










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.110 no.1 Pretoria ene. 2020
http://dx.doi.org/10.7196/samj.2020.v110i1.14281
IN PRACTICE
COCHRANE CORNER
Interventions for preventing unintended pregnancies among adolescents
E L DavidsI, II; T KredoIII; C MathewsIV, V
IBPsych, MA, MPH, PhD; Cochrane South Africa, South African Medical Research Council, Cape Town, South Africa
IIBPsych, MA, MPH, PhD; Adolescent Health Research Unit, Division of Child and Adolescent Psychiatry, Department of Psychiatry and Mental Health, Faculty of Health Sciences, University of Cape Town, South Africa
IIIMB ChB, MMed (Clinical Pharmacology), Dip HIV Man, PhD; Cochrane South Africa, South African Medical Research Council, Cape Town, South Africa
IVBA, MSc (Med), PhD Adolescent Health Research Unit, Division of Child and Adolescent Psychiatry, Department of Psychiatry and Mental Health, Faculty of Health Sciences, University of Cape Town, South Africa
VBA, MSc (Med), PhD Health Systems Research Unit, South African Medical Research Council, Cape Town, South Africa
ABSTRACT
South Africa (SA) has an increasingly high rate of unintended pregnancies among adolescents, which are coupled with poor contraception knowledge. We highlight a systematic review that evaluated the effects of prevention interventions for unintended adolescent pregnancies, and provide implications for practice that are relevant to the SA context. The findings suggest the need for multifaceted interventions that are aligned with adolescent sexual and reproductive health best practices to address the unmet contraception knowledge gap, as well as unintended pregnancies among adolescents.
Pregnancy during adolescence is considered both an antecedent and consequence of school dropout in South Africa (SA).[1] Pregnancy during adolescence has implications that may result in detrimental health, educational, social and economic outcomes.[2] Many SA adolescents find themselves in an environment with a growing burden of HIV, where sexual and reproductive health needs are influenced by the numerous social determinants of health, such as poverty. The SA National Adolescent Sexual and Reproductive Health and Rights Framework Strategy[3] recommends the strengthening of interventions for adolescents, thus aiming to reduce the incidence of sexually transmitted infections and HIV, as well as unplanned and unintended pregnancies. Many interventions aimed at addressing unintended adolescent pregnancies have been evaluated, with varying evidence regarding what works best.[4]
Intervention and methods
We highlight a systematic review evaluating the effects of interventions to prevent unintended adolescent pregnancies.[5]
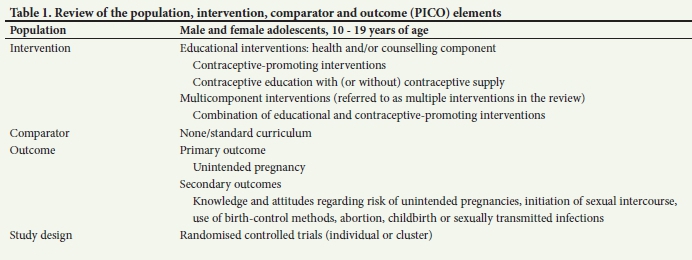
Educational and contraceptive-promoting interventions are included, which are intended to increase knowledge and change attitudes regarding the associated risk of unintended pregnancies. Interventions promoting correct and consistent use of contraceptives and delaying sexual debut were also included. The primary outcome of the review was unintended pregnancy, with sexual debut and condom use at last sex among the secondary outcomes. Table 1 outlines the eligible population, intervention, comparison and outcome (PICO).
