at a slightly increased risk of adverse events related to the skin (1.2 times higher: aOR 1.2; 95% CI 0.55 - 2.62; p=0.7).
Discussion
This is the first study that compares adverse events related to varying doses of CFZ used for DR TB treatment in SA patients. The main finding was that there is an association between the dose of CFZ prescribed at different weight bands and the odds of an adverse event occurring. High doses of CFZ (>200 mg) in patients weighing <50 kg were associated with an increased frequency of adverse events. A similar correlation between CFZ dosage and adverse events, with a decrease in dose found to reduce the severity of the adverse events, was previously reported by Xu et al.[23] This was the case for any adverse event as well as adverse events related to the gastrointestinal tract and skin in our patient population. It was found that CFZ administration at any dose (100 mg or >200 mg) at any weight was associated with an increased chance of chest pain. A limitation of the study is that ECGs are not recommended routinely in patients receiving CFZ as standard of care in the guidelines, so this information was not available in the majority of the patients' folders. In the absence of objective tests such as an ECG or measurement of cardiac enzymes, chest pain was used as a surrogate marker of a possible cardiac adverse event, as this is the most common symptom of a cardiac event.
Several studies have assessed the safety and efficacy of CFZ for DR TB, with promising results of increased efficacy.[17-20] Doses used in all studies ranged from 50 mg to 300 mg, with many studies not reporting the doses prescribed. Safety information related to CFZ is available, with common side-effects of gastrointestinal and skin-related adverse events being reported. Similar common adverse events were found in the present study. However, ours is the only study that has focused on dose-related adverse events.
The jury is still out with regard to the need for a higher loading dose of CFZ followed by a daily maintenance dose, in view of the pharmacokinetic properties of CFZ.[12] Studies reporting on the optimal (safe and effective) dose of CFZ are lacking. Weight-based dosing was suggested by Gopal et al.[18] following a systematic review, and a dose of 100 mg/d in patients weighing >33 kg and 50 mg/d in patients weighing <33 kg was recommended. It was noted by the authors that although the optimal dose of CFZ is unknown, their recommendation was based on clinical experience and the published literature.[6] Schaad-Lanyi et al.[24] also suggested that in order to avoid the long-lasting accumulation towards steady state, higher daily loading doses are recommended at the beginning of therapy, followed by a daily maintenance dose. Previous WHO guidelines for the programmatic management of patients with DR TB recommended weight-based dosing.[9-11] Current SA guidelines[27] also suggest weight-based dosing of CFZ, which is supported by information currently under review that emanated from the present study. No studies have been conducted to assess dose-related efficacy or adverse events in SA patients.
Study limitations
The study has several limitations. Exclusion of patients from the study population owing to incorrect file numbers and the retrospective analysis limit the study conclusions. This was identified as a system failure, and corrective actions were implemented. The retrospective nature of the study relied on the clinicians documenting adverse events that patients experienced, which could be incomplete. The lack of objective blood results and ECG results made it difficult to confirm the adverse events documented.
Despite these limitations, the study contributes important knowledge on CFZ dose-related adverse events in a largely HIV-infected SA cohort with DR TB.
Conclusions and recommendations
This is the first study to provide data on CFZ dose-related adverse events in the SA population, and must be taken into consideration as SA reviews its DR TB guidelines. The increased risk associated with higher doses of CFZ in low-weight patients makes a case for active drug safety monitoring as part of standard of care. Routine monitoring of patients for cardiac dysrhythmias or QT prolongation (i.e. using an ECG), and for electrolyte imbalances (especially serum potassium) that can predispose to cardiotoxicity, is also recommended in view of the increased risk of chest pain at any dose that was reported in this study.
Declaration. This article was part of the submission towards NM's PhD (Health Sciences).
Acknowledgements. The authors thank the hospital management and all healthcare workers at the study site for their assistance and support. The assistance of Dr Cathy Connolly with statistical guidance and interpretation is greatly appreciated.
Author contributions. NM was responsible for the literature search, study design, data collection, data analysis and interpretation. All authors contributed equally to the analysis and write-up of the manuscript.
Funding. NM was supported by University of KwaZulu-Natal School of Health Sciences for registration fees, seed funding was provided by the Medical Education Partnership Initiative (MEPI) Grant Implementation Science Traineeship Program funded by the US President's Emergency Plan for AIDS Relief (PEPFAR) through the Fogarty International Centre, National Institutes of Health (grant #D43TW00231), and a further grant was awarded by CAPRISA, MRC TB-HIV Pathogenesis and Treatment Research Unit, Durban, South Africa.