The authors conducted a comprehensive search, without any language restrictions, using the Cochrane Central Register of Controlled Trials, MEDLINE, Embase, Dissertations Abstracts
Online, Grey Literature Network, HealthStar, PsycINFO, CINAHL, POPline, LILACS, Social Science Citation Index, Science Citation Index, and Specialist Health Promotion Register - until November 2015. Researchers in the field of adolescent sexual and reproductive health (SRH) were contacted with regard to unpublished or ongoing trials. All records were assessed independently by two review authors to determine eligibility. The authors used a standard data form to extract relevant details, including methodological quality assessed using the Cochrane risk-of-bias tool.[6] All outcomes were analysed using Review Manager (RevMan). Overall certainty was assessed with Grading of Recommendations, Assessment, Development and Evaluations (GRADE).
Results
The review included 53 randomised controlled trials, with a total of 105 368 participants, including 4 studies from low- and middle-income countries and the remaining studies from high-income countries. A large proportion of the studies were conducted in schools, and interventions were categorised as: (i) educational; (ii) contraceptive promoting; or (iii) multicomponent, consisting of educational and contraceptive-promoting interventions.
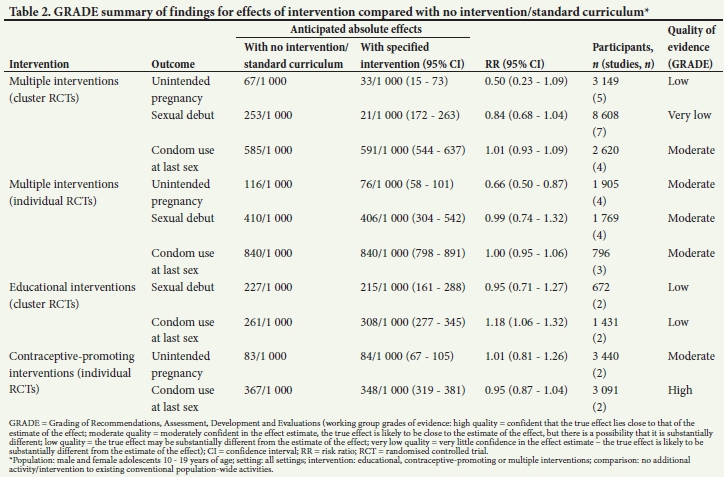
Multicomponent interventions probably reduced the risk of unintended pregnancy in the intervention group compared with the control group by 34% (risk ratio (RR) 0.66; 95% confidence interval (CI) 0.50 - 0.87; 4 studies; 1 905 participants; moderate certainty). There was little or no difference reported between the control and intervention groups for sexual debut and condom use at last sex in multicomponent interventions. The effects of only educational interventions on unintended pregnancy were not measured. There was low-certainty evidence that educational interventions may result in little or no difference in sexual debut. However, there may be an increase in self-reported condom use at last sex (RR 1.18; 95% CI 1.06 - 1.32; 2 studies; 1 431 participants; low certainty). Contraceptive-promoting interventions alone probably have little or no effect on the risk of unintended pregnancy (RR 1.01; 95% CI 0.81 -1.26; 2 studies; 3 440 participants; moderate certainty) or condom use at last sex (RR 0.95; 95% CI 0.87 - 1.04; 2 studies; 3 091 participants; high certainty). The findings are summarised in Table 2.
Conclusions
The authors conclude that multicomponent interventions, including educational and contraceptive-promoting components, had the potential to reduce unintended pregnancies among adolescents.