Conflicts of interest. None.
References
1. World Health Organization. Global Tuberculosis Report 2019. https://www.who.int/tb/publications/globalreport (accessed 15 April 2019). [ Links ]
2. World Health Organization. The use of bedaquiline in the treatment ofmultidrug-resistant tuberculosis: Interim policy guidance. Geneva: WHO, 2013. www.ncbi.nlm.nih.gov/pubmed/23967502 (accessed 1 December 2019). [ Links ]
3. Tiberi S, Muâoz-Torrico M, Duarte R, Dalcolmo M, DAmbrosio L, Migliori GB. New drugs and perspectives for new anti-tuberculosis regimens. Pulmonology 2018;24(2):86-98. https://doi.org/10.1016/j.rppnen.2017.10.009 [ Links ]
4. Sharma D, Dhuriya YK, Deo N, Bisht D. Repurposing and revival of the drugs: A new approach to combat the drug resistant tuberculosis. Front Microbiol 2017;8:2452. https://doi.org/10.3389/fmicb.2017.02452 [ Links ]
5. National Department of Health, South Africa. Interim clinical guidance for the implementation of injectable-free regimens for rifampicin-resistant tuberculosis in adults, adolescents and children. 2018. http://www.tbonline.info/media/uploads/documents/dr_tb_clinical_guidelines_for_rsa_september_2018.pdf (accessed 20 November 2019). [ Links ]
6. Guglielmetti L, Le Dú D, Jachym M, et al. Compassionate use of bedaquiline for the treatment of multidrug-resistant and extensively drug-resistant tuberculosis: Interim analysis of a French cohort. Clin Infect Dis 2015;60(2):188-194. https://doi.org/10.3201%2Feid2505.181823 [ Links ]
7. National Department of Health, South Africa. Introduction of new drugs and drug regimens for the management of drug resistant tuberculosis in South Africa: Policy framework. Version 1.1: June 2015. http://www.nicd.ac.za/assets/files/Acrobat%20Document.pdf (accessed 1 December 2019). [ Links ]
8. World Health Organization. Active tuberculosis drug-safety monitoring and management (aDSM): Framework for Implementation. 2015. https://www.who.int/tb/publications/aDSM/en/ (accessed 1 December 2019). [ Links ]
9. World Health Organization. Guidelines for the programmatic management of drug-resistant tuberculosis. 2008. https://www.who.int/tb/challenges/mdr/programmatic_guidelines_for_mdrtb/en/ (accessed 1 December 2019). [ Links ]
10. World Health Organization. Guidelines for the programmatic management of multidrug-resistant tuberculosis. 2011. https://www.who.int/tb/challenges/mdr/programmatic_guidelines_for_mdrtb/en/ (accessed 1 December 2019). [ Links ]
11. World Health Organization. Companion handbook to the WHO guidelines for the programmatic management of drug resistant tuberculosis. 2014. https://www.who.int/tb/challenges/mdr/programmatic_guidelines_for_mdrtb/en/ (accessed 1 December 2019). [ Links ]
12. World Health Organization. WHO consolidated guidelines on drug-resistant tuberculosis treatment. 2019. https://apps.who.int/iris/handle/10665/311389?show=full (accessed 1 December 2019). [ Links ]
13. National Department of Health, South Africa. Standard treatment guidelines and essential medicines list for South Africa: Paediatric hospital level STGs and EML. 2017 edition. http://www.health.gov.za/index.php/component/phocadownload/category/456-hospital-level-paediatrics (accessed 1 December 2019). [ Links ]
14. National Department of Health, South Africa. Standard treatment guidelines and essential medicines list for South Africa: Primary health care level. 2018 edition. http://www.kznhealth.gov.za/pharmacy/PHC-STG-2018v1.pdf (accessed 1 December 2019). [ Links ]
15. Misra N, Padayatchi N, Naidoo P. Factors impacting on access to clofazimine in KwaZulu Natal, South Africa. Ponte J 2017;73(11):377-389. https://doi.org/10.21506/j.ponte.2017.11.24 [ Links ]