Implications for policy and practice in South Africa
Pregnancy during adolescence can have a devastating effect on health and wellbeing, lasting into adulthood, and undermining the health and wellbeing of the next generation. It is a major contributor to maternal and child mortality, and leads to dropping out of school, lower educational achievement, other negative socioeconomic effects, and intergenerational cycles of ill-health and poverty.[7-9] To ensure targeted action and to track progress in achieving adolescent health, a Lancet commission on adolescent health and wellbeing
proposed 12 headline indicators encompassing health needs, health risks and social determinants of health. In recognition of the impact of adolescent pregnancy, one of these headline indicators is 'met need for contraception[10]
In SA, adolescent women aged 15-19 years have a poorer knowledge regarding contraception, a higher unmet need for contraception and a higher prevalence of unintended pregnancies than adults.[11] The SA Demographic and Health Survey 2016 found that 16% of adolescent girls 15 - 19 years of age had begun bearing children.[12] The systematic review in this article can inform SA initiatives to meet adolescents' needs for contraception and prevent unintended pregnancies.[5] The review confirms that to prevent unintended pregnancies, it is not enough to provide health promotion in schools and other settings to increase adolescents' motivation to access contraceptive services. The review provides evidence that to make a difference, initiatives need to be multifaceted, a finding which is aligned to best practice for promoting SRH.[13] Effective strategies include a combination of interventions to generate demand for adolescent SRH services, and interventions to improve the supply and accessibility of high-quality adolescent-responsive SRH services. In SA, a school is one of the appropriate platforms for demand generation interventions, because the system is tasked with providing comprehensive SRH education by means of the life-orientation curriculum.[14] Yet, school-based educational initiatives may not adequately address SRH challenges faced by young people[15] and may ignore adolescent girls' and young women's narratives of sexuality,[16] thus perpetuating stigmatisation of adolescent sexuality. In designing effective strategies, it is important to recognise and address the structural constraints adolescents face in accessing contraceptives from health services. Issues such as stigmatisation of adolescent sexuality, their use of SRH services and lack of support from parents and health workers act as barriers to youth-friendly SRH services.[17] The early, pioneering SA National Adolescent Friendly Clinic Initiative (NAFCI) is an example of a multifaceted intervention to promote adolescent SRH.[18] The long-term impact attributed to NAFCI is a lower likelihood of teen childbearing, enabling adolescents to complete more years of schooling and earn higher wages when they are young adults.[19] This exemplifies the potential for achieving 'triple dividend' with effective interventions to prevent unintended pregnancy during adolescence: better health and wellbeing during adolescence and adulthood, which will benefit the next generation.[20]
Declaration. None.
Acknowledgements. The authors would like to acknowledge support from the SA Medical Research Council's Office of AIDS and TB Research.
Author contributions. ELD, TK and CM contributed equally to the manuscript. ELD wrote the first draft, with further inputs from TK and CM.
Funding. None.
Conflicts of interest. Cochrane Corners are co-ordinated from Cochrane SA, but the views expressed in this article are those of the authors and do not necessarily reflect the views or policies of Cochrane or the SA Medical Research Council.
References
1. Stoner MC, Rucinski KB, Edwards JK, et al. The relationship between school dropout and pregnancy among adolescent girls and young women in South Africa: A HPTN 068 analysis. Health Educ Behav 2019;46(4):559-568. https://doi.org/10.1177/1090198119831755 [ Links ]
2. Wado YD, Sully EA, Mumah JN. Pregnancy and early motherhood among adolescents in five East African countries: A multi-level analysis of risk and protective factors. BMC Pregnancy Childbirth 2019;19(1):59. https://doi.org/10.1186/s12884-019-2204-z [ Links ]
3. Department of Social Development. National Adolescent Sexual and Reproductive Health and Rights Framework Strategy. 2015. http://srjc.org.za/wp-content/uploads/2019/10/02-National-Adolescent-Sexual-and-Reproductive-Health-and-Rights-Framework-Strategy-pdf-003.pdf (accessed 13 June 2019). [ Links ]
4. Kâgesten A, Parekh J, Tunçalp Õ, Turke S, Blum RW. Comprehensive adolescent health programs that include sexual and reproductive health services: A systematic review. Am J Public Health 2014;104(12):e23-e36. https://doi.org/10.2105/AJPH.2014.302246 [ Links ]
5. Oringanje C, Meremikwu MM, Eko H, Esu E, Meremikwu A, Ehiri JE. Interventions for preventing unintended pregnancies among adolescents. Cochrane Database Syst Rev 2016;(4):1-88. https://doi.org/10.1002/14651858.CD005215.pub2 [ Links ]
6. Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. The Cochrane Collaboration, 2011. www.cochrane-handbook.org (accessed 29 May 2019). [ Links ]
7. World Health Organization. Adolescent Pregnancy. Geneva: WHO, 2018. https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnancy (accessed 23 June 2019). [ Links ]
8. Gigante DP, de França GV, de Lucia Rolfe E, et al. Adolescent parenthood associated with adverse socio-economic outcomes at age 30 years in women and men of the Pelotas, Brazil: 1982 birth cohort study. Br J Obstet Gynaecol 2019;126(3):360-367. https://doi.org/10.1111/1471-0528.15428 [ Links ]
9. Bahamondes L. Long term social consequences of adolescent pregnancy. Int J Obstet Gynaecol 2019;126(3):368. https://doi.org/10.1111/1471-0528.15428 [ Links ]
10. Azzopardi PS, Hearps SJ, Francis KL, et al. Progress in adolescent health and wellbeing: Tracking 12 headline indicators for 195 countries and territories, 1990 -2016. Lancet 2019;393(10176):1101-1118. https://doi.org/10.1016/S0140-6736(18)32427-9 [ Links ]
11. Chersich MF, Wabiri N, Risher K, et al. Contraception coverage and methods used among women in South Africa: A national household survey. S Afr Med J 2017;107(4):307-314. https://doi.org/10.7196/SAMJ.2017.v107i4.12141 [ Links ]
12. National Department of Health, Statistics South Africa, South African Medical Research Council and Inner City Fund. South Africa Demographic and Health Survey 2016. Pretoria: NDoH, 2019. [ Links ]
13. Denno DM, Hoopes AJ, Chandra-Mouli V. Effective strategies to provide adolescent sexual and reproductive health services and to increase demand and community support. J Adolesc Health 2015;56(1):S22-S41. https://doi.org/10.1016/j.jadohealth.2014.09.012 [ Links ]
14. Glover J, Macleod C. Rolling out Comprehensive Sexuality Education in South Africa: An Overview of Research Conducted on Life Orientation Sexuality Education. Grahamstown: Rhodes University, 2016. https://www.ru.ac.za/media/rhodesuniversity/content/criticalstudiesinsexualitiesandreproduction/documents/Life_Orientation_Policy_Brief_Final.pdf (accessed 28 July 2019). [ Links ]
15. Ngabaza S, Shefer T. Sexuality education in South African schools: Deconstructing the dominant response to young people's sexualities in contemporary schooling contexts. Sex Educ 2019;19(4):422-435. https://doi.org/10.1080/14681811.2019.1602033 [ Links ]
16. Mayeza E, Vincent L. Learners' perspectives on life orientation sexuality education in South Africa. Sex Educ 2019;19(4):472-485. https://doi.org/10.1080/14681811.2018.1560253 [ Links ]
17. Margherio C. Centering female agency while investigating contraceptive use: A case study in Agincourt, South Africa. Int J Equity Health 2019;18(1):60. https://doi.org/10.1186/s12939-019-0965-7 [ Links ]
18. Dickson-Tetteh K, Pettifor A, Moleko W. Working with public sector clinics to provide adolescent-friendly services in South Africa. Reprod Health Matters 2001;9(17):160-169. [ Links ]
19. Branson N, Byker T. Causes and consequences of teen childbearing: Evidence from a reproductive health intervention in South Africa. J Health Econ 2018;57:221-235. https://doi.org/10.1016/j.jhealeco.2017.11.006 [ Links ]
20. Patton GC, Sawyer SM, Santelli JS, et al. Our future: A Lancet commission on adolescent health and wellbeing. Lancet 2016;387(10036):2423-2478. https://doi.org/10.1016/S0140-6736(16)00579-1 [ Links ]
 Correspondence:
Correspondence:
E L Davids
eugene.davids@mrc.ac.za
Accepted 31 July 2019


{kind=link}
{kind=link}