16. Medicines Control Council of South Africa. Section 21 application form. 2017. https://www.sahpra.org.za/documents/786a43016.12_Section_21_Application_Form_Jun17_v2.pdf (accessed 1 December 2019). [ Links ]
17. Padayatchi N, Gopal M, Naidoo R, et al. Clofazimine in the treatment of extensively drug-resistant tuberculosis with HIV coinfection in South Africa: A retrospective cohort study. J Antimicrob Chemother 2014;69(11):3103-3107. https://doi.org/10.1093/jac/dku235 [ Links ]
18. Gopal M, Padayatchi N, Metcalfe JZ, O'Donnell MR. Systematic review of clofazimine for the treatment of drug-resistant tuberculosis. Int J Tuberc Lung Dis 2013;17(8):1001-1007. https://doi.org/10.5588/ijtld.12.0144 [ Links ]
19. Hwang TJ, Dotsenko S, Jafarov A, et al. Safety and availability of clofazimine in the treatment of multidrug and extensively drug-resistant tuberculosis: Analysis of published guidance and meta-analysis of cohort studies. BMJ Open 2014;4:e004143. https://doi.org/10.1136/bmjopen-2013-004143 [ Links ]
20. Dey T, Brigden G, Cox H, Shubber Z, Cooke G, Ford N. Outcomes of clofazimine for the treatment of drug-resistant tuberculosis: A systematic review and meta-analysis. J Antimicrob Chemother 2013;68(2):284-293. https://doi.org/10.1093/jac/dks389 [ Links ]
21. O'Donnell MR, Padayatchi N, Kvasnovsky C, Werner L, Master I, Horsburgh CR. Treatment outcomes for extensively drug-resistant tuberculosis and HIV co-infection. Emerg Infect Dis 2013;19(3):416-424. https://doi.org/10.3201/eid1903.120998 [ Links ]
22. Tang S, Yao L, Hao X, et al Clofazimine for the treatment of multidrug-resistant tuberculosis: Prospective, multicenter, randomized controlled study in China. Clin Infect Dis 2015;60(9):1361-1367. https://doi.org/10.1093/cid/civ027 [ Links ]
23. Xu HB, Jiang RH, Xiao HP. Clofazimine in the treatment of multidrug-resistant tuberculosis. Clin Microbiol Infect 2012;18(11):1104-1110. https://doi.org/10.1111/j.1469-0691.2011.03716.x [ Links ]
24. Schaad-Lanyi Z, Dieterle W, Dubois J-PP, Theobald W, Vischer W. Pharmacokinetics of clofazimine in healthy volunteers. Int J Lepr 1987;55(1):9-15. [ Links ]
25. Nix DE, Adam RD, Auclair B, Krueger TS, Godo PG, Peloquin CA. Pharmacokinetics and relative bioavailability of clofazimine in relation to food, orange juice and antacid. Tuberculosis 2004;84(6):365-373. https://doi.org/10.1016/j.tube.2004.04.001 [ Links ]
26. Grosset JH, Tyagi S, Almeida DV, et al. Assessment of clofazimine activity in a second-line regimen for tuberculosis in mice. Am J Respir Crit Care Med 2013;188(5). https://doi.org/10.1164/rccm.201304-0753OC [ Links ]
27. National Department of Health, South Africa. Management of drug-resistant tuberculosis: Policy guidelines (updated January 2013). https://www.idealhealthfacility.org.za/docs/National-Priority-Health-Conditions/Management%20of%20Drug-Resistant%20Tuberculosis%202013.pdf (accessed 1 December 2019). [ Links ]
28. Wallis RS. Cardiac safety of extensively drug-resistant tuberculosis regimens including bedaquiline, delamanid and clofazimine. Eur Respir J 2016;48:1526-1527. https://doi.org/10.1183/13993003.01207-2016 [ Links ]
29. Aung KJM, van Deun A, Declercq E, et al. Successful '9-month Bangladesh regimen' for multidrugresistant tuberculosis among over 500 consecutive patients. Int J Tuberc Lung Dis 2014;18(10):1180-1187. https://doi.org/10.5588/ijtld.14.0100 [ Links ]
30. Cholo MC, Steel HC, Fourie PB, Germishuizen WA, Anderson R. Clofazimine: Current status and future prospects. J Antimicrob Chemother 2012;67(2):290-298. https://doi.org/10.1093/jac/dkr444 [ Links ]
 Correspondence:
Correspondence:
NMisra
nirupa.misra@kznhealth.gov.za
Accepted 29 July 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